Dr Bryan Betty General Practitioner Porirua Union and Community Health Service East Porirua
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Dr Bryan Betty
General Practitioner
Porirua Union and Community Health Service
East Porirua
14:00 - 14:55 WS #138: Biologics and Biosimilars: Why should GP’s be interested?
15:05 - 16:00 WS #150: Biologics and Biosimilars: Why should GP’s be interested? (Repeated)
Biologics and Biosimilars: why GP’s should be interested Dr Bryan Betty, Deputy Medical Director, PHARMAC G.P. East Porirua

Overview • Global National Context • What are Biologics and Biosimilars? • GP’s: Specific Issues • Summary

The funding environment

Bang for the buck
Health care wants will always exceed resources available…
Demand
Ability
to pay
… so choices need to be made
PHARMAC’s role
“To secure for eligible people in need of pharmaceuticals, the best
health outcomes that can reasonably be achieved, and from within
the amount of funding provided.”
Note: ‘pharmaceuticals’ = medicine, therapeutic medical device, related product or related thing
Our principles:
• The budget is capped: approx. $800 million
• There is an opportunity cost to every decision
• Nationally consistent and equitable access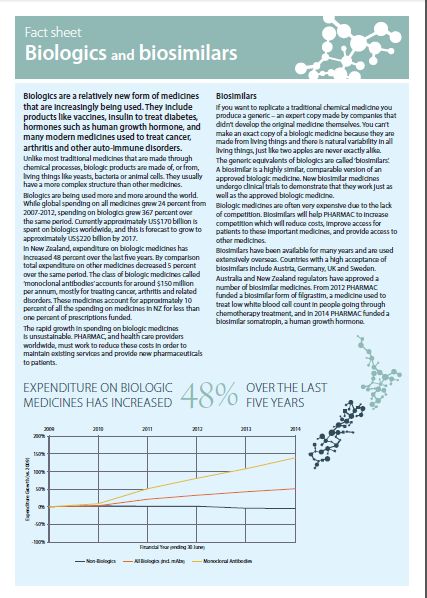
Working to a Fixed Budget
PHARMAC’s management model
New Medicines
Savings Competition
re-investment in the sector e.g. Generics
PHARMAC’s long-term impact
22.7m 41.8mBiologics Challenge
The promise of biologics……
• Biologics have had a profound effect health through
treatment of many diseases
• Primarily rheumatology, inflammatory conditions and oncology
• Filgrastim, pegfilgrastim, erythropoetin, somatropin, insulins
• Adalimumab, etanercept, rituximab, trastuzumab (‘mAbs’)
• Potential for wide application across a range of diseases
• Anti-TNF inhibitors for inflammatory conditions :
Rh.A, psoriasis, IBDControlling Rheumatoid Arthritis
Thermal imaging of hand and ..and after Mab therapy
elbow joints before……
http://users.ox.ac.uk/~path0116/tig/new1/thefg.gifChallenges of biologics
International Expenditure NZ Expenditure Growth
Major growth area in
healthcare
• Global spend on all medicines
grew 24% from 2007-2012
• Biologics spend grew 367%
over the same time period
• Global biologics sales forecast to
grow to US$220 billion by 2017
• Source The Global Use of Medicines: Outlook through 2017.
Report by the IMS Institute for Healthcare Informatics .Growth in biologics in NZ is unsustainable…..
Top 20 CPB funded meds by cost
• 2500 Meds
funded
• These 20 meds
1/3 total budgetThe Challenge…
Biologics are the fastest growing category of medicines in NZ
48% increase over the last five years
Monoclonal antibodies (mAbs) largest and fastest growing segment
Approx. 10% of total NZ medicines expenditureCompetition for biologics is needed
+
= =
More Lower Increasing
competition Prices valueThe good news is many biologic patents have expired or are nearing
expiration…
2013 global
Brand name Active sales Patent expiry
Treatment
(Supplier) ingredient (US$ EU/US
billion)
MabThera (Roche) rituximab Arthritis, NHL 8.6 Nov 2013/Dec 2018
Herceptin (Roche) trastuzumab Breast cancer 6.8 Jul 2014/Jun 2019
insulin
Lantus (Sanofi) Diabetes 7.8 2014/2014
glargine
Remicade (Janssen) infliximab Arthritis 8.9 Aug 2014/Sep 2018
Enbrel (Pfizer) etanercept Arthritis 8.3 Feb 2015/Nov 2028
Neulasta (Roche) pegfilgrastim Neutropenia 4.4 Aug 2017/Oct 2015
Humira (Abbvie) adalimumab Arthritis 10.7 Apr 2018/Dec 2016
Avastin (Roche) bevacizumab Cancer 7 Jan 2022/Jul 2019
….opportunities for competition and lower pricesWhat are Biologics and Biosimilars?
