Evaluation of the safety and effectiveness of the disposable endoscope for endoscopic rubber band ligation of internal hemorrhoids: A prospective ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Evaluation of the safety and effectiveness of the
disposable endoscope for endoscopic rubber band
ligation of internal hemorrhoids: A prospective
randomised controlled trial
Wen Xu
Southern Medical University Shenzhen Hospital
Guili Xia
Southern Medical University Shenzhen Hospital
Laihe Li
Southern Medical University Shenzhen Hospital
Ge Cao
HuiZhou Xzing Technology Co., Ltd
Xianhuan Yan
HuiZhou Xzing Technology Co., Ltd
Ling Dong
Southern Medical University Shenzhen Hospital
Ying Zhu ( zhuying1@smu.edu.cn )
Southern Medical University Shenzhen Hospital
Research Article
Keywords: Endoscopes, Ligation, Hemorrhoids, Safety, Effectiveness
Posted Date: January 6th, 2023
DOI: https://doi.org/10.21203/rs.3.rs-2439306/v1
License: This work is licensed under a Creative Commons Attribution 4.0 International License.
Read Full License
Page 1/16Abstract
Purpose
We aimed to compare not only the safety and effectiveness of endoscopic rubber band ligation (ERBL)
for treating grade II-III internal hemorrhoids using disposable endoscopes versus reusable endoscopes,
but also maintenance cost of them.
Method
This was a prospective randomised controlled trial with 42 patients who underwent ERBL for grade II-III
internal hemorrhoids using either a disposable endoscope (n = 21) or a reusable endoscope (n = 21).
Safety was assessed by postoperative infection rate, in-procedure vital stability, and incidence of device-
related adverse events. Effectiveness was assessed by endoscopic image clarity, flexibility, matching
between the endoscope and surgical instrument, and therapeutic effect. Cost accounting of maintenance
was also estimated.
Results
In terms of safety, although neutrophil count on a postoperative day (POD) 1 in the disposable endoscope
group was significantly higher than in the reusable endoscope group (P = 0.008), no patients in either
group had a postoperative infection. No life-threatening events, equipment failure or device-related
adverse effects occurred during the procedures in either group. In terms of effectiveness, image clarity (P
= 0.599) and endoscopic flexibility (P = 0.057) were mildly inferior in disposable endoscope group, but no
significant differences were found. Matching between the endoscope and ligating device was 100% in
both groups. The therapeutic effects on POD 30 were similar in both groups (P = 0.611). The maintenance
cost of reusable endoscope was 214.74RMB per case when disposable endoscope was 0.
Conclusion
Compared with reusable endoscopes, disposable endoscopes are equally safe, feasible, and reliable in
ERBL for internal hemorrhoids, and maintenance cost can be totally saved.
Clinical trial registration was completed (ChiCTR2200060014) on May 14, 2022.
1 Introduction
The common endoscope is repeatedly utilized in modern times. After each use, it needs to be cleaned and
sterilised before being used again, which is a complicated and time-consuming process. Concerns have
been raised over the possibility that reusable endoscopes cannot be fully sterilised [1, 2]. Previous reports
Page 2/16regarding antibiotic-resistant bacteria transmitted through gastroscopes have also attracted the attention
of endoscopists [3]. The EndoFresh® disposable endoscope (XZING-W200B, HuiZhou Xzing Technology
Co., Ltd., China) has been developed to reduce the risk of hospital infection and avoid cleaning and
sterilising procedures, especially during the COVID-19 pandemic. The safety and technical performance
of the disposable endoscope are comparable with reusable endoscopes used in routine examinations [4,
5]. However, minimally invasive gastrointestinal treatment using disposable endoscopes has not been
reported yet.
Treatment of minimally invasive internal hemorrhoids using endoscopes has proven effective and safe
for patients with grade I-III symptomatic internal hemorrhoids [6]. Patients with grade II and III internal
hemorrhoids with prolapse are mainly treated with endoscopic rubber band ligation (ERBL) [7]. As early
as 2002, ERBL performed in the retroflexed position has been proven to be easily available, safe, and
effective in treating symptomatic hemorrhoids [8, 9]. However, whether disposable endoscope-guided
ERBL is equally feasible as ERBL using traditional reusable endoscopes has not been explored yet.
