ONLINE TRAININGS FOR GENERAL PRACTITIONERS TREATMENT OPTIONS ON COVID-19 - a collaboration between - RKI
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
ONLINE TRAININGS
FOR GENERAL PRACTITIONERS
TREATMENT OPTIONS ON COVID-19
a collaboration between
1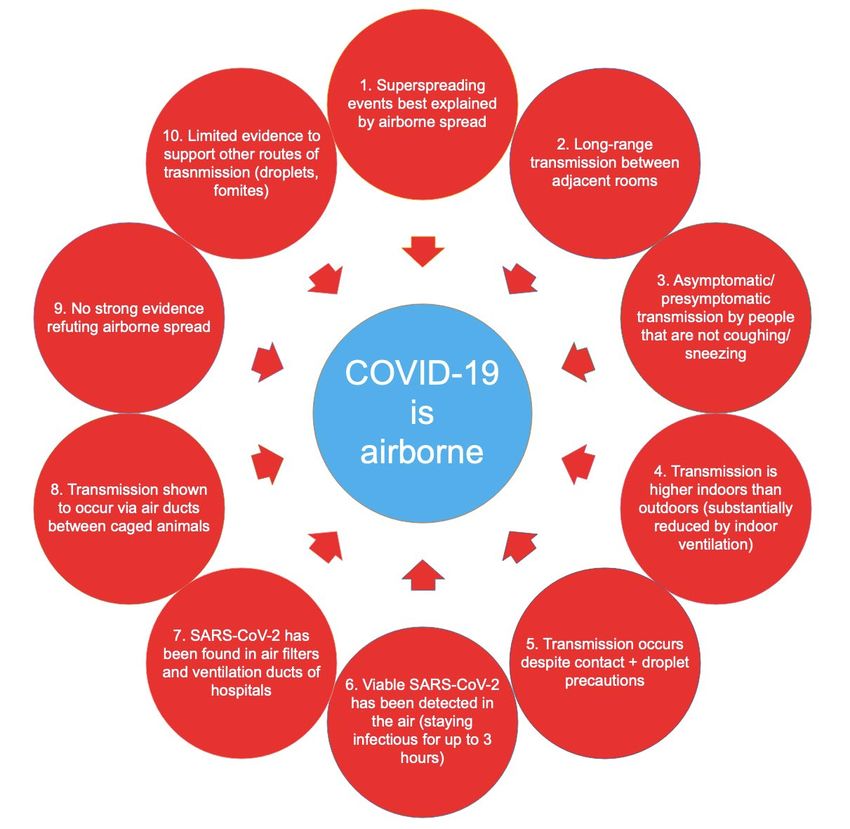
Webseminar schedule
• 10.00 – 11.30 am
• Organisational information
• presentation: Initial respiratory assessment and care
Department of Infectious Diseases, Charité
Dr. Alexander Uhrig
Dr. Miriam Stegemann
• Q&A/ discussion
2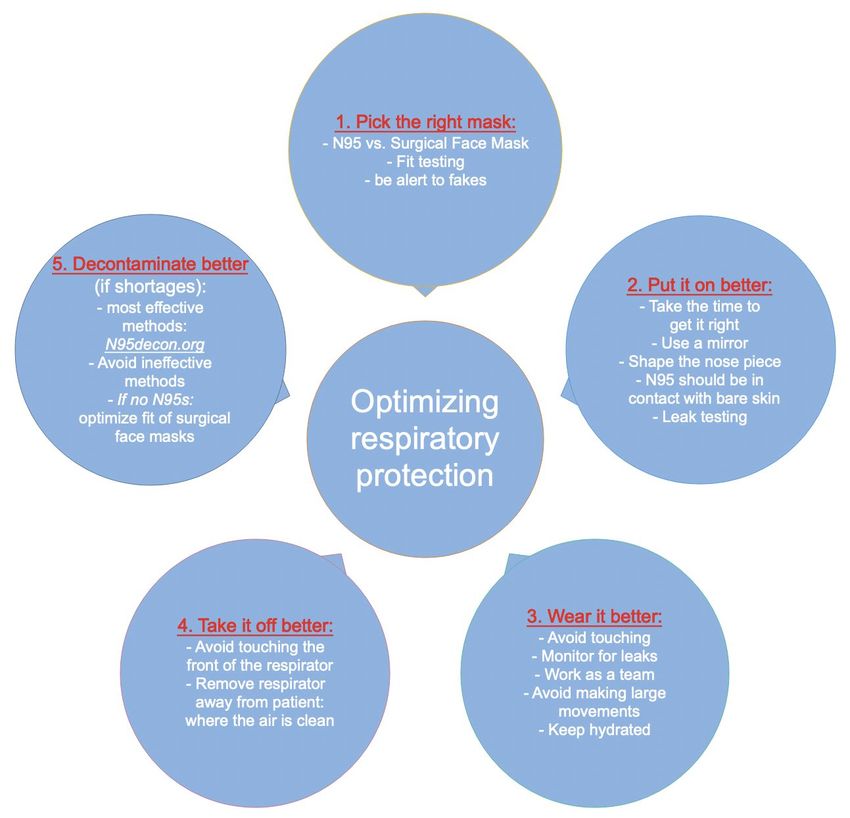
Use of the chat
• For question/ technological issues
• 1. Send questions regarding the content of the presentation
• 2. Raise a hand when you want to ask a question/participate in discussion
2. 1.