Biopharmaceuticals aka “Biologics”
Produced by, or extracted from, living organisms(as opposed to
synthesized chemical process)
Many made using recombinant DNA technology in bacteria,
yeast or mammalian cells
• hormones : insulin, growth hormone
• monoclonal antibodies: autoimmune diseases (Rh.A, Psoriasis, IBD)
and cancers
• blood products: haemophilia
• immunomodulators :multiple sclerosis
• vaccinesBiologics are inherently variable
Variability is natural in biologic systems
genetics + environment
Variation in itself is not necessarily an issue:
The key is determining the clinical consequences, if any, of known (and
unknown) variation
• Potential consequences of
variation
• None
• Loss of efficacy
• Enhancement of efficacy
• Safety
• ImmunogenicityGenerics versus Biologics/Biosimilars
• Innovator small molecules vs. generics
• Chemically synthesized to identical molecular structure
• Innovator biologics vs. Biosimilars
• Both made in living systems therefore have inherent variability
• Micro- heterogeneity: small differences between batches.
• Applies to both biologics and biosimilars
• Regulatory process: Different pathway, extensive evidence
required biosimilarsWhat is a Biosimilar?
Herd 1 Herd 2
A Glass of Milk
‘Biosimilar’Biologics and Biosimilars
“Biosimilars” must be highly similar to an originator reference
product.
• Not better, or worse to the originator product
Biosimilars must demonstrate comparable quality, safety and
efficacy to an approved reference biologic
• No clinically meaningful differences
Natural variability means exact copies can’t be made
• Even original biologics being used today are different form their first
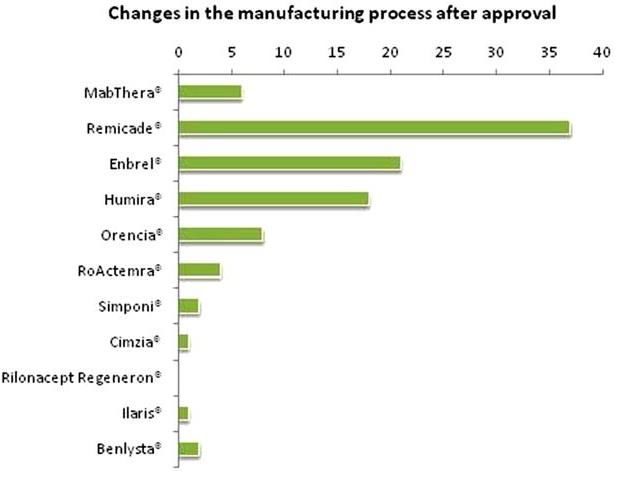
batchVariability of Innovator Biologics
Changes include:
Change in supplier of cell culture media
New purification methods
New manufacturing sites
Changes for innovator molecules 37 changes
approved by comparability exercise – for infliximab
rarely require clinical trials
“ the medicine that a clinician administers to a patient today is not ‘identical’ (but
comparable) to the medicine authorised years ago”
“no batch of any reference product is ‘identical’ to the previous one - ‘non-
identicality’ is a normal feature of biotechnology”
From Schneider C K Ann Rheum Dis 2013;72:315-318Variability of biologics and biosimilars
Acceptable for biologic
Not Acceptable
Acceptable for biosimilar
Biosimilars fall within the ‘goal posts’ of the original biologics’
quality variation
McCamish, M and Woollett, G. mAbs (March/April 2011) 3:2, 209-217Biologics and Biosimilars
• Unlike the original biologics Phase III studies the aim of biosimilar clinical trials is not
to prove benefit of treatment per se to patients.
