Experimental pilot study for augmented reality enhanced elbow arthroscopy - Nature
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

www.nature.com/scientificreports
OPEN Experimental pilot study
for augmented reality‑enhanced
elbow arthroscopy
Michiro Yamamoto1*, Shintaro Oyama1, Syuto Otsuka2,3, Yukimi Murakami3,
Hideo Yokota3 & Hitoshi Hirata1
The purpose of this study was to develop and evaluate a novel elbow arthroscopy system with
superimposed bone and nerve visualization using preoperative computed tomography (CT) and
magnetic resonance imaging (MRI) data. We obtained bone and nerve segmentation data by CT and
MRI, respectively, of the elbow of a healthy human volunteer and cadaveric Japanese monkey. A life
size 3-dimensional (3D) model of human organs and frame was constructed using a stereo-lithographic
3D printer. Elbow arthroscopy was performed using the elbow of a cadaveric Japanese monkey. The
augmented reality (AR) range of error during rotation of arthroscopy was examined at 20 mm scope–
object distances. We successfully performed AR arthroscopy using the life-size 3D elbow model and
the elbow of the cadaveric Japanese monkey by making anteromedial and posterior portals. The
target registration error was 1.63 ± 0.49 mm (range 1–2.7 mm) with respect to the rotation angle of the
lens cylinder from 40° to − 40°. We attained reasonable accuracy and demonstrated the operation of
the designed system. Given the multiple applications of AR-enhanced arthroscopic visualization, it has
the potential to be a next-generation technology for arthroscopy. This technique will contribute to the
reduction of serious complications associated with elbow arthroscopy.
Abbreviations
AR Augmented reality
CT Computed tomography
MRI Magnetic resonance imaging
3D 3-Dimensional
CG Computer graphics
STL Standard triangulated language
VCAD Volume computer aided design
Available evidence supports the use of elbow arthroscopy to manage multiple conditions including rheumatoid
arthritis, osteoarthritis, tennis elbow, and osteochondritis dissents. A major drawback of elbow arthroscopy is
the risk of intraoperative complications, including serious neurovascular injuries1. The small working space and
near adjacency of neurovascular and arthroscopic portals make elbow arthroscopy a technically demanding
procedure. Successful elbow arthroscopy requires extensive knowledge of the spatial correlations among the
neurovasculature, entry portals, and joint structures.
Recent advancements in sophisticated image processing technology have made precise preoperative simu-
lations a possibility, and they are becoming increasingly common in clinical practice2. However, this valuable
set of information is ineffectively utilized in elbow arthroscopy at arguably the most decisive point: during the
procedure3. The ability to access such data that is optimized for use and seamlessly integrated into the surgi-
cal navigation system has remained elusive. We propose that the safety of standard elbow arthroscopy can be
improved by incorporating augmented reality (AR). AR can allow the delivery of selective complex and highly
useful information through computer graphics (CG) superimposed onto real-time video.
AR-assisted surgery is expanding rapidly in the field of sports, trauma, oncology, spine, and a rthroplasty4,5.
AR is an important technology because it enables the demonstration of the positional relationship between
1
Department of Hand Surgery, Nagoya University Graduate School of Medicine, 65 Tsurumai‑cho, Showa‑ku,
Nagoya 466‑8550, Japan. 2Department of Mechanical Engineering, Tokyo University of Science, Noda,
Japan. 3Image Processing Research Team, RIKEN Center for Advanced Photonics, Wako, Japan. *email: michi‑ya@
med.nagoya‑u.ac.jp
Scientific Reports | (2021) 11:4650 | https://doi.org/10.1038/s41598-021-84062-7 1
Vol.:(0123456789)
www.nature.com/scientificreports/
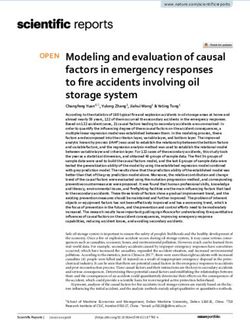
Figure 1. A real size 3-dimensional (3D) model of organs and frame. The model was constructed using a
standard triangulated language (STL) 3D printer (Object500 Connex, Stratasys Ltd, US.).
implants and targeted tissues to help complex interventions. However, AR-assisted arthroscopy has only few
reports including knee and wrist a rthroscopy6,7. Neurovascular injury is less significant with knee and wrist
arthroscopy, because important neurovascular structures do not run near the portal or in the surgical field.