3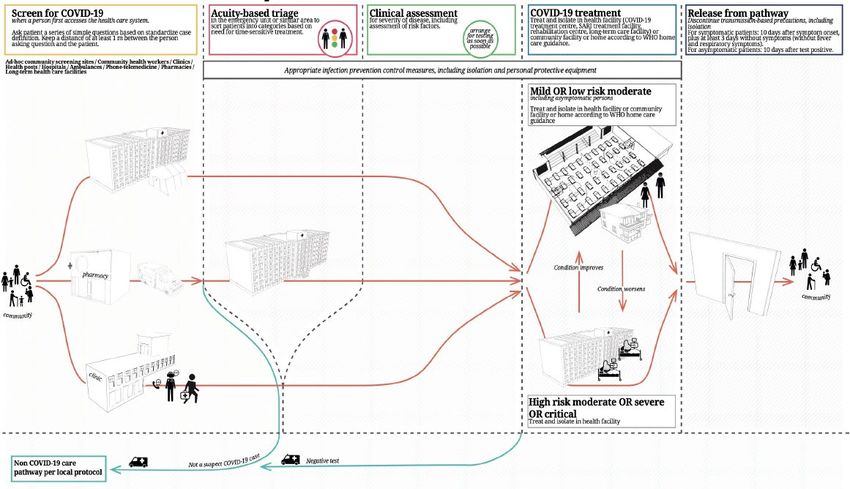
Evaluation of the web seminar • For quality assurance of the training series • Link is shared at the end of the meeting Juni 2021 Infektiologie-Beratungs-Netzwerk 4
Onlinetrainings for GPs: treatment options on COVID-19
Initial respiratory assessment
and care 05.08.
Department of Infectious Diseases, Charité
Dr. Alexander Uhrig
Dr. Miriam Stegemann
First procedures in case of
respiratory deterioration: 10.08.
Non-invasive ventilatory
support
Department of Anesthesiology and Intensive
Care Medicine, Charité
Dr. Nicolai Andrees
Dr. Julius J. Grunow
Basic treatment and cure
under non-ICU conditions 12.08.
Department of Infectious diseases,
Charité
Dr. Alexander Uhrig
Dr. Miriam Stegemann
Stabilization of a critical patient
for referral with ambulance 17.08.
