Encéphalites auto-immunes: données récentes - Romain Sonneville - Journee ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Encéphalites auto-immunes: données récentes
Romain Sonneville
Médecine Intensive - Réanimation
APHP, Hôpital Bichat Claude Bernard, Paris
Université de Paris, INSERM UMR1148
romain.sonneville@aphp.fr @romsonnevil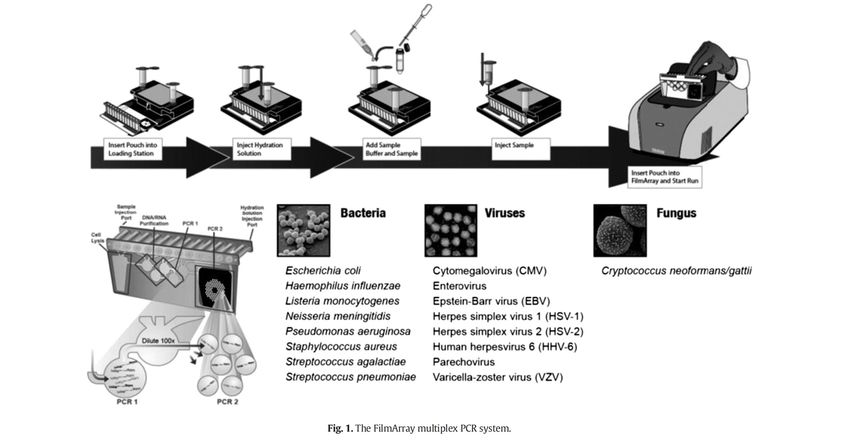
Conflicts of interest RS received grants from the French Ministry of Health, the French society of intensive care medicine (SRLF) and the European society of intensive care medicine (ESICM.
De quoi parle-t-on ? Epidémiologie et pronostic Prise en charge initiale Causes principales justifiant un traitement spécifique Pronostic à long terme Conclusion
Encephalitis
Inflammation Brain parenchyma
Causes Viral
Immune-mediated
Altered mental status +
Fever +
Meningism +/-
Focal signs +/-
Seizures +/-
Encéphalite aiguë
• MAJOR CRITERION : altered mental status lasting ≥24 h
(altered level of consciousness, lethargy or personality change)
• MINOR CRITERIA (at least 3 for probable or confirmed encephalitis)
– Fever >38°C (within 72H before or after presentation)
– New-onset seizures
– Focal sign(s)
– CSF pleocytosis : ≥ 5 cell/mm3
– Brain imaging findings consistent with encephalitis
– EEG alterations compatible with encephalitis
A. Venkatesan, Clin Infect Dis 2013
Encéphalite aiguë
CONFIRMED encephalitis
If there is…
– evidence of acute CNS infection with a microorganism associated with
encephalitis (CSF PCR)
OR
– laboratory evidence of an autoimmune condition associated with
encephalitis (Antibody testing in blood and CSF )
OR
– pathologic confirmation of brain inflammation (brain biopsy)
A. Venkatesan, Clin Infect Dis 2013
Encéphalite aiguë
CONFIRMED encephalitis
If there is…
– evidence of acute CNS infection with a microorganism associated with
encephalitis (CSF PCR)
OR
– laboratory evidence of an autoimmune condition associated with
encephalitis (Antibody testing in blood and CSF )
OR
– pathologic confirmation of brain inflammation (brain biopsy)
A. Venkatesan, Clin Infect Dis 2013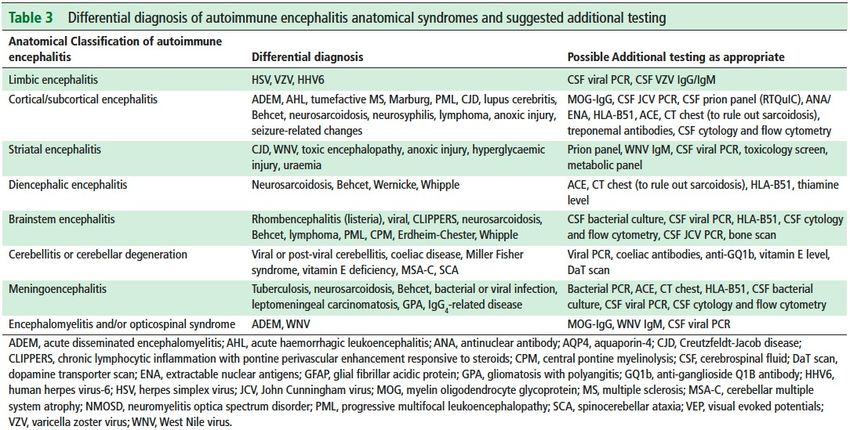
New Eng J Med 2018

Lancet Neurol 2016
J Neurol Neurosurg Psychiatry 2021
