Elevated HCG and retroperitoneal adenopathy after clomiphene therapy for infertility
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Case report
Elevated HCG and retroperitoneal adenopathy after
BMJ Case Rep: first published as 10.1136/bcr-2022-249766 on 26 April 2022. Downloaded from http://casereports.bmj.com/ on July 1, 2022 by guest. Protected by copyright.
clomiphene therapy for infertility
Raj Vikesh Tiwari ,1 Maria Di Jiang,2 Keith Jarvi,3 Robert Hamilton4
1
Urology, University of Toronto, SUMMARY enlarged retroperitoneal nodes with the largest
Toronto, Ontario, Canada In the context of an elevated human chorionic measuring 18 mm at the left para- aortic region.
2
Medical Oncology, Princess gonadotropin (HCG) with enlarged retroperitoneal nodes There were smaller nodes at precaval and retro-
Margaret Hospital Cancer caval region ranging from 7 to 8 mm (figure 1). It
and absent testicular tumours, clinicians will consider a
Centre, Toronto, Ontario,
diagnosis of extragonadal germ cell tumours. We report was noted that the nodes appeared to have signif-
Canada
3
Division of Urology, Sinai the case of a man in his thirties who while on treatment icant fat content. There was no prior imaging for
Health System, Toronto, Ontario, for subfertility with clomiphene citrate was noted to have comparison. The adrenal glands were normal bilat-
Canada enlarged retroperitoneal nodes and elevated HCG levels erally. The patient was promptly referred to the
4
Division of Urology, University of 75 IU/L. Chemotherapy with bleomycin, etoposide multidisciplinary testicular cancer clinic and clomi-
Health Network, Toronto, and cisplatin originally planned was deferred when two phene was discontinued.
Ontario, Canada separate retroperitoneal nodal biopsies returned as At the testicular cancer clinic, tumour markers
benign fibroadipose tissue and HCG levels spontaneously were repeated demonstrating elevated HCG of
Correspondence to down-trended to 4 IU/L within 4 months of clomiphene 75 IU/L and normal alpha fetoprotein of 4.8 UG/L
Dr Raj Vikesh Tiwari; and lactate dehydrogenase of 195 U/L. Hormonal
citrate discontinuation. Follow-up imaging revealed
raj.tiwari@u hn.ca
regression of the retroperitoneal nodes. panel revealed elevated testosterone of 39.1 nmol/L
and suppressed FSH and LH levels of 0.1 IU/L. CT
Accepted 17 April 2022
of the chest revealed no metastasis. Ultrasound of
the testes performed revealed normal sized testes
BACKGROUND
bilaterally and while no discrete tumours were
We believe this case emphasises that a closer inter-
noted, extensive microlithiasis was observed on
rogation of tumour marker trends, nodal imaging
the right side and felt could be in keeping with an
characteristics and retroperitoneal nodal histology
Azzopardi lesion of burnt out tumour (figure 2).
is necessary prior to planning chemotherapy in
His case was reviewed at our Multidisciplinary
similar patients with human chorionic gonado-
germ cell tumour rounds and it was felt he likely
tropin (HCG) elevation on clomiphene citrate (CC).
had a germ cell tumour. In line with European
Association of Urology guidelines2 for stage IIA
CASE PRESENTATION good risk non- seminomatous germ cell tumours
We present a 37-year-old man with no prior signif- counselling was performed for three cycles of
icant medical or surgical history who presented bleomycin, etoposide and cisplatin chemotherapy.
with secondary subfertility. He had 1 live birth However, prior to proceeding, in view of the atyp-
3 years prior followed by two miscarriages, and ical nodal imaging findings a percutaneous biopsy
despite trying to conceive for over 1 year was of the largest left para-aortic node was performed.
unsuccessful. He was a 6 pack- year smoker and Histology returned as fibroadipose tissue with no
discontinued smoking 7 years prior to presentation. malignancy seen. Additionally, his HCG levels had
Physical examination revealed bilateral normal dropped down to 9 IU/L by 2 months after stopping
sized descended testicles and normal secondary clomiphene. This prompted a decision to defer the
sexual characteristics. Blood investigations related chemotherapy and continue surveillance.
