Evidence-Based Recommendations and Best Practices for Promoting Healthy Eating Behaviors in Children 2 to 8 Years
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Evidence-Based Recommendations and Best Practices for Promoting Healthy Eating Behaviors in Children 2 to 8 Years Technical Report | October 2021 Healthy Eating Research A National Program of the Robert Wood Johnson Foundation

Healthy Eating Research Evidence-Based Recommendations and Best Practices for Promoting Healthy Eating Behaviors in Children 2 to 8 Years Technical Report | October 2021

Expert Panel Members
Jennifer Fisher, PhD, MA, Panel Co-Chair Lori A. Francis, PhD
Professor, Department of Social and Behavioral Sciences Associate Professor, Department of Biobehavioral Health
Associate Director, Center for Obesity Research and Education Penn State University
Temple University State College, Pennsylvania
Philadelphia, Pennsylvania
Maureen M. Black, PhD
Julie Lumeng, MD, Panel Co-Chair Professor, Department of Pediatrics
Professor of Pediatrics, Medical School University of Maryland School of Medicine
Professor of Nutritional Sciences, School of Public Health Baltimore, MD
University of Michigan Distinguished Fellow
Ann Arbor, Michigan RTI International
Research Triangle Park, North Carolina
Alison Tovar, PhD, MPH
Associate Professor, Department of Nutrition & Food Sciences Monica L. Baskin, PhD
University of Rhode Island Professor, Division of Preventive Medicine
South Kingston, Rhode Island University of Alabama at Birmingham School of Medicine
Adjunct Associate Professor of Behavioral and Social Sciences, Birmingham, Alabama
School of Public Health Brown University
Rafael Pérez-Escamilla, PhD
Providence, Rhode Island
Professor of Public Health, Social and Behavioral Sciences
Jason A. Mendoza, MD, MPH Principal Investigator, Yale-Griffin CDC Prevention Research
Professor of Public Health Sciences, Fred Hutchinson Cancer Center (PRC)
Research Center Director, Office of Public Health Practice
Professor of Pediatrics, University of Washington School of Director, Global Health Concentration
Medicine Director, Maternal Child Health Promotion Program
Investigator, Seattle Children’s Research Institute Yale School of Public Health
Seattle, Washington New Haven, Connecticut
Jerica Berge, PhD, MPH, LMFT Sarah Bowen, PhD, MS
Professor and Vice Chair, Department of Family Medicine and Professor, Department of Sociology and Anthropology
Community Health North Carolina State University
University of Minnesota Medical School Raleigh, North Carolina
Minneapolis, Minnesota
Sheryl O. Hughes, PhD
Kirsten K. Davison, PhD Associate Professor, Pediatrics-Nutrition
Donahue and DiFelice Endowed Chair USDA/ARS Children’s Nutrition Research Center
Associate Dean for Research Baylor College of Medicine
Boston College School of Social Work Houston, Texas
Chestnut Hill, Massachusetts
Stephanie Anzman-Frasca, PhD
Kyung Rhee, MD, MSc, MA Associate Professor of Pediatrics
Professor of Pediatrics, Vice Chair of Equity, Diversity, University at Buffalo
and Inclusion Buffalo, New York
Chief, Division of Child and Community Health
Susan L. Johnson, PhD
Medical Director, Medical Behavioral Unit, Rady Children’s
Section of Nutrition, Department of Pediatrics
Hospital of San Diego, Department of Pediatrics
University of Colorado Denver, Anschutz Medical Campus
University of California, San Diego
Aurora, CO
San Diego, California
2 October 2021 | Technical Report
Panel Conveners Suggested Citation
Mary Story, PhD, RD Fisher J, Lumeng J, Miller L, Smethers A, Lott M. Evidence-
Director, Healthy Eating Research Based Recommendations and Best Practices for Promoting
Professor, Global Health and Community and Family Medicine Healthy Eating Behaviors in Children 2 to 8 Years.
Associate Director of Education and Training Durham, NC: Healthy Eating Research; 2021. Available at:
Duke Global Health Institute https://healthyeatingresearch.org.
Duke University
Durham, North Carolina
Megan Lott, MPH, RD Acknowledgements
Deputy Director, Healthy Eating Research
Duke Global Health Institute The expert panel was supported by Healthy Eating Research
Duke University (HER), a national program of the Robert Wood Johnson
Durham, North Carolina Foundation. HER and the authors thank the expert panel
members for their engagement and contributions throughout
the development of the recommendations. Mary Story,
Panel Support PhD, RD (Director, HER) provided guidance and counsel
throughout the process, as well as editorial input and review.
Alissa Smethers, PhD, RD, LDN
Lauren Dawson, MPH (Communications and Program
Postdoctoral Fellow, Monell Chemical Senses Center
Associate, HER) and Emily Callahan, MPH, RDN (EAC
Philadelphia, Pennsylvania
Health & Nutrition, LLC) provided editorial input and review
Lindsey Miller, MPH of the technical report and executive summary. We would
Research Analyst, Healthy Eating Research also like to thank Jamie Bussel, MPH (Robert Wood Johnson
Duke Global Health Institute Foundation) for her guidance and counsel throughout the
Duke University expert panel process.
Durham, North Carolina
Lexi Wang
Graduate Student Worker, Healthy Eating Research
Duke Global Health Institute
Duke University
Durham, North Carolina
Evidence-Based Recommendations and Best Practices for
| October 2021 3
Promoting Healthy Eating Behaviors in Children 2 to 8 Years
Table of Contents
Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6
Purpose and Aim . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6
Rationale and Conceptual Frameworks and Models . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 7
Building on the Foundations of Responsive Approaches to Feeding Infants and Toddlers . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 7
Conceptual Model and Frameworks Informing the Expert Panel’s Approach . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 7
Background: The Typical Development of 2- to 8-Year-Olds . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 10
Growth Across Domains of Development from Ages 2 to 8 Years . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 10
Dietary Patterns of Children Ages 2 to 8 Years . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 12
Development of Food Acceptance during Childhood . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 15
Development of Healthy Appetites and Growth during Childhood . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 16
Methodology . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 18
Expert Panel Methodology . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 18
Literature Review Methodology . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 18
Development of Recommendations . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 18
Key Considerations for Reviewing the Evidence and Developing Recommendations . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 19
Narrative Review of the Evidence . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 20
Parenting Styles, Feeding Styles, and Food Parenting Practices . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 20
Fathers, Other Caregivers, and the Family System . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 21
Promoting Food Acceptance . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 22
Promoting Healthy Appetites and Growth . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 24
Evidence-Based Recommendations . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 27
Recommendations for Promoting Acceptance of Healthful Foods . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 28
Recommendations for Promoting Healthy Appetites and Growth . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 29
Implementation Considerations . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 30
Family Economics . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 31
Early Care and Education Programs . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 31
National School Meal Programs . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 32
Health Care System . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 33
Food and Nutrition Assistance Programs . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 34
Food and Beverage Marketing Targeting Children . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 34
Priorities for Future Research . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 35
Research Needs on the Development of Food Acceptance during Childhood . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 35
Research Needs on the Development of Healthy Appetites and Growth during Childhood . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 35
Conclusion . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 37
Appendices . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 38
References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 49
4 October 2021 | Technical Report
Definitions
Appetite:1 Appetite is defined as an instinctive or natural desire in the early eating environment shapes subsequent food
to eat and is described by hunger, satiation, and satiety. Hunger acceptance development.