De quoi parle-t-on ? Epidémiologie et pronostic Prise en charge initiale Causes principales justifiant un traitement spécifique Pronostic à long terme Conclusion
203 patients
Adults > 16 yrs
18 months, 2008-2009
Infections 42% Unknown 37%
Immune-mediated 21%
J Granerod, Lancet Infectious Diseases 2010Cause
Figure 2: Age distribution of cases by cause
ADEM=acute disseminated encephalomyelitis. ANT=antibody-associated cause. HS
MTB=Mycobacterium tuberculosis. VZV=varicella zoster virus.
203 patients Immunocompetent Imm
Adults > 16 yrs patients* (n=172) pat
18 months, 2008-2009 Herpes simplex virus 37 (22%, 16–28) 1(
Acute disseminated encephalomyelitis 23 (14%, 9–19) ··
Antibody-associated encephalitis 15 (9%, 5–14) 1(
Mycobacterium tuberculosis 9 (5%, 2–10) 1(
Varicella zoster virus 4 (2%, 0·6–6) 6(
Streptococci 4 (2%, 0·6–6) ··
Enterovirus 3 (2%, 0·4–5) ··
Dual finding ·· 3(
Toxoplasma gondii ·· 2(
J Granerod, Lancet Infectious Diseases 2010Nationwide Inpatient Sample, 2000-2010, US hospitals,
n=238,567 patients
Incidence: 7.3 (95%CI 7.1-7.6) encephalitis
hospitalizations per 100,000 population
Unknown etiology 50% of cases
Among patients with identified etiology
- viral infections 48%
- autoimmune causes 33%
Average length of hospital stay: 11.2 days ICU admission 50%
Mortality: 5.6%
Plos One 2014Poor outcome25%
Eur J Neurol 2015De quoi parle-t-on ? Epidémiologie et pronostic Prise en charge initiale Causes principales justifiant un traitement spécifique Mesures symptomatiques Pronostic à long terme Conclusion
Epidemiological Clinical Diagnostic
data findings studies
Medical history Neurological signs BRAIN MRI with gd
Immunosuppression Optic nerve CSF (cultures, PCR)
Medications Extra-neurological signs EEG
Seasonal/epidemic context ? Serologies
Recent travel ? Immunology tests
Contacts:
animals +/- brain biopsy ? ?
Insects
Recent immunization
A. Venkatesan, Clin Infect Dis 2013J Neurol Neurosurg Psychiatry 2021
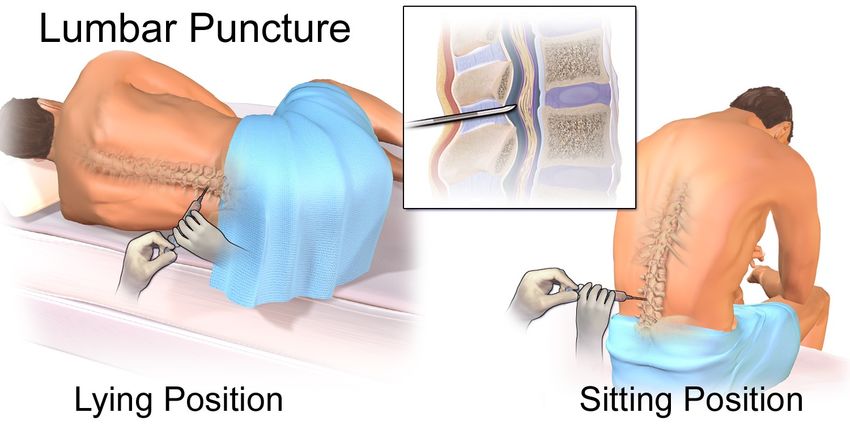
Recommandations SPILF 2017 Grade A : la quantité de LCS à prélever doit être d’au moins 120 gouttes (1ml =20 gouttes) 1ml pour biochimie 5 ml pour microbiologie (bactériologie +/- BK, virologie, mycologie….) Conserver LCS à +4°C puis à -80°C si possible
14 pathogens
in 1 hour !
