February 2022 Viracta Therapeutics, Inc - Precision Oncology for Virus-Associated
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Viracta Therapeutics, Inc.
February 2022
Precision
Oncology for
Virus-Associated
Cancers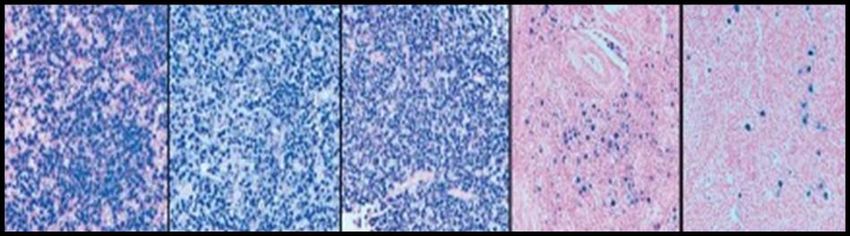
Forward Looking Statements
This communication contains "forward-looking" statements within the meaning of the Private Securities Litigation Reform Act of 1995, which are based on current
expectations, estimates and projections based on information currently available to management of Viracta Therapeutics, Inc. (“Viracta” or the “Company”),
including, without limitation, statements regarding: Viracta’s development pipeline, including nanatinostat and vecabrutinib; the details, timeline and expected
progress for Viracta’s ongoing trials; the expected ability of Viracta to undertake certain activities and accomplish certain goals with respect to its clinical program in
EBV+ lymphoma, EBV+ solid tumors, other virus-associated malignancies or its programs; expectations regarding future therapeutic and commercial potential with
respect to Viracta’s clinical program in EBV+ lymphoma, EBV+ solid tumors or other virus-associated malignancies; the ability of Viracta to support multiple new
drug application filings and approvals from the NAVAL-1 trial; the potential of Viracta’s synthetic lethality approach and Viracta's ability to expand the impact and
broaden the reach of its therapeutic approach; the expected data from the EBV+ solid tumor trial in 2022; Viracta’s plans to meet with the FDA to discuss
preliminary results from the NAVAL-1 trial and amending the NAVAL-1 protocol to add patients as necessary to enable registration; Viracta’s plans to provide
updates on NAVAL-1 in the second half of 2022; the significance of Viracta’s data being featured at the 2021 ASH Annual Meeting; Viracta's cash projections and
the sufficiency its cash and cash equivalents to fund operations into 2024; the future availability of capital under Viracta’s credit facility; the expected future
milestones and key upcoming events and their significance; and other statements that are not historical facts. Risks and uncertainties related to Viracta that may
cause actual results to differ materially from those expressed or implied in any forward-looking statement include, but are not limited to: Viracta’s ability to
successfully enroll patients in and complete its ongoing and planned clinical trials; Viracta's plans to develop and commercialize its product candidates, including all
oral combinations of nanatinostat and valganciclovir; the timing of initiation of Viracta's planned clinical trials; the timing of the availability of data from Viracta's
clinical trials; the possibility that previous preclinical and clinical results may not be predictive of future clinical results; the timing of any planned investigational new
drug application or new drug application; Viracta's plans to research, develop and commercialize its current and future product candidates; the clinical utility,
potential benefits and market acceptance of Viracta's product candidates; Viracta's ability to identify additional products or product candidates with significant
commercial potential; developments and projections relating to Viracta's competitors and its industry; the impact of government laws and regulations; Viracta's
ability to protect its intellectual property position; and Viracta's estimates regarding future expenses, capital requirements and need for additional financing.
These risks and uncertainties may be amplified by the COVID-19 pandemic, which has caused significant economic uncertainty. If any of these risks materialize or
underlying assumptions prove incorrect, actual results could differ materially from the results implied by these forward-looking statements. Additional risks and
uncertainties that could cause actual outcomes and results to differ materially from those contemplated by the forward-looking statements are included under the
caption “Risk Factors” and elsewhere in Viracta’s most recent filings with the SEC and any subsequent reports on Form 10-K, Form 10-Q or Form 8-K filed with the
SEC from time to time and available at www.sec.gov. The forward-looking statements included in this communication are made only as of the date hereof.
Viracta assumes no obligation and does not intend to update these forward-looking statements, except as required by law or applicable regulation.