refers to biological cues and underlying processes that lead to the
initiation of eating, whereas satiation refers to cues and processes Food neophobia:6 A tendency to avoid or refuse new or
that bring an eating episode to an end, and satiety refers to cues unfamiliar foods. Food neophobia is a developmentally
and processes that inhibit further eating until hunger returns. appropriate reaction for young children that generally resolves
with repeated exposure.
Caregiver:2 A person who provides direct care to a child with
activities of daily living. Caregivers (e.g., parents, grandparents, Food parenting practices:7 The intentional (i.e., goal-
guardians, childcare providers) have the capacity to influence the oriented) or unintentional behaviors and actions performed
development of healthy eating behaviors among children 2 to 8 by a parent that influences their child’s behaviors and actions.
years by shaping the physical and social environments in which Food parenting practices are thought to reflect three higher
eating occurs, by serving as social role models that children learn order dimensions:
to emulate, and by using food parenting practices to guide and
■ Structure:7 The organization of children’s environments to
socialize children’s experiences related to eating.
facilitate children’s competence to engage in healthy behaviors
Feeding styles:3 Feeding styles represent the application of and avoid unhealthy behaviors, such as creating meal- and
parenting styles to feeding practices and are defined as the broad snack-time routines for a child, and providing consistency in
approach used by caregivers during eating episodes, including the atmosphere and the amounts and types of foods available.
the emotional climate. Like parenting styles, feeding styles are
■ Autonomy support:7 Supporting the child’s developing
characterized in terms of demandingness and responsiveness.
psychological autonomy (e.g., giving choices) and
Demandingness refers to how much the parent encourages
independence by supporting of the child’s self-feeding
or controls eating, and responsiveness refers to how parents
skills, engagement with food, choice and preferences, and
respond to the child’s cues and needs to encourage eating and
nutritional knowledge.
support children’s developing autonomy.
■ Coercive control:7 Parents’ pressure, intrusiveness, and
■ Authoritative:4 Authoritative parenting styles provide
dominance in relation to children’s feelings, thoughts,
reasonable expectations for their child, set limits, foster child
and behaviors.
autonomy, respect the child’s opinion, provide warmth,
and exhibit both high responsiveness/warmth and high Healthy growth:8 Physical growth rates vary by age and with
demandingness/control. Authoritative feeding styles actively changes in children’s energy and nutrient needs. Growth
encourage child eating using non-directive behaviors and are is assessed by comparing a child’s weight and/or height to
responsive to the child’s eating cues and needs for autonomy. established norms. The Centers for Disease Control and
Prevention provide age- and sex-specific growth charts for
■ Authoritarian:4 Authoritarian parenting styles employ
evaluating growth of children aged 2 to 8 years and include
power-assertive behaviors with their child and are generally
indices of weight-for-age, stature-for-age, and body mass index-
unresponsive to the child’s needs. Authoritarian feeding
for-age. Healthy patterns of growth show a consistent trajectory
styles use highly directive behaviors to influence eating in an
over time. Any major shifts in growth patterns indicate the need
unsupportive way and are not responsive to the child’s eating
for further assessment.
cues and needs for autonomy.
Parenting styles:7 A constellation of parental attitudes and
■ Indulgent:4 Indulgent parenting styles display warmth and
beliefs toward child rearing, which create an emotional climate
acceptance, but lack the necessary monitoring behaviors
through which parental practices are expressed, including
needed for children’s developing autonomy. Indulgent
the quality of parent-child interactions. Parenting styles
feeding styles make few demands on the child to eat, but are
reflect the intersection of two independent dimensions—
responsive to the child’s eating cues and needs for autonomy.
demandingness (i.e., expectations for self-control, limit
■ Uninvolved:4 Uninvolved parenting styles are not appreciably setting) and responsiveness (i.e., sensitivity or nurturing).
interactive and make few demands on children. Uninvolved There are four types of parenting styles: (1) authoritative (high
feeding styles make few demands on the child to eat and demandingness, high responsiveness); (2) authoritarian (high
are not responsive to children’s eating cues and needs demandingness, low responsiveness); (3) indulgent/permissive
for autonomy. (low demandingness, high responsiveness); and (4) uninvolved/
neglectful (low demandingness, low responsiveness).
Food acceptance:5 The level of liking of a particular food.
The biology of taste provides a foundational guide for food Picky eating:6 Characterized by consuming a limited type and
acceptance (e.g., easily accepting sweet tastes and rejecting amount of foods, unwillingness to try new foods, and rejecting
bitter tastes), while children’s experiences and learning foods based on certain sensory characteristics or textures.
Evidence-Based Recommendations and Best Practices for
| October 2021 5
Promoting Healthy Eating Behaviors in Children 2 to 8 Years
Introduction
Purpose and Aim
Childhood is a period of tremendous cognitive, socio-
emotional, and physical development. Nutrition plays a vital
The Dietary Guidelines for Americans, revised every
role in growth, development, and overall health, as well as
five years, provide evidence-based recommendations
in the prevention of obesity and other lifelong, diet-related
about what foods and beverages to consume, and in
chronic diseases.9 Childhood is also recognized as a critical
what amounts, to promote health, prevent disease,
period for the development of eating behaviors and habits that
and meet nutrients needs across the lifespan. However,
reflect a complex interplay of biological predispositions for
the DGAs have not provided science-based advice or
taste preferences and early experiences and learning in diverse
detailed recommendations on how to feed children.
environments, which ultimately serve as a child’s general
Guidance on both what and how to feed children is
orientation to eating.10,11
critical for the development of healthy eating behaviors,
food acceptance, and achieving a healthy weight.
