DISTRIBUTIONAL IMPACTS OF RETAIL VACCINE AVAILABILITY - Cowles ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
DISTRIBUTIONAL IMPACTS OF RETAIL VACCINE AVAILABILITY
By
Judith A. Chevalier, Jason L. Schwartz, Yihua Su, and Kevin R. Williams
April 2021
Updated July 2021
COWLES FOUNDATION DISCUSSION PAPER NO. 2280
COWLES FOUNDATION FOR RESEARCH IN ECONOMICS
YALE UNIVERSITY
Box 208281
New Haven, Connecticut 06520-8281
http://cowles.yale.edu/Distributional Impacts of Retail Vaccine
Availability*
Judith A. Chevalier, Yale School of Management and NBER
Jason L. Schwartz, Yale School of Public Health
Yihua Su, Yale School of Public Health
Kevin R. Williams, Yale School of Management and NBER
July 2021
Abstract
We examine the potential for exploiting retailer location choice in targeting health
interventions. Using geospatial data, we quantify proximity to vaccines created by a
U.S. federal program distributing COVID-19 vaccines to commercial retail pharmacies.
We assess the distributional impacts of a proposal to provide vaccines at Dollar Gen-
eral, a low-priced general merchandise retailer. Adding Dollar General to the federal
program would substantially decrease the distance to vaccine sites for low-income,
rural, and minority U.S. households, groups for which COVID-19 vaccine take-up has
been disproportionately slow.
* Authors are listed alphabetically and contributed equally. The authors thank the Tobin Center at Yale
University for funding.
11 Introduction
A substantial literature in industrial organization studies firm locational investments,
documenting that locations are chosen in part on the basis of proximity to target cus-
tomers.1 In this paper, we explore the potential for leveraging the locational investments of
profit-maximizing firms to improve a public health intervention that requires widespread
physical distribution. Specifically, we examine the use of commercial retail locations to
distribute vaccines against COVID-19 in the United States. While response efforts to
this pandemic are unprecedented, the vaccination distribution campaign has important
characteristics in common with any potential large-scale public health intervention that
requires widespread participation.
During the COVID-19 pandemic, the United States was one of the first countries to
transition from vaccine scarcity to abundance. The U.S. distribution effort relied exten-
sively on commercial retail distribution partners through the Federal Retail Pharmacy
Program (FRPP), a strategy for reaching the public that contrasts the approaches of sev-
eral other vaccine-abundant nations (for example, Israel, England, and Canada). In its
first six months, the FRPP effort administered over 96 million vaccine doses at approx-
imately 41,000 commercial pharmacy partner locations, including long-term care phar-
macies (Centers for Disease Control and Prevention, 2021b). In contrast, while there are
11,500 community pharmacies in England, they were largely not used for COVID-19 vac-
cines; there were only 1,700 total vaccine sites in England in Spring of 2020 (Chakelian,
2021; NHS, 2021). While the U.S. presdient announced that 90% of Americans live within
5 miles of a vaccine site, the British government has announced that the "vast majority" of
people in England live within 10 miles of one (The White House, 2021; NHS, 2021).
Because retailers have an incentive to locate themselves proximate to potential cus-
tomers, it is unsurprising that distributing the vaccine through large pharmacy chains
provides proximity to a substantial number of Americans. In this paper, we use geospa-
tial data to characterize the vaccine proximity created by the FRPP. An important challenge
1
See, for example, Mazzeo (2002), Jia (2008), Harrison and Seim (2019) for evidence. In addition, literature
in operations research prescribes methods for using planning support systems for locational choice, for
example Newing et al. (2020).
2to the proximity benefits of the FRPP is that the demographics served by large retail may
not coincide with the demographics for whom vaccine takeup has proven challenging.
We show that overall proximity to retail partners is slightly higher for high-income house-
holds than for low-income households, a problematic finding, as the latter group is more
likely to face transportation challenges. We additionally show that proximity to FRPP
pharmacies is much lower for rural Americans than urban Americans.
We then analyze the distributional implications of potential enhanced retail model. In
March 2021, the director of the U.S. Centers for Disease Control and Prevention (CDC)
and the company Dollar General (DG) confirmed reports that they were exploring a part-
nership through which COVID-19 vaccines would be administered in DG retail locations
(Dollar General Stores, 2021; Boomey, 2021).2 DG is a low-cost "dollar store" retailer
whose self-described strategy is to provide low-priced necessities in a small store foot-
print, concentrating in areas that other retailers do not find attractive (Nassauer, 2017). If
an agreement were to be reached, such a partnership would likely not ultimately involve
all 16,805 DG locations but could nonetheless greatly increase the scope of the current
FRPP. We show that the addition of this retailer and/or its major dollar store rival to the
extant federal retail-based strategy would demonstrably improve the proximity of low-
income households to their closest federal retail vaccine site. Adding DG locations would
also substantially improve vaccine proximity for rural Americans. We show that the ge-
ographic targeting of dollar stores in general, and Dollar General in particular, greatly
improve vaccine proximity for demographic groups for which vaccine takeup has lagged.
The FRPP represents an effort to provide vaccine proximity. Studies in several coun-
tries suggest that, on net, policies allowing vaccine administration in pharmacies increase
influenza vaccination rates (Spinks et al., 2020). Recent literature also demonstrates that
the closure of a local pharmacy can have durable impacts on patient medication compli-
ance (Qato et al., 2019). Of course, while proximity to vaccines is likely important, it is
only one factor that influences vaccination rates. In a report issued before the COVID-19
pandemic and applicable to all vaccines (and indeed voluntary public health interventions
2
To our knowledge, the idea for a DG vaccine partnership was first proposed by researchers at the Rural
Health Service Providers Network in West Virginia (Young, 2021).