Department of Anesthesiology and Intensive Care
Medicine, Charité
Dr. Nicolai Andrees
Dr. Julius J. Grunow 5
05.08.2021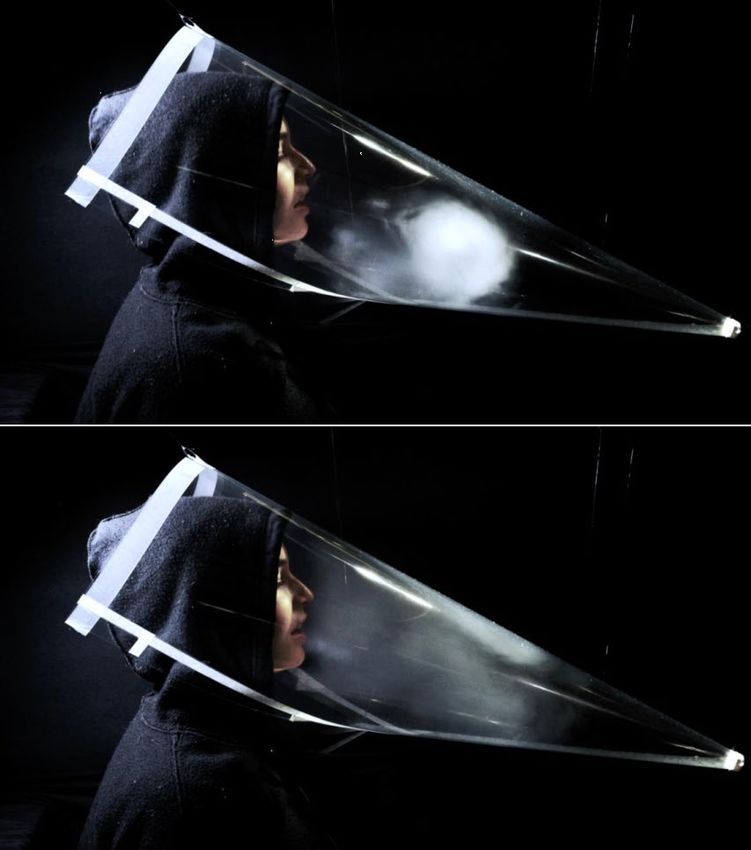
05.08.2021 Initial respiratory assessment and care - Dr. Uhrig, Dr. Stegemann 6

Learning Objectives • Epidemiology – Spectrum of disease- Course of illness • Screening – Triage – Risk Stratification • Recognition of hypoxemic respiratory failure • Understand how COVID-19 is transmitted • How to stay safe from an airborne pathogen (IPC) • COVID-19 diagnostics 05.08.2021 Initial respiratory assessment and care - Dr. Uhrig, Dr. Stegemann 7
Background – Epidemiology
Situation by WHO Region
New COVID-19 cases reported by day in Africa by African Union region
05.08.2021 Initial respiratory assessment and care - Dr. Uhrig, Dr. Stegemann 8
Background – Spectrum of disease manifestation 05.08.2021 Initial respiratory assessment and care - Dr. Uhrig, Dr. Stegemann 9

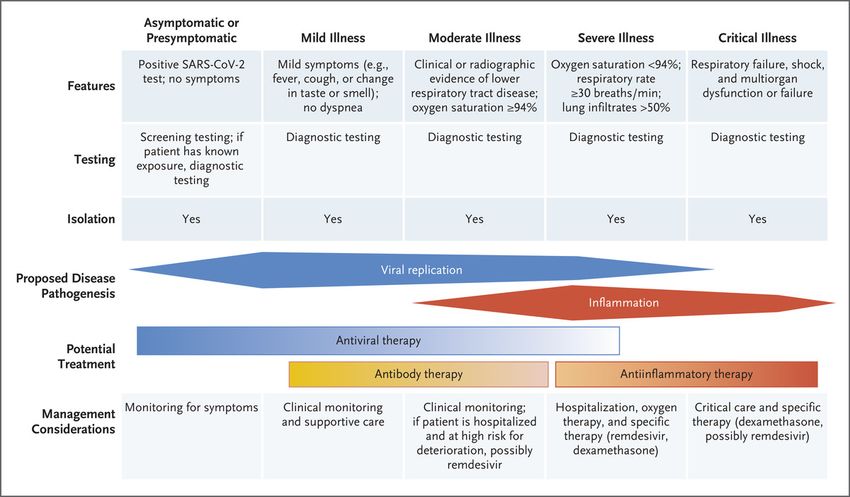
Background – Course of illness COVID-19
Characteristics, Diagnosis, and Management of Covid-19 According to Disease Stage or Severity.
RT Gandhi et al. N Engl J Med 2020;383:1757-1766.
05.08.2021 Initial respiratory assessment and care - Dr. Uhrig, Dr. Stegemann 10SUSPECT CASE - Case definition
SUSPECT CASE
A patient with any acute respiratory illness:
Fever AND at least one sign/symptom of respiratory disease
(cough, shortness of breath etc.)
Epidemiological information:
• Having been in contact with a confirmed or probable COVID-19 case
• history of travel to or residence in a location reporting confirmed cases
➠ can only increase the index of suspicion
➠ does not exclude the possibility of COVID-19
Rwanda COVID-19 CLINICAL MANAGEMENT GUIDELINES, 3rd Edition Sept 2020
05.08.2021 Initial respiratory assessment and care - Dr. Uhrig, Dr. Stegemann 11PROBABLE and CONFIRMED CASE - Case definition
PROBABLE CASE (or presumptive positive as per lab result terminology):
A suspect case for whom testing for the COVID-19 virus is presumptive.