The home is the first fundamental food and eating environment
in which a child’s eating habits emerge and it remains a critical
To address this critical information gap, Healthy
environment throughout childhood. Research conducted over
Eating Research convened a national panel of experts
the past four decades has highlighted the powerful role parents
to develop evidence-based recommendations and best
play in shaping the family food environment, both by providing
practices for promoting healthy nutrition and eating
a model of eating behavior that children learn to emulate and by
behaviors in typically developing children from 2 to 8
shaping a variety of interactions through which eating behaviors
years of age.
are socialized.12-14 Children’s early experiences and learning about
foods and eating are also shaped by diverse interactions outside
the home, including with other caregivers and peers, such as in
early care and education and eventually school and after-school Recommendations reflect extensive basic and applied research
settings. These interactions expose children to a wide range of expertise of panel members on topics including children’s food
eating environments and social influences. Thus, all caregivers preferences and eating behaviors, parenting styles, feeding styles,
who routinely care for and feed children have the capacity to food parenting practices, settings where children receive care,
influence the development of healthy eating behaviors. child obesity, and cultural and socioeconomic influences.16
Data from the 2017-2018 National Health and Nutrition This report includes the following nine sections:
Examination Survey indicate that U.S. children 2 to 5 years of
age consume approximately 75 percent of daily energy intake 1. Introduction to children’s eating behaviors;
at home highlighting the important role of parents in shaping
the early development of children’s eating behaviors.15 However, 2. Rationale for developing recommendations and
approximately 60 percent of U.S. children under the age of 5 presentation of conceptual frameworks and models that
are in a non-parental childcare arrangement. Further, by the informed this work;
time children reach school age, somewhere between 33 and 38
percent of daily energy intake occurs outside the home. These 3. Background on the typical development of 2- to 8-year-
trends underscore that children’s eating occurs and is shaped olds, including growth and dietary patterns, and the
by caregiving and food environments in a variety of settings, development of food acceptance and healthy appetites
including home, childcare, school, and other places where and growth;
children spend a large portion of their time and eating occurs
such as homes of relatives or friends. 4. Methodology used to develop these recommendations;
This report presents evidence-based recommendations for 5. Review of the evidence considered;
promoting healthy eating behaviors in children aged 2 to
8. Recommendations reflect expert consensus on current 6. Recommendations for promoting food acceptance and
scientific knowledge in two broad areas: (1) promoting healthy appetites and growth;
acceptance of healthful foods; and (2) promoting healthy
appetites and growth. Research on the development of 7. Considerations for implementing the recommendations;
children’s eating behaviors is relatively new, but rapidly
evolving. The recommendations in this report were developed 8. Future research needs; and
through a review of scientific research and consensus of a
panel of national experts with diverse expertise in nutrition, 9. Conclusions.
pediatrics, psychology, child development, and sociology.
6 October 2021 | Technical Report
Rationale and Conceptual Frameworks and Models
Building on the Foundations of Responsive Approaches responsive feeding and sleeping routines. Economic and social
to Feeding Infants and Toddlers determinants of health, including income, education, and home
environments and resources were highlighted as important
A child’s first 1,000 days (conception through 24 months of considerations for understanding and implementing responsive
age) is a dynamic period for the development of feeding skills, feeding. The recommendations presented in this report build
food acceptance patterns, and growth. While preferences on the foundations of those guidelines and focus on promoting
for the basic tastes (i.e., sweet, salty, sour, bitter, umami) are healthy eating behaviors in children 2 to 8 years old.
biologically determined, preferences for foods must be learned
and are acquired through experiences shaped by caregiving. Conceptual Model and Frameworks Informing the
In 2017, Healthy Eating Research, a national program of Expert Panel’s Approach
the Robert Wood Johnson Foundation, released “Feeding
Guidelines for Infants and Young Toddlers: A Responsive The expert panel’s identification of key elements necessary for
Parenting Approach”17 with the goal of empowering caregivers promoting children’s healthy eating behaviors is informed by
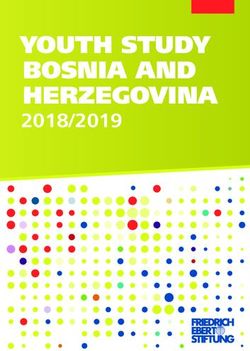
to promote optimal nutrition and development by offering the socioecological model of children’s weight and dietary intake
healthier food and beverage options in response to child hunger shown in Figure 1. The model is adapted from prior work
and satiety cues. A diverse panel of experts was brought together focused on child obesity,20,21 and highlights the multiple levels of
to synthesize the scientific literature and develop evidence-based influence ranging from biology to culture.
feeding guidelines for caregivers that focused on what and how
to feed infants and toddlers. That panel also aimed to inform Frameworks for parenting and feeding styles and for food
inclusion of dietary guidance for children under 2 years of age parenting practices guided the panel’s conceptualization of healthy
in the U.S. Dietary Guidelines for Americans (DGA); the DGA eating and illustrated the role of caregivers. The literature on
included recommendations for this age group for the first time children’s healthy eating and obesity prevention has traditionally
in the 2020-2025 edition.18 included a substantial focus on the proximal influence of parents
as key agents of change in shaping children’s eating behaviors
Responsive feeding approaches are characterized by emotional and weight gain. But to more fully examine how parents
support and the provision of developmentally appropriate influence children’s eating habits, it is necessary to understand
foods, eating environments, and responses to child hunger and the difference between the concepts of parenting, parenting
fullness cues.17,19 The 2017 report concluded that principles of styles, feeding styles, and food parenting practices. “Parenting”
responsive feeding associated with healthy eating are critical is the term generally used to explain how a parent influences a
for fostering optimal child development and growth and child’s behaviors and development, whereas “parenting style” is a
foundational for food acceptance. Guidelines were developed constellation of parental attitudes and beliefs toward child rearing,
separately for infants and toddlers and covered a broad range which create an emotional climate through which parental
of feeding aspects, including what to feed, interpretation of practices are expressed.22 Parenting styles are characterized in
hunger and fullness cues, how to introduce new foods, and terms of demandingness (i.e., expectations for self-control, limit
Figure 1. Socioecological
Model of Children's Weight COMMUNITY
Food
and Dietary Intake
advertising Culture
Parenting FAMILY
Child feeding
style
practices
Peer behavior Sibling CHILD
behavior
Modeling Socioeconomic
Eating Weight & Dietary
Biology of eating status
behavior intake
behavior
Food in
Temperament
School the home
Nutrition
Parental eating knowledge
behavior
Policy
Child care
Neighborhood food
accessibility
Evidence-Based Recommendations and Best Practices for
| October 2021 7
Promoting Healthy Eating Behaviors in Children 2 to 8 Yearssetting) and responsiveness (i.e., sensitivity or nurturing). These In contrast to parenting and feeding styles, food parenting
dimensions are used to describe four types of parenting styles: (1) practices are specific goal-directed parent actions or behaviors
authoritative; (2) authoritarian; (3) permissive/indulgent; and (4) designed to influence children’s eating behaviors.22 Research on
uninvolved/neglectful (Table 1). food parenting practices, primarily led by Leann Birch, began
to receive increasing attention in the scientific literature in the
This framework of general parenting style, developed in the late 1990’s.25 Food parenting practices are conceptualized to be
1960’s by Diana Baumrind,23 began to be applied to feeding relatively more amenable to change than parenting styles and
styles in the mid-2000’s.24 “Feeding styles” are the broad approach therefore are often targets of interventions that aim to influence
that parents take to feed children, and the emotional climate in children’s eating behaviors.