3of many types), the World Health Organization (WHO) Strategic Advisory Group of Ex-
perts (SAGE) examined the causes of “delay in acceptance or refusal of vaccination despite
availability of vaccination services”. SAGE endorsed a “3Cs” model, identifying “com-
placency, confidence, and convenience” as key impediments to vaccination (MacDonald
et al., 2015). These factors can all potentially play a role in hindering or limiting the suc-
cess of national COVID-19 vaccine campaigns, delaying take-up of essential subsequent
booster vaccines, or challenging the response to future pandemics.3 The highly visible
public health impacts of COVID-19 have likely played a role in reducing complacency, as
suggested by prior research examining vaccination responses to disease outbreaks (Oster,
2018). Clearly, reducing vaccine hesitancy and promoting vaccine confidence remains a
crucial public health challenge (CDC, 2021), both for COVID-19 and for other vaccina-
tions. This challenge is not directly addressed by improving vaccine proximity. However,
several studies provide evidence for conforming peer effects in vaccine takeup (see, for
example, Rao et al. (2007) and Bodine-Baron et al. (2013) for a discussion of other stud-
ies). In a setting with strong conforming peer effects, strategies that improve vaccination
among the least reluctant, such as providing convenience and subsidies, may ultimately
improve takeup among the reluctant. On the other hand, a vaccination strategy that uses
dollar store retailers as one component would be counterproductive if the presence of
vaccinations at these outlets erodes confidence. While this is possible, it is unclear why
dollar store clinics would be more confidence-eroding than mobile clinics, pop-up clinics
at other unconventional sites, and other strategies that have been attempted.
Our findings have implications beyond the U.S. and beyond COVID-19. As modern
retail chains optimize their product assortments and locations to target particular de-
mographic groups, our findings suggest that using retail locations to distribute vaccines
provides governments a mechanism to exploit corporate locational strategies to bring
vaccines to hard-to-reach demographic groups. For example, there are similarities be-
tween the U.S. dollar store chains and Oxxo, a retail chain with nearly 17,000 locations in
Mexico that offers convenience store items and cash services for the unbanked (FEMSA,
3
“Complacency” refers to a belief that the benefits of vaccine are low. “Confidence” refers to concerns
about the safety of vaccines or vaccination providers. “Convenience” refers to geographic and other
difficulties in finding the available vaccines.
42019). While we focus on vaccine distribution, the strategy of using a demographically-
targeted retailer as a partner could be employed for a variety of public health or social
interventions—such as recruiting diverse clinical trial participants, providing information
about government benefits, or distributing disaster preparedness or relief supplies.
Our paper proceeds as follows. Section 2 discusses our data and methodology. In
Section 3, we estimate the distributional impacts of using DG as vaccination locations, In
Section 4, we undertake a partial analysis of state vaccine locations. Section 5 concludes.
2 Data and Methodology
Our analysis focuses on U.S. vaccine distribution, where, on a weekly basis, nearly all
available doses are allocated to state governments or directly to participants in the FRPP.4
The CDC describes the FRPP for COVID-19 vaccination as "a collaboration between the
federal government, states and territories, and 21 national pharmacy partners and inde-
pendent pharmacy networks to increase access to COVID-19 vaccination across the U.S."
(Centers for Disease Control and Prevention, 2021a). The program is intended to work
in parallel with vaccination sites established and supported at the state level (and using
state-allocated vaccine doses).
We bring together data from several sources. First, we obtain a list by state of FRPP
chains from the Centers for Disease Control (Centers for Disease Control and Prevention,
2021a). For each pharmacy partner, in each state, we match these chains by name to the
Historical Business Information Files from ReferenceUSA (Infogroup, 2005-2021), accessed
March 14, 2021. We were unable to match the pharmacy network CPESN, a partner in
eleven states, and MHCN, a partner in four states. From ReferenceUSA, we obtain the
universe of retail locations of these federal partners.
It is important to note that not all pharmacy locations for a given chain (and state)
are necessarily providing vaccines. Moreover, some locations may have provided vacci-
nations intermittently. This is because the supply of vaccine was constrained overall at
4
A small number are reserved for direct federal vaccination efforts, such as those coordinated by the
Department of Defense or Department of Veterans Affairs.
5earlier stages of the program, but also because some retailers—due to freezer constraints,
for example—can only offer a subset of the vaccines authorized for use. Thus, some
chains only offered vaccinations when specific vaccines were available. We nonetheless
include all locations that may be used as vaccination sites to measure proximity. In March
2021, representatives of these chains explicitly noted that, as the vaccine became more
abundant, more of their outlets would supply them, a plan subsequently confirmed by
the Biden administration (Barker, 2021; Robbins and Weiland, 2021; The White House,
2021).
We further supplement our analysis using vaccine locations found on state COVID-
19 response websites. State vaccine sites are dynamic; we use active vaccine sites as
of the week of March 22, 2021. Therefore, our analysis does not necessarily reflect the
complete buildout of state capacity at the peak of state vaccination efforts, although we
do include in our analysis announced locations that did not have appointments available
at the time of data collection. Some states also list pharmacies found through the federal
partnership program; our analysis is unaffected by potential duplicates as we select the
closest vaccination site to each Census tract. Additionally, these files may allow us to
incorporate Federally Qualified Health Centers and locations that we cannot match using
the ReferenceUSA data.
We obtain vaccine locations for 21 states that either post a file containing all locations
or present users with an interactive map of locations.5 Figure 4 contains a list of the states
and the corresponding websites we used for data collection.
In order to examine the implications of a partnership with DG and a hypothetical
partnership with the other large dollar store chain, Dollar Tree, we download all of their
locations from ReferenceUSA. We remove from analysis a small number of headquarters,
distribution centers, and apparent non-retail outlets that are listed in ReferenceUSA.
We examine the social vulnerability metrics for the Census tracts containing these
outlets and measure distances from the these retail outlets to households. We use the
5
We collect data for AL, AR, CT, GA, IL, KS, MD, ME, MO, MS, ND, NJ, NV, OH, OK, PA, SC, WA,
WI, and WV. First, we download either the PDF, HTML, or JSON found on from each state’s COVID-19
response website. We then process the files and extract the addresses. We then geocode each site using
https://geocode.localfocus.nl/. Our analysis includes "success" and "doubt" matches, and excludes "failed"
matches.
