Digital Technology for AMD Management in the Post-COVID-19 New Normal
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Digital Technology for AMD Management in the Post-COVID-19 New Normal Sim, S. S., Yip, M. Y., Wang, Z., Tan, A. C. S., Tan, G. S. W., Cheung, C. M. G., Chakravarthy, U., Wong, T. Y., Teo, K. Y. C., & Ting, D. S. (2021). Digital Technology for AMD Management in the Post-COVID-19 New Normal. Asia-Pacific Journal of Ophthalmology, 10(1), 39-48. https://doi.org/10.1097/APO.0000000000000363 Published in: Asia-Pacific Journal of Ophthalmology Document Version: Publisher's PDF, also known as Version of record Queen's University Belfast - Research Portal: Link to publication record in Queen's University Belfast Research Portal Publisher rights Copyright 2021 Asia-Pacific Academy of Ophthalmology. Published by Wolters Kluwer Health, Inc. on behalf of the Asia-Pacific Academy of Ophthalmology. This is an open access article distributed under the terms of the Creative Commons Attribution-Non Commercial-No Derivatives License 4.0 (CCBYNC-ND), where it is permissible to download and share the work provided it is properly cited. The work cannot be changed in any way or used commercially without permission from the journal. General rights Copyright for the publications made accessible via the Queen's University Belfast Research Portal is retained by the author(s) and / or other copyright owners and it is a condition of accessing these publications that users recognise and abide by the legal requirements associated with these rights. Take down policy The Research Portal is Queen's institutional repository that provides access to Queen's research output. Every effort has been made to ensure that content in the Research Portal does not infringe any person's rights, or applicable UK laws. If you discover content in the Research Portal that you believe breaches copyright or violates any law, please contact openaccess@qub.ac.uk. Download date:24. Dec. 2021
REVIEW ARTICLE
Digital Technology for AMD Management in the Post-COVID-19
New Normal
Shaun Sebastian Sim, MD yz, Michelle YT Yip, MD yz, Zhaoran Wang, BSc yz
Anna Cheng Sim Tan, MD yz, Gavin Siew Wei Tan, MD, PhD yz
Chui Ming Gemmy Cheung, MD, FRCOphth yz, Usha Chakravarthy, MD, PhD§
Tien Yin Wong, MD, PhD yz, Kelvin Yi Chong Teo, MD yz, and Daniel SW Ting, MD, PhD yz
Purpose: The COVID-19 pandemic has put strain on healthcare systems
and the availability and allocation of healthcare manpower, resources and
A ge-related macular degeneration (AMD) is a leading cause
of irreversible visual impairment in people over the age of
50 years.1 The global prevalence of any type of AMD has been
infrastructure. With immediate priorities to protect the health and safety of
reported to be 8.7%.2 Although approximately 170 million indi-
both patients and healthcare service providers, ophthalmologists globally
viduals are afflicted, the global prevalence of AMD is expected to
Downloaded from http://journals.lww.com/apjoo by BhDMf5ePHKav1zEoum1tQfN4a+kJLhEZgbsIHo4XMi0hCywCX1AWnYQp/IlQrHD3i3D0OdRyi7TvSFl4Cf3VC4/OAVpDDa8KKGKV0Ymy+78= on 06/02/2021
were advised to defer nonurgent cases, while at the same time managing
increase to 288 million by 2040.2–4 AMD can be classified into
sight-threatening conditions such as neovascular Age-related Macular
early-stage, intermediate-stage, and advanced-stage AMD. Early-
Degeneration (AMD). The management of AMD patients both from a
or intermediate-stage AMD is characterized by the presence of
monitoring and treatment perspective presents a particular challenge for
drusen and retinal pigment epithelial changes, and these may not
ophthalmologists. This review looks at how these pressures have encour-
affect vision significantly at these stages. Advanced-stage AMD,
aged the acceptance and speed of adoption of digitalization.
however, tends to be vision threatening and these individuals may
Design and methods: A literature review was conducted on the use of
present with either geographic atrophy (nonexudative AMD) or
digital technology during COVID-19 pandemic, and on the transformation
choroidal neovascularization (exudative AMD).
of medicine, ophthalmology and AMD screening through digitalization.