which feeding occurs. Similar to parenting styles, feeding styles
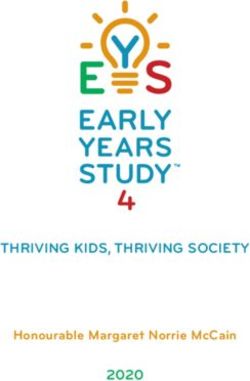
are generally conceptualized as consisting of two dimensions: (1) The most contemporary conceptualization of food parenting
demandingness, which refers to how much the parent encourages is represented in a model set forth by Vaughn et al.,7 which
or controls eating (e.g., limit setting, rules, expectations), and provides the framework for food parenting used in this
(2) responsiveness, which refers to how parents respond to report (Figure 2). Many different types of food parenting
the child’s cues and needs to encourage eating and support practices have been identified and are broadly described in
children’s developing autonomy. There are also four types of three dimensions: coercive control, structure, and support
feeding styles (Table 2). for child autonomy (Table 3). Food parenting practices
reflecting coercive control, such as intrusiveness and pressure,
are thought to be counterproductive to the development of
Figure 2. Conceptualization of Food Parenting (Vaughn et al, Nutrition Reviews, 2016)
Restriction
Food-based threats
Parent's pressure, and bribes to eat
Pressure to eat
intrusiveness, and
Coercive dominance in relation to Food-based threats
Threats and bribes
Control children's feelings and and bribes to behave
thoughts, as well as Using food to control
their behaviors Non-food incentives
negative emotions
attitudes and beliefs, knowledge, resources (financial, time), values, etc.
to eat
Precursors or determinants of Food Parenting Practices: ability,
Rules and limits
Limited/guided
choices
Atmosphere of meals
Monitoring
Distractions
Meal and snack
routines Family presence
Parent's organization of
Food Parenting children's environment Modeling
Structure Meal and snack
Practices to facilitate children's
schedule
competence Food availability
Food accessibility
Neglect
Unstructured
practices
Indulgence
Nutrition education
Child involvement
Encouragement
Promoting psychological
Autonomy
autonomy and
Support or Praise
encouragement of
Promotion
independence Reasoning
Negotiation
8 October 2021 | Technical ReportTable 1. Parenting Styles
Dimensions
Parenting Styles Characteristics
Demandingness Responsiveness
Nurturing, affectionate, non-punitive, discipline through
Authoritative High High
guidance, open communication
Strict, inflexible, high expectations, high supervision,
Authoritarian High Low
obedience
Permissive Low High Nurturing, affectionate, few or inconsistent boundaries
Uninvolved Low Low Emotionally detached, inconsistent boundaries
Table 2. Feeding Styles
Dimensions
Feeding Styles Characteristics
Demandingness Responsiveness
Parental involvement, nurturance, reasoning, and structure
Authoritative High High
during feeding
Restrictive, punitive, rejecting, and power-assertive behaviors
Authoritarian High Low
during feeding
Warmth and acceptance in conjunction with a lack of
Indulgent Low High
monitoring of the child’s eating behaviors
Little control and involvement with the child during
Uninvolved Low Low
eating episodes
Table 3. Food Parenting Practices
Food Parenting
Definition Examples
Dimensions
Parental pressure, intrusiveness, and
Restriction, pressure to eat, threats and bribes, using
Coercive Control dominance in relation to children’s feelings,
food to control negative emotions
thoughts, and behaviors
Parents’ organization of children’s environment
Rules and limits, limited/guided choices, monitoring,
to facilitate children’s competence in
Structure routines, modeling, food availability, accessibility,
engaging in healthy behaviors and avoiding
and preparation
unhealthy behaviors
Autonomy support Promoting psychological autonomy and Nutrition education, child involvement, encouragement,
or promotion encouragement of child’s independence praise, reasoning, negotiation
Evidence-Based Recommendations and Best Practices for
| October 2021 9
Promoting Healthy Eating Behaviors in Children 2 to 8 Yearshealthful eating behaviors. Alternatively, practices providing Background: The Typical Development
structure are believed to promote healthful eating behaviors of 2- to 8-Year-Olds
and discourage unhealthful behaviors by organizing the
environment to facilitate these outcomes. Similarly, practices Growth Across Domains of Development from Ages 2
that support children’s autonomy are believed to support healthy to 8 Years
eating behaviors by providing encouragement and support of
independence and internalization of healthful behaviors. It is important to recognize that the development of children’s
eating behaviors is largely dependent upon overall child
Different food parenting practices have different effects at development, traditionally defined in four major domains:
different ages. For example, among children 7 and older, motor, cognitive, language, and social/emotional. Despite
structured guidance/rule-making is more effective in preventing great variation in development across these domains between
unhealthy eating, while for children 6 and younger, rewarding individual children, key developmental milestones can be tied
with verbal praise is more effective in promoting healthy eating to certain age ranges. The panel applied established evidence on
and in preventing unhealthy eating.26,27 While most of the the stages of child development to identify key milestones in the
literature on food parenting practices has focused on controlling development of children’s eating behaviors.29 A general overview
practices, including restriction, monitoring, and pressure to of typical development and how each may relate to eating
eat,28 there are a growing number of studies assessing how behavior is provided in Table 4. Gross motor development
practices focused on structure and autonomy support impact has been omitted given it is less related to eating behavior;
dietary behaviors and weight status. instead, more detail has been included on fine-motor and oral-
motor development.