2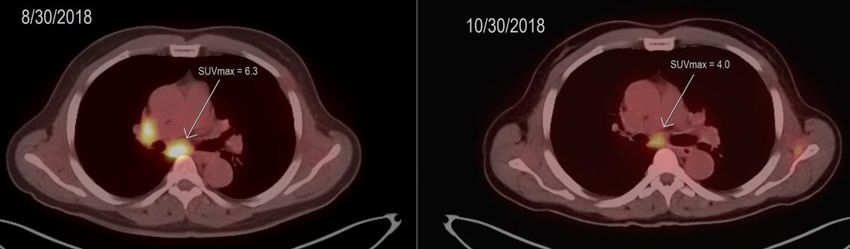
Viracta Therapeutics
A precision oncology company focused on the treatment of virus-associated malignancies
Novel “Kick & Kill” all-oral approach to EBV+ cancers; uniquely targets a latent virus to enable synthetic lethality
Pivotal NAVAL-1 study in multiple R/R EBV+ lymphoma subtypes; update expected in 2H 2022
Multinational Phase 1b/2 study in advanced EBV+ solid tumors; preliminary efficacy data anticipated in 2H 2022
Pipeline of preclinical assets and additional virus targets
Strong balance sheet with cash runway into mid-2024; durable IP out to at least 2040
EBV+: Epstein-Barr Virus Positive; R/R: Relapsed/Refractory
3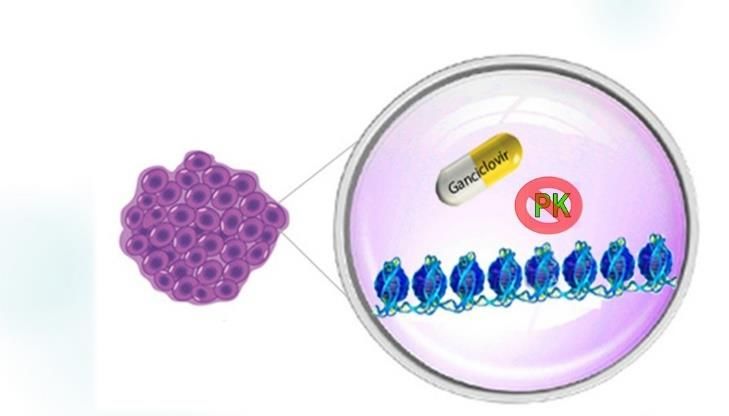
Pipeline of Clinical and Preclinical Product Candidates
Innovative approaches to virus-associated cancers
PRODUCT CANDIDATES INDICATION PRECLINICAL EARLY-STAGE CLINICAL LATE-STAGE CLINICAL
Nana-val Relapsed/Refractory
(nanatinostat + valganciclovir) EBV+ Lymphoma NAVAL-1 Pivotal Trial: Enrolling
Recurrent/Metastatic
Nana-val Phase 1b/2 Trial: Enrolling
EBV+ Solid Tumors
Vecabrutinib
I-O Combinations
BTK/ITK inhibitor, in combination
Multiple Undisclosed
w/ CAR T-cell therapy
VRx-510* Oncology
PDK-1 inhibitor Multiple Undisclosed
HPV+ cancers
Other HDACi Combinations I-O Combinations
Multiple Undisclosed
EBV+: Epstein-Barr Virus Positive; I-O: Immuno-oncology; HPV: Human papillomavirus; *formerly SNS-510
4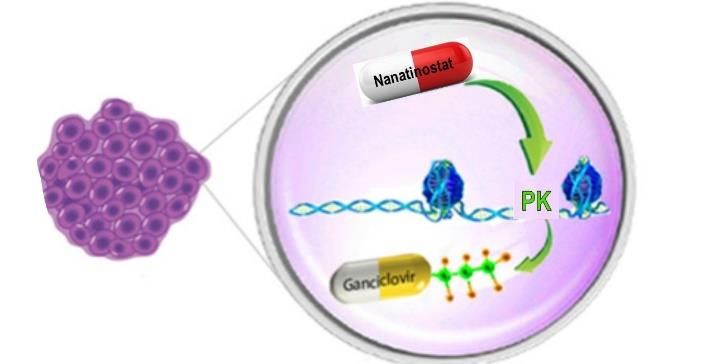
Epstein-Barr Virus (EBV): A High Global Cancer Priority
EBV+ malignancies account for ~2% of all new cancers globally, currently no approved therapies
▪ ~ 90% of the adult population are infected w/ EBV
▪ Persists as a life-long latent infection, remaining
dormant within cell nuclei
▪ Latency confers resistance to anti-viral therapies and
facilitates evasion of immune detection
EBV infects cells Latent infection Latently infected
▪ Linked to a variety of cancers established in cells can continue
subset of cells to proliferate,
• ~310,000 new cases/year of lymphoma, NPC and GC
evade immune
▪ Poor prognosis, no approved therapies detection, and
become malignant
▪ Responsible for ~180,000 cancer deaths/year*
Source: Wu L, et al. Exp. Therapeutic Med. 15: 3687, 2018; Kahn,G, et al. BMJ 10:1136, 2020. NPC: Nasopharyngeal carcinoma; GC: Gastric cancer
5
Viracta’s Oral “Kick and Kill” Approach Selectively Targets EBV+ Cancer Cells
Nanatinostat sensitizes EBV+ tumors to the cytotoxic effects of ganciclovir
LATENCY THE KICK THE KILL
EBV is latent in cancer cells and viral Nanatinostat selectively and Cytotoxic GCV inhibits DNA
kinase genes are silenced potently induces expression of EBV replication by chain termination
epigenetically. protein kinase (PK), which leading to apoptosis in EBV+ cancer
Valganciclovir, an antiviral prodrug of activates GCV and converts it to its cells. This combination approach is
ganciclovir (GCV), is inactive in the cytotoxic form a form of synthetic lethality
absence of the expression of the viral
protein kinase (PK)
6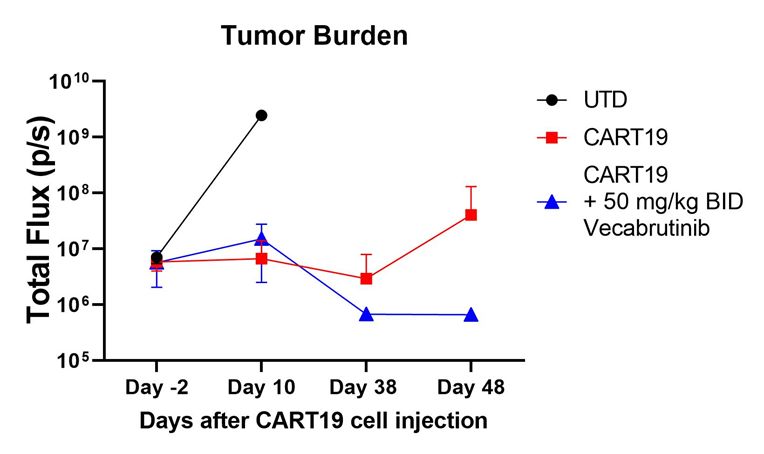
Nana-val: EBV+ Lymphoma Program
EBV is Easily Detectable and Associated with Inferior Survival Outcomes in
Several Lymphoma Subtypes
Diffuse Large B-Cell Lymphoma Peripheral T-cell Lymphoma Hodgkin's Lymphoma
(Progression-Free Survival) (Overall Survival) (Failure-Free Survival)
EBV is detectable by in situ hybridization for EBV encoded RNA (EBER-ISH) EBV positivity, by lymphoma subtype
DLBCL Plasmablastic NK/T AITL HL DLBCL 5-10%
PTCL, NOS 25-58%
AITL 70-80%