The management of AMD spans a large spectrum, from a
Results: In the management of AMD, the implementation of artificial
simple screening of early AMD to complex, repeated treatments
intelligence and “virtual clinics” have provided assistance in screening,
with intravitreal vascular endothelial growth factor (VEGF)
diagnosis, monitoring of the progression and the treatment of AMD. In
inhibitors that require close monitoring and frequent visits in
addition, hardware and software developments in home monitoring
neovascular AMD (nAMD). Current management strategies in
devices has assisted in self-monitoring approaches.
nAMD have evolved from the fixed monthly regimens proposed
Conclusions: Digitalization strategies and developments are currently
by the initial registration trials (CATT, MARINA, ANCHOR) to
ongoing and underway to ensure early detection, stability and visual
regimens such as treat and extend AMD (TREX-AMD).5–9 These
improvement in patients suffering from AMD in this COVID-19 era. This
regimens that take into account real-world clinical considerations,
may set a precedence for the post COVID-19 new normal where digital
attempt to mitigate high treatment burdens but still require
platforms may be routine, standard and expected in healthcare delivery.
frequent interactions between patients and doctors in hospital
settings for investigations and treatments. These management
Key Words: AI, AMD, Covid-19, digital healthcare, telemedicine
strategies have worked well to date to prevent vision loss in
(Asia Pac J Ophthalmol (Phila) 2021;10:39–48) patients with AMD but need to adapt to face the potentially life-
threatening challenges from a pandemic such as the coronavirus
disease 2019 (COVID-19).
The COVID-19 was declared by the World Health Organi-
Submitted November 4, 2020; accepted November 30, 2020. zation (WHO) as a pandemic on March 11, 2020.10–13 Ophthal-
From the Singapore National Eye Centre,; ySingapore Eye Research Institute,; mologists, like other healthcare providers, are faced with the
zOphthalmology and Visual Sciences Academic Clinical Program, Duke-NUS
Medical School, National University of Singapore, Singapore; and §Queen’s responsibility of providing essential care while ensuring they are
University of Belfast Royal Victoria Hospital, Belfast, Ireland. not vectors of the disease. In response to the crisis, many
S.S.S. and M.Y.T.Y. contributed equally to this work.
Drs Tien Wong and Daniel Ting are the co-inventors of a deep learning system for international ophthalmology societies and colleges quickly pub-
the detection of retinal diseases. lished guidelines and recommendations for best practices.14–16
The authors have no conflicts of interest to declare.
Address correspondence and reprint requests to: Daniel Ting, Assistant Professor, Earlier this year, these ophthalmology societies recommended
Duke-NUS Medical School, National University of Singapore, Consultant, that ophthalmologists cease to provide any treatment other than
Surgical Retina, Singapore National Eye Centre, Head, Artificial Intelligence
and Digital Innovation, Singapore Eye Research Institute. urgent or emergent care. Several measures have been proposed to
E-mail: daniel.ting45@gmail.com; Kelvin Teo, MD, 11 Third Hospital Ave- minimize COVID-19 spread among ophthalmic care providers
nue, Singapore 168751, consultant, Medical Retina, Singapore National Eye
Centre. E-mail: kelvin.teo.y.c@singhealth.com.sg and patients: administrative control to lower patient attendance
Copyright ß 2021 Asia-Pacific Academy of Ophthalmology. Published by Wolters and suspension of elective services, patient triage system at
Kluwer Health, Inc. on behalf of the Asia-Pacific Academy of Ophthalmology.