Therefore, previous AR arthroscopy reports of the knee and wrist provided only superimposed bone and joint
3D data. On the other hand, all nerves around the elbow are at risk of injury during arthroscopy. Development of
a novel technology using AR for elbow arthroscopy is needed with superimposed bone and nerve visualizations
based on computed tomography (CT) and magnetic resonance imaging (MRI) data.
The purpose of this study was to develop and evaluate a novel elbow arthroscopy system that uses AR tech-
nology to superimpose nerve data on an arthroscopy monitor. We hypothesize that the accuracy of the resulting
AR enhancement to standard arthroscopy would be acceptable.
Methods
Experiment 1. Data collection, processing and 3D modeling of body organs. Skin, bone, and nerve segmen-
tation data of the elbow of a healthy human volunteer was obtained by CT and MRI. Inter-modal voxel registra-
tion was performed using ANT software with a SyN non-linear registration algorithm and affin r egistration8.
Segmentation and refinement were performed using VoTracer software (Riken, Wako, Japan, http://www.riken
.jp/brict/Ijiri/VoTracer/)9. All segmented lesion data were exported as standard triangulated language (STL)
data.
We added support frame STL data to correctly coordinate bones and nerves upon 3D printing and printed
a life-size 3D model of organs and frame using a stereo-lithographic 3D printer (Object500 Connex, Stratasys
Ltd, US.) (Fig. 1).
Setup of elbow arthroscopy and device tracking system. We used a tracking system (MicronTracker3 H3-60
model; ClaroNav, Toronto, Canada) for surgical device tracking. MicronTracker3 is an optical pose tracking
system with a unique ability to track unlimited number of tools simultaneously.
Each tracking marker used in the system was composed of black and white regions, and the system computed
target locations at the intersection of four high-contrast regions. Each of the four black and white boundary lines
independently served to pinpoint the location of targets called ‘Xpoints’.
Unlike bright spot markers, Xpoints have information on location and orientation. This additional discrimi-
nating characteristic reduces erroneous mismatches between targets on the left and right images. It also reduces
marker misidentification, as matching the characteristics of the observed targets against templates leads to
identification. As misleading bright reflection spots are more common in an operating environment compared
with Xpoints, the use of Xpoints reduces the risk of misidentification.
The markers were identified with reference to a marker template database and allowed to distinguish between
multiple different instruments. Furthermore, the database can be updated during run-time, allowing new marker
templates to be added by presenting them to the camera and assigning names to them. We placed different
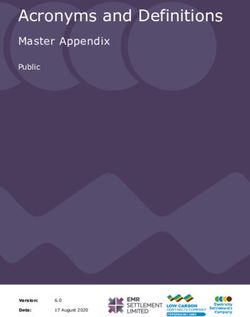
markers onto each 3D model baseplate and used the arthroscopy camera for tracking. To stabilize markers on
the arthroscopy camera, we made custom stainless-steel guides that could attach markers on the arthroscope
with a 30° angled lens (Fig. 2a).
Scientific Reports | (2021) 11:4650 | https://doi.org/10.1038/s41598-021-84062-7 2
Vol:.(1234567890)
www.nature.com/scientificreports/
Figure 2. Elbow arthroscopy and tracking device system. Red arrows indicate Xpoints (a) The Schema of
augmented reality (AR) arthroscopy system. This figure was designed by Dr. Shintaro Oyama using Adobe
Illustrator CS5 software (https://www.adobe.com/jp) (b).