Dark blue:
ENKTL 100%
EBV-RNA PTLD 60-80%
Hodgkin’s 20-30%
Follicular ~3%
Source: Lu et al. Sci Rep. 2015; Haverkos et al. Int J Cancer. 2017; Dupuis et al. Blood. 2006; Kanakry et al. Blood 2013; Swerdlow et al. (2017) WHO classification of Tumours of the Haematopoietic
and Lymphoid Tissues; Mackrides et al. Am J Hematol. 2019. DLBCL: Diffuse large B cell lymphoma; PTCL: Peripheral T cell lymphoma; HL: Hodgkin lymphoma;
8
Nana-val: Phase 1b/2 Trial in R/R EBV+ Lymphoma
▪ Open-label, dose escalation/expansion study of Nana-val combination in patients with recurrent EBV+ lymphoma
▪ Eligibility: R/R EBV+ lymphoma (any histology), ≥1 prior therapy with no curative options per Investigator
▪ Endpoints: Response rate (ORR by PET-CT; Lugano 2014), response duration, safety, clinical benefit rate (CBR)
▪ Dosing Schedule: nanatinostat 20mg PO daily, days 1-4/week + valganciclovir 900mg PO daily
▪ Phase 1b (n=25): Identified recommended Phase 2 dose (RP2D); Phase 2: Expansion at the RP2D (n=30)
CYCLE 1 CYCLE 2 CYCLE 3 CYCLE 4
Continued until disease
progression or
28 Days 28 Days 28 Days 28 Days withdrawal
PET-CT PET-CT
▪ Final data presented at the American Society of Hematology Annual Meeting (ASH) 2021
PO: by mouth
9
Heavily Pretreated Patient Population with All Major Subtypes of Aggressive
Lymphomas Represented
Key Patient Characteristics N=55 EBV+ Lymphoma Subtype Enrolled (n)
Median age (y), (range) 60 (19-84) B-NHL 10 (18%)
No. of previous lines of antineoplastic DLBCL 7
therapy - no. (%) Other B Cell 3
• 1 13 (24%) T/NK-NHL 21 (38%)
• 2 19 (35%)
ENKTL 9
• ≥3 23 (42%) PTCL-NOS 5
Median no. prior therapies (range) 2 (1-11) AITL 6
Brentuximab 14 (26%) CTCL 1
ASCT/alloSCT 12 (22%)
Immunodeficiency-associated LPD 13 (24%)
Checkpoint inhibitor 9 (16%)
HDAC inhibitor PTLD 4
6 (11%)
EBV CTL Other [SLE (2), CVID (1), PI (1)] 4
5 ( 9%)
HIV-associated lymphoma 5
Refractory to last therapy (n,%) 41 (75%)
Hodgkin (cHL) 11 (20%)
Exhausted all therapies per
53 (96%) Total 55
Investigator
Data cutoff: October 28, 2021, Presented at ASH 2021. DLBCL: Diffuse large B-cell lymphoma, ENKTL: Extranodal NK/T-Cell Lymphoma, PTCL: Peripheral T-cell lymphoma, AITL: Angioimmunoblastic
T-cell lymphoma, CTCL: Cutaneous T-cell lymphoma, PTLD: Post-transplant lymphoproliferative disease
10Complete Responses Observed Across Multiple EBV+ Lymphoma Subtypes
Median time to response: 1.8 months (range: 33-162 days)
PTCL- Hodgkin
All patients DLBCL Other B- ENKTL CTCL HIV-L IA-LPD
NOS/AITL (cHL)
(n=43) (n=6) NHL (n=2) (n=8) (n=1) (n=4) (n=6)
(n=6) (n=10)
Response
ORR 17 (40%) 4 (67%) - 5 (63%) 4 (67%) - - 3 (50%) 1 (10%)
CR 8 (19%) 2 (33%) - 1 (13%) 3 (50%) - - 2 (33%) -
PR 9 (21%) 2 - 4 1 - - 1 1
SD 7 (16%) 1 - - 1 - - 5
PD 19 (44%) 1 2 3 1 1 4 3 4
Clinical benefit
24 (56%) 5 (83%) 5 (63%) 5 (83%) 3 (50%) 6 (60%)
rate
*Evaluable patients: EBER-ISH with ≥1 post-treatment response assessment
77% 96%
Data cutoff: October 28, 2021, Presented at ASH 2021; DLBCL: Diffuse large B-cell lymphoma, ENKTL: Extranodal NK/T-Cell Lymphoma, PTCL/ AITL: Peripheral T-cell lymphoma/ Angioimmunoblastic
T-cell lymphoma, IA-LPD: Immunodeficiency-associated lymphoproliferative disorders, CTCL: Cutaneous T-cell lymphoma; ORR: Overall Response Rate, CR: Complete Response, PR: Partial Response, 11
SD: Stable Disease, PD: Progressed Disease, Clinical Benefit Rate = CR + PR + SD ≥ 6 months; EBER-ISH: Epstein-Barr encoding region in situ hybridizationDuration of Response for All Patients by Lymphoma Subtype
DLBCL
T/NK-NHL