J. Rhein, Diagn Microbiol Infect Dis 2015Unbiased metagenomic next-generation sequencing
Nature Review Neurol 2020Recommandations SPILF 2017 Grade A : si elle est possible, l’IRM cérébrale est l’imagerie à réaliser en première intention (Diffusion, FLAIR, T2*, T1 gadolinium)
Brain MRI patterns
« Grey » Normal « Limbic » « Demyelination »
Autoimmune encephalitis ?
SubmittedCortical /
Limbic subcortical Striatal
Diencephalic Brainstem Meningoencephalitis
J Neurol Neurosurg Psychiatry 2021J Neurol Neurosurg Psychiatry 2021
61 patients with autoimmune encephalitis Abnormal FDG-PET 52 (85%) patients, with 42/52 patients showing only hypometabolism
De quoi parle-t-on ? Epidémiologie et pronostic Prise en charge initiale Causes principales justifiant un traitement spécifique Mesures symptomatiques Pronostic à long terme Conclusion
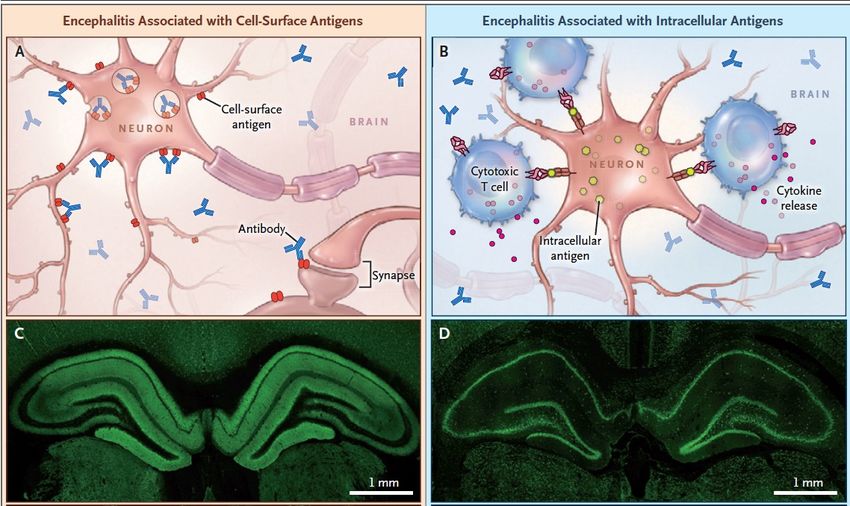
Anti-NMDA receptor encephalitis
• Encephalitis associated with CSF IgG antibodies against the GLuN1 subunit
of the NMDA receptor
• Good correlation between Ab levels and symptoms
• Associated with tumor (50%)
J Dalmau, Lancet Neurol 2011New Eng J med 2018
Variable N= 77 patients Variable N= 77 patients
Age, years 24 (20-31) Presence of tumor 36/76 (47)
Female sex 68/76 (89%) Delay between ICU 24 (14-51)
GCS, median (IQR) 11 (7-13) admission and tumor
resection, median (IQR)
Seizures / status epilepticus 30 (76%) days
CSF WBC, n / mm3 36 (9-112)
CSF protein levels, g/l 0.4 (0.3-0.6)
Normal CT scan 49/62 (95%)
Normal brain MRI 56 / 75 (75%)
Am j Resp Crit Care Med 2017Variable N= 77 patients
Delay between ICU admission and immunotherapy, 8 (2-16)
median (IQR) days
First-line immunotherapy
Steroids 61/74 (82%)
IVIg 71/74 (89%)
Plasma exchange 17/74 (23%)
Second-line immunotherapy
Cyclophosphamide 6/45 (13%)
Rituximab 24/45 (53%)
Both 15/45 (33%)
Am j Resp Crit Care Med 2017N=1552 patients from 652 articles 1105/1508 female patients (73%) 707/1526 aged < 18 years (46%) Median age at onset: 20 (0-85) years 389/1524 patients (25.6%) had a tumor (ovarian tumor 324/1524 (21%)) ICU admission : 488/964 (50.6%)
Immune-mediated relapsing symptoms (
Median 39 (26–43) days after onset of encephalitis
Behavioral symptoms
Status epilepticus
MRI : new contrast enhancement
