Exertional angina pectoris associated with post-exercise ST segment elevation and nearly normal coronary arteries1
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Case Reports
Exertional angina pectoris associated with
post-exercise ST segment elevation and
nearly normal coronary arteries 1
H. David Millit, M.D.
Rajesh Gaglani, M.D. 2
James P. Antalis, M.D. 3
The authors describe a patient with effort-induced discomfort and occasional palpitations. O n e a c h occasion,
angina pectoris and nearly normal coronary arteries the chest discomfort was precipitated by e x e r t i o n a n d re-
who had ST segment elevation after stress ECG in the lieved within ten minutes by rest. T h e patient d e n i e d any
postexercise recovery period. The patient experienced episodes o f nonexertional chest d i s c o m f o r t , a n d his only
angina only during exercise. Exercise-induced ST seg- o t h e r complaint was intermittent heart p o u n d i n g , or skip-
ment elevation, although uncommon, may be second- ping. Results o f physical e x a m i n a t i o n w e r e essentially nor-
ary to a variety of causes. Selective coronary angiog- mal. B l o o d pressure was 1 2 0 / 8 0 m m H g ; pulse was 7 0
raphy is often indicated for the diagnosis and appro- b e a t / m i n a n d regular. T h e r e was n o j u g u l a r v e n o u s disten-
priate management of the patient. sion, and carotid upstroke was normal. L u n g s w e r e clear.
Cardiac examination revealed normal heart t o n e s a n d an
Index terms: Angina pectoris • Coronary vessels apical S 4 . T h e r e m a i n d e r o f t h e e x a m i n a t i o n was unremark-
• Electrocardiography able. A H o l t e r m o n i t o r d o c u m e n t e d sinus r h y t h m (SR) with
periods o f symptomatic ventricular bigeminy; n o chest dis-
Cleve Clin Q 51:71-75, Spring 1984
c o m f o r t or repolarization changes w e r e n o t e d d u r i n g the
m o n i t o r period. A resting ECG was normal.
T h e patient's symptomatic r h y t h m disturbance was con-
T h e traditional value of stress electrocardiog- trolled with disopyramide p h o s p h a t e (Norpace), a n d h e was
raphy in the evaluation of chest pain has been given nitroglycerin f o r use as necessary. His activities w e r e
the documentation of exercise-induced S T seg- limited until cardiac w o r k u p c o u l d b e c o m p l e t e d , a n d h e
r e m a i n e d f r e e of pain until stress testing. A t that time, h e
ment depression. Recently, there has been re- u n d e r w e n t a g r a d e d treadmill e x e r c i s e test using t h e N a u g h -
newed interest in S T segment elevation at rest, ton protocol. T w e l v e - l e a d ECGs w e r e r e c o r d e d e v e r y min-
with exercise, and in the postexercise period. We ute with c o n t i n u o u s m o n i t o r i n g o f lead V 5 . T h e patient
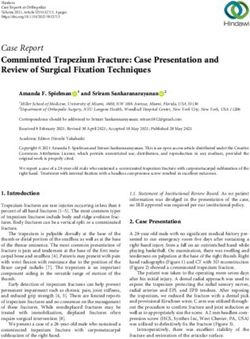
wish to describe a patient with only effort-in- exercised for 12 minutes to a heart rate o f 1 6 4 b e a t / m i n
duced angina pectoris and nearly normal coro- without chest discomfort or abnormal E C G r e s p o n s e (Fig.