Table 4. Growth Across Domains of Development
Between ages 2 and 3 years, children can eat without assistance. They can use a spoon to scoop food
and a fork to stab food (though they may not always successfully get the food to their mouths). Children
can use straws effectively, but are just beginning to use an open-mouthed cup independently. Children are
able to chew with a closed mouth and can manage more textured foods like raw vegetables and meat. By
this age, children have acquired molars, and are learning to chew and grind with their molars efficiently.
Motor
Development
Between ages 4 and 5 years, children can spread and cut with a knife. They can drink from an open-
mouthed cup without assistance and without spilling.
Between ages 5 and 8 years, children can use a fork and knife together to cut food and are able to use
cutlery without being too messy.
Between ages 2 and 3 years, children can match and sort by shape and color (e.g., separate the green
spherical peas from the orange cubed carrots). They understand the concept of “two” (e.g., “you can have
two cookies”) and the idea of counting. They know common colors (e.g., tomatoes are red, bananas are
yellow). Children this age begin to be able to bargain.
By age 4 years, children understand the concepts of “same” and “different” (e.g., “that is the same peanut
butter that we eat at home”). Children this age begin to understand time (e.g., “snack time is in one hour,”
“you can have that candy tomorrow”).
Cognitive
Development By age 5 years, children can count ten or more items (e.g., “you can get yourself 10 crackers”) and
understand consecutive concepts (big, bigger, biggest). Children this age are aware of rules and will test
boundaries by arguing the rules.
Between ages 5 and 8 years, children begin to better understand others’ perspectives, and that
other people can have different opinions from their own. They begin to understand that objects can be
categorized in different ways (e.g., vegetables vs. fruits; or as organic vs. not). Children this age can
imagine the consequences of something happening without it actually happening (e.g., “What will happen if
we leave the casserole in the oven too long?”).
10 October 2021 | Technical ReportBetween ages 2 and 3 years, children can follow simple and familiar 2-step instructions (e.g., “Sit down
and eat your cereal.”). They can discern affect and meaning based on the speaker’s tone of voice (e.g., a
stern, “Eat your crackers,” versus an inviting, “Eat your crackers”). Children this age are only just beginning
to be able to take conversational turns and are typically speaking in 2- to 3-word sentences (e.g., “I want
cookie”), but much detail is lacking.
By age 4 years, children know names for groups or categories (e.g., apples and oranges are both fruit),
which has implications for teaching about healthy eating. They can express themselves using words like
“because” or “if” (e.g., “I don’t like this food because it has spots on it.”) Children ask more “why” questions
(e.g., “Why do I need to eat this?”), and their questions will become more abstract and complex (e.g., “If
I eat this, can I have ice cream?”). By age 4 years, children are also able to understand and use words to
express emotions (e.g., “I am scared to eat that.”)
By age 5 years, children can proficiently talk about events that have happened in the past or will happen in
Language the future, can follow directions with more than one step, and can engage more effectively in a conversation
Development by taking turns. Therefore, children are able to begin to describe what they ate at a friend’s house or at
preschool earlier that day, can request foods that they had at grandma’s house last week, and can ask
about going out for ice cream later that day. When parents deliver prompts to children to eat, the prompts
may become more complex with multiple steps as children better understand these multi-step instructions
(e.g., “you need to eat your carrots and drink your milk before you can leave the table”). Children’s greater
sophistication in conversations can contribute to lengthier negotiations in response to a command to eat
their vegetables—instead of simply responding, “No,” or, “I don’t want to,” the child can now effectively
engage in a multi-step, back-and-forth discussion with the parent. Children have also learned that using
less direct language can be more effective in getting what they want—instead of saying, “I want that
cookie,” the child has learned that saying, “Those cookies smell good. Could I have one?” is likely to be
more effective.
Between 5 and 8 years, children develop the ability to read, and therefore the ability to take in more written
information about food (i.e., reading menus or food packages, and therefore also being newly influenced by
written advertising).
Between ages 2 and 3 years, children will become increasingly interested in modeling the behavior of
others (i.e., eating like others eat). They tend to like routines and may become upset when routines are
disrupted (e.g., when a snack is not offered at the usual time). Children are developing the ability to employ
self-regulation strategies learned from previous experiences (e.g., distracting themselves while waiting for
a snack). Children can begin to remember rules and can wait for a toy or a treat for about a minute and
focus attention for about a minute. Children this age begin to understand that others can think and believe
different things than they do (e.g., that when a parent thinks the soup is delicious, the soup may or may not
be delicious in the child’s own opinion).
By age 4 years, children can understand and relate to how others are feeling (e.g., recognize that one
child is excited, and another child is sad that the birthday cake has fruit in it). By this age, children may
begin feeling generous and share food with friends, and they more readily express their likes and dislikes
(e.g., “She likes peas. I don’t like peas.”). Children this age prefer to play with other children and may be
increasingly influenced by peer behaviors (e.g., the food preferences of preschool peers may particularly
influence their food choices). At this age, children still cannot differentiate between real and make believe
Social/Emotional
(and may therefore be easily influenced by food advertising delivered by favorite characters). At this age,
Development
children typically can focus their attention for about 5 to 15 minutes. They can also describe ways to cope
with anger or sadness.
By age 5 years, children can use words to describe more complex emotions (e.g., “I’m jealous she has
pizza.”). Children this age are better at managing strong emotions, and less likely to have tantrums. They
are also better able to hide the truth (e.g., “I ate the broccoli,” even when it is in a napkin in their pocket).
At this age, children become more adept at apologizing for inadvertent mistakes (i.e., “I’m sorry I spilled my
milk.”).
Between ages 5 and 8 years, children increasingly want to be liked and please their friends (and may
therefore become increasingly influenced by the eating behaviors of peers). They are spending more time
with peers who have a growing influence on eating behavior. Children this age tend to test boundaries, but
are generally still eager to please and begin to experience embarrassment (i.e., sneaking a cookie, and
then being embarrassed when they are found out). At this age, children are often able to disguise emotions
when they are upset (e.g., pretend to like the dinner served at a friend’s house).