In this study, we randomly used disposable or reusable endoscopes for ERBL in patients with grade II-III
internal hemorrhoids. This study aimed to compare the incidence of postoperative infection, endoscopic
flexibility, image clarity, device-related adverse events, clinical effects and maintenance cost of these two
types of endoscopes.
2 Patients And Methods
2.1 Study population
We recruited patients with symptomatic internal hemorrhoids diagnosed at Shenzhen Hospital of
Southern Medical University between May 14, 2022, and June 7, 2022. On July 7, 2022, the trial stopped
with the end of follow-up of the last recruited patient. This study was conducted in accordance with the
Ethical Guidelines of the Declaration of Helsinki. The Medical Ethics Committee of Shenzhen Hospital of
Southern Medical University approved this prospective cohort study (NYSZYYEC20210034) on April 20,
2022. Clinical trial registration was completed (ChiCTR2200060014) on May 14, 2022. Internal
hemorrhoids were graded according to Goligher's classification [10] (Table 1). The inclusion criteria are as
follows[11]: (1) Age of 18 to 75 years, with no limitation according to sex; (2) grade II-III internal
haemorrhoids with accompanying symptoms, such as bleeding, prolapse, or itching; (3) conservative
treatment for grade II-III internal haemorrhoids such as diet regulation and drugs has proven ineffective;
(4) patients unwilling to undergo haemorrhoidectomy. The exclusion criteria are as follows[12]: (1) Grade
IV haemorrhoids, mixed haemorrhoids, or external haemorrhoids; (2) internal haemorrhoids accompanied
by incarceration, thrombosis, erosion, or infection; (3) patients with severe systemic diseases who cannot
tolerate endoscopic treatment; (4) patients with perianal infectious diseases or anal fistulae; (5) patients
with active inflammatory bowel disease; (6) patients with coagulation dysfunction or using
anticoagulants; (7) pregnant women.
Page 3/16Table 1
Goligher’ s Classification
Grade Degree of Prolapse
I No prolapse
II Prolapse on defecation with spontaneous reduction
III Prolapse on defecation requiring manual reduction
IV Irreducible prolapse
According to the estimation formula of test sample content of single-group target value method, when the
significance level is 0.05 and the test efficiency (1-β) = 0.8, the estimated sample size is: N = 21, therefore,
a total of 42 patients were recruited. The random numbers were generated by computer, and the patients
were assigned to either the disposable endoscope group (n = 21, EndoFresh®, XZING-W200B, HuiZhou
Xzing Technology Co., Ltd) or the reusable endoscope group (n = 21, EG-600WR, Fuji Film Co., Ltd) orderly
according to random numbers. All patients were evaluated before treatment with a medical history review,
laboratory examination (blood tests, hypersensitive C-reactive protein (hs-CRP), coagulation function, and
infectious diseases), and electrocardiography (ECG). All patients signed informed consent forms for the
treatment and were informed of the risks associated with the treatment. All patients underwent whole
bowel preparation before ERBL.
2.2 Endoscopic rubber band ligation (ERBL)
Patients were treated with ERBL. After the multiple band ligation device (Speedband®, M00542251,
Boston Scientific Co., Ltd, USA) was attached to the endoscope, hemorrhoids were suctioned into the
ligating device, and then an elastic band was released. The above steps were repeated until the prolapsed
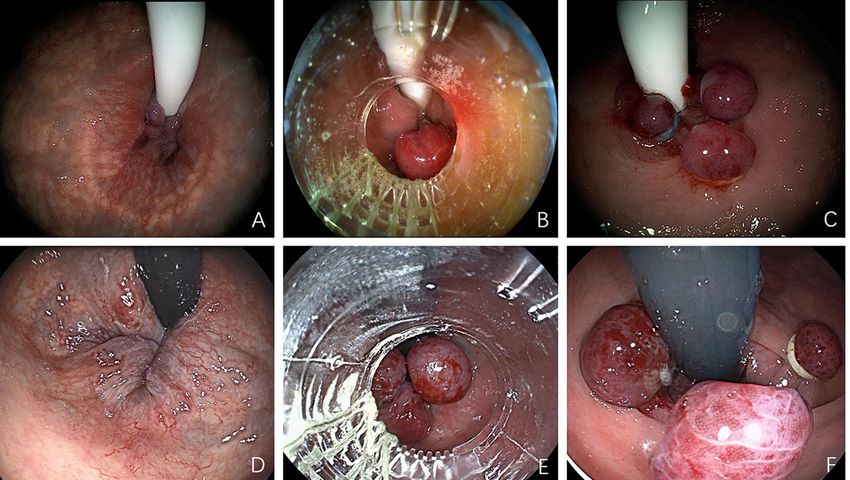
hemorrhoids were relieved, and no more than seven ligations in total were performed per patient (Fig. 1,
Supplementary Material, Video 1 and 2).