Median duration of response =
10.4 months (n=17)
100 censored subjects
90
80
70
Event-free probability
IA-LPD 60
50
40
30
20
10
Hodgkin 0 Me dian duration of re sponse : 10.4 (3.7, NA)
(cHL) 0 2 4 6 8 10 12 14 16 18 20 22 24 26 28 30 32
Time, Months
Months
Data cutoff: October 28, 2021, Presented at ASH 2021; DLBCL: Diffuse large B-cell lymphoma, NHL: Non-Hodgkin’s lymphoma, IA-LPD: Immunodeficiency-associated lymphoproliferative disorders
12Favorable Safety Profile
Grade 3/4 treatment-emergent AEs in ≥3 patients (5%)
▪ Oral regimen was generally well-tolerated
Phase 1b Phase 2
G3 G4 G3 G4
▪ Most common TEAEs overall were:
• Nausea (38%)
Thrombocytopenia 5 (20%) 3 (12%) 1 (3%) 2 (7%) • Thrombocytopenia (36%)
• Neutropenia (34%)
Neutropenia 4 (16%) 5 (20%) 3 (10%) 4 (13%) • Anemia, constipation (both 31%)
Anemia 4 (16%) - 6 (20%) 1 (3%) • Creatinine elevation, diarrhea, fatigue (all 26%)
• Decreased appetite (22%)
Lymphopenia 2 (8%) 3 (12%) 2 (7%) 1 (3%)
▪ Serious adverse events (SAEs) occurred in 16
Leukopenia 1 (4%) 2 (8%) 1 (3%) 1 (3%) patients (29%); 8 in Phase 2
Acute kidney injury 2 (8%) 1 (4%) - 1 (3%) • Treatment-emergent SAEs occurring in ≥2 patients
were febrile neutropenia, acute kidney injury and
GI hemorrhage 2 (8%) - 2 (7%) - pneumonia (all n=2)
Febrile neutropenia 1 (4%) - 2 (7%) 1 (3%) ▪ Potential for combining with other chemo-and/or
immunotherapies
Data cutoff: October 28, 2021, Presented at ASH 2021
13Case Studies
CASE STUDY 01 CASE STUDY 02
37 y.o. female, extranodal NK/T-cell Lymphoma (ENKTL) 58 y.o. male, peripheral T-cell lymphoma (PTCL)
Refractory to 2nd line autologous stem cell transplantation; Durable PR following prior HDACi therapy and autologous
durable response >28 months and counting stem cell transplantation
▪ SMILE (L-asparaginase-containing) plus radiotherapy (1st ▪ CHOEP regimen (1st line); romidepsin/ASCT (2nd line);
Line), ASCT (2nd line); refractory to last therapy romidepsin (3rd line) with disease progression at 5 months
• Relapses post- SMILE regimen generally have a poor ▪ Durable PR on Nana-val (10.6 months)
prognosis, with a median overall survival of 4-6 months
▪ Patient was being considered for palliative care
▪ Partial remission 1.9 months after start of oral Nana-val
HDACi: HDAC inhibitor; ASCT: Autologous stem cell transplantation; CHOEP: CHOP, etoposide; PR: Partial Response
14ORR/DoR from Single Arm Studies in R/R Lymphoma Receiving Accelerated
Approval
Nana-val ORR/DoR in EBV+ lymphoma compares favorably with other drugs receiving accelerated approval
25
Median Duration of Response (mDoR, months)
tafasitamab/lenalidomide
zanubrutinib
20 Bubbles represent ORR/DoR for single-arm
ibrutinib
accelerated approvals:
Nana-val
EBV+ T cell
romidepsin Nana-val
15 EBV+ DLBCL Teal T-cell lymphomas
copanlisib
tazemetostat (WT)
DLBCL (Kymriah® ORR 50%; mDoR NR)
bendamustine Red
pralatrexate (Lisocabtagene ORR 73%; mDOR NR
10
umbralisib axicabtagene
belinostat bortezomib Blue Other lymphomas
vorinostat
5 brentuximab vedotin Response data for Nana-val in T-cell and
duvelisib
Orange Diffuse large B-cell lymphoma
selinexor
0
0 20 40 60 80 100
Overall Response Rate (ORR)
R/R: Relapsed/refractory; NR: Not reached
15NAVAL-1: Pivotal Phase 2 Trial in R/R EBV+ lymphoma
Global basket study with an adaptive Simon 2-stage design
▪ Patient population: Stage 1 Stage 2
• R/R lymphoma with ≥ 2 prior therapies
EBV + Multiple lymphoma subtypes
and no curative options
- Extranodal NK/T cell lymphoma: ≥1 prior therapy EBV+ DLBCL, NOS
• Two-stage study design estimated to enroll ~140