CSF : antibodies against NMDAR +
=> Dramatic improvement following immunotherapy
T Armangue, Neurology 2015• 51 patients with HSV encephalitis, Spain, 2014-2017
• Autoimmune encephalitis occurred in 14/51 (27%) patients
• It was associated with development of neuronal antibodies and usually
presented within 2 months after treatment of herpes simplex encephalitis.
Lancet Neurology 2018Intensive Care Medicine 2019
Lancet Neurol 2020
Nationwide surveillance study of acute
neurological
and psychiatric complications of COVID-19 Other n=3: 2%
N=135 patients
PNS n=6: 5%
Encephalopathy n=39: 31%
Stroke n=77: 62%
Confirmed encephalitis n=7
Acute ischemic stroke n=57
Neuro-psychiatric symptoms n=32
ICH n=9
Vasculitis n=1
Other n=10
Lancet Psychiatry 2020N=222 patients PNS
9% Ischemic stroke
Encephalitis
13%
36%
Encephalopathy
42%
Clinical Microbiology and Infection 2020Mutiple, large > 2cm abnormalities on T2-weighted imaging
Non-severe presentation = sequential therapy
No improvement ?
High dose
IVIg or PLEX
corticosteroids
Or IgIV or PLEX if steroids IVIG first if agitation or bleeding disorders
contraindicated PLEX first if hyponatremia, high risk of thrombosis, or
brain/spinal demyelination
J Neurol Neurosurg Psychiatry 2021Severe presentation* = combination therapy
*severe NMDARE, refractory status epilepticus, severe dysautonomia …
FIRST LINE No improvement ? SECOND LINE
High dose
Rituximab
corticosteroids
OR
+
Cyclophosphamide
IgIV or PLEX
IVIG first if agitation or bleeding disorders Rituximab in known or highly suspected antibody-
PLEX first if hyponatremia, high risk of mediated immunity (e.g. NMDARE)
thrombosis, Cyclophosphamide in case of cell-mediated
or brain/spinal demyelination immunity (classical paraneoplastic syndromes)
J Neurol Neurosurg Psychiatry 2021N=290 patients with encephalitis, Bichat medical ICU, Paris, France
Convulsive status epilepticus = 20%
Immune-mediated 12 29
HSV-1 11 29
Undetermined 21 72
VZV 2 12
Bacterial 10 82
0% 20% 40% 60% 80% 100%
Status epilepticus No status epilepticus
Medicine 2016RCT, IVIg versus placebo, n=17 adult patients
De quoi parle-t-on ? Epidémiologie et pronostic Prise en charge initiale Causes principales justifiant un traitement spécifique Pronostic à long terme Conclusion
100
90