2.3 Evaluation measures
Follow-up visits were performed on postoperative day (POD) 1, POD 7, and POD 30, and the follow-up
items are listed below.
2.3.1 Safety measures
(1) Primary outcome measures: Postoperative infection
The primary outcome measure was the postoperative infection rate. Blood tests, hs-CRP, temperature, and
anal pain were measured on POD 1 and POD 7. We mainly focused on white blood cell (WBC) and
neutrophil (NEUT) counts among the blood tests. Anal pain intensity was quantified by the Visual
Analogue Scale (VAS), with scores on a scale of 0–10, where 0–3 indicates mild pain, 4–6 indicates
moderate pain, 7–9 indicates severe pain, and 10 indicates excruciating pain [12].
Page 4/16Evaluation criteria were formulated referring to the CDC definitions of nosocomial surgical site infections
[13]: (1) WBC count > 10×109/L, (2) NEUT count > 6.3×109/L, (3) hs-CRP > 10 mg/L, (4) temperature >
38°C, and (5) VAS of anal pain continuously > 4 with suppuration. Additionally, pathogens were cultured.
Patients who met all five items above were considered to have a postoperative infection.
(2) Secondary outcome measures: Trends of WBC count, NEUT count, and hs-CRP level
WBC count, NEUT count, and hs-CRP levels measured before the operation, on POD 1, and POD 7 were
compared within and between groups.
In-procedure stability
In-procedure vital sign stability was evaluated based on the changes in blood pressure and heart rate
measured before anaesthesia, during ERBL, and 10 ± 5 minutes after the procedure. Subjects whose
blood pressure and heart rate changed more than 20% from baseline were defined as 'unstable' [14].
Incidence of equipment failure and device-related adverse events
Equipment failure, such as image interruption, water delivery blockage, or leakage, and adverse events
during or within 1 hour after the operation, such as mucosa damage, bowel perforation, massive
haemorrhage, or instability of vital signs, were recorded.
2.3.2 Effectiveness measures
(1) Primary outcome measures: ERBL feasibility
Evaluation method: The operator evaluated endoscopic image clarity, flexibility, clinical operability, and
matching between the endoscope and surgical instrument.
Evaluation criteria:
(1) Image clarity was graded as follows: (A) Good brightness, contrast, and clarity: accurate identification
of the anal and dentate lines was possible, and internal hemorrhoids could be clearly identified. (B) Fair
brightness, contrast, and clarity: rough identification of the anal and dentate lines was possible, and
internal hemorrhoids could be roughly identified. (C) Poor brightness, contrast, and clarity: identification
of the anal and dentate lines was not possible, and internal hemorrhoids could not be identified.
(2) Endoscopic flexibility was graded as follows: (A) The endoscope could be easily retroflexed from the
forward position. (B) The endoscope could be roughly retroflexed from the forward position. (C) The
endoscope failed to be retroflexed from the forward position.
(3) Matching between the endoscope and ligating device was graded as follows: (A) The endoscope and
ligating device matched perfectly, and the operation went smoothly. (B) The endoscope and ligating
Page 5/16device matched roughly, and the operation procedure was slightly affected. (C) The endoscope and
ligating device could not match, and the operation failed to proceed.
ERBL feasibility was considered 'qualified' if all items were graded 'A' or 'B'. If any one item was graded 'C',
ERBL feasibility was considered 'unqualified'. The qualification rate of ERBL feasibility = (the number of
'qualified' cases/the number of subjects in each group) × 100.
(2) Secondary outcome measures: Postoperative follow-up
Evaluation method: All subjects underwent outpatient follow-up on POD 30 after ERBL to assess the
therapeutic efficacy.