to subfertility revealed elevated testosterone of
42.1 nmol/L and low follicle stimulating hormone
OUTCOME AND FOLLOW-UP
(FSH) and luteinising hormone (LH) levels of
A further 2 months later, his HCG had dropped
0.1 IU/L, respectively. Semen analysis parameters
to 4 IU/L. CT imaging revealed the retroperitoneal
revealed volume of 3.8 mL (normal >1.5 mL),
nodes to be regressing slightly with the largest now
motility of 47% (normal >32%) and sperm concen-
measuring 14 mm (figure 3). A repeat CT-guided
tration of 3.45 million per mL (normal 15 million/
percutaneous biopsy redemonstrated fibroadi-
mL).1 In view of low FSH, LH levels and reduced
pose tissue with no malignancy noted. The patient
sperm concentration the patient was started on CC
remains well and asymptomatic. Tumour markers
at 25 mg every 2 days for 3 months. HCG testing
© BMJ Publishing Group will be monitored again in 3 months’ time with
Limited 2022. No commercial was not performed prior to initiation of CC as it is
interval imaging 6 months later. Table 1 illustrates
re-use. See rights and not routine to do so.
the trend of tumour markers.
permissions. Published by BMJ. After 2 months of therapy blood investigations
revealed that testosterone had risen to 828 nmol/L
To cite: Tiwari RV,
Di Jiang M, Jarvi K, et al. BMJ with both FSH and LH remaining suppressed. DISCUSSION
Case Rep 2022;15:e249766. HCG was elevated at 35 IU/L and CT scans of CC is a selective oestrogen receptor modulator
doi:10.1136/bcr-2022- the abdomen and pelvis performed to asses for that occupies oestrogen receptors in the hypothal-
249766 contributary adrenal abnormalities instead revealed amus and pituitary leading to gonadotropin release
Tiwari RV, et al. BMJ Case Rep 2022;15:e249766. doi:10.1136/bcr-2022-249766 1
Case report
BMJ Case Rep: first published as 10.1136/bcr-2022-249766 on 26 April 2022. Downloaded from http://casereports.bmj.com/ on July 1, 2022 by guest. Protected by copyright.
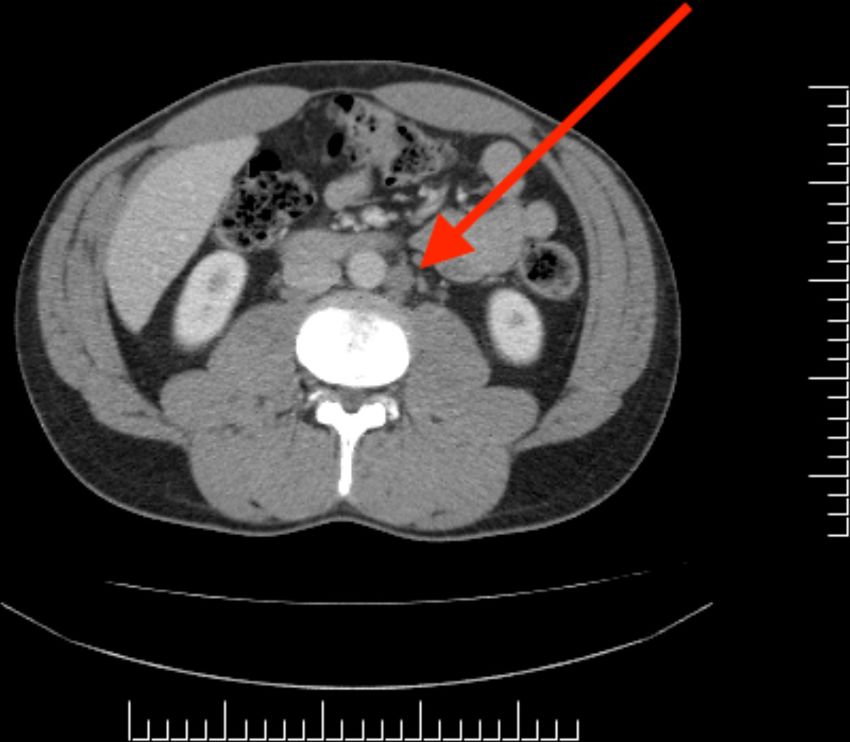
Figure 1 CT showing an enlarged fatty appearing para-aortic Figure 3 CT showing the same para-aortic retroperitoneal lymph
retroperitoneal lymph node measuring 18 mm at initial diagnosis (red node regressing to 14 mm after stoppage of clomiphene citrate (red
arrow). arrow).