1), with termination o f t h e test b e c a u s e o f dyspnea. Occa-
nary arteries who exhibited S T segment elevation sional premature ventricular contractions (PVCs) w e r e
after stress ECG in the postexercise period. n o t e d at rest, which did n o t increase in f r e q u e n c y with
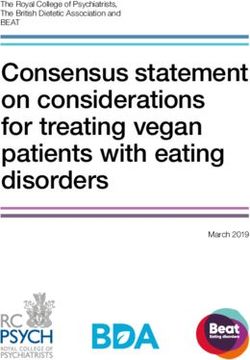
exercise. A t o n e m i n u t e into the r e c o v e r y period, while
Case report supine, t h e patient e x h i b i t e d S T s e g m e n t elevation, a n d by
A 38-year-old white man p r e s e n t e d to W h e e l i n g Hospital, two minutes h e c o m p l a i n e d o f his typical "chest pain." Fur-
W h e e l i n g , West Virginia, with a two-year history o f chest ther S T s e g m e n t elevation to a m a x i m u m o f 9 m m had
occurred by three minutes into the r e c o v e r y period, with
an injury current n o t e d in leads II, III, aV F , V 5 , a n d VK (Fig.
' Cardiology Specialists, Ltd. (H.D.M.), Professional Center, Medi-
2). H e was given nitroglycerin for what was t h o u g h t to b e
cal Park, Wheeling, WV 26003. Submitted for publication April
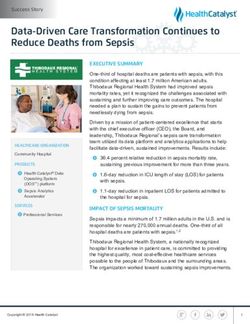
1983; accepted July 1983. exercise-induced coronary artery spasm, with c o m p l e t e res-
2
Dr. Gaglani is a Cardiology Fellow at Mount Carmel Medical olution o f t h e chest d i s c o m f o r t a n d ECG c h a n g e s o v e r the
Center, Columbus, OH. n e x t 15 minutes (Fig. 3). T h e patient was hospitalized in
3
Dr. Antalis is a family practitioner in Shadyside, OH. view o f the acute ECG changes, but n o e v i d e n c e o f myocar-
71
Downloaded from www.ccjm.org on March 7, 2022. For personal use only. All other uses require permission.72 Cleveland Clinic Quarterly Vol. 51, No. 1
I A VR V 1 VA
— .1
II '•AfL rtJ
A VL
\ » V; 5
v/ — •v —
j" A
- /
A J: /A A —
[II
AVF Y:Î V6
-1 A S —-I V iv
1A
AV R V1 V4
I
f vwr - v r W« f V -
\ mm,mi \ \
! /*>Spring 1984 Exertional angina pectoris 73
I Wfi <
V1 V4
•
f~J r-/
•wt *
/ - J
X \ \
"T)
T 1 /
I1
f;
\VL |
A
U
v:2 \fi
/ K «cjL rf »
A
V»
f
r / V J i /
\
f
J- N
III
^ VF i 1
/€
À j •j74 Cleveland Clinic Quarterly Vol. 51, No. 1
AVR V1 V 4
il A VL V2 V 5
- u - y u - A i i A ^ '
in A VF V3 V 6
Fig. 3. Electrocardiogram taken at 15 minutes of recovery after patient had received sublingual nitroglycerine. T r a c i n g has
returned to normal.
o c c u r r i n g d u r i n g exercise a n d suggested that in s e g m e n t elevation o c c u r r i n g a f t e r exercise, b u t
a d d i t i o n to c o r o n a r y a r t e r y spasm, S T s e g m e n t those cases r e p r e s e n t severe c o r o n a r y atheroscle-
elevation may be secondary to a n t e r i o r myocar- rosis with i m m i n e n t myocardial infarction o r
dial i n f a r c t i o n , critical p r o x i m a l left a n t e r i o r de- death.
s c e n d i n g c o r o n a r y a r t e r y o b s t r u c t i o n , a n d left T h e p r o g n o s t i c implication of exercise-in-
v e n t r i c u l a r apical a n e u r y s m . S T s e g m e n t eleva- d u c e d S T s e g m e n t elevation is n o t entirely clear.