(„presumptive“ being the result of the test reported by the laboratory using
Antigen Test or PCR method)
OR
A suspect case for whom testing could not be performed for any reason.
CONFIRMED CASE
• laboratory confirmation of COVID-19 infection using a PCR method
• irrespective of clinical signs and symptoms
Rwanda COVID-19 CLINICAL MANAGEMENT GUIDELINES, 3rd Edition Sept 2020
05.08.2021 Initial respiratory assessment and care - Dr. Uhrig, Dr. Stegemann 12Why Identification and Triage matter 05.08.2021 Initial respiratory assessment and care - Dr. Uhrig, Dr. Stegemann 13
Lowering In-Hospital Transmission of COVID-19 05.08.2021 Initial respiratory assessment and care - Dr. Uhrig, Dr. Stegemann 14
Screening for COVID-19
Case Definition: any acute respiratory illness
fever and at least one sign/symptom of respiratory disease:
cough, shortness of breath etc.
All patients should be
screened for COVID-19
using case definition
at the first point
they access the health system
Screening: ▶ Isolating patients who are potentiallypositive cases of COVID-19
▶ Reducing the spread of the virus within facilities
Modified from: WHO Interim Guidance 19 March 2020
COVID-19 Clinical Management Guidelines Rwanda MoH/RBC
05.08.2021 Initial respiratory assessment and care - Dr. Uhrig, Dr. Stegemann 15Isolation 05.08.2021 Initial respiratory assessment and care - Dr. Uhrig, Dr. Stegemann 16
Triage
Triage: ▶ systematically sorting patients by the severity of their clinical syndrome
▶ matching patients with health care resources
▶ regardless of disease state (COVID-19 positive/negative)
Modified from: WHO Interim Guidance 19 March 2020
COVID-19 Clinical Management Guidelines Rwanda MoH/RBC
05.08.2021 Initial respiratory assessment and care - Dr. Uhrig, Dr. Stegemann 17Triage: Severity of Illness Scoring
qSOFA CURB65
Criteria Criteria
Abnormal mental status Confusion
RR ≥ 22 BUN > 19 mg/dl
SBP ≤ 100 RR ≥ 30
SBP < 90 /DBP ≤60 [mmHg]
Age ≥ 65 years
Interpretation Interpretation
> 1: mortality ≥ 10% 0: 0.6% mortality
1: 2.7% mortality
2: 6.8% mortality
3: 14% mortality
4-5: 28% mortality
Rapid Emergency Medicine Score (REMS)
Fan G Eur Respir J 2020;56:2002113
Hu H Acad Emerg Med 2020;27:461-468
05.08.2021 Initial respiratory assessment and care - Dr. Uhrig, Dr. Stegemann 18Triage : Risk Stratification
• Older age (≥ 64 years)
• Male sex
• Development of ARDS/need for mechanical ventilation
• Severity of organ dysfunction on admission
• Markers of inflammation/coagulation
• Select laboratory studies: Lymphopenia, Neutrophilia, Troponin↑
• Comorbidities:
The ACCCOS Investigators Lancet 2021; 397: 1885–94
05.08.2021 Initial respiratory assessment and care - Dr. Uhrig, Dr. Stegemann 19Triage: Severity of Illness
Matching patients with healthcare resources:
• Treatment
• Treatment location }
depend on severity of illness
and risk stratification
WHO Therapeutics and COVID-19 Living Guideline 20 November 2020
05.08.2021 Initial respiratory assessment and care - Dr. Uhrig, Dr. Stegemann 20Minimum-Better-Best Monitoring of Respiratory Failure
Minimum: Observation of cyanosis, work of breathing, retractions
measuring the respiratory rate
Better: Pulse oximetry and end-tidal capnography
Best: Point-of-care blood gas analysis
Trends are more important than single values
in assessing wether a patient is at risk for decompensation
• Thorough physical examination is critical in evaluating a patient
suspected of having respiratory distress
• Use a stepwise “look, listen and feel” approach
(inspection, auscultation, palpation)
• “appearance of the patient”:
hypoxemic respiratory failure normally manifests as anxiety/combativeness
hypercapnic respiratory failure normally presents with somnolence
05.08.2021 Initial respiratory assessment and care - Dr. Uhrig, Dr. Stegemann 21Treatment location
• Home care • Treatment Facility • Hospital
• Community-based • Hospital with:
care with: - mechanical ventilation
- oxygen therapy - vasopressor therapy
- HFNC oxygen (?) - renal replacement (?)