Evidence-Based Recommendations and Best Practices for
| October 2021 11
Promoting Healthy Eating Behaviors in Children 2 to 8 YearsDietary Patterns of Children Ages 2 to 8 Years Table 5. Recommended Intakes
The food and beverages children consume have a profound
Age 2-4 Years 5-8 Years
influence on their health and development. Because children
do not consume nutrients in isolation, it is important to look
Males Females Males Females
at dietary patterns—the combinations of foods consumed over
time. A healthy dietary pattern is needed for children to meet Energy (kcal) a
1,000- 1,000- 1,200- 1,200-
nutrient and energy needs and to support healthy weight and 1,600 1,400 2,000 1,800
prevention of chronic disease. Establishing a healthy dietary
pattern early in life is critical in order to lay the foundation for Food Group Servings
healthy dietary patterns that continue across the lifespan. Table
5 outlines healthy dietary patterns for males and females 2 to 8 Vegetables
1.0-2.0 1.0-1.5 1.5-2.5 1.5-2.5
years of age. Goals for food group intakes are based on calorie (cup eq/day)
needs, which vary by age, sex, height, weight, and activity level;
this is why ranges of intake are listed for each food group. Fruits
1.0-1.5 1.0-1.5 1.0-2.0 1.0-1.5
(cup eq/day)
The 2020-2025 Dietary Guidelines for Americans (DGA)18
Whole Grains
defines a healthy U.S.-style dietary pattern as including: (1) 1.5-3.0 1.5-2.5 2-3 2-3
(ounce eq/day)
vegetables of all types—dark green, red, and orange; beans, peas,
and lentils; starchy; and other vegetables; (2) fruits, especially Dairy (cup eq/day) 2.0-2.5 2.0-2.5 2.5 2.5
whole fruit; (3) grains, at least half of which are whole grains;
(4) dairy, including fat-free or low-fat milk, yogurt, and cheese, Protein Foods
2-5 2-4 3-5.5 3-5
and/or lactose-free versions and fortified soy beverages and (ounce eq/day)
yogurt as alternatives; (5) protein foods, including lean or
low-fat meats and poultry, eggs, seafood, beans, peas, lentils, Oils (g/day) 15-22 15-17 17-24 17-22
nuts, seeds, and soy products; and (6) oils, including vegetable
oils and oils in foods, such as seafood and nuts. Foods in such Dietary Components to Limit
healthy dietary patterns are assumed to be in nutrient-dense
forms and prepared with minimal added saturated fat, added Saturated Fat
(% of total calories 10 10
sugars, refined starches, or sodium (salt). not to exceed)
The current dietary patterns of children aged 2 to 8 years do Added Sugars
not align with the recommendations put forth by the 2020- (% of total calories 10 10
2025 DGA.18 For example, by 2 years of age, a child is more not to exceed)
likely to eat processed foods high in sodium and added sugar
than fruits or vegetables on any given day.30 The Healthy Eating 1,200 (age 2-3)
Index (HEI) score, a diet quality measure that assesses how well Sodium (mg/day)b 1,500
dietary intakes align with the Dietary Guidelines for Americans, 1,500 (age 4)
highlights the need for dietary improvements in children across
all developmental periods. In children 2 to 8 years of age, the Acronyms and abbreviations: EER = estimated energy requirement;
eq = cup-equivalents; kcal = kilocalories; mg = milligrams
average HEI scores range from a low of 55 (ages 5-8) to a high
of 61 (ages 2-4) on a scale of 0 to 100, indicating that overall Footnotes:
children’s diet quality is poor.18 a = Energy needs vary based on many factors, including age, sex,
height, weight, and activity level. To estimate specific energy needs
for an individual, please refer to the DRI Calculator for Healthcare
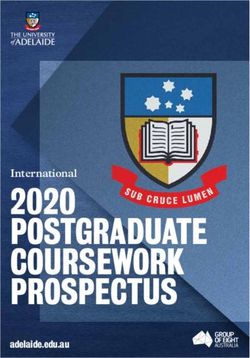
Figure 3 illustrates the percentage of U.S. children ages 2 Professionals, available at nal.usda.gov/fnic/dri-calculator.
to 3 and 4 to 8 who are below, at, or above dietary goals for
b = Recommendation is to reduce intakes if above these values, which
food group intakes. Fifity to sixty percent of these children are the Chronic Disease Risk Reduction Intakes established by the
meet intake recommendations for fruit, but less than 15 National Academies of Sciences, Engineering, and Medicine in the DRIs
percent and 7 percent do so for vegetables and whole grains, for Sodium and Potassium, published by the National Academies Press
in 2019.
respectively. Fifty-one percent of 2- to 3-year-old children meet
recommendations for dairy intake, but this number drops Source: Dietary Guidelines for Americans, 2020-2025. Table 3-1:
to 27 percent among 4- to 8-year-old children. Seventy-two Healthy U.S.-Style Dietary Pattern for Children Ages 2 Through 8,
percent of 2- to 3-year-olds and 63 percent of 4- to 8-year-olds With Daily or Weekly Amounts From Food Groups, Subgroups, and
Components, page 74
meet recommendations for protein foods.31 These less-than-
12 October 2021 | Technical ReportFigure 3. Dietary Intakes Compared to Recommendations: Percent of US Children Who Are Below, At, or Above Each
Dietary Goal or Limit
Figure 3a. Ages 2-3 intake below rec or above limit – Male
intake at/above rec or below limit – Female
Fruit
Vegetables
Whole Grain
Dairy
Protein
Added Sugar*
Sodium*
Saturated Fat*
*Ages 1-3 -100 -80 -60 -40 -20 0 20 40 60 80 100
Figure 3b. Ages 4-8 intake below rec or above limit – Male
intake at/above rec or below limit – Female
Fruit
Vegetables
Whole Grain
Dairy
Protein
Added Sugar
Sodium
Saturated Fat
-100 -80 -60 -40 -20 0 20 40 60 80 100
Evidence-Based Recommendations and Best Practices for
| October 2021 13
Promoting Healthy Eating Behaviors in Children 2 to 8 Yearsoptimal intake patterns are related to inadequate intakes of
Figure 4a. Distribution of Snack Occasions for Males and
nutrients such as calcium, potassium, vitamin D, and fiber that
Females 2-5 Years of Age
are important for children’s growth and development. Because
of documented disparities in diet quality by race, ethnicity, 30%
Males
income, and education, some children are at a higher risk of Females
25%
consuming a poor-quality diet.31,32
20%
Additionally, the DGAs recommend that children limit intakes
of added sugar as well as saturated fat to less than 10 percent 15%
of daily energy, and to reduce intakes of sodium that are above
1,200 mg/day (ages 2-3) or 1,500 mg/day (ages 4-8). Only 10%
about half of younger (ages 1-3) and close to one-quarter of
5%
older (ages 4-8) children meet the recommendation for added
sugar,31 and about 15 percent (ages 1-3) and 12 percent (ages 0%
4-8) of children meet the recommendation for saturated fat.33 0 1 2 3 4 5 6 7+
Only about 6 percent of children ages 1-3 and 4 percent of Number of Daily Snack Occasions
children ages 4 to 8 meet sodium recommendations.34
With regard to the context of young children’s nutrient intakes,
almost one-third of daily calories (29% for males and 28% for Figure 4b. Distribution of Snack Occasions for Males and