patients Peripheral T-cell Further
expansion of
▪ Primary end point: Objective response
Extranodal NK/T (2L) Expand cohorts promising
rate (ORR) by IRC from Stage 1 cohorts with
HIV-associated meeting efficacy additional
▪ Potential to further expand cohorts with
threshold patients may
promising activity after Stage 2
PTLD support
▪ Anticipate providing an update on initial registration
Hodgkin
cohort(s) that have advanced from Stage 1
into Stage 2 in H2 2022
Other
R/R: Relapsed/refractory; DLBCL: Diffuse Large B-Cell Lymphoma; PTLD: Post-transplant lymphoproliferative disorder
16Key Regulatory Achievements
Orphan Drug Designations End of Phase 2 Meeting
Fast Track Designation
granted for Nana-val: (November 2020)
(November 2019)
• EBV+ diffuse large b-cell Obtained alignment on design of
For the treatment of
lymphoma (DLBCL), NOS - 2021 Phase 2 pivotal study:
relapsed/refractory (R/R) EBV+
• T-cell lymphoma - 2020 lymphoid malignancies • NAVAL-1: Single arm basket
• Post-transplant study with an adaptive design
lymphoproliferative disorder in R/R patients with EBV+
(PTLD) - 2019 lymphomas
• Plasmablastic lymphoma - 2019
17Encouraging Feedback from Physicians and Payors for Nana-val
Primary market research for Viracta’s differentiated approach in EBV+ Lymphoma
Unmet Need EBV Testing Potential Nana-val Utilization Forecast
▪ 10%-15% of all lymphomas are ▪ Familiarity with EBV-associated ▪ Positive perceptions of Nana-val ▪ Potential upside in share of
EBV-associated in U.S. cancers is not yet universal by physicians and payors due EBV+ patients, duration of
to: therapy, and price
▪ ~10,000 EBV+ lymphomas/year in
▪ Opportunity to drive significant • Novel MOA
U.S.: ▪ Opportunity for long-term
awareness • Promising preliminary clinical
• EBV+ DLBCL: ~3,000 upside:
efficacy and safety data
• EBV+ PTCL: ~1,200 ▪ Opportunity to increase testing • Convenient oral dosing • Other EBV+ malignancies
• EBV+ ENKTL: ~500 in community clinics • Earlier LoT/combination
• EBV+ HIV Lymphoma: ~1,100 ▪ Strong interest in earlier LoT, • Increased testing rates
• EBV+ PTLD: ~1,000 ▪ Testing rates could reach >90% combination use, mostly for DLBCL
• EBV+ Hodgkin: ~3,200 within 2 years of Nana-val launch
▪ EBV-positivity adversely affects KOL/Payer TPP Reaction:
the clinical outcome
Source: 2021 Nanatinostat-VGCV Market Assessment; Epidemiology of Epstein-Barr virus Associated Cancers in the US, Tessellon, Inc., 2020
LoT: Line of therapy; TPP: Target Product Profile
18Nana-val: EBV+ Solid Tumor Program
Preclinical Proof of Concept for Nana-val in EBV+ Solid Tumors
*** *** ***
▪ Annual incidence of nasopharyngeal
** carcinoma (NPC) and gastric carcinoma
(GC):
• North America: ~5,500
• Global: ~218,000
% Tumor Mass
▪ High unmet need, especially for R/R
disease
▪ Efficacy of combination approach initially
reported in murine models of EBV+ NPC
and GC using a first generation
intravenous (IV) HDACi + IV ganciclovir
Tumor: EBV- NPC EBV+ NPC EBV+ NPC EBV+ GC
(HONE1) (HA) (C666-1) (SNU-719)
Control GCV Romidepsin Romidepsin + GCV
Source: Hui KW, et al. Int J Cancer:138.125-136 (2016); Epidemiology of Epstein-Barr virus Associated Cancers in the US, Tessellon, Inc., 2020; Kahn,G, et al. BMJ 10:1136,2020
R/R: Relapsed/refractory; HDACi: HDAC inhibitor
20Nanatinostat Induction of EBV Protein Kinase in Tumor Cells and
Accumulation in Tumor Tissue
Induction by Nanatinostat of EBV Protein Kinase RNA High Tumor Uptake of Nanatinostat in a
in SNU-719 EBV+ Gastric Carcinoma Cell Line Murine Xenograft Tumor Model