Augmented reality image processing during training surgery. While performing elbow arthroscopy on the gen-
erated 3D model, an AR-calculated CG image was superimposed onto the arthroscopic video view by our AR
system.
The system summary is as follows (Fig. 2b).
1. Arthroscopy image data was captured on the computer through a digital video capture card connected to
the arthroscopy camera system.
2. The data of the 3D model base plate and the arthroscopy camera body loci were provided by MicronTracker3,
which was able to trace target information using a customized software developed using the MicronTracker
software developers’ kit. All the following transformation matrices Tij from PiO (xi , yi , zi ) to PjO (xj , yj , zj ) are
a 3 × 3 vector matrix in 3D real vector space.
Scientific Reports | (2021) 11:4650 | https://doi.org/10.1038/s41598-021-84062-7 3
Vol.:(0123456789)
www.nature.com/scientificreports/
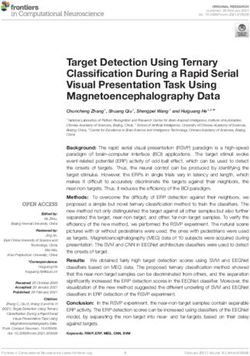
Figure 3. Reverse distortion correction using lens distortion matrix. White arrows show differences before and
after correction. Appropriate distortion of the shape on the monitor was corrected.
The coordination system of the 3D model of organs and the arthroscopy camera were defined as ƩM and ƩA.
The transformation matrix from the MicronTracker3 sensor ( Ps) to the marker reference point (fiducial point) of
ƩM:_(PM0 = ƩM (x, y, z = 0, 0, 0)) and ƩA: (PA0 = ƩA (x, y, z = 0, 0, 0)) was determined by stereo-triangulating the optical marker
TsM and TsA. The transformation matrix from PM0 to each organ STL model reference point PO was pre-defined
as TMO (although organ models include skin, radius, ulna, humerus, radial nerve, ulnar nerve, median nerve,
musculocutaneous nerve, and they were handled separately in calculation, 3D relationships between these models
were static; therefore, the reference points of these models were expressed as single points in this expression ( PO),
and PA0 to the tip of arthroscopy light rod PT was pre-defined as TAT before examination.
3. Our custom-made software installed on the computer calculated each 3D organ model and arthroscopy
light fiber rod position and direction. The position of the virtual camera was placed on the PT and rotated
according to the lens-offset angle (in this experiment, it was 30°); therefore, the coordination system of
camera sight Ʃc must consider this angle.
Calculation to transform ƩM to Ʃc is as follows:
−1
= TAT = TsA TsM
c A M
Each 3D organ model data was rendered according to this transformation. A homogenous transformation
can be constructed to register the virtual arthroscopy view to the real arthroscopy view. This calculation was
performed with the assistance of OpenCV software (Intel, US).
4. The rendered image 3 was superimposed on the image 1 and displayed on the monitor.
Correction of barrel distortion in fisheye lens. The CG position and shape were initially different due to lens dis-
tortion. However, the CG position and shape were corrected to match the arthroscopic view using lens distortion
parameters, which were estimated from the calibration p attern10. Reverse distortion correlation was performed
using a lens distortion matrix. The matrix was pre-calculated using the calibration pattern of the arthroscopy
camera (Fig. 3).
Experiment 2. Data collection, processing and 3D modeling of organs. Elbow (1/2 of upper arm ~ 1/2 of
forearm) of a Japanese monkey cadaver was used for this experiment. The X-ray CT data of the cadaveric elbow
were used with modeled frame data that could be precisely attached to the humerus and ulna on the posture at
90° elbow flexion and 90° forearm pronation. The frame was printed on a 3D printer (Davinci 1.0A / XYZ Print-
ing, Inc. US.) using acrylonitrile butadiene styrene plastic. The frame was then fixed to the cadaver elbow with
epoxy resin to ensure that it could not be easily moved (Fig. 4a).