which leads to increased testicular stimulation, spermatogenesis
and testosterone production.3 CC is used from 1960 for ovula- trophoblastic malignancies and germ cell tumours of both the
tion induction in women. It has been used off-label for men in testis and ovary. A short half-life of 36 hours makes it a useful
subfertility and hypogonadism as the US Food and Drug Admin- prognostic biomarker. In testicular cancer, HCG elevations are
istration did not approve the medication, because of unclear seen in 40%–50% of patients with non-seminomatous germ cell
effectiveness.4 In a systemic review and meta-analysis of men on tumours and 15%–20% of seminomatous germ cell tumours.6
CC for hypogonadism, Huijben et al5 reported the side effects Elevations of HCG have also been also rarely reported in several
of CC to be seen in 4%–11% of patients ranging from mood non-trophoblastic tumours such as carcinomas of the pancreas,
changes, blurred vision, breast/nipple tenderness and fatigue. breast, bladder, prostate and neuroendocrine tumours.7 Beyond
HCG is a glycoprotein produced by trophoblastic tissues its role in diagnostics, HCG is also used for treatment of hypo-
and its identification is most commonly clinically used for the gonadism while maintaining fertility. The exogeneous adminis-
diagnosis of pregnancy, where it chiefly acts to promote proges- tration of HCG has increasingly been used as a popular weight
terone release. HCG is also expressed in both trophoblastic loss drug either by intramuscular injection or via oral ingestion
and non- trophoblastic human malignancies and plays a role despite there being no evidence proving its efficacy.8 Other
in cell transformation, angiogenesis, metastasis and immune factors leading to potential spurious HCG elevations include
escape thereby contributing to cancer progression. Its role as a marihuana intake,9 illicit substance use10 and iatrogenic hypogo-
tumour marker is crucial for clinical management of gestational nadism after orchiectomy for germ cell tumours.11 In the case of
our patient, thorough investigations did not yield any potential
cause of the HCG elevation.
In retrospect, the presence of retroperitoneal nodal enlarge-
ment acted as a red-herring. An important lesson for us was to
prioritise atypical imaging characteristics (fatty appearance) and
slow growth rate as features pointing against malignancy. This
was important as it made us proceed with a biopsy first approach
instead of chemotherapy first, which ultimately provided a
benign diagnosis. We do recognise the inherent limitations of
biopsy sensitivity, however with two separate biopsies spread
over 2 months the accuracy is enhanced. Also, we found that
Table 1 Biochemical and clinical progress
Date HCG (IU/L) Clinical progress
July 2021 Not checked Started on CC
September 2021 35 Para-aortic node on imaging
October 2021 75 Staging at testis multidisciplinary clinic. CC
discontinued. First node biopsy
Figure 2 Ultrasound right testis showing widespread testicular December 2021 9 Second node biopsy
calcifications in keeping with impression of Azzopardi lesion (burnt out January 2022 4 Para-aortic node regression on imaging
testicular tumour). CC, clomiphene citrate; HCG, human chorionic gonadotropin.
2 Tiwari RV, et al. BMJ Case Rep 2022;15:e249766. doi:10.1136/bcr-2022-249766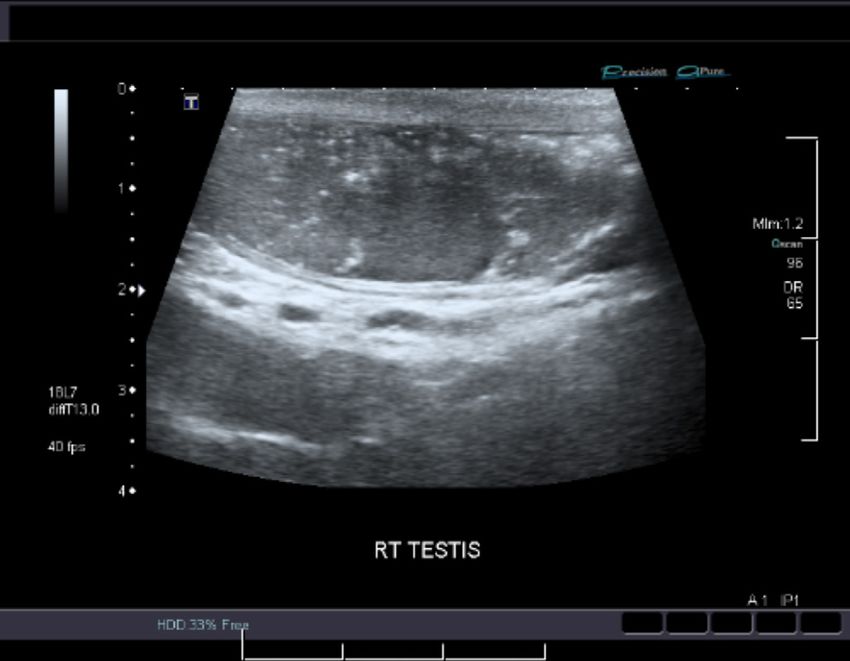
Case report
bringing the case for discussion at our multi-disciplinary testic- Funding The authors have not declared a specific grant for this research from any
BMJ Case Rep: first published as 10.1136/bcr-2022-249766 on 26 April 2022. Downloaded from http://casereports.bmj.com/ on July 1, 2022 by guest. Protected by copyright.
ular cancer rounds (attended by urologists, medical oncologists, funding agency in the public, commercial or not-for-profit sectors.
radiation oncologists, radiologists and pathologists) provided Competing interests None declared.
more thorough discussion and scrutiny of the images facilitating Patient consent for publication Consent obtained directly from patient(s).
better clinical decision making. Provenance and peer review Not commissioned; externally peer reviewed.