9
140
8
120
7
tumor (ng/g) concentration
6 100
Fold Increase
Plasma (ng/ml) or
5 80
4
60
3
40
2
1 20
0 0
Untreated DMSO Nstat 200nM Plasma Tumor
Nanatinostat (50 mg/kg dose)
Source: Moffat, et al. J. Med Chem. 53: 24, 2010.; Nstat: Nanatinostat
21Nana-val in Advanced EBV+ Solid Tumors: Phase 1b/2 Study Overview (301)
Preliminary efficacy data from Phase 1b portion expected in the second half of 2022
▪ Evaluating safety and preliminary efficacy of
Nana-val alone and in combination with Phase 1b dose escalation
EBV+ R/M NPC
pembrolizumab N = up to 18 patients
▪ Patient population: Up to 88 patients
• Phase 1b: Establish Phase 2 Dose
– Dose selection: EBV + recurrent/metastatic
nasopharyngeal carcinoma (R/M NPC)
– Dose expansion: Other recurrent EBV + solid tumors
• Phase 2: EBV+ R/M NPC Phase 1b dose expansion Phase 2
Other EBV+ solid tumors EBV+ R/M NPC
▪ Endpoints: (gastric cancer, lymphoepithelioma, N = 60 patients
leiomyosarcoma)
• Phase 1b: Dose limiting toxicities N = up to 10 patients
• Phase 2: ORR by RECIST Nana-val Nana-val ± anti-PD-1
• Secondary: Safety, efficacy, PK
ORR: Objective Response Rate, RECIST: Response Evaluation Criteria in Solid Tumors, PK: Pharmacokinetics
22Nana-val “Kick & Kill” Approach Protected by a Durable IP Portfolio
Granted patents provide protection into at least 2040
2000 2005 2010 2015 2020 2025 2030 2035 2040 2045
Nanatinostat Composition of Matter Expiration January 2027
US 7,932,246 (Granted) (Including Patent Term Adjustment)
Methods of Treatment with Nana-val
Expiration March 2031
10,857,152 (Granted)
Nana-val Dosing Schedule
Expiration May 2040
US 10,953,011 (Granted)
Additional intellectual property (IP) protection
▪ Additional pending applications for expanded patent protection in various methods and formulations
▪ Eligible for Patent Term Extension upon approval in the US
▪ Eligible for 7 years of market exclusivity upon approval in the US based on 4 granted Orphan Drug designations
▪ Eligible for 8+2+1 years data exclusivity in Europe
▪ Eligible for 6 months pediatric exclusivity, which is stackable to all other exclusivities
23Vecabrutinib in CAR T-cell Therapy
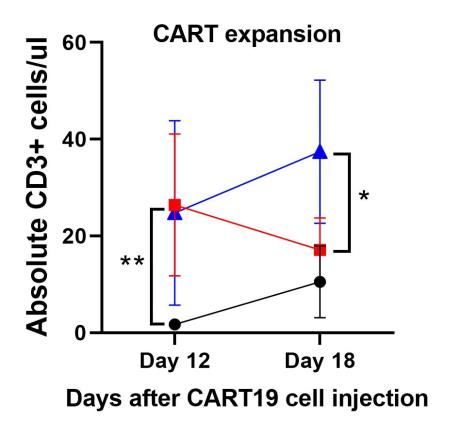
Vecabrutinib Positively Regulated CAR T-Cell Therapy
Vecabrutinib improved CAR T efficacy in a murine model of mantle cell lymphoma
▪ Vecabrutinib is a well-tolerated, non-covalent and reversible inhibitor of Bruton’s kinase and interleukin 2-inducible kinase
▪ While CAR T-cell therapy is successful in treating a subset of patients with hematologic malignancies, its use is limited by
resistance due to T-cell dysfunction (exhaustion) and toxicities due to cytokine release syndrome and neurotoxicity
Increased T-cell Increased T-cell Killing
Reduced Tumor Burden
Proliferation In Vitro
MCL Murine Model MCL Murine Model In vitro: JeKo-1 + CAR T cells (1:1)
Data presented at ASH 2021. CAR: Chimeric antigen receptor
25Vecabrutinib Positively Regulated CAR T-Cell Therapy
Reducing CAR-T related toxicity: dose dependent inhibition of pro-inflammatory cytokines
IL-6 IL-10 IL-1rα
JeKo-1 + CAR T cells (1:1) JeKo-1 + CAR T cells (1:1) JeKo-1 + CAR T cells (1:1)
Preclinical data presented at ASH 2021 demonstrate the potential of vecabrutinib to increase the
efficacy and safety of CAR T cell therapy, by increasing T-cell proliferation and persistence and
decreasing production of pro-inflammatory cytokines
Data presented at ASH 2021. CAR: Chimeric antigen receptor
26Recent Accomplishments and Anticipated 2022 Milestones