X-ray CT and MRI of the elbow and frame were performed, and these datasets were used to obtain the bone
and nerve data using methods similar to those used in experiment 1. We obtained bone segmentation from
the CT data and nerve segmentation from the MRI data of a cadaveric Japanese monkey elbow. Segmentation
and refinement were performed using VoTracer software (Riken, Wako, Japan). All segmented lesion data were
exported as STL data (Fig. 4b).
Scientific Reports | (2021) 11:4650 | https://doi.org/10.1038/s41598-021-84062-7 4
Vol:.(1234567890)
www.nature.com/scientificreports/
Figure 4. Elbow of a Japanese monkey cadaver and Standard Triangulated Language (STL) data. We used the
elbow (1/2 of upper arm ~ 1/2 of forearm) of a Japanese monkey cadaver. From X-ray computed tomography
(CT) data of the cadaveric elbow, we modeled frame data that can be precisely attached to humerus and ulna
on the posture of 90° elbow flexion, 0° forearm pronation (a). We obtained bone segmentation from CT data
and nerves from magnetic resonance imaging (MRI) data of a cadaveric Japanese monkey elbow. Segmentation
and refinement were performed using VoTracer software (Riken, Wako, Japan) (http://www2.riken.jp/brict/
Ijiri/VoTracer). This figure was generated by Dr. Shintaro Oyama using L-Phinus V5 Ver. 5.01 software (https
://l-phinus.jp/software.html) (b).
Setup of elbow arthroscope and device tracking system. The tracking system setup was similar to experiment
1 except that we added an anti-pollution barrier to the system. A washable stainless-steel base plate was con-
structed to stabilize the elbow frame and placed at different markers on the baseplate and the arthroscopy cam-
era head. The relative position between the baseplate and elbow frame was static. The 3D model base plate and
arthroscopy camera body loci data were provided by MicronTracker3. The rendered images were superimposed
on the real-time view and displayed on the AR monitor.
Augmented reality image processing during training surgery. Elbow arthroscopy was performed on the monkey
elbow through anteromedial and posterior portals. While operating on the cadaver elbow, the AR calculated C
image was superimposed onto the arthroscopic video by the same method as described in experiment 1. Reg-
istration of the CG data positioning was adjusted manually using the shapes of the capitellum and radial head
obtained from an arthroscopic view.
Accuracy evaluation of AR position during rotation of arthroscopy. The AR range of error was examined to
evaluate the accuracy of the system. The surgeon usually uses an arthroscope with a 30° angled lens for elbow
arthroscopy and obtains the field of view by rotating the lens. We investigated the extent of target registration
errors during the rotation of the lens. By installing a marker on the lens cylinder in addition to the marker
installed on the camera head of the elbow arthroscope, the coordinate transformation matrix from the marker
installed on the camera head to the marker on the lens cylinder of the arthroscope estimates the rotation angle
around the axis. By estimating the direction of the elbow arthroscope from the estimated rotation angle, a 3D
model that follows the rotation of the lens cylinder is superimposed.
Markers were installed on the camera head and lens cylinder. The working distance was set to 20 mm to
superimpose the 3D model using an elbow arthroscope whose various parameters were estimated by camera
calibration (Fig. 5a).
A circular model with a diameter of 2 mm was used as the 3D model, and a checkerboard was used as the
object. It was designed such that the center of the circle of the circular model and the intersection of the check-
erboard overlap if there is no error in the superimposed position (Fig. 5b).
The target registration error was obtained from the superimposed display to evaluate the position accuracy.
The angle of the lens cylinder was changed by 10° within the measurable range (− 40° < θ < 40°) of MicronTracker3
(Fig. 5c).
Ethics approval and consent to participate. The study protocol was approved by the Ethics Committee
of Nagoya University Hospital (2020-0013). Informed consent was obtained from all participants in this study.
All methods in this study were performed in accordance with relevant guidelines and regulations.