females) for children 2 to 5 years old are contributed by foods Females 6-11 Years of Age
and beverages consumed during snacks. Among children 6 to 11 30%
Males
years of age, approximately one-quarter of daily calories (26% Females
for males and 24% for females), are contributed by foods and 25%
beverages consumed during snacks.35 This is not surprising given
20%
that among children ages 2 to 5, 52 percent of males and 45
percent of females consume 3 to 4 snacks per day, and among 15%
children ages 6 to 11, 41 percent of males and 38 percent of
females consume 3 to 4 snacks per day (Figures 4a and 4b).35 10%
It is also noteworthy that a considerable portion of young 5%
children’s daily calories are contributed by foods and beverages
consumed away from home. Among children 2 to 5 years of 0%
0 1 2 3 4 5 6 7+
age, 25 percent and 27 percent of calories consumed by males Number of Daily Snack Occasions
and females, respectively, are contributed by these foods. Among
children 6 to 11 years of age, 33 percent and 38 percent of
calories consumed by males and females, respectively, are from Source: U.S. Department of Agriculture ARS. Snacks: Percentages
foods and beverages consumed away from home.36 of Selected Nutrients Contributed by Food and Beverages Consumed
at Snack Occasions, by Gender and Age, What We Eat in America,
NHANES 2017-2018. 2020. (https://www.ars.usda.gov/ARSUser-
Childhood obesity has been a significant health problem for Files/80400530/pdf/1718/Table_29_DSO_GEN_17.pdf).
the past 30 years and is undoubtedly related to children’s
poor dietary patterns. According to the National Health and
Nutrition Examination Survey,32 between 1999-2000 and
2017-2018 prevalence of obesity has plateaued among children
younger than 2 years of age at about 9 percent and at about 14
percent for children 2 to 5 years of age. In contrast, prevalence
of obesity has increased during this time among children ages 6
to 19 years. Between 1999-2002 and 2015-2018, the prevalence
of obesity among children aged 6 to 11 years increased from
nearly 16 percent to more than 19 percent, and youth aged 12
to 19 years experienced an increase from 16 percent to nearly 21
percent. Early data from 2020 are showing further increases in
child overweight and obesity during the COVID-19 pandemic,
with the greatest changes being among children ages 5 to 11.37
14 October 2021 | Technical ReportRates of obesity among children of color are disproportionately Taste preferences vary from person to person. Sensitivity
higher than rates among white children, and have continued to to bitterness, in particular, is known to vary greatly among
increase across all ages for the past 30 years.38 For comparison, individuals; one person may detect bitterness at a low
only 3 percent to 4 percent of U.S. children ages 2 to 5 and 6 to concentration whereas another may be insensitive to its taste or
11 years are classified as underweight (defined as sex- and age- require very high concentrations to detect it. Genetic variation
specific BMIC being less than the fifth percentile).39 in the TAS2R38 gene produces individual differences in
sensitivity to the bitter tastants,60 such as 6-n-propylthiouracil
The overall pattern suggests that accumulated lifetime exposures (PROP).61 Children who exhibit sensitivity to the bitter taste
(biological, behavioral, environmental, and systemic) continue of PROP tend to have lower liking and intake of some raw
to drive ongoing increases in obesity prevalence across the life vegetables (e.g., spinach and broccoli), while also tending to
course. Obesity, once established, is very likely to persist.40 have higher liking/intakes of sweet foods and consume less fat
Understanding the development of obesity and how to support than non-tasters.58,61 Individual differences in taste preferences
healthy eating behaviors in childhood is essential. Further, for bitterness as well as sweetness have been found to differ
understanding the development of food acceptance and based on age, race/ethnicity, family history of addiction/
healthy appetites among children is foundational to multi- depression, and taste receptor genotype.56,62,63 Children with
level approaches to prevent obesity and support healthy eating sensitivity to bitter tastes may require additional strategies to
behaviors in childhood. learn to like some healthful foods with bitter taste profiles such
as using dips and sauces, using preparation methods that yield
Development of Food Acceptance during Childhood milder tastes, and reinforcing children’s willingness to try foods
through praise and/or small non-food rewards.58,64
Children eat what they like and like what they know.41
Young children’s intake of foods is closely aligned with food The biology of taste provides a foundational guide for food
preferences,42-44 underscoring the fundamental role the acceptance; however, children’s experiences and learning in their
development of healthy food preferences plays in promoting early eating environments shape the course of food preferences
healthful eating patterns. A large body of research shows that and eating habits. For example, children’s heightened
children are born with innate preferences for taste that predispose preferences for the taste of sweet compared with those of adults
them to readily like some foods and be initially wary of others.45-47 enhances the atrractiveness and ready acceptance of foods high
Preferences for food, on the other hand, are learned through in sweetness.65-70 Yet children also develop liking and preferences
experiences that are inherently social in nature, highlighting the for foods through associative learning and familiarization that
powerful role of caregivers and the family eating environment in occur as they accumulate eating experiences, underscoring the
shaping children’s acceptance of healthful foods.14,48 The nature role of the family and socialization of eating behaviors.71,72 For
of children’s eating experiences varies with the contexts in which instance, sweet foods are often provided to children as treats or
eating occurs as well as the people with whom children eat and rewards for good behavior, providing social reinforcement of
generally reflects a wide range of family, cultural, and broader children’s liking for foods they are biologically predisposed to
socio-environmental and socio-economic influences. find attractive.73,74 Further, food media advertisements targeting
children have been shown to encourage children’s liking of,
Taste Preferences requests for, intake of, and loyalty to advertised brands and the
Biologically programmed taste preferences provide a strong unhealthy foods which are typically featured.