tion o c c u r r i n g only d u r i n g t h e postexercise Lahiri et al s d e s c r i b e d 5 patients with a n g i n a w h o
p e r i o d has most o f t e n been seen in p a t i e n t s with e x h i b i t e d S T s e g m e n t depression d u r i n g t r e a d -
s o m e history of rest pain, which leads o n e to mill exercise testing followed by S T s e g m e n t
suspect u n d e r l y i n g c o r o n a r y a r t e r y spasm. Wei- elevation a n d chest pain in t h e postexercise pe-
n e r et al IL ' h a v e d o c u m e n t e d postexercise S T riod. T h r e e of these 5 patients e x p e r i e n c e d myo-
s e g m e n t elevation in 4 patients, 3 d e s c r i b i n g rest cardial infarction within eight weeks of t h e ex-
pain a n d 2 with fixed c o r o n a r y a r t e r y obstruc- ercise test, a n d 2 died. AU 5 patients d e m o n -
tion. His s e c o n d p a t i e n t was similar to ours, b o t h strated significant c o r o n a r y atherosclerosis. In
a d m i t t i n g to e x e r t i o n a l chest d i s c o m f o r t only a n d a n o t h e r study 1 0 of 8 2 patients with variant an-
b o t h w i t h o u t significant fixed c o r o n a r y a r t e r y gina, 2 5 h a d S T s e g m e n t elevation d u r i n g exer-
o b s t r u c t i o n s . T h e case described by M c L a u g h l i n cise, a n d 3 of these sustained myocardial infarc-
et a l ' 3 (chest pain a f t e r e x e r t i o n ) a g r e e d m o r e tions within t h r e e m o n t h s of t h e exercise test.
closely with t h e t e m p o r a l relation of S T s e g m e n t T w o of t h e 3 h a d severe c o r o n a r y atherosclerosis,
elevation o c c u r r i n g a f t e r an exercise test, coro- a n d b o t h died suddenly. C i p r i a n o et al' :> o b s e r v e d
n a r y a r t e r i o g r a p h y in that case revealing n o r m a l a g r o u p of 2 5 patients f o r a m e a n of 2.7 years
c o r o n a r y a r t e r i e s wth spasm i n d u c e d by e r g o n o v - a f t e r d o c u m e n t e d c o r o n a r y a r t e r y spasm. A m o r e
ine maleate. O t h e r s 4 , " have also d o c u m e n t e d S T serious prognosis was associated with significant
Downloaded from www.ccjm.org on March 7, 2022. For personal use only. All other uses require permission.Spring 1984 Exertional angina pectoris 75
fixed coronary artery narrowing than with nor- 6. Chahine RA, Raizner AE, Ishimori T. T h e clinical significance
of exercise-induced ST-segment elevation. Circulation 1976;
mal or nearly normal coronary arteries.
54:209-213.
Coronary artery spasm may be implicated in 7. Specchia G, De Servi S, Falcone C, et al. Coronary arterial
almost all of the different clinical manifestations spasm as a cause of exercise-induced ST-segment elevation in
of myocardial ischemia, may or may not be asso- patients with variant angina. Circulation 1979; 59:948-954.
ciated with fixed coronary artery obstruction, 8. Lahiri A, Subramanian B, Millar-Craig M, Crawley J, Raftery
and may lead to ST segment elevation either in EB. Exercise-induced S-T segment elevation in variant angina.
Am J Cardiol 1980; 4 5 : 8 8 7 - 8 9 4 .
the exercise or postexercise period. Every effort 9. Sriwattanakomen S, Ticzon AR, Zubritzky SA, et al. S-T
should be made to define the underlying mech- segment elevation during exercise: electrocardiographic and
anism of the anginal syndrome in a given individ- arteriographic correlation in 38 patients. Am J Cardiol 1980;
ual, since this may help to determine proper 45:762-768.