Evaluation criteria: (1) Cured: haematochezia and prolapse symptoms disappeared completely, and
wounds healed completely. (2) Effective: haematochezia and prolapse symptoms were improved,
hemorrhoids were reduced or displayed incomplete atrophy, and wounds healed well. (3) Invalid:
haematochezia and prolapse symptoms were not alleviated or were aggravated.
2.3.3 Cost accounting
The cost of maintenance for each endoscope was estimated, including sterilization, repair and storage
costs.
2.4 Statistical analyses
Data were analysed using Statistical Product and Service Solutions Version 26.0 (SPSS, International
Business Machines Corporation). Since there was no loss of follow-up in this trial, the protocol set
population was consistent with the full analysis set population. Measurement data were analysed using
the paired t-test or Wilcoxon rank sum test between the two groups. The variance of repeated
measurement analysis was performed for intragroup and intergroup comparisons. Count data were
summarised by frequency and percentage (n [%]) and compared using the Chi-square test or Fisher's
exact test. A P-value of < 0.05 was considered statistically significant.
3. Results
3.1 General information
No significant between-group differences were observed for sex, age, grading of internal hemorrhoids, pre-
operation WBC and NEUT counts, hs-CRP, blood pressure, or heart rate (Table 2).
Page 6/16Table 2
Baseline Characteristics of the Patients
Disposable Endoscope Reusable Endoscope P-
Group (n = 21) Group (n = 21) Value
Age (years) 39.81 ± 7.17 41.48 ± 9.17 0.330
Gender, n (%)
Male 9 (42.86%) 9 (42.86%) 1.000
Female 12 (57.14%) 12 (57.14%)
Classification of Internal
Haemorrhoids, n (%)
III 12 (57.14%) 14 (66.67%) 0.525
II 9 (42.86%) 7 (33.33%)
3.2 Safety measures
(1) Primary outcome measures: Postoperative infection
NEUT count > 6.3×10^9/L was 66.67% in the disposable endoscope group and 19.05% in the reusable
endoscope group on POD 1, which were significantly different (P = 0.002). However, NEUT count >
6.3×10^9/L on POD 7, WBC count > 10×10^9/L and hs-CRP > 10 mg/L on POD 1 and POD 7 were not
significantly different between the groups. The mean temperature (°C) on POD 1 and POD 7 was 36.42 ±
0.33 and 36.30 ± 0.20 respectively in the disposable endoscope group and 36.45 ± 0.21 and 36.40 ± 0.21
respectively in the reusable endoscope group. The mean VAS on POD 1 and POD 7 was 0.95 ± 1.02 and
0.10 ± 0.44 respectively in the disposable endoscope group and 0.71 ± 0.85 and 0.24 ± 0.70 respectively in
the reusable endoscope group. No patients in either group suffered from suppuration. In summary, no
patients in either group suffered from postoperative infection (Table 3).
Page 7/16Table 3
Comparisons of Postoperative Infection between Groups
Disposable Endoscope Group Reusable Endoscope Group P-
(N = 21) (N = 21) Value
WBC POD 1, n (%)
> 10×109/L 7 (33.33%) 2 (9.52%) 0.133
≤ 10×109/L 14 (66.67%) 19 (90.48%)
WBC POD 7, n (%)
> 10×109/L 1 (4.76%) 0 (0%) 1.000
≤ 10×109/L 20 (95.24%) 21 (100%)
NEUT POD 1, n (%)
> 6.3×109/L 14 (66.67%) 4 (19.05%) 0.002
≤ 6.3×109/L 7 (33.33%) 17 (80.95%)
NEUT POD 7, n (%)
> 6.3×109/L 3 (14.29%) 0 (0%) 0.231
≤ 6.3×109/L 18 (85.71%) 21 (100%)
hs-CRP POD 1, n (%)
> 10 mg/L 0 (0%) 0 (0%) -
≤ 10 mg/L 21 (100%) 21 (100%)
hs-CRP POD 7, n (%)
> 10 mg/L 0 (0%) 2 (9.52%) 0.469
≤ 10 mg/L 21 (100%) 19 (90.48%)
Temperature, n (%)
> 38℃ 0 (0.0%) 0 (0.0%) -
≤ 38℃ 21 (100.0%) 21 (100.0%)
VAS, n (%)
>4 0 (0.0%) 0 (0.0%) -
≤4 21 (100.0%) 21 (100.0%)
WBC, white blood cell count; POD, postoperative day; NEUT, neutrophil
Page 8/16Disposable Endoscope Group Reusable Endoscope Group P-
(N = 21) (N = 21) Value
Suppuration, n (%)
Yes 0 (0.0%) 0 (0.0%) -
No 21 (100.0%) 21 (100.0%)
Postoperative Infection,
n (%)
Yes 0 (0.0%) 0 (0.0%) -