Scientific Reports | (2021) 11:4650 | https://doi.org/10.1038/s41598-021-84062-7 5
Vol.:(0123456789)
www.nature.com/scientificreports/
Figure 5. Augmented reality (AR) system error calculation during arthroscopy rotation. Markers were installed
on the camera head and lens cylinder. The working distance was set to 20 mm (Fig. 5a). A circular model with
a diameter of 2 mm was used as the 3D model, and a checkerboard was used as the object (Fig. 5b). The target
registration error was obtained from the superimposed display to evaluate the position accuracy. The angle of
the lens cylinder was changed by 10° within the measurable range (-40° < θ < 40°) of MicronTracker 3 (Fig. 5c).
Figure 5a–c were designed by Syuto Otsuka using PowerPoint for Microsoft 365.
Results
Experiment 1. We successfully performed AR arthroscopy for the full-size 3D elbow model. The CG data
was superimposed onto the elbow arthroscopy video in real-time. We performed a registration to co-visualize
the image of the patient’s elbow structures and the CG made by preoperative images. After manual modification
of the position, scale, and orientation, the accuracy of the superimposed CG data was deemed acceptable on the
AR monitor.
Scientific Reports | (2021) 11:4650 | https://doi.org/10.1038/s41598-021-84062-7 6
Vol:.(1234567890)www.nature.com/scientificreports/
Figure 6. Augmented reality (AR) arthroscopy on cadaveric Japanese monkey elbow. Capitellum and
radial head were visualized through the anteromedial portal and visualized on the scope monitor (a). The
humeroradial joint and radial nerve (white arrows) were superimposed on the real view (b). The red arrow
indicates a third person view using the stereo camera on the optical tracking device.
Figure 7. The target registration error. The target registration error was 1.63 ± 0.49 mm (range, 1–2.7 mm) with
respect to the rotation angle of the lens cylinder from 40° to − 40°.
Experiment 2. AR arthroscopy of the cadaveric Japanese monkey elbow was performed (Fig. 6a). The
humeroradial joint and radial nerve were superimposed on the real-time view and displayed on the AR monitor.
Although the radial nerve was not seen on the scope monitor as it was located behind the joint capsule, the posi-
tion of the radial nerve was clearly observed. This was helpful to the surgeon in creating a lateral portal, thereby
avoiding radial nerve injury (Fig. 6b).
Accuracy evaluation of AR position during rotation of arthroscopy. The target registration error
was 1.63 ± 0.49 mm (range 1–2.7 mm) at a 20 mm scope-object distance, with respect to the rotation angle of the
lens cylinder from 40° to − 40° (Fig. 7).
Scientific Reports | (2021) 11:4650 | https://doi.org/10.1038/s41598-021-84062-7 7
Vol.:(0123456789)www.nature.com/scientificreports/
Discussion
We integrated AR technology into elbow arthroscopy. We have demonstrated that the workings of the system
and the accuracy of this AR system were deemed satisfactory. Through further iterations and refinements, AR-
enhanced arthroscopic visualization has the potential to be a transformative technology. This technique will
contribute to reducing the risk of serious complications associated with elbow arthroscopy.
The rapid development of endoscopy has enabled minimally invasive surgeries. However, this technique has
a spatial perception disadvantage. The surgeon needs to alternate between the macroscopic view of the surgical
field and the endoscopic view. AR navigation has recently been employed during brain, spinal, plastic, maxil-
lofacial, and several other highly technically demanding s urgeries11–13. However, few studies have focused on its
use in upper limb arthroscopy7. There is an unmet need for the next-generation arthroscopy system especially
designed for the elbow because of the high incidence of associated intraoperative complications.
Creating AR-enhanced navigation requires 3D preoperative imaging of the target tissue, AR display, tracking
system, and a software to calculate the arthroscopy position and direction for each 3D organ.
VoTracer is a software employed for volume computer-aided design (VCAD) of pre-operative CT and MRI
data. Segmentation and refinement of bone and nerve data can be performed using this software. A limitation
associated with all VCAD software programs is the need for manual work in creating CG of the target tissue.