6latitudes and longitudes of the retail outlets provided by ReferenceUSA and map these
to Census data on households. Throughout this analysis, we use Census data at the
Census tract level. There are approximately 74,000 Census tracts in the US, with a target
population of 4,000 per tract. Some tracts were unavailable for processing, leaving us with
73,088 Census tracts. As is common in the literature, we will assume that all households
live at the geographic centroid of the Census tract and calculate the great circle distance
from the Census tract centroids to each of the retail outlets in our database. We use the
minimum-calculated distance for each Census tract to a vaccine location for our analysis.
Because vaccine eligibility was set by individual states until April 2020, many sites require
state residency, and allocations are at the state level, we calculate distances to the closest
same-state retail location; we assume that people located near a state border will not
obtain the vaccine at an out-of-state location.6
We also characterize the Census tracts within which the retail outlets are located.7 To
do this, we match each Census tract not only to the Census data provided directly by
the Census, but to the tract-level data on the Social Vulnerability Index 2018 Database
US (SVI) provided by the CDC. SVI is a composite of Census data used to identify
communities that may require the greatest support during, or following, a disaster; it has
been widely adopted by federal and state health officials during COVID-19 as a tool to
design vaccination efforts and to assess their performance with respect to equity (Centers
for Disease Control and Prevention, Agency for Toxic Substances and Disease Registry,
2021; Hughes, 2021). We are able to match 72,173 SVI tracts to the Census data.
Using the same methodology as used in Murthy et al. (2021), we use data from the
National Center for Health Statistics to classify counties as urban or rural. We classify
everyone living in a Census tract in a rural county as a rural dweller and everyone living
in a census tract in an urban county as an urban dweller.
In our examination of the current composition of the FRPP, we find 26,246 retail
pharmacy outlets that belong to chains that are designated as pharmacy partners in the
6
We make an exception for North Dakota, for which we have not found retail outlets of any federal
pharmacy partner that was listed as a partner for North Dakota on the CDC website.
7
We use the 2019 American Community Survey 5-Year Data (2009-2019), Census Bureau Geocoder, and
TIGER/Line Shapefiles downloaded from
https://www.baruch.cuny.edu/confluence/display/geoportal/US+Census+Population+Centroids
7Table 1: Characteristics of U.S. Pharmacy Partner Program
Population Type Area Share Share Sharehouseholds are more than a mile from the closest pharmacy partner could indeed create
a barrier to vaccination. Unsurprisingly, there is a large gap in proximity between adults
living in rural versus rural areas. A study by the CDC, using the same metro-urban
classification as we use found that, for the period December 14, 2020–April 10, 2021,
adult COVID-19 vaccination rates were lower in rural counties (38.9%) vs. urban counties
(45.7%) (Murthy et al., 2021). The table also shows a large disparity in proximity between
Hispanic and non-Hispanic people. This disparity in proximity is particularly concerning
as COVID-19 vaccination rates for Hispanic people have been shown to be low (Ndugga
et al., 2021). Furthermore, a survey undertaken during March 2021 identified Hispanic
people as disproportionately likely to report that they want a vaccine as soon as possible
but have been unable to receive one (Hamel et al., 2021), suggesting a role for access in
explaining this group’s vaccination rates.
We obtain addresses for 10,439 vaccination sites on state websites, corresponding to
8,455 unique geographic coordinates. The mean and median number of locations per state
is 403 and 275, respectively. There are a few outliers. The West Virginia file contains only
23 locations because it lists only state-coordinated vaccine clinics. Missouri and Ohio list
over 1,300 locations.
Outlets of the major dollar store chains have more than doubled since 2005. Our data
records 16,805 DG stores as of early 2021 and 15,629 Dollar Tree stores (which are branded
as Dollar Tree or Family Dollar, following a merger of those two chains in 2015). While
dollar stores blanket the continental US, the coverage of the two major chains is particularly
dense in the Southeast and in several of the poorest US states. DG is most dense per capita
in Alabama, Arkansas, and Mississippi, with nearly 20 stores per 100,000 population.
There is also substantial density throughout the South, including West Virginia, where the
idea of using DG for vaccinations was first proposed (Young, 2021). The other major dollar
store chain, Dollar Tree, although similar in terms of overall store counts, is substantially
more dispersed geographically. It is most dense in Louisiana, New Mexico, and West
Virginia, with nine to ten stores per 100,000 population. State-by-state data are provided
in Figure 5 in the Appendix.
The rapid expansion of dollar stores in the U.S. has been controversial. One recent
9report from the Institute for Local Self-Reliance refers to dollar store chains as "an invasive
species in America’s left behind places" (Donahue and Mitchell, 2018). Activists cite
linkages between the variety of food sold at dollar stores and the prevalence of dollar
stores and obesity, although recent research has questioned whether there is a causal link
from dollar stores to obesity directly (Allcott et al., 2019). While a causal link has not
been established, some authors have argued that the influx of dollar stores cause the
exit of traditional supermarkets and grocery stores, creating food deserts, and numerous
localities have instituted regulations to curb dollar store growth (Misra, 2018).
Whether the growth of dollar stores has negative impacts is beyond the scope of this
research. However, our hypothesis is that the criticisms of dollar stores derive precisely
from their potential advantage in a vaccine distribution program. If dollar stores are
more prevalent in locations proximate to low-income households than are other types of
retailers, then they are uniquely suited to improving vaccine access.
The Social Vulnerabiity Index (SVI) was created by the Centers for Disease Control to
design and evaluate health and disaster programs. The measure is intended to capture "the
degree to which a community exhibits certain social conditions, including high poverty,
low percentage of vehicle access, or crowded households may affect that community’s
ability to prevent human suffering and financial loss in the event of disaster. These factors
describe a community’s social vulnerability" (CDC-ATSDR, 2018).
The SVI is calculated at the Census tract level. For each tract, the overall SVI index
(called RPL-THEMES) "ranks the tract on 15 social factors, including unemployment,
minority status, and disability...." (CDC-ATSDR, 2018). The numerical value of SVI for
Census tract i is the fraction of all Census tracts which are less vulnerable than tract i.