- steroid therapy
- DTV prophylaxis
- antiviral therapeutics (?)
Prepare a pathway through the healthcare system for
• Patients with different severity of illness
• Patients with worsening severity of illness
05.08.2021 Initial respiratory assessment and care - Dr. Uhrig, Dr. Stegemann 22COVID-19 Care Pathway - Overview
WHO COVID-19 Clinical management Living Guidance, January 2021
05.08.2021 Initial respiratory assessment and care - Dr. Uhrig, Dr. Stegemann 23COVID-19 is an airborne infection
Wilson NM Anaesthesia 2020;75(8):1086-1095
05.08.2021 Initial respiratory assessment and care - Dr. Uhrig, Dr. Stegemann 24Risk Stratification Strategies and Diagnostic Modalities
• Chest CT: higher sensitivity, far lower specificity (compared to RT-PCR)
• Chest X-ray: lower sensitivity compared to RT-PCR and Chest CT
• Lung Ultrasound: high sensitivity, point-of-care utility
• ? Feasibility in every patient during a pandemic?
• ? Costs of of routine diagnostic imaging (to the patient/to the health care system)?
• ? Material resources on-site: how many machines? Hours of availability?
• ? Availability of human resources for diagnostic imaging during a pandemic?
➠ targeted use of imaging modalities when testing resources are limited/unavailable
➠ targeted use of imaging modalities in patients with moderate/severe symptoms and
concern for a false negative RT-PCR
➠ targeted use of imaging modalities in RT-PCR-positive patients
with worsening symptoms
Barros LM Am J Trop Med Hyg 2021;104:3-11
05.08.2021 Initial respiratory assessment and care - Dr. Uhrig, Dr. Stegemann 25Understand how COVID-19 is transmitted Transmission by droplets Airborne transmission Large respiratory droplets that fall quickly Small infectious particles staying in the air (gravity mechanism) Droplet Precautions: Airborne precautions: • Reducing direct contact • Ventilation of rooms • Cleaning surfaces • Air filtration • Physical barriers • Reducing crowding • Physical distancing • Reducing time spent indoors • Use of masks within droplet distance • Use masks whenever indoors • Respiratory hygiene • Attention to mask quality and mask fit • Wearing high-grade protection only for • Higher-grade protection for healthcare aerosol-generating procedures staff and frontline workers 05.08.2021 Initial respiratory assessment and care - Dr. Uhrig, Dr. Stegemann 26
Evidence for airborne transmission
Greenhalgh T Lancet 2021;397(10285):1603-1605
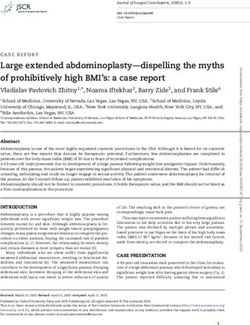
05.08.2021 Initial respiratory assessment and care - Dr. Uhrig, Dr. Stegemann 27Respirator Activity vs. Respiratory Procedures
Talking without mask
Talking with mask Coughing with mask
Wilson NM Anaesthesia 2021;10.1111/anae.15475 online ahead of print
05.08.2021 Initial respiratory assessment and care - Dr. Uhrig, Dr. Stegemann 28Respirator Activity vs. Respiratory Procedures
1 3
2 4
Different time points of a cough
Wilson NM Anaesthesia 2021;10.1111/anae.15475 online ahead of print
(without a mask)
05.08.2021 Initial respiratory assessment and care - Dr. Uhrig, Dr. Stegemann 29Respirator Activity vs. Respiratory Procedures
HFNC NIPPV-D closed limb NIPPV-S open limb
Respiratory ACTIVITY
is the primary source of aerosols,
NOT respiratory PROCEDURES
Wilson NM Anaesthesia 2021;10.1111/anae.15475 online ahead of print