foundation for food acceptance in childhood. Newborns show
distinct preferences for sweet and umami tastes and initial Food Neophobia
rejection of sour and bitter tastes.47,49 These predispositions A common challenge to the acceptance of healthful foods during
are thought to have evolved to favor survival by encouraging childhood is food neophobia, defined as fear of or reluctance
consumption of energy-rich foods and discouraging consumption to eat new foods.6,75 The degree of food neophobia changes as
of toxins and spoiled foods. Taste preferences change as a child develops, with relatively low levels seen in late infancy
development proceeds across childhood. For instance, children during the introduction to complementary foods. However,
have heightened preferences for salt,50,51 sweetness,51-53 and sour54 children show pronounced and normative increases in food
in comparison to adults.38,53-57 Children also show heightened neophobia during toddlerhood and preschool years, where levels
sensitivity for some bitter tastes throughout early childhood into are at the highest point seen across the lifespan.76 During this
adolescence.55,58 These patterns underscore that children establish time, children may be reluctant to try and accept new foods and
eating habits in a fundamentally different sensory world than become more selective about the foods they are willing to try
adults, with normative tendencies to prefer sweet foods and reject and eat.77,78 Reflecting biological taste predispositions, children
bitter tasting foods like some vegetables.55,59 may be particularly wary of some healthful foods like vegetables
that are not terribly sweet, are not energy-rich, and can often be
bitter.79 These normative trends are a common cause of concern
Evidence-Based Recommendations and Best Practices for
| October 2021 15
Promoting Healthy Eating Behaviors in Children 2 to 8 Yearsfor many parents when children become more limited in what around behavior but also through a variety of behaviors that
they are willing to eat and show resistance to try new foods. For shape children’s exposure to new and healthful foods. Like food
most children food neophobia is relatively short-lived and tends neophobia, many children show signs of picky eating during
to diminish with age as children enter the school years.76 early childhood that tend to lessen with age.68,112
Picky eating Development of Healthy Appetites and Growth during
A related challenge to acceptance of healthful foods during Childhood
childhood is picky eating. Although there is not agreement in
the field on a formal definition of picky eating (also known Children’s regulation of eating behaviors reflects complex and
as “food fussiness”),76,80,81 the most commonly accepted dynamic interactions between biology and the environment.
definition is the rejection of a substantial amount of foods It has historically been believed that children are born with
that are familiar (as well as unfamiliar).76,82-89 Picky eating is an innate capacity to regulate their own eating behavior. For
generally considered to consist of three key characteristics: (1) example, in some controlled research studies, young children
consuming a limited variety (food selectivity)65,69,70,76,89-103 and demonstrated an ability to self-regulate short-term energy intake
amount of foods;76,90-94,104 (2) rejecting foods based on certain by making adjustments to subsequent food intake in response
sensory characteristics (appearance, aroma, feel, texture, or to the energy content of foods previously consumed.114,115 A
flavor),69,76,84,90,91 often requiring the preparation or presentation growing body of evidence, however, has demonstrated that this
of meals in a very particular way;65,69,90,92,95-99 and (3) capacity varies widely among children and at younger ages than
unwillingness to try new foods (food neophobia).76,79,88,91,105-107 previously thought.115 Children’s capacity to regulate intake
Some have hypothesized that picky eating could be only parent has been shown to be influenced by the types and amounts of
perception,96 but observational and experimental studies provide foods available, the social aspects of the eating environment,
some validation,66,92,98 for example by indicating that picky eaters and children’s behavioral and biological predispositions
consume a lower variety of vegetables69,92 and have lower total towards eating.
intakes of vegetables.69
Appetite is defined as an instinctive or natural desire to eat.
The varying definitions result in an unclear prevalence of picky Behavioral predispositions towards eating are broadly described
eating. Of the 25 percent of children identified by parents to in terms of food approach and food avoidance. Food approach
have feeding difficulties, only an estimated 1 to 5 percent meet is defined as a combination of behaviors characterized by food
criteria for a feeding disorder.67,94,108,109 Avoidant restrictive food responsiveness (i.e., the degree to which external food cues
intake disorder (ARFID), also described as extreme picky eating encourage an individual to eat) and the reinforcing value of
where a child does not consume enough calories to grow and food (i.e., the willingness to consciously work to obtain food).10
develop properly, was added to the Diagnostic and Statistical Some examples of food approach behaviors include eating in the
Manual of Mental Disorders V (DSM-V) in 2013 and requires absence of hunger (i.e., the number of calories a child consumes
one or more of the following: (1) significant weight loss, when palatable foods are offered following a satiating meal) and
faltering growth, or nutritional deficiency; (2) dependence on emotional eating (i.e., greater likelihood of eating in response
enteral feeding or oral nutritional supplements; or (3) marked to negative affect). Food avoidance is defined as a combination
interference with psychosocial functioning. The prevalence of of behaviors characterized by satiety sensitivity (i.e., the degree
ARFID and effective treatment modalities is an active area of to which one is capable of ceasing consumption in response
research. Treatment of ARFID is outside the scope of this report. to internal signals—typically conceptualized as signals from
the gut).10
Children with picky eating tend to have lower intakes of
vegetables,69,79,92,110 some micronutrients (iron, zinc), and Observational studies indicate that children with higher levels
fiber.68 Importantly, however, picky eating does not have a of food approach or motivation to eat tend to have higher body
consistent association with weight status and growth.6,68,111 mass index,10,116-122 whereas children with higher levels of food
Picky eaters show higher levels of negative affect, and sensory avoidance tend to have poorer diet quality. These behavioral
sensitivities to sight, sound, taste, smell, touch, and pain.78 predispositions are thought to be shaped, in part, by genetic
Picky eating has also been shown to be related to dimensions influences and have trait-like qualities. Individual differences
of child temperament including children’s enjoyment of novel in eating behaviors are reliably observed by parents beginning
experiences and sociability. While picky eating appears to have in infancy and track over time. Furthermore, twin and family
a trait-like, heritable component,88,112 it also has been associated studies provide evidence that eating behaviors reflecting appetite
with caregiver characteristics, including caregiver neophobia, are heritable or under genetic influence. Therefore, the evidence
dietary restraint, external cue eating, dietary intake, and for promoting healthy appetites in children necessarily overlaps
home availability.6,113 These observations highlight caregivers’ with the evidence for preventing and treating childhood obesity.
influence on not only contributing to genetic predispositions
16 October 2021 | Technical ReportYou can also read