No 21 (100.0%) 21 (100.0%)
WBC, white blood cell count; POD, postoperative day; NEUT, neutrophil
(2) Secondary outcome measures: Trends of WBC count, NEUT count, and hs-CRP level (Fig. 2)
(1) WBC counts: The mean WBC counts (×10^9/L) before the operation, on POD 1, and POD 7 were 6.66
± 1.42, 8.44 ± 2.65, and 7.32 ± 1.44, respectively, in the disposable endoscope group, and 6.01 ± 1.32, 7.37
± 2.32, and 6.81 ± 1.36 respectively in the reusable endoscope group. There was no interaction in WBC
counts between the groups at different measurement times, and no significant difference in WBC counts
was found between the groups (P = 0.087). Significant differences were observed in WBC counts at
different measurement times (P = 0.000).
(2) NEUT counts: The mean NEUT counts (×10^9/L) before the operation, on POD 1, and POD 7 were
3.93 ± 1.14, 6.74 ± 2.03, and 4.78 ± 1.37, respectively, in the disposable endoscope group and 3.33 ± 1.17,
5.24 ± 1.89, and 4.28 ± 1.06, respectively, in the reusable endoscope group. There was no interaction in
NEUT counts between the groups at different measurement times. Significant differences were observed
in NEUT counts between the groups (P = 0.008). Significant differences were also observed in NEUT
counts at the different measurement times (P = 0.000).
(3) Hs-CRP: The mean hs-CRP levels (mg/L) before the operation, on POD 1, and POD 7 were 1.10 ± 1.43,
1.50 ± 1.83, and 3.93 ± 3.18, respectively, in the disposable endoscope group and 1.08 ± 0.83, 1.49 ± 1.47,
and 7.49 ± 15.86, respectively, in the reusable endoscope group. No interaction of hs-CRP level between
the groups was observed at different measurement times. There was no significant difference in hs-CRP
levels between the groups (P = 0.342). A significant difference in hs-CRP levels was observed at the
different measurement times (P = 0.016).
In-procedure stability
(1) In-procedure vital sign stability
During ERBL, systolic pressure stability, diastolic pressure stability, and heart rate stability were 85.71%,
66.67%, and 90.48%, respectively, in the disposable endoscope group, and 95.24%, 95.24%, and 90.48% in
Page 9/16the reusable endoscope group, respectively. Only diastolic pressures were statistically different between
the two groups (P = 0.049).
After the procedure (10 ± 5 minutes), systolic pressure stability, diastolic pressure stability, and heart rate
stability were 80.95%, 80.95%, and 85.71%, respectively, in the disposable endoscope group, and 90.48%,
80.95%, and 80.95%, respectively, in the reusable endoscope group. The difference between the two
groups was not statistically significant.
(2) Incidence of equipment failure and operation-related adverse events
No equipment failure or operation-related adverse events occurred in either the disposable or the reusable
endoscope groups.
3.3 Effectiveness measures
(1) Primary outcome measures: ERBL feasibility
Image clarity: Grade A was assigned to 18 operations (85.71%), and grade B was assigned to 3 (14.29%)
in the disposable endoscope group. Grade A was assigned to 20 operations (95.24%), and grade B was
assigned to 1 (4.76%) in the reusable endoscope group. The difference between the two groups was not
statistically significant (P = 0.599).
Endoscopic flexibility: Grade A was assigned to 16 operations (76.19%), and grade B was assigned to 5
(23.81%) in the disposable endoscope group. Grade A was assigned to 21 operations (100.00%), and
grade B was assigned to 0 (0%) in the reusable endoscope group. The difference between the two groups
was not statistically significant (P = 0.057).
Matching between endoscope and ligating device: Grade A was assigned to 21 operations (100.00%), and
grade B was assigned to 0 (0%) in both groups. The difference between the two groups was not
statistically significant.