05.08.2021 Initial respiratory assessment and care - Dr. Uhrig, Dr. Stegemann 30How to stay safe from an airborne pathogen
Improve
= Use N95 respirators
or better + environmental
ventilation
+ Vaccination
05.08.2021 Initial respiratory assessment and care - Dr. Uhrig, Dr. Stegemann 31Optimizing respiratory protection
Prather KA Science 2020;368(6498):1422-1424
05.08.2021 Initial respiratory assessment and care - Dr. Uhrig, Dr. Stegemann 32Optimizing respiratory protection 05.08.2021 Initial respiratory assessment and care - Dr. Uhrig, Dr. Stegemann 33
Improve environmental ventilation
1. Outside is safest
2. Open windows
3. Avoid overcrowding
4. Set extractor fans to blow outwards
5. Unblock airvents
6. Use fans carefully
7. Caution with ductless split air conditioning systems
8. Use open vehicles for transport
9. Keep staff rooms safe
10. Optimize built-in ventilation systems of hospital buildings
www.cibse.org/coronavirus-covid-19
www.ashrae.org/technical-resources/resources
www.rehva.eu/activities/covid-19-guidance
www.essentialcriticalcare.org
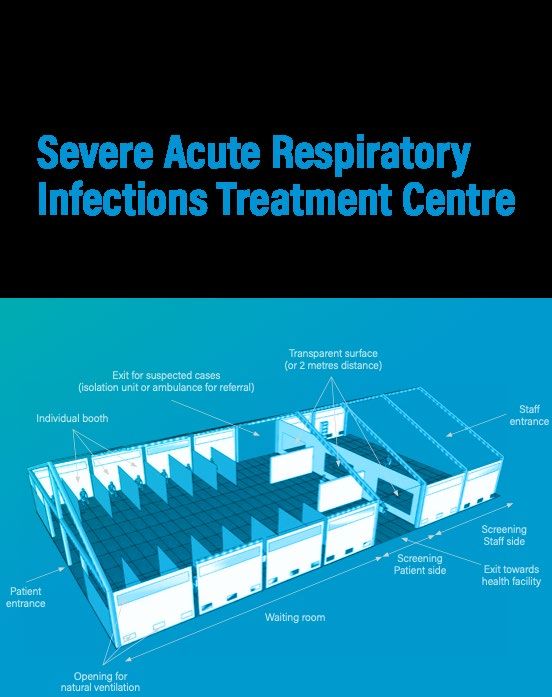
05.08.2021 Initial respiratory assessment and care - Dr. Uhrig, Dr. Stegemann 34Planning a treatment facility for SARI
Basic layout of a treatment center for Severe Acute Respiratory Infections
05.08.2021 Initial respiratory assessment and care - Dr. Uhrig, Dr. Stegemann 35Guidance for SARI Treatment Centers 05.08.2021 Initial respiratory assessment and care - Dr. Uhrig, Dr. Stegemann 36
Testing for COVID-19: nasopharyngeal swab (video)
Link to the video:
https://www.facebook.com/TheNewEnglandJournalofMedicine/videos
/how-to-obtain-a-nasopharyngeal-swab-
specimen/686695658810993/?extid=SEO----
Marty FM N Engl J Med 2020; 382:e76
05.08.2021 Initial respiratory assessment and care - Dr. Uhrig, Dr. Stegemann 37Laboratory diagnosis 05.08.2021 Initial respiratory assessment and care - Dr. Uhrig, Dr. Stegemann 38
Discharge criteria for confirmed COVID-19 cases
TEST BASED CRITERIA:
One negative result of COVID-19 RT-PCR checking for RdRp gene (CT values >
35), obtained from a sample taken after 7 days counting from the day the
positive sample was collected.
SYMPTOMS BASED CRITERIA:
• For symptomatic patients: 10 days after symptom onset, plus at least 3
additional days without symptoms (including fever and without
respiratory symptoms).
• For asymptomatic patients: 10 days after positive test for Covid-19.
• NB: some cases are admitted with positive COVID-19 RT-PCR results with
CT values for RdRp gene more than 30 and sometimes even close to the
cut off of 40. These particular situations are discussed case by case, and
the control RT-PCR test might be scheduled much sooner than 7 days.
Rwanda COVID-19 CLINICAL MANAGEMENT GUIDELINES, 3rd Edition Sept 2020
05.08.2021 Initial respiratory assessment and care - Dr. Uhrig, Dr. Stegemann 39End of the first training session
Questions?
05.08.2021 Initial respiratory assessment and care - Dr. Uhrig, Dr. Stegemann 40Contact details and legal notice Contact details • EFFO@rki.de Legal Notice • Publisher: www.rki.de | Editor: www.rki.de/zbs7 • Content: www.infektiologie- pneumologie.charite.de/en/services/medical_focus/ • Illustration: www.goebel-groener.de | Photographs: www.effo.rki.de 05.08.2021 Initial respiratory assessment and care - Dr. Uhrig, Dr. Stegemann 41
You can also read