Fine anatomical knowledge of the elbow, especially of the nerve route, is required to complete segmentation and
refinement of the tissues. The technology for extracting and superimposing information on large skeletons in
the hip and shoulder joints has already been established, and clinical application has advanced14,15. However, no
attempt has been made to create a 3D CG that includes information on nerves with a diameter of approximately
10 mm around the elbow joint and display it on an arthroscopy monitor. The highlight of the current study is
that elbow arthroscopic surgery, which causes many complications of nerve damage, will be transformed into
safe surgery by this technology.
There are several methods of display for AR. See-through glasses and 3D projection mapping are possible AR
displays. See-through glasses have a drawback in that it is difficult to obtain an accurate AR view superimposed
on the real view. See-through glasses need to track the pupil positions in real-time for registration. 3D projec-
tion mapping is another way to display the AR view. In order to obtain an AR view on the patient’s skin, the
video projector has to be set over the patient in the operating room. As both deep and superficial structures are
displayed on the skin surface, a significant error of perception is noted when more than two surgeons see the AR
display11. We employed a video-based display with two monitors for real and AR-enhanced views. This system
was a natural fit for arthroscopy, as the surgeon could simultaneously confirm the real and AR-enhanced view.
In this system, the surgeon can select to watch the real view or AR-enhanced view depending on the situation.
However, in another AR study, fewer gaze shifts reduced task completion time and e rrors16. In the near future,
it is necessary to develop a system that suppresses the gaze shifts of surgeons using fewer monitors with higher
precision AR using real-time data.
A variety of tracking systems are available for clinical settings, such as infrared camera-based tracking, the
tag video tracking, and electromagnetic tracking12,17,18. The accuracy of the tracking device is very important
in the clinic as it is directly linked to safety. We used an optical tracking device, MicronTracker3. It was able to
trace each target information in real-time using a customized software developers’ kit. The accuracy of this track-
ing system was deemed acceptable, and the position error was 1.63 ± 0.49 mm (range 1 to 2.7 mm) at a 20 mm
scope-object distance, while rotation of the arthroscopy was 40° to − 40°. The error when the rotation angle of
the lens cylinder is 0° represents the cumulative error other than the rotation angle estimation error, such as
the parameter estimation that occurs during camera calibration and the estimation of positional orientation
by MicronTracker3. Whether this accuracy is sufficient for clinical application needs to be confirmed in future
clinical studies after further ensuring safety.
Arthroscopy simulator training improves the performance of students and residents during knee and shoul-
der surgery19–23. Recently, multiple types of virtual reality-based training simulators for arthroscopy have been
reported22. Among these simulators, high-fidelity virtual reality simulation was reported to be superior to the
low-fidelity model to acquire arthroscopic skills23. An AR-enhanced arthroscopic system with superimposed tasks
can be a high-fidelity training tool for surgical education. This system can also provide a third-person view using
the stereo camera on the optical tracking device, MicronTracker3. The third-person view and record of track-
ing makers provide a trainee feedback regarding the handling of scope and other instruments during surgery.
AR-enhanced navigation for arthroscopy may become the next generation arthroscopy system. However,
this study has some limitations. First, we used preoperative imaging techniques, such as CT and MRI, but not
real-time information of the target tissue. The size and location of the lesion at the time of surgery may differ
from the preoperative data. Second, the elbow flexion angle was fixed in our experiments; however, surgeons in a
clinical setting typically move the elbow during arthroscopy. Superimposed CG data, therefore, needs to change
according to the elbow angle. AR with real-time data of the target tissue is required to solve these problems.
Intraoperative CT, MRI, or ultrasonography may be employed to obtain intraoperative data of the target tissue.
Actually, nerves around the elbow can be clearly visualized using u ltrasonography24,25. In addition, an algorithm
for intraoperative data is required.