Qualified ERBL feasibility (grade A and B) was 100% in both groups (Table 4).
Page 10/16Table 4
Comparisons of ERBL Feasibility between Groups
Disposable Endoscope Reusable Endoscope P-
Group (n = 21) Group (n = 21) Value
Endoscopic flexibility, n (%)
A 16 (76.19%) 21 (100.0%) 0.057
B 5 (23.81%) 0 (0.0%)
Matching between endoscope and
ligating device, n (%)
A 21 (100.0%) 21 (100.0%) -
B 0 (0.0%) 0 (0.0%)
Acceptable clinical operability, n (%)
A 18 (85.71%) 21 (100.0%) 0.231
B 3 (14.29%) 0 (0.0%)
Image clarity, n (%)
A 18 (85.71%) 20 (95.24%) 0.599
B 3 (14.29%) 1 (4.76%)
Qualified ERBL feasibility, n (%)
Yes 21 (100.0%) 21 (100.0%) -
No 0 (0.0%) 0 (0.0%)
ERBL, endoscopic rubber band ligation
(2) Secondary outcome measures: Postoperative follow-up of therapeutic effect
In the disposable endoscope group, the number of cases regarded as 'cured' was 12 (57.1%), 'effective'
was 9 (42.9%), and 'invalid' was 0 (0%). In the reusable endoscope group, the number of cases regarded
as 'cured' was 13 (61.9%), 'effective' was 7 (33.3%), and 'invalid' was 1 (4.8%). The difference in
therapeutic effects between the two groups was not statistically significant (P = 0.611).
3.4 Cost counting
The total maintenance cost of reusable endoscope was 214.74RMB/case, including the cost of
endoscopic sterilization (183.15 ± 0.00) RMB, the cost of endoscopic repair (25.30 ± 0.00) RMB, and the
cost of endoscopic storage (6.29 ± 0.00) RMB, when the maintenance cost of disposable endoscope was
0.
Page 11/164. Discussion
Internal hemorrhoids are a group of soft veins formed by congestion in the varicose venous plexus above
the dentate line under the mucosa and anal skin at the lower end of the rectum [15]. Symptomatic internal
hemorrhoids mainly present as prolapse, bleeding, itching, and pain [16]. ERBL refers to endoscopic-
assisted ligation of hemorrhoids to create fibrosis of the rectal wall, which can prevent prolapse and
bleeding by reducing the blood flow into the haemorrhoidal venous plexus [17]. Guidelines for the
treatment of hemorrhoids in France [18] in 2016 and in America [18] in 2018 indicated that for patients
with grade I and II internal hemorrhoids and grade III internal hemorrhoids with mucosal prolapse, ERBL is
the first choice of treatment. This study is the first prospective randomised controlled trial comparing the
safety and clinical feasibility of disposable endoscope- and reusable endoscope-guided ERBL of internal
hemorrhoids.
Regarding safety, although the NEUT count on POD 1 in the disposable endoscope group (6.74 ±
2.03×10^9/L) was higher than in the reusable endoscope group and mildly exceeded the upper limit of
the normal range (6.3×10^9/L), the count returned to normal levels on POD 7, and no postoperative
infection was diagnosed in either group. While in-procedure stability of diastolic blood pressure in the
disposable endoscope group was slightly worse than in the reusable endoscope group, no life-threatening
events happened. These results suggest that the overall safety of disposable endoscopes is guaranteed.
It is worth mentioning that the hs-CRP level in one patient in the reusable endoscope group was extremely
high (75.68 mg/L) on POD 7, but no fever or severe anal pain were reported, and WBC and NEUT counts
were within normal ranges. This abnormal elevation of hs-CRP level may be due to the patient's history of
uraemia. The patient had a satisfactory therapeutic effect without adverse events, which implies ERBL
may be a good alternative for patients who cannot tolerate haemorrhoidectomy.
Although the gradings of image clarity and endoscopic flexibility of the disposable endoscopes were
lower than the reusable endoscopes (manifesting as a higher-grade B rate in the disposable endoscope
group), all patients in both groups underwent ERBL successfully. The feasibility rate of the disposable
endoscope was 100%. Additionally, follow-up on POD 30 revealed that more than half of subjects in both
groups reported that their symptoms of hemorrhoids were completely alleviated. These results indicate
that disposable endoscopes can provide a promising alternative for ERBL. However, image brightness,
sharpness, and contrast, as well as the curvature of the disposable endoscope, may require improvement
to meet the needs of accurate diagnosis and complex operation.