Thus, higher values of SVI are more vulnerable, and one tenth of all Census tracts are
assigned to each SVI decile bin.
The stated intent of the SVI is to assist health officials in identifying those communities
that may—as a result of these characteristics—require additional support during a public
health emergency or other hazardous event. It has been used by states and private entities
to calibrate disaster response prior to the COVID-19 pandemic (Flanagan et al., 2018)
and SVI measures have been shown to be correlated with worse COVID-19 outcomes
10(Karaye and Horney, 2020). During the ongoing vaccination program, CDC and states
have released data evaluating the relationship between vaccination coverage and social
vulnerability as measured via SVI (Hughes, 2021).
Clearly, to improve vaccine access for those least likely to have easy transportation, it is
desirable to have vaccine sites located in high-SVI locations. We examine the distribution
of SVI measures of Census tracts in which pharmacy partners are located. We compare
these to the distribution of SVI measures for DG stores. We also compare these to the
distribution of SVI measures for the other major dollar store chain, Dollar Tree/Family
Dollar.
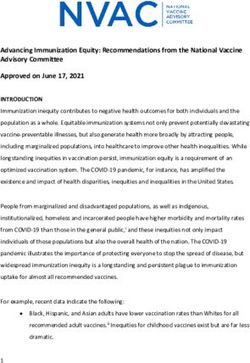
In Figure 1, we show the fraction of all pharmacy partners located in each decile bin
of SVI, the fraction of all DG stores located in each decile bin of SVI, and the fraction of all
Dollar Tree stores located in each decile bin of SVI.
The roughly 26,000 pharmacy partners that we have mapped are nearly evenly dis-
tributed across the SVI deciles. However, the highest SVI decile, composed of the Census
tracts estimated to have the highest social vulnerability, contain the smallest fraction of
the pharmacy partner locations. The figure for DG illustrates why it could be a valuable
federal partner in reaching vulnerable communities. DG stores are noticeably underrep-
resented in the lowest SVI Census tracts. Strikingly, the proportion of Dollar Tree Stores
increases monotonically with SVI decile.
Given the vaccination gap between rural and urban areas, we also examine the propen-
sity of these retailers to locate in urban versus rural areas. We find that 87% of the Federal
Retail Pharmacy Partners are located in urban counties as are 82% of Dollar Trees and 72%
of Family Dollar stores. In contrast, only 59% of Dollar General stores are located in urban
counties; we show below that distributing vaccines through Dollar General is particularly
powerful in improving vaccine proximity for rural residents.
3 Evidence on the retail program and proximity to vaccines
Household income is an important component of SVI. It is well-established that seasonal
flu vaccination rates increase with income (Linn et al., 2010); lower-income households
11Figure 1: Distribution of stores by Census tract SVI
Pharmacy Dollar General Dollar Tree
20
Percent of store type in SVI decile
10
0
1 2 3 4 5 6 7 8 910 1 2 3 4 5 6 7 8 910 1 2 3 4 5 6 7 8 910
SVI decile SVI decile SVI decile
Notes: Share of Pharmacy partners, DG, and Dollar Tree Stores by social vulnerability index (SVI)
deciles, continental U.S. For example, if an outlet of a chain is located in a Census tract for which
95% of all Census tracts are less vulnerable using the full SVI index, the outlet will be counted to
be in the top SVI decile in the graph.
face numerous barriers to vaccination such as access to scheduling technologies and
transportation (Schmid et al., 2017; Press et al., 2021). Vaccine take-up for lower-income
households would likely improve with greater proximity to a vaccination site, especially
a vaccination site within walking distance. Thus, we examine here the proximity to
retail pharmacy outlets of low-income households. Following the Census, we consider
low-income households to be households with less than $35,000 in annual income. We
consider the proximity of the current pharmacy partners to these households, as well as
12the proximity that would occur if all DG locations were added as vaccine locations.
In the continental U.S., 48.9% of low-income households reside within 1 mile of an
outlet of one of the current pharmacy partner chains. This may overestimate access if all
chain outlets will not supply vaccines. Access climbs to 60.5% if the vaccine were offered at
all DG outlets. For comparison, a slightly higher fraction of high-income households (with
income greater than $100,000 are close to a federal pharmacy site than are low-income
households, 49.5%. However, as might be expected by the high average SVI index of
dollar store locations, adding DG as a partner does not increase the fraction of households
located within 1 mile of an outlet as dramatically for high-income households as it does for
low-income households. While adding DG to the vaccine distribution program increases
the share of low-income households within a mile of a partner from 48.9% to 60.5%, for
high-income households the share within a mile of a partner is increased from 49.5% to
54.9% with the addition of DG locations. Similarly, when considering less than 2 mile
proximity and less than 5 mile proximity, a smaller share of low-income households have
proximity to pharmacy partners than do high-income households for each cutoff. Adding
DG reverses this, and a larger fraction of low-income households are within 2 or 5 miles
of a partner when DG is added to the program.
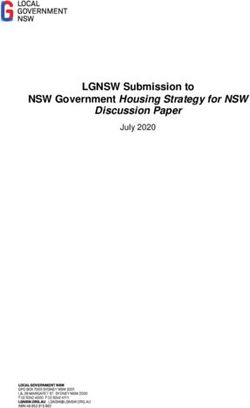
Adding DG to the FRPP greatly improves overall access to vaccines, but proximity
improvements vary greatly across states. Figure 2-(a) shows, for each state, the share of
low-income households located less than 1 mile from a pharmacy partner. On the left
of each bar pair for each state, the current pharmacy partner is shown and on the right
the impact of adding DG is illustrated. In some states, such as Alaska and Hawaii, there
are no DG stores and thus the figure shows no improvement (the two bars are of equal
height). However, in some states, particularly in the South and Midwest, the hypothetical
addition of DG to the pharmacy program dramatically increases the share of low-income
households less than 1 mile from a pharmacy partner. The raw data are included in
Figure 6 in the Appendix.