Conclusions
The technological integration of AR with arthroscopy was successful. We attained satisfactory accuracy and
demonstrated the working of such a system. Upon resolution of some limitations, AR-enhanced arthroscopic
visualization has the potential to become the next-generation arthroscopy. Elbow arthroscopy requires signifi-
cant training for surgeons, and even skilled surgeons have reported complications during surgery. We believe
that AR-enhanced arthroscopy will reduce the risk of serious complications associated with elbow arthroscopy.
Scientific Reports | (2021) 11:4650 | https://doi.org/10.1038/s41598-021-84062-7 8
Vol:.(1234567890)www.nature.com/scientificreports/
Data availability
The datasets during the current study are available from the corresponding author on reasonable request.
Received: 17 October 2020; Accepted: 11 February 2021
References
1. Desai, M. J. et al. Major peripheral nerve injuries after elbow arthroscopy. Arthroscopy 32(6), 999-1002.e8 (2016).
2. Yamamoto, M., Murakami, Y., Iwatsuki, K., Kurimoto, S. & Hirata, H. Feasibility of four-dimensional preoperative simulation for
elbow debridement arthroplasty. BMC Musculoskelet. Disord. 17, 144 (2016).
3. Miyake, J. et al. Arthroscopic debridement in the treatment of patients with osteoarthritis of the elbow, based on computer simula-
tion. Bone Joint J. 96B(2), 237–41 (2014).
4. Laverdière, C. et al. Augmented reality in orthopaedics: a systematic review and a window on future possibilities. Bone Joint J.
101B(12), 1479–88. https://doi.org/10.1302/0301-620X.101B12.BJJ-2019-0315.R1 (2019).
5. Jud, L. et al. Applicability of augmented reality in orthopedic surgery: a systematic review. BMC Musculoskelet. Disord. 21(1), 103.
https://doi.org/10.1186/s12891-020-3110-2 (2020).
6. Dario, P. et al. A novel mechatronic tool for computer-assisted arthroscopy. IEEE Trans. Inf. Technol. Biomed. 4(1), 15–29. https
://doi.org/10.1109/4233.826855 (2000).
7. Zemirline, A. et al. Augmented reality-based navigation system for wrist arthroscopy: feasibility. J. Wrist Surg. 2(4), 294–298 (2013).
8. Avants, B. B., Tustison, N. & Song, G. Advanced normalization tools (ANTS). Insight J. 2, 1–35 (2009).
9. Ijiri T, & Yokota H. Contour‐based interface for refining volume segmentation. Computer Graphics Forum. Paper presented at:
Computer Graphics Forum 2010;29(7):2153–60.
10. Melo, R., Barreto, J. P. & Falcão, G. A new solution for camera calibration and real-time image distortion correction in medical
endoscopy–initial technical evaluation. IEEE Trans. Bio. Med. Eng. 59(3), 634–644 (2012).
11. Kersten-Oertel, M. et al. Augmented reality in neurovascular surgery: feasibility and first uses in the operating room. Int. J. Comput.
Assist. Radiol. Surg. 10(11), 1823–1836 (2015).
12. Nicolau, S., Soler, L., Mutter, D. & Marescaux, J. Augmented reality in laparoscopic surgical oncology. Surg. Oncol. 20(3), 189–201
(2011).
13. Shuhaiber, J. H. Augmented reality in surgery. Arch. Surg. 139(2), 170–174 (2004).
14. Ponce, B. A., Menendez, M. E., Oladeji, L. O., Fryberger, C. T. & Dantuluri, P. K. Emerging technology in surgical education: com-
bining real-time augmented reality and wearable computing devices. Orthopedics 37(11), 751–757. https://doi.org/10.3928/01477
447-20141023-05 (2014).
15. Ogawa, H., Hasegawa, S., Tsukada, S. & Matsubara, M. A pilot study of augmented reality technology applied to the acetabular
cup placement during total hip arthroplasty. J. Arthroplast. 33(6), 1833–1837. https://doi.org/10.1016/j.arth.2018.01.067 (2018).
16. Polvi, J. et al. Handheld Guides in inspection tasks: augmented reality versus picture. IEEE Trans. Vis. Comput. Graph. 24(7),
2118–2128. https://doi.org/10.1109/TVCG.2017.2709746 (2018).