therapy. Worsening of angina pectoris associated 10. Waters DD, SzlachcicJ, Bourassa MG, Scholl J-M, Théroux
P. Exercise testing in patients with variant angina: results,
with high doses of beta blocker may even suggest correlation with clinical and angiographic features and prog-
coronary artery spasm. 16 Apart from exercise nostic significance. Circulation 1982; 6 5 : 2 6 5 - 2 7 4 .
testing, a 24-hour recording of ambulatory ECGs 11. Bruce RA, Gey GO, Cooper MN, Fisher LD, Peterson DR.
demonstrating ST segment elevation may be use- Seattle heart watch: initial clinical, circulatory and electrocar-
ful in the detection of coronary artery spasm. diographic responses to maximal exercise. Am J Cardiol 1974;
33:459-469.
More recently, transtelephonic monitoring has
12. Weiner DA, Schick EC, Hood WB, Ryan TJ. ST-segment
been suggested for the patient with extremely elevation during recovery from exercise. A new manifestation
infrequent episodes of resting angina pectoris. of Prinzmetal's variant angina. Chest 1978; 74:133-138.
Finally, coronary arteriography with interven- 13. McLaughlin PR, Doherty PW, Martin RP, Goris ML, Harri-
tions such as ergonovine maleate 18 or cold pressor son DC. Myocardial imaging in a patient with reproducible
testing 19 may have to be included in the investi- variant angina. Am J Cardiol 1977; 3 9 : 1 2 6 - 1 2 9 .
14. Sweet RL, Sheffield LT. Myocardial infarction after exercise-
gation of the anginal syndrome to define the true induced electrocardiographic changes in a patient with variant
physiologic mechanism. angina pectoris. Am J Cardiol 1974; 3 3 : 8 1 3 - 8 1 7 .
15. Cipriano PR, Koch FH, Rosenthal SJ, Schroeder JS. Clinical
References course of patients following the demonstration of coronary
1. Prinzmetal M, Kennamer R, Merliss R, Wada T, Naci B. artery spasm by angiography. Am Heart J 1981; 101:127-
Angina pectoris. I. A variant form of angina pectoris. Am J 134.
Med 1959; 27:375-388. 16. Robertson RM, Wood AJJ, Vaughn WK, Robertson D. Ex-
2. Oliva PB, Potts DE, Pluss RG. Coronary arterial spasm in acerbation of vasotonic angina pectoris by propranolol. Cir-
Prinzmetal angina. Documentation by coronary arteriog- culation 1982; 65:281-285.
raphy. New Engl J Med 1973; 288:745-751. 17. Ginsburg R, Lamb IH, Schroeder JS, Harrison DC. Long-
3. Fortuin NJ, Friesinger GC. Exercise-induced S-T segment term transtelephonic electrocardiographic monitoring in the
elevation. Clinical, electrocardiographic and arteriographic detection and evaluation of variant angina. Am Heart J 1981;
studies in twelve patients. Am J Med 1970; 49:459-464. 102:196-201.
4. Kemp GL. Value of treadmill stress testing in variant angina 18. Heupler FA, Proudfit WL, Razavi M, Shirey EK, Greenstreet
pectoris. Am J Cardiol 1972; 30:781-783. R, Sheldon WC. Ergonovine maleate provocative test for
5. DetryJ-MR, Mengeot P, Rousseau MF, CosynsJ, Ponlot R, coronary arterial spasm. Am J Cardiol 1978; 4 1 : 6 3 1 - 6 4 0 .
Brasseur LA. Maximal exercise testing in patients with spon- 19. Raizner AE, Chahine RA, Ishimori T , et al. Provocation of
taneous angina pectoris associated with transient ST segment coronary artery spasm by the cold pressor test. Hemodynamic,
elevation. Risks and electrocardiographic findings. Br Heart arteriographic and quantitative angiographic observations.
J 1975; 37:897-903. Circulation 1980; 62:925-932.
Downloaded from www.ccjm.org on March 7, 2022. For personal use only. All other uses require permission.You can also read