In the U.S., substantial disparities have also been identified between urban and rural
populations (Murthy et al., 2021). Racial and ethic disparities in COVID-19 vaccine
distribution have been identified in the U.S. and other countries with otherwise successful
13vaccination programs (Paton, 2021; Rosen et al., 2021). In the U.S., White and Asian
individuals have been vaccinated at a rate greater than their share of the population, of
cases, and of deaths. In contrast, Black and Hispanic individuals had, as of the end of
March 2021, been undervaccinated by these metrics (Ndugga et al., 2021). Improving
proximity of vaccine providers to these groups may help ameliorate such disparities. To
explore this, we measure the impact of adding DG to the FRPP on proximity of vaccination
cites to different racial and ethnic subgroups of the population. These are shown in Table
2.
A few patterns are notable. Importantly, we find that the impact of adding DG to the
program particularly improves proximity in rural counties. Only 22.4% of rural adults
live within a mile of a current Federal Retail Pharmacy Partner, but this improves to 33.5%
by adding DG to the program. For rural adults, the fraction living within 5 miles of a
partner improves from 56.8% to 79.7% by adding DG to the program.
While we find that a higher share of the Black population is within 1 mile of a pharmacy
partner than the white population, the improvement in proximity of adding DG outlets
as vaccine sites is particularly large for the Black population. Adding DG to the program
would improve the fraction of Black individuals within a mile of a partner site from
53.6% to 66.1%. The improvement in proximity from adding DG to the program is
also disproportionately large for the Hispanic population relative to the non-Hispanic
population. The share of Hispanic people less than a mile from a partner site is 44.9%
without DG and 53.4% with DG.
14Figure 2: Sub-populations with federal partner with and without DG at
Table 2: Impacts of adding Dollar General vaccine sites
Current partners w/ Dollar General
Population Share Share Share Share
typeslightly higher within 1 mile access to low-income households. Interestingly, this finding
is not true for wider distance bands. More low-income households are within 2 or 5
miles from the current pharmacies plus DG than are within 2 or 5 miles from the current
pharmacies plus Dollar Tree.
As suggested above, if the goal were to improve vaccine access in rural areas, Dollar
Tree is a somewhat less valuable partner than Dollar General. While 33.5% of rural adults
live within a mile of a current pharmacy partner or Dollar General, that share is only
28.9% for current pharmacy partners or Dollar Tree/Family Dollar.
The overall findings again mask some cross-state heterogeneity. As Figure 3 in the
Appendix shows, the share of low-income households within a mile of a pharmacy partner
plus hypothetical dollar store partner is, in many states, similar whether the dollar store
partner is DG or Dollar Tree. Dollar Tree’s locations are particularly attractive relative to
DG in the West. DG provides better proximity in the South and Midwest, especially in
states with a large rural population fraction, such as Alabama, Arkansas, Kansas, Iowa,
and West Virginia.
4 State Allocations and State Vaccination Sites
We find that dollar stores vaccine sites would substantially expand vaccine proximity for
low-income and rural households, particularly in the South and Southeastern U.S. Thus
far, our analysis has examined only dollar stores plus chains that are partners in the FRPP.
However, as discussed above, while some vaccine doses are allocated to this program,
doses are also allocated to states to supply the vaccination sites that states support. The
state sites consist of mass vaccination sites as well as any small pop-up sites organized by
the state. While some states augment the federal program by distributing vaccine to retail
pharmacies not part of the FRPP, others do not. While we have characterized the retail
program as novel, and the federal government’s stated purpose for using it is to improve
geographic access, without direct evidence on the state vaccine programs, it is difficult to
assess the importance of the federal retail program (or a proposed partnership with DG)
in improving proximity.
17To examine this, we scraped 21 state COVID-19 vaccine websites to find the full
listing of vaccination sites in the state. These listings typically included federal pharmacy
partners and Federally Qualified Health Centers. However, they typically included only
sites that were actively providing vaccinations when we scraped the site. For each of the
states, we match the listings with our current list of FRPP and create a listing of state
sites that excludes federal retail partners.9 Having constructed that set, we then calculate
the distance of households to their closest within-state state vaccination site, using the
methodology described above. It is possible that some states offer vaccines at locations
not listed on their state site, such as temporary pop-up sites. We then examine, for low-
income households, the proximity benefits of adding the FRPP to the roster of vaccine
sites and the potential benefits of adding DG to the set of vaccine sites.
Table 3 shows the share of low-income households within 1 mile or 5 miles of a state
site, the share within a mile of a pharmacy partner and/or state site, and the share within
a mile of a pharmacy partner, state site, and/or DG. States vary considerably in the extent
to which their vaccine sites provide substantial proximity to low income people. For
example, we find that fewer than 15.2% of the low-income population lives within a mile
of a state vaccination site for Georgia, Kansas, Maine, South Carolina, and West Virginia.
For all of these states, adding the locations of federal retail pharmacy partners share of
low-income households living within a mile of a vaccine site (state plus federal retail
partner). For West Virginia, proximity improves from 3.2% of low income households less
than a mile from a vaccine site to 23% including the federal retail partners. For the other
low-proximity states (Georgia, Kansas, Maine, and South Carolina), the addition of the
federal retail pharmacy partners improves the share of low-income households within a
mile of a partner to at least 30%. The proximity benefits of DG are also not redundant
with the state sites; adding DG to the federal program plus state sites would improve the
share of low-income households within a mile of a vaccine site by more than 14 percentage
points in all of the states with initially low proximity except Maine.
9
The few federal partners that we could not match to RefUSA will not be eliminated from the state site
list by this method.
18Table 3: Characteristics of federal pharmacy and state vaccine sites
FRPP, though most of this waste appears to have occurred when Walgreens and CVS
(two federal retail partners) were exclusively vaccinating long term care centers (Pfeif-
fer, 2021). In addition, a retail pharmacy cannot achieve the throughput per hour of a
mass vaccination site. The use of dollar stores as vaccination sites would require address-
ing additional logistical challenges; importantly, dollar stores currently lack employees
trained to administer vaccines. While the logistical challenges of coordinating vaccines
with a dollar store company may be formidable, policymakers have shown a willingness
to undertake logistically challenging initiatives to reach these populations. For example,
the Biden administration announced a “Shots at the Shop” initiative in which up to 1,000
independently-owned beauty shops and barbershops could apply for $1,000 grants to
provide vaccination information and host vaccine sites. Like dollar stores, these shops
would not normally be staffed with personnel who can provide injections. In contrast
to an initiative involving a dollar store chain, this effort requires creating incentives for
myriad independent entities to participate and the sites that apply to participate may not
necessarily be the most locationally valuable.