This is an open access article distributed under the terms of the Creative entrances to identify at-risk patients, and the promotion of the
Commons Attribution-Non Commercial-No Derivatives License 4.0 (CCBY- use of personal protective equipment.17–19 Although these mea-
NC-ND), where it is permissible to download and share the work provided it is
properly cited. The work cannot be changed in any way or used commercially sures were important to reduce the risk of COVID-19 spread,
without permission from the journal. these measures are unsustainable in the long-term especially
ISSN: 2162-0989
DOI: 10.1097/APO.0000000000000363 because we have yet to see an “end” to this pandemic.
ß 2021 Asia-Pacific Academy of Ophthalmology. https://journals.lww.com/apjoo | 39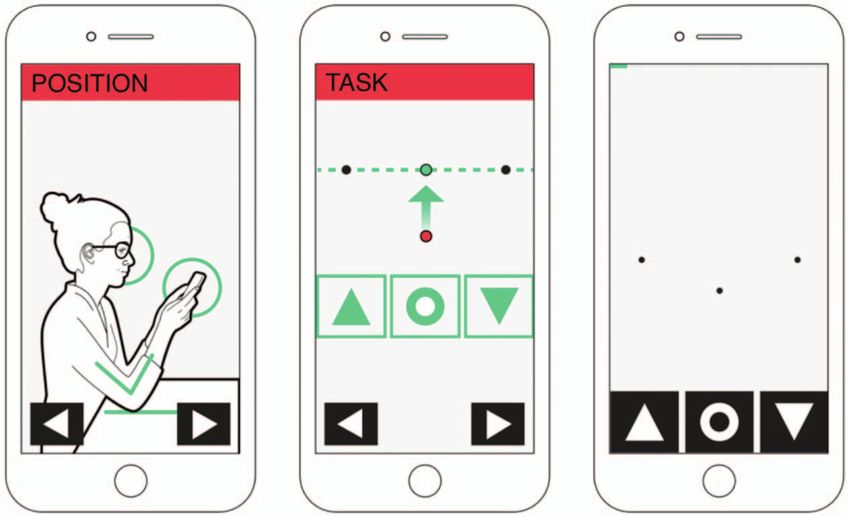
Sim et al Asia-Pacific Journal of Ophthalmology Volume 10, Number 1, January/February 2021
Hence, in order to cope with these measures and the high Among the first premises that encouraged the development of
burden of care associated with the management of nAMD, retina telemedicine was the recognition of the need to provide medical
subspecialty clinics have been forced to adopt practices that assistance to remotest areas. In the 1960s, along with the devel-
differed from traditional treatment patterns.20 Although many opment of The Space Program in preparation for space missions,
of these strategies are practical and safe, there is an opportunity to the National Aeronautic and Space Administration in the United
further improve the management of AMD through the use of States initiated the monitoring of astronauts’ health to provide
digital technology. Here, we review the current and future options medical aid if needed through remote teleconsultations.35,36 Since
of digital technology and how these may improve the manage- then, the use of teleconsultations has increased in medicine and
ment of AMD in the post-COVID world. ophthalmology. Australia has largely capitalized on teleconsul-
tations and implemented schemes to review acute ophthalmolog-
ical conditions remotely.37 These measures have resulted in
IMPACT OF COVID-19 WORLDWIDE improved patient convenience by cutting the need for extensive
The COVID-19 pandemic that has plagued 2020 has affected travel for medical advice and are also cost saving by reducing
people from all corners of the globe. As of December 29, 2020, over unnecessary acute transfers.38 Virtual clinics have reduced the
79 million individuals globally have been infected with the novel workload on tertiary centers and improved the efficiency of eye
coronavirus and over 1.7 million people people have lost their lives clinics, particularly for glaucoma services.39 There has been
to it.21 The sudden surge of patients has strained healthcare increased adoption of digital platforms around the globe alongside
infrastructure across the world, with resources stretched to the the internet of things (IoT) that further allows for wider access