17. Pagador, J. B. et al. Augmented reality haptic (ARH): an approach of electromagnetic tracking in minimally invasive surgery. Int.
J. Comput. Assist. Radiol. Surg. 6(2), 257–263 (2011).
18. Teber, D. et al. Augmented reality: a new tool to improve surgical accuracy during laparoscopic partial nephrectomy? Preliminary
in vitro and in vivo results. Eur. Urol. 56(2), 332–338 (2009).
19. Aïm, F., Lonjon, G., Hannouche, D. & Nizard, R. Effectiveness of virtual reality training in orthopaedic surgery. Arthroscopy 32(1),
224–232 (2016).
20. Cannon, W. D. et al. Improving residency training in arthroscopic knee surgery with use of a virtual-reality simulator. A rand-
omized blinded study. J. Bone Joint Surg. Am. 96(21), 1798–806 (2014).
21. Rebolledo, B. J., Hammann-Scala, J., Leali, A. & Ranawat, A. S. Arthroscopy skills development with a surgical simulator: a com-
parative study in orthopaedic surgery residents. Am. J. Sports Med. 43(6), 1526–1529 (2015).
22. Vaughan, N., Dubey, V. N., Wainwright, T. W. & Middleton, R. G. A review of virtual reality based training simulators for ortho-
paedic surgery. Med. Eng. Phys. 38(2), 59–71 (2016).
23. Banaszek, D. et al. Virtual reality compared with bench-top simulation in the Acquisition of arthroscopic skill: a randomized
controlled trial. J. Bone Jt. Surg. Am. 99(7), e34 (2017).
24. McCartney, C. J., Xu, D., Constantinescu, C., Abbas, S. & Chan, V. W. Ultrasound examination of peripheral nerves in the forearm.
Reg. Anesth. Pain Med 32(5), 434–439 (2007).
25. Heinemeyer, O. & Reimers, C. D. Ultrasound of radial, ulnar, median, and sciatic nerves in healthy subjects and patients with
hereditary motor and sensory neuropathies. Ultrasound Med. Biol. 25(3), 481–485 (1999).
Author contributions
M.Y., S.O., and H.Y. have full access to all of the data in the study and take responsibility for the integrity of the
data and the accuracy of the data analysis. Study concept and design: M.Y. and H.Y. Acquisition of data: M.Y.,
S.O., S.O., and Y.M. Analysis and interpretation of data: M.Y. and H.H. Drafting of the manuscript: M.Y. and
S.O. Critical revision of the manuscript for important intellectual content: M.Y. and H.H. Administrative, techni-
cal, or material support: S.O., Y.M. and H.Y. Study supervision: M.Y., H.H., and H.Y. All authors have read and
approved the final submitted manuscript.
Funding
Research reported in this publication was supported by the Japan Society for the Promotion of Science under
Award # 26462262 of the Grant-in-Aid for Scientific Research. The contents of this manuscript are the sole
responsibility of the authors and do not represent the official views of the Japan Society for the Promotion of
Science.
Competing interests
The authors declare no competing interests.
Additional information
Correspondence and requests for materials should be addressed to M.Y.
Reprints and permissions information is available at www.nature.com/reprints.
Scientific Reports | (2021) 11:4650 | https://doi.org/10.1038/s41598-021-84062-7 9
Vol.:(0123456789)www.nature.com/scientificreports/
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and
institutional affiliations.
Open Access This article is licensed under a Creative Commons Attribution 4.0 International
License, which permits use, sharing, adaptation, distribution and reproduction in any medium or
format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the
Creative Commons licence, and indicate if changes were made. The images or other third party material in this
article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the
material. If material is not included in the article’s Creative Commons licence and your intended use is not
permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from
the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
© The Author(s) 2021
Scientific Reports | (2021) 11:4650 | https://doi.org/10.1038/s41598-021-84062-7 10
Vol:.(1234567890)You can also read