Of course, enhancing proximity to vaccination sites is not sufficient to ensure high
rates of vaccination due to vaccine reluctance. Nonetheless, a retail distribution strategy
that includes dollar stores provides a template for other public health efforts. For exam-
ple, subsequent COVID-19 boosters may be required on a large scale. Annual influenza
vaccination similarly relies on rapidly delivering vaccines to tens of millions of Americans
in a compressed period, often through the use of temporary large-scale vaccination clinics
outside of traditional health care settings. Reported rates of influenza vaccine administra-
tion are lower among low-income older adults, the age group—as with COVID-19—at the
greatest risk of severe disease-related outcomes (Artiga et al., 2020). Such sites could be
similarly variable for a variety of other health screenings or services, including providing
information and signup opportunities for state and federal benefits programs; many such
benefit programs are plagued by incomplete take-up by eligible populations (Wright et al.,
2017; Finkelstein and Notowidigdo, 2019). The extant locational infrastructure of retail
chains in general, and dollar stores in particular, make them a credible partner for any
initiative that requires the large-scale in-person participation of the general public.
206 References
Allcott, Hunt, Rebecca Diamond, Jean-Pierre Dubé, Jessie Handbury, Ilya Rahkovsky,
and Molly Schnell (2019) “Food deserts and the causes of nutritional inequality,” The
Quarterly Journal of Economics, 134 (4), 1793–1844.
Artiga, Samantha, Josh Michaud, Jennifer Kates, and Kendal Orgera (2020) “Racial
disparities in flu vaccination: implications for COVID-19 vaccination efforts,” Kaiser
Family Foundation, September, 15.
Barker, Aaron (2021) “Walmart exec says supply-demand dynamic of vaccine rollout
could soon shift,” https://www.click2houston.com/news/local/2021/03/11/
walmart-exec-says-supply-demand-dynamic-of-vaccine-rollout-could-soon-shift.
Bodine-Baron, Elizabeth, Sarah Nowak, Raffaello Varadavas, and Neeraj Sood (2013)
“Conforming and non-conforming peer effects in vaccination decisions,”Technical
report, National Bureau of Economic Research.
Boomey, Nathan (2021) “CDC, Dollar General exploring partnership to speed up
COVID-19 vaccine rollout,” USA Today, https://www.usatoday.com/story/money/
2021/03/09/dollar-general-cdc-covid-vaccines/6925995002/.
CDC (2021) “Building Confidence in COVID-19 Vaccines,”
https://www.cdc.gov/vaccines/covid-19/vaccinate-with-confidence.html.
Centers for Disease Control and Prevention (2021a) “Pharmacies Participating in the
Federal Retail Pharmacy Program,” https://www.cdc.gov/vaccines/covid-19/
retail-pharmacy-program/participating-pharmacies.html.
(2021b) “Understanding the Federal Retail Pharmacy Program for COVID-19
Vaccination,” https:
//www.cdc.gov/vaccines/covid-19/retail-pharmacy-program/index.html.
Centers for Disease Control and Prevention, Agency for Toxic Substances and Disease
Registry (2021) “CDC Social Vulnerability Index,”
https://www.atsdr.cdc.gov/placeandhealth/svi/index.html.
Centers for Disease Control and Prevention, Agency for Toxic Substances and Disease
Registry/ Geospatial Research, Analysis, and Services Program (2018) “CDC SVI
Documentation 2018,” https://www.atsdr.cdc.gov/placeandhealth/svi/
documentation/SVI_documentation_2018.html.
Chakelian, Anoosh (2021) “The high street Covid-19 vaccine question: Why is the
government overlooking pharmacies that could vaccinate a million people a week?”
New Statesman, https://www.newstatesman.com/politics/health/2021/01/
covid-19-coronavirus-vaccine-scandal-pfizer-astrazeneca-pharmacy-jabs.
21Dollar General Stores (2021) “Ongoing Efforts for COVID 19,”
https://www.dollargeneral.com/ongoing-efforts-for-covid-19.html.
Donahue, Marie and Stacy Mitchell (2018) “Dollar stores are targeting struggling urban
neighborhoods and small towns. One community is showing how to fight back,”
Institute for Local Self-Reliance.
FEMSA (2019) “FEMSA Investor Presentation,” https:
//femsa.gcs-web.com/static-files/1da845d6-486c-4f53-8efb-0207a6cd4747.
Finkelstein, Amy and Matthew J Notowidigdo (2019) “Take-up and targeting:
Experimental evidence from SNAP,” The Quarterly Journal of Economics, 134 (3),
1505–1556.
Flanagan, Barry E, Elaine J Hallisey, Erica Adams, and Amy Lavery (2018) “Measuring
community vulnerability to natural and anthropogenic hazards: the Centers for
Disease Control and Prevention’s Social Vulnerability Index,” Journal of environmental
health, 80 (10), 34.
Hamel, Liz, Lunna Lopes, Audrey Kearney, and Mollyann Brodie (2021) “Kaiser Family
Foundation Covid Vaccine Monitor: March 2021,”
https://www.kff.org/coronavirus-covid-19/poll-finding/
kff-covid-19-vaccine-monitor-march-2021/.
Harrison, Teresa D and Katja Seim (2019) “Nonprofit Tax Exemptions, For-Profit
Competition and Spillovers to Community Services,” The Economic Journal, 129 (620),
1817–1862.
Hughes, Michelle M (2021) “County-Level COVID-19 Vaccination Coverage and Social
Vulnerability—United States, December 14, 2020–March 1, 2021,” MMWR. Morbidity
and Mortality Weekly Report, 70.