• It is to prove biosimilarity to the original biologic
• Intended to be clinically equivalent.Biosimilar development Pathway
Comprehensive and thorough
• More extensive and complex than for generic medicines
Head-to-head studies with the original biologic medicine
Pre clinical data:
comparable analytics and manufacturing
Clinical data :
• Phase I
• Comparable PK & PD
• Phase III
• Comparable quality, efficacy and safety
• Phase IV
• Post approval risk-management planG.P Issues
Immunogenicity
All biologics and biosimilars, confer a risk of immunogenicity
Neutralizing antibodies (anti-drug antibodies)
• Loss of efficacy e.g. infliximab 17-60%, often methotrexate co-
prescribed
• Anaphylaxis (rare) , Red Cell Aplastic Anaemia(1990’s) erythropoietin
Regulators require extensive data for biologics and biosimilars to assess
risk of immunogenicity
Ongoing real world pharmacovigilance undertaken for biologics and
biosimilars to assess any potential rare reactionsSpecific GP clinical issues with biologics/biosimilars
1. Issues with biosimilars same as for original biologic
(Variability)
2. Majority of mAb biologics in GP practice are
immunomodulatory (Inflammatory disease)
Anti-TNFs adalimumab (Humira) , etanercept (Enbrel)
Rheumatoid arthritis, Psoriasis, Crohn’s Disease, Ulcerative Colitis
3. Initial specialist Rx, follow-up scripts GP’s.Specific GP clinical issues with biologics/biosimilars
1. Contraindicated in patients with :
severe active infections including sepsis, active tuberculosis,
opportunistic infections
2. Caution in patients with:
active infections: including chronic or localised infections until infections
are controlled.
patients who have been exposed to tuberculosis,
Hepatitis B virus (HBV) infection, (reactivation can been fatal)
moderate to severe alcoholic hepatitis
moderate to severe heart failure (NYHA class III/IV).
Malignancy within 5 yearsSpecific GP clinical issues monitoring
1. Develop serious infection: Prompt action contact specialist
2. Heart failure developing or worsening with mild CCF
3. Interstitial lung disease - dry cough, increase SOB
4. Periodic skin exam for non - melanoma skin cancers
5. Vaccination prior to commencing, avoid live vaccines during
treatment (MMR, varicella, BCG)
6. Not proven in pregnancy: Contraception
7. Surgery with-held
8. Bloods may Include: FBC (cytopenias), CRP, LFT
9. Long term: Lymphoma risk (2-2.5* risk)PHARMAC and Biologics
PHARMAC’s Work on Biosimilars
Drugs Change in Cost and Access
• Filgrastim / Pegfilgrastim
• Somatropin
Total Drug Cost
• Erythropoietin
• Infliximab
• Insulin Glargine
• Adalimumab/Etanercept Number of PatientsCreating competition: filgrastim
“The introduction of lower cost biosimilar filgrastim and the subsequent price reduction on
pegfilgrastim means we use fewer hospital resources and deliver optimal chemotherapy
more safely to more women with breast cancer.”
Dr Richard Isaacs, Medical Oncologist, Palmerston NorthSummary
G.P’s: Biologics and Biosimilars
• Increasingly important in General Practice
• G.P’s will have patients on biologics, and biosimilars into the future. :
• Increasingly see patients on these medications and expected to review:
(Esp: Rh.A., Psoriasis, IBD)
• Biosimilar not generic versions of biological medicines.
• Biologics/Biosimilar using living systems : inherently variable
• Biosimilars comparable safety and efficacy to biologicsG.P’s: Biologics and Biosimilars
• Trials need to demonstrate: Comparable, Quality, Efficacy, Safety.
• Immunogenicity and micro-heterogenicity important concepts.
• Neutralizing anti-bodies
• Adverse Events: reported to CARM
• Monitoring: Serious infection developing, CCF, interstitial lung, non-
melanoma skin ca, vaccinations. (Fluvax), pregnancy, surgery.Questions
More Information www.pharmac.govt.nz www.bpac.org.nz
You can also read