As far as we know in the current literature, this is the first
Case reports provide a valuable learning resource for the scientific community and
case report of possible HCG elevation related to CC use and can indicate areas of interest for future research. They should not be used in isolation
its subsequent decrease with discontinuation. We do recognise to guide treatment choices or public health policy.
the limitation of not having a pre-CC treatment HCG level as a
baseline to compare with. Looking back, the elevation of testos-
ORCID iD
terone pre-CC may have been explained by pre-existing HCG
Raj Vikesh Tiwari http://orcid.org/0000-0003-3893-5859
elevations, but this would still not provide explanations for the
HCG drop later on. While there is no evidence so far linking the
two the significant decrease in HCG levels with CC withdrawal REFERENCES
in the absence of any other treatment is notable and warrants 1 Cooper TG, Noonan E, von Eckardstein S, et al. World Health organization reference
further studies. values for human semen characteristics*‡. Hum Reprod Update 2010;16:231–45.
2 Albers P, Albrecht W, Algaba F. European association of urology guidelines on
testicular cancer. Eur Urol 2011;60:304–19.
Learning points 3 Surampudi P, Swerdloff RS, Wang C. An update on male hypogonadism therapy.
Expert Opin Pharmacother 2014;15:1247–64.
► Human chorionic gonadotropin elevation in patients on 4 Wheeler KM, Sharma D, Kavoussi PK, et al. Clomiphene citrate for the treatment of
clomiphene citrate with concomitant enlarged retroperitoneal hypogonadism. Sex Med Rev 2019;7:272–6.
nodes requires closer assessment, which may allow the 5 Huijben M, Lock MTWT, de Kemp VF, et al. Clomiphene citrate for men with
hypogonadism: a systematic review and meta-analysis. Andrology 2022;10:451–69.
avoidance of unnecessary chemotherapy and its various 6 Mann K, Saller B, Hoermann R. Clinical use of hCG and hCG beta determinations.
morbid side effects. Scand J Clin Lab Invest Suppl 1993;216.
► Retroperitoneal nodal biopsies are a prudent diagnostic 7 Sisinni L, Landriscina M. The role of human chorionic gonadotropin as a tumor marker
strategy in cases of diagnostic doubt. : biochemical and clinical aspects. Advances in cancer biomarkers;867:159–76.
8 Olsen TG, Barnes AA, King JA. Elevated HCG outside of pregnancy--diagnostic
► Multidisciplinary rounds are essential in providing improved
considerations and laboratory evaluation. Obstet Gynecol Surv 2007;62:669–74.
care for patients with indeterminate clinical picture. 9 Garnick MB. Spurious rise in human chorionic gonadotropin induced by marihuana in
patients with testicular cancer. N Engl J Med 1980;303:p177.
10 Lehikoinen A, Voutilainen R, Romppanen J, et al. The effect of maternal alcohol and
Twitter Raj Vikesh Tiwari @drrajvtiwari drug abuse on first trimester screening analytes: a retrospective cohort study. BMC
Contributors RVT the clinical fellow summarised the case, reviewed the images Pregnancy Childbirth 2020;20:562.
and was the primary author under the supervision of MDJ, KJ and RH who are 11 Germa JR, Arcusa A, Casamitjana R. False elevations of human chorionic
managing staff medical oncologists and urologists who assisted with revision of the gonadotropin associated to iatrogenic hypogonadism in gonadal germ cell tumors.
manuscript. Cancer 1987;60:2489–93.
Copyright 2022 BMJ Publishing Group. All rights reserved. For permission to reuse any of this content visit
https://www.bmj.com/company/products-services/rights-and-licensing/permissions/
BMJ Case Report Fellows may re-use this article for personal use and teaching without any further permission.
Become a Fellow of BMJ Case Reports today and you can:
► Submit as many cases as you like
► Enjoy fast sympathetic peer review and rapid publication of accepted articles
► Access all the published articles
► Re-use any of the published material for personal use and teaching without further permission
Customer Service
If you have any further queries about your subscription, please contact our customer services team on +44 (0) 207111 1105 or via email at support@bmj.com.
Visit casereports.bmj.com for more articles like this and to become a Fellow
Tiwari RV, et al. BMJ Case Rep 2022;15:e249766. doi:10.1136/bcr-2022-249766 3You can also read

















