In this study, the EndoFresh® disposable endoscopes (XZING-W200B, HuiZhou Xzing Technology Co.,
Ltd) used with ERBL have two light-emitting diodes (LEDs) and a 110° view angle, which can clearly
identify the anorectal and dentate lines to confirm the location of ligation [16]. Additionally, the 10.8 mm
outer diameter insertion tube and 3.00 mm diameter instrument channel can fit with the Speedband®
multiple band ligation device. Moreover, ERBL is always performed when the endoscope is in a retroflexed
position [9, 19], and a 180° upwards bending angle is adequate for the ligation device to reach the
hemorrhoids.
Page 12/16Disposable endoscopes can be used directly after they are removed from the packaging and discarded
following the medical waste management principles after use [20], which can completely prevent cross-
contamination among patients especially amid the COVID-19 pandemic.
Compared with the reusable endoscope, the disposable endoscope does not need sterilization and repair
and is discarded after use, which saves the sterilization, repairing and storage cost for 214.74RMB/case.
The development history of disposable endoscopes shows that the product cost of disposable
endoscopes should be further reduced with the increase of production capacity in the future.
5. Conclusion
In conclusion, disposable endoscope can be an appropriate alternative in the ERBL of internal
hemorrhoids for similar safety and effectiveness to reusable endoscope. It can also save cost and time
for maintenance and storage. However, as this was a single-centre study, the number of patients was
small. The purpose of this study is to obtain real clinical use data through small sample of clinical use,
which can be used to guide large-scale clinical application of the product after marketing. A multi-centre
study with more patients and a longer period of follow-up are required in the future to guarantee the
feasibility of disposable endoscope use.
Declarations
Competing Interests: The authors have no relevant financial or non-financial interests to disclose.
Authors' contributions:
All authors contributed to the study conception and design. Wen Xu drafted the article, Guili Xia and Laihe
Li analysed and interpreted the data, Ge Cao and Xianhuan Yan put forward the conception, Ling Dong
designed the protocol, Ying Zhu was responsible for critical revision of the article for important
intellectual content and final approval of the article. All authors read and approved the final manuscript.
Acknowledgments
We thank Elsevier Language Editing Services for editing a draft of this manuscript.
Funding
No funding was received for conducting this study.
Conflict of interest
The authors have no relevant financial or non-financial interests to disclose.
References
Page 13/161. Chua, T., Kyanam Kabir Baig, K., Leung, F. et al. (2021) GIE Editorial Board top 10 topics: advances in
GI endoscopy in 2020. Gastrointest. Endosc. https://doi.org/10.1016/j.gie.2021.06.011
2. Mark, J., Underberg, K. and Kramer, R. (2020) Results of duodenoscope culture and quarantine after
manufacturer-recommended cleaning process. Gastrointest. Endosc. 91 (6), 1328-1333.
https://doi.org/10.1016/j.gie.2019.12.050
3. Bajolet, O., Ciocan, D., Vallet, C. et al. (2013) Gastroscopy-associated transmission of extended-
spectrum beta-lactamase-producing Pseudomonas aeruginosa. The Journal of hospital infection 83
(4), 341-3. https://doi.org/10.1016/j.jhin.2012.10.016
4. Donghoon, K., Chul‑Hyun, L., Myung‑Gyu, C. et al. (2019) An Operable, Portable, and Disposable
Ultrathin Endoscope for Evaluation of the Upper Gastrointestinal Tract. Digestive diseases sciences
64 (7), 1901-1907. https://doi.org/10.1007/s10620-019-5478-0
5. Luo, X., Ji, M., Zhang, S. et al. (2022) Disposable versus reusable gastroscope: a prospective
randomized non-inferiority trial. Gastrointest. Endosc. https://doi.org/10.1016/j.gie.2022.03.024
6. Makanjuola, A., Balogun, O., Osinowo, A. et al. (2020) Comparison of rubber band ligation with 3%
polidocanol injection sclerotherapy for the treatment of internal haemorrhoids at a Nigerian tertiary
hospital. Niger Postgrad Med J 27 (4), 311-316. https://doi.org/10.4103/npmj.npmj_232_20
7. Abiodun, A., Alatise, O., Okereke, C. et al. (2020) Comparative study of endoscopic band ligation
versus injection sclerotherapy with 50% dextrose in water, in symptomatic internal haemorrhoids.