Infogroup (2005-2021) “ReferenceUSA Business Historical Data Files,”
10.7910/DVN/GW2P3G.
Jia, Panle (2008) “What happens when Wal-Mart comes to town: An empirical analysis
of the discount retailing industry,” Econometrica, 76 (6), 1263–1316.
Karaye, Ibraheem M and Jennifer A Horney (2020) “The impact of social vulnerability on
COVID-19 in the US: an analysis of spatially varying relationships,” American journal of
preventive medicine, 59 (3), 317–325.
Linn, Shauna T, Jack M Guralnik, and Kushang V Patel (2010) “Disparities in influenza
vaccine coverage in the United States, 2008,” Journal of the American Geriatrics Society,
58 (7), 1333–1340.
MacDonald, Noni E et al. (2015) “Vaccine hesitancy: Definition, scope and
determinants,” Vaccine, 33 (34), 4161–4164.
22Mazzeo, Michael J (2002) “Product choice and oligopoly market structure,” RAND
Journal of Economics, 221–242.
Misra, Tanvi (2018) “The Dollar Store Backlash has begun,” Bloomberg City Lab,
https://www.bloomberg.com/news/articles/2018-12-20/
when-the-closest-grocery-store-is-a-dollar-store.
Murthy, Bhavini Patel, Natalie Sterrett, Daniel Weller, Elizabeth Zell, Laura Reynolds,
Robin L Toblin, Neil Murthy, Jennifer Kriss, Charles Rose, Betsy Cadwell et al. (2021)
“Disparities in COVID-19 vaccination coverage between urban and rural
counties—United States, December 14, 2020–April 10, 2021,” Morbidity and Mortality
Weekly Report, 70 (20), 759.
Nassauer, Sarah (2017) “One Nation Divisible: How Dollar General Became Rural
America’s Store of Choice,” Wall Street Journal, https://www.wsj.com/articles/
how-dollar-general-became-rural-americas-store-of-choice-1512401992.
Ndugga, Nambi, Olivia Pham, Latoya Hill, Samantha Artiga, Raisa Alam, and Noah
Parker (2021) “Kaiser Family Foundation:Latest Data on COVID-19 Vaccinations
March 31 2021,” https://www.kff.org/coronavirus-covid-19/issue-brief/
latest-data-on-covid-19-vaccinations-race-ethnicity/.
Newing, Andy, Nick Hood, and Iain Sterland (2020) “Planning support systems for retail
location planning,” in Handbook of Planning Support Science: Edward Elgar Publishing.
NHS (2021) “National Health Service to invite all people 40 and over for life saving
COVID-19 jab,” https://www.england.nhs.uk/2021/04/
nhs-to-invite-all-people-40-and-over-for-life-saving-covid-19-jab/.
Oster, Emily (2018) “Does disease cause vaccination? Disease outbreaks and vaccination
response,” Journal of health economics, 57, 90–101.
Paton, James (2021) “UK Vaccination Rates Struggle in Places Worst-Hit by COVID,”
Bloomberg Equality, https://www.bloomberg.com/news/features/2021-03-30/
britain-s-ethnic-vaccine-gap-risks-more-covid-19-cases-deaths-in-deprived-areas.
Pfeiffer, Sacha (2021) “CVS, Walgreens Are America’s Epicenters For COVID-19 Vaccine
Waste,” NPR, https://www.npr.org/2021/05/09/995264941/
cvs-walgreens-are-americas-epicenters-for-covid-19-vaccine-waste.
Press, Valerie G, Megan Huisingh-Scheetz, and Vineet M Arora (2021) “Inequities in
Technology Contribute to Disparities in COVID-19 Vaccine Distribution,” in JAMA
Health Forum, 2, e210264–e210264, American Medical Association.
Qato, Dima M, G Caleb Alexander, Apurba Chakraborty, Jenny S Guadamuz, and
John W Jackson (2019) “Association between pharmacy closures and adherence to
cardiovascular medications among older US adults,” JAMA network open, 2 (4),
e192606–e192606.
23Rao, Neel, Markus M. Möbius, and Tanya Rosenblat (2007) “Social networks and
vaccination decisions,” Working Papers 07-12, Boston, MA,
http://hdl.handle.net/10419/55601.
Robbins, Rebecca and Noah Weiland (2021) “A U.S. program aiming to channel a huge
number of vaccines through pharmacies will start soon,”
https://www.nytimes.com/2021/02/02/us/covid-vaccine-pharmacies.htm.
Rosen, Bruce, Ruth Waitzberg, and Avi Israeli (2021) “Israel’s rapid rollout of
vaccinations for COVID-19,” Israel journal of health policy research, 10 (1), 1–14.
Schmid, Philipp, Dorothee Rauber, Cornelia Betsch, Gianni Lidolt, and Marie-Luisa
Denker (2017) “Barriers of influenza vaccination intention and behavior–a systematic
review of influenza vaccine hesitancy, 2005–2016,” PloS one, 12 (1), e0170550.
Spinks, Jean, Emilie Bettington, Martin Downes, Lisa Nissen, and Amanda Wheeler
(2020) “Does policy change to allow pharmacist provision of influenza vaccination
increase population uptake? A systematic review,” Australian Health Review, 44 (4),
582–589.
The White House (2021) “Fact Sheet: President Biden Announces 90% of the Adult U.S.
Population will be Eligible for Vaccination and 90% will have a Vaccination Site Within
5 Miles of Home by April 19,”
https://www.whitehouse.gov/briefing-room/statements-releases/2021/03/29/
fact-sheet-president-biden-announces-90-of-the-adult-u-s-population-will-be-eligible
Wright, Bill J, Ginny Garcia-Alexander, Margarette A Weller, and Katherine Baicker
(2017) “Low-cost behavioral nudges increase Medicaid take-up among eligible
residents of Oregon,” Health Affairs, 36 (5), 838–845.
Young, A. Toni (2021) “COVID-19 Preparedness in Rural America,”
https://www.youtube.com/watch?v=x5X4IPi2hlI.