ANTICIPATED H2 2022
H2 2021
Preliminary Phase 1b
Initiated Phase 1b/2 trial in
efficacy data from
advanced EBV+ solid
advanced EBV+ solid
tumors
tumor trial
H1 2021 H2 2021 ANTICIPATED H2 2022
Initiated NAVAL-1, a global Presented final data from Update on NAVAL-1
pivotal clinical trial for R/R Phase 1b/2 study in R/R EBV+ cohort(s) progressing from
EBV+ lymphomas lymphoma (ASH 2021) Stage 1 to Stage 2
R/R: Relapsed/refractory
27Experienced Management Team Involved with Multiple Success in Oncology
Ivor Royston, MD Lisa Rojkjaer, MD Daniel Chevallard, CPA
President and Chief Executive Officer Chief Medical Officer Chief Operating Officer & Chief Financial Officer
Hybritech
Ayman Elguindy, PhD Cheryl Madsen Patric Nelson, MBA
Chief Scientific Officer Senior VP, Regulatory Affairs Senior VP, Business Dev. & Corporate Strategy
Biljana Nadjsombati, PharmD Shelly Vandertie Mark McCamish, MD, PhD
VP, Pharmaceutical Development VP, Finance Strategic Advisor
28Viracta Therapeutics: Investment Thesis
Addressing an unmet medical need with a novel, all-oral,
targeted therapeutic approach representing a new MOA Execution of pre-clinical studies in immuno-oncology
for the treatment of EBV-associated cancers
Delivered positive efficacy and safety data from Phase
1b/2 clinical trial in advanced EBV+ lymphoma with poor Durable IP estate with protection out to 2040
prognosis
Enrolling patients in a global pivotal study for the treatment
Strong balance sheet with projected runway into 2024 and
of R/R EBV+ lymphoma to support potential accelerated
through multiple clinical data readouts
approval
Enrolling patients in a multinational Phase 1b/2 trial in
advanced EBV+ solid tumors; evaluating the safety and Experienced management team led by a CEO with
preliminary efficacy of Nana-val alone and in combination multiple successes in oncology
with pembrolizumab
R/R: Relapsed/refractory, EBV: Epstein-Barr Virus
29Thank you
Appendix
Viracta Therapeutics, Inc. - Formation & Financing History
Acquired CHR-3996 (now First Patient Enrolled in EBV+ T-cell lymphoma ODD
Nanatinostat) from Chroma Lymphoma Phase 1b/2 EOP2 Meeting w FDA
Therapeutics in exchange for Series C Financing ($10M) Series E Financing ($40M)
equity in Viracta (for all uses in
Salubris partnership for China Announced Merger with Sunesis and $65M
all geographies)
Concurrent Financing
2015 2016 2017 2018 2019 2020 2021
Viracta Therapeutics seeded Series B Financing ($9M) Fast Track Designation granted Closed merger;
(Series A) by Latterall Venture Orphan Drug Designations (3) NASDAQ: VIRX
Partners & Forward Ventures Ph1b data presented at ASH oral Initiated EBV+ lymphoma
Issued patent for Viral Gene session pivotal study (Q2 2021)
Activation Series D Financing ($17M) Initiated EBV+ solid tumor
Ph1b/2 (Q4 2021)
32Board of Directors and Scientific Advisory Board
Board of Directors Scientific and Clinical Advisors
Roger J. Pomerantz, MD Michael Huang, MBA Douglas Faller, MD, PhD Ronald Levy, MD
Chairman of the Board Managing Partner, Taiwania Capital Scientific Founder & Chairman, Scientific Advisory Board, Professor & Director of the Lymphoma Program at
former Cancer Center Director & Vice Chairman of the Stanford University School of Medicine; member of the
President, Chief Executive Officer &
Samuel Murphy, PhD Division of Medicine, Boston University National Academy of Medicine and the National
Chairman of the Board, ContraFect
Corporation CEO, Salubris Biotherapeutics, Inc.; Robert Baiocchi, MD, PhD Academy of Sciences