Niger Postgrad Med J 27 (1), 13-20. https://doi.org/10.4103/npmj.npmj_128_19
8. Berkelhammer, C. and Moosvi, S. (2002) Retroflexed endoscopic band ligation of bleeding internal
hemorrhoids. Gastrointest. Endosc. 55 (4), 532-7. https://doi.org/10.1067/mge.2002.122618
9. Fukuda, A., Kajiyama, T., Arakawa, H. et al. (2004) Retroflexed endoscopic multiple band ligation of
symptomatic internal hemorrhoids. Gastrointest. Endosc. 59 (3), 380-4.
https://doi.org/10.1016/s0016-5107(03)02818-9
10. Goligher, J.C. (1980) Surgery of the Anus, Rectum and Colon. Ann. Surg. 192.
11. Bernal, J., Enguix, M., López García, J. et al. (2005) Rubber-band ligation for hemorrhoids in a
colorectal unit. A prospective study. Revista espanola de enfermedades digestivas : organo oficial de
la Sociedad Espanola de Patologia Digestiva 97 (1), 38-45. https://doi.org/10.4321/s1130-
01082005000100005
12. Chivate, S., Killedar, M., Ladukar, L. et al. (2022) Transanal Suture Mucopexy for Hemorrhoids.
Diseases of the colon rectum 65 (5), 742-749. https://doi.org/10.1097/dcr.0000000000002191
13. TC, H., RP, G., WJ, M. et al. (1992) CDC definitions of nosocomial surgical site infections, 1992: a
modification of CDC definitions of surgical wound infections. Am. J. Infect. Control 20 (5), 271-4.
https://doi.org/10.1016/s0196-6553(05)80201-9
14. Early, D., Lightdale, J., Vargo, J. et al. (2018) Guidelines for sedation and anesthesia in GI endoscopy.
Gastrointest. Endosc. 87 (2), 327-337. https://doi.org/10.1016/j.gie.2017.07.018
15. Jacobs, D. (2014) Clinical practice. Hemorrhoids. The New England journal of medicine 371 (10),
944-51. https://doi.org/10.1056/NEJMcp1204188
Page 14/1616. Schleinstein, H., Averbach, M., Averbach, P. et al. (2019) Endoscopic band ligation for the treatment of
hemorrhoidal disease. Arq. Gastroenterol. 56 (1), 22-27. https://doi.org/10.1590/s0004-
2803.201900000-15
17. Qureshi, W. (2018) Office management of hemorrhoids. Am. J. Gastroenterol. 113 (6), 795-798.
https://doi.org/10.1038/s41395-018-0020-0
18. Higuero, T., Abramowitz, L., Castinel, A. et al. (2016) Guidelines for the treatment of hemorrhoids
(short report). J. Visc. Surg. 153 (3), 213-8. https://doi.org/10.1016/j.jviscsurg.2016.03.004
19. Kovacs, T. and Jensen, D. (2019) Varices: Esophageal, Gastric, and Rectal. Clin. Liver Dis. 23 (4), 625-
642. https://doi.org/10.1016/j.cld.2019.07.005
20. Jin, P., Wang, X., Yu, D. et al. (2014) Safety and efficacy of a novel disposable sheathed gastroscopic
system in clinical practice. Journal of gastroenterology hepatology 29 (4), 757-61.
https://doi.org/10.1111/jgh.12482
Figures
Figure 1
Retroflexed endoscopic view of hemorrhoids before, during, and after endoscopic rubber band ligation (a-
c present disposable endoscopic view, d-f present reusable endoscopic view).
Page 15/16Figure 2
Difference between WBC, NEUT, and Hs-CRP at different times.
WBC, white blood cell count, NEUT, neutrophil count, Hs-CRP, hypersensitive C-reactive protein
Supplementary Files
This is a list of supplementary files associated with this preprint. Click to download.
video1withnarration.mp4
video2withnarration.mp4
Page 16/16You can also read