80
100 mRS
70 90 6
5
% of patients
80
60 mRS 4
70 6
5
3
% of patients
50 60 4 2
3
50 2 1
1
0
40 40
0
30
30 20
10
20
0
M3 M6 M9 M12 M18 M24
10
Number 76 76 70 74 57 56
of patients
0
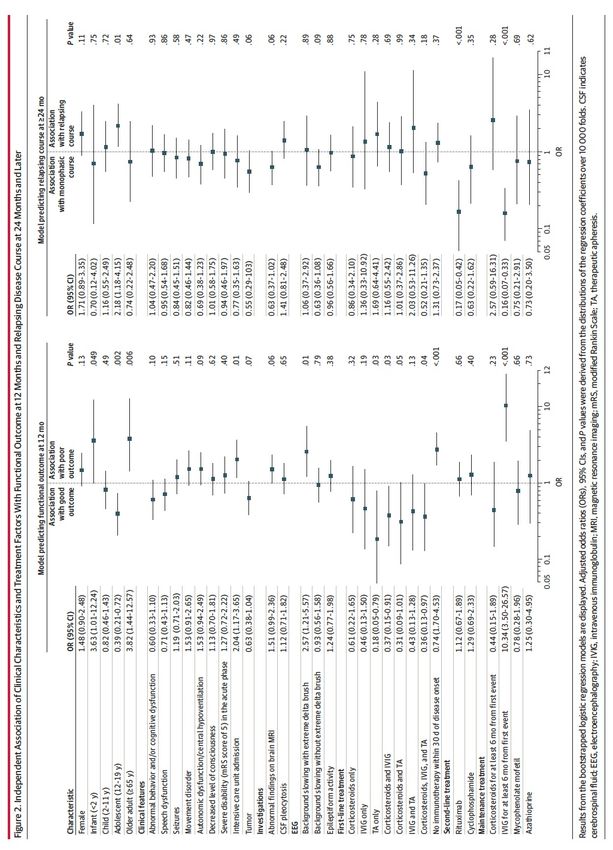
M3 M6 M9 M12 M18 M24 Am j Resp Crit Care Med 2017Multivariate analysis of factors of good neurological outcome at 6 months (mRS < 2)
n= 76 ICU patients
*before ICU admission or following 8 days of ICU admission Am j Resp Crit Care Med 2017Neurology 2019
Neurol Neuroimmunol Infl 2019
Aug 202
Encephalitis in Intensive Care Pronostic à long terme des encéphalites en réanimation (Encephalitica, PHRC-IR 2015) Cohorte prospective multicentrique 50 centres de réanimation en France Inclusion: Toute ME à LCR « clair » + GCS < 14 Biobanking (LCR, plasma): J0, J14 350 patients CJP: mRankin J90 inclus
The EURopean study on Encephalitis in intensive CAre units
The “EURECA” study
Epidemiology and outcomes of all-cause encephalitis in the ICU
Clinicaltrial.gov registration : NCT03144570
ESICM endorsement ✔
ESICM grant : Established investigator award 2017 ✔
Study status : completed
599 patients
romain.sonneville@aphp.fr included !De quoi parle-t-on ? Epidémiologie et pronostic Prise en charge initiale Causes principales justifiant un traitement spécifique Pronostic à long terme Conclusion
Encéphalites …
• Un syndrome neurologique aigu associé à une morbi-mortalité significative
• Causes dysimmunitaires 20%
• Evaluation multimodale précoce
• Neurologique : IRM, EEG, Immunologie LCS – sang, PET scan
• Générale : bilan néoplasique
• Immunothérapie précoce combinée d’emblée dans les formes sévères
(corticoïdes + IgIV ou PLEX)
• Suivi à long terme ++Lancet 2019
Merci J !
Acknowledgment
Bichat Claude Bernard university hospital NeuroID consortium staff members, Bichat
Intensive care medicine staff members Pr. Y Yazdanapanah
Pr. X. Lescure
INSERM U1137, CHU Bichat Paris Dr N. pfeiffer Smadja
Dr. E de Montmollin Dr J. Savatowsky
Dr. C. Dupuis
Prof. L Bouadma U1124, CHU PURPAN Toulouse
Prof. JF Timsit Dr. B. Sarton
Prof. S. Silva
INSERM U1148, CHU Bichat
M Cantier ICUREsearch
C Legouy S. Ruckly, Q. Staquly
T Rambaud Dr. C. Féger
Prof. N Kubis
Prof. N Ajzenberg Saint Denis hospital
Prof. M Mazighi Dr. P. JaquetYou can also read