VP and Head of Int’l Business Associate Professor, Associate Director for Translational
Ivor Royston, MD Pierluigi Porcu, MD
Development, Salubris & Clinical Science in the Division of Hematology, The
President and Chief Executive Officer, Director of the Hematologic Malignancies and
Pharmaceuticals Ohio State University
Viracta Hematopoietic Stem Cell Transplantation Division in
Corey Casper, MD, MPH the Department of Medical Oncology for Sidney
Jane Barlow, MD, MPH, MBA Nicole Onetto, MD Chief Medical Officer at Infectious Disease Research Kimmel Cancer Center at Thomas Jefferson University
EVP & CCO, Real Endpoints, Professional Director Institute (IDRI), Co-Director of University of
former Associate CMO, CVS Health Washington/Fred Hutch Center for AIDS Research Hao Shen, PhD
Stephen Rubino, PhD, MBA
Professor of Microbiology, University of Pennsylvania
Chief Business Officer, Celyad Charles Cobbs, MD
Flavia Borellini, PhD
Oncology SA Director of the Ivy Center for Advanced Brain Tumor Daniel Von Hoff, MD
Professional Director, former Chief Treatment, Swedish Neuroscience Institute, Seattle Physician in Chief, Distinguished Professor,
Executive Officer, Acerta Pharma Barry Simon, MD
Translational Genomics Research Institute (TGen),
Chief Corporate Affairs Officer, Carl June, MD
Professor in Immunotherapy, Pathology & Laboratory
Phoenix AZ
Tom Darcy ImmunityBio
Medicine, Director, Center for Cellular Immunotherapies, Chief Scientific Officer, US Oncology Research
Chairman of the Audit Committee
Gur Roshwalb, MD, MBA Director, Parker Institute for Cancer Immunotherapy,
Audit Partner, PricewaterhouseCoopers Lawrence Young, PhD
Managing Director, aMoon University of Pennsylvania
(Retired) Vice President & Director of the Warwick Cancer
Shannon Kenney, MD Research Centre at University of Warwick, UK
Professor of Oncology and Medicine, Wattawa Bascon
Professor in Cancer Research,Virology Program Leader,
University of Wisconsin Carbone Cancer Center
33Patients with Recurrent EBV+ Lymphomas Need More Treatment Options
Accelerated approval path available given lack of options for patients
Subtypes 1st Line SoC 2nd Line Options Limitations of Current Treatment Paradigm
TL or Salvage ChemoRx + • Outlook for refractory patients is bleak
DLBCL R-CHOP
ASCT • CAR-T for 3rd line
Peripheral T-cell CHO(E)P or BV+CHP for HDACi, BV, or Salvage • High unmet need with lack of standard of care in R/R disease
Lymphoma/AITL CD30+ ChemoRx • Clinical trial preferred for 1L and R/R disease (less responsive to CHOP)
Extranodal NK/ L-asparaginase-based Salvage ChemoRx+ ASCT, • Dismal prognosis if R/R to L-asparaginase-based Rx (mOS ~5 mos)
T cell Lymphoma (SMILE)+/- radiotherapy anti-PD1, Trial • Clinical trial preferred for R/R disease
Post-transplant Immunosuppression, Rituximab or
• Clinical trial preferred for R/R disease
Lymphoma (PTLD) rituximab, or R-CHOP R-CHOP
• No preferred therapy for R/R HL
Hodgkin BV +/- anti-PD1
ABVD • Higher treatment-related mortality in older patients
Lymphoma or ASCT
• Outcomes are uniformly poor for R/R disease
Therapy abbreviations
ABVD adriamycin, bleomycin, vinblastine, dacarbazine R-CHOP rituximab, cyclophosphamide, doxorubicin, vincristine, prednisone
ASCT autologous stem cell transplant CHOEP CHOP, etoposide
BV brentuximab vedotin SMILE dexamethasone, methotrexate, ifosfamide, L-asparaginase, etoposide
CHP cyclophosphamide, doxorubicin, prednisone TL tafasitamab, lenalidomide
ChemoRx chemotherapy
34You can also read

















