247 Appendix
Table 4: State-Coordinated Vaccine Locations
State Website
Alabama https://bamatracker.com/providers
Alaska https://anchoragecovidvaccine.org/providers/
Arkansas https://www.healthy.arkansas.gov/programs-services/topics/covid-19-map-of-1-a-pharmacy-locations
Connecticut https://www.211ct.org/search?page=1&location=Connecticut&taxonomy_code=11172&service_area=connecticut
Georgia http://www. dph.georgia.gov/locations/covid-vaccination-site
Illinois https://coronavirus.illinois.gov/s/vaccination-location
Kansas https://kdhe.maps.arcgis.com/apps/instant/nearby/index.html?appid=2cf619afb6c74320a26855840a8ca3e3
Maine https://www.maine.gov/covid19/vaccines/vaccination-sites
Maryland https://maryland.maps.arcgis.com/apps/instant/nearby/index.html?appid=0dbfb100676346ed9758be319ab3f40c&find=
Mississippi https://msdh.ms.gov/msdhsite/_static/14,0,420,976.html#providerMap
Missouri https://covidvaccine.mo.gov/map/Approved-Vaccinators.pdf
North Dakota https://app.powerbigov.us/view?r=eyJrIjoiNmY1ZWFiMzktYzMzNC00ZTQxLTkxZTAtNWRiMzkyYzYzMjk0IiwidCI6
IjJkZWEwNDY0LWRhNTEtNGE4OC1iYWUyLWIzZGI5NGJjMGM1NCJ9
Nevada https://www.immunizenevada.org/covid-19-vaccine-locator
New Jersey https://newjersey.github.io/vaccine-locations/NJ-COVID-19-Vaccine-Locations.pdf
Ohio https://coronavirus.ohio.gov/wps/portal/gov/covid-19/dashboards/covid-19-vaccine/covid-19-vaccine-provider-dashboard
Oklahoma https://vaccinate.oklahoma.gov/en-US/vaccine-centers/
Pennsylvania https://padoh.maps.arcgis.com/home/item.html?id=d169e1d2ae454bec928d046156dd7186
South Carolina https://sc-dhec.maps.arcgis.com/apps/instant/nearby/index.html?appid=514e64ead13e4f508147dad8f483da38
Washington https://www.doh.wa.gov/YouandYourFamily/Immunization/VaccineLocations#
West Virginia https://dhhr.wv.gov/News/2021/Pages/COVID-19-Vaccination-Clinics-March-2-7,-2021.aspx
Wisconsin https://dhsgis.wi.gov/server/rest/services/DHS_COVID19/COVID19_Vaccine_Provider_Sites/MapServer/0/query?
where=1%3D1&text=&objectIds=&time=&geometry=&geometryType=esriGeometryEnvelope&inSR=&
spatialRel=esriSpatialRelIntersects&relationParam=&outFields=*&returnGeometry=false&returnTrueCurves=false
&maxAllowableOffset=&geometryPrecision=&outSR=&returnIdsOnly=false&returnCountOnly=false&orderByFields=&
groupByFieldsForStatistics=&outStatistics=&returnZ=false&returnM=false&gdbVersion=&returnDistinctValues=false&
resultOffset=&resultRecordCount=&queryByDistance=&returnExtentsOnly=false&datumTransformation=&
parameterValues=&rangeValues=&f=pjson
Notes: Websites used to gather state-coordinated vaccine locations.
25Table 5: Summary Statistics for U.S. Dollar Stores, Selected Years
Dollar Dollar Dollar General Dollar Tree
General Tree per 100K per100K
Alabama 791 317 16.26 6.52
Alaska 0 0 0 0
Arizona 123 306 1.77 4.4
Arkansas 463 198 15.48 6.62
California 229 781 .58 1.99
Colorado 56 234 1.01 4.23
Connecticut 69 126 1.93 3.52
Delaware 48 65 5.06 6.85
District of Columbia 0 6 0 .88
Florida 927 1160 4.5 5.63
Georgia 944 719 9.17 6.98
Hawaii 0 0 0 0
Idaho 0 95 0 5.63
Illinois 587 547 4.58 4.27
Indiana 596 371 8.98 5.59
Iowa 276 110 8.81 3.51
Kansas 250 121 8.59 4.16
Kentucky 596 346 13.42 7.79
Louisiana 586 453 12.57 9.71
Maine 59 103 4.43 7.73
Maryland 138 237 2.3 3.95
Massachusetts 54 250 .79 3.66
Michigan 588 648 5.91 6.51
Minnesota 170 190 3.08 3.44
Mississippi 549 249 18.37 8.33
Missouri 564 302 9.26 4.96
Montana 0 40 0 3.84
Nebraska 130 70 6.83 3.68
Nevada 21 113 .72 3.87
New Hampshire 40 71 2.98 5.28
New Jersey 156 317 1.76 3.57
New Mexico 106 190 5.07 9.08
New York 499 662 2.54 3.37
North Carolina 896 743 8.82 7.32
North Dakota 44 36 5.85 4.79
Ohio 887 552 7.62 4.74
Oklahoma 472 241 12.05 6.15
Oregon 60 100 1.47 2.45
Pennsylvania 806 654 6.3 5.11
Rhode Island 21 73 1.99 6.91
South Carolina 575 396 11.6 7.99
South Dakota 60 42 6.94 4.86
Tennessee 832 403 12.51 6.06
Texas 1591 1732 5.71 6.21
Utah 11 126 .36 4.14
Vermont 38 24 6.08 3.84
Virginia 441 459 5.24 5.46
Washington 3 140 .04 1.92
West Virginia 240 191 13.12 10.44
Wisconsin 210 275 3.63 4.76
Wyoming 3 45 .52 7.73
Notes: Number of dollar stores and stores per 100,000 population, by state. Data from
RefUSA.
26Table 6: Vaccine Access—Low-Income Households
Table 7: Vaccine Access—Black Population
Table 8: Vaccine Access—Hispanic Population
Figure 3: Percentage of Low-Income Households with Federal Pharmacy Partner at
Table 9: Vaccine Access—Alternative Partners and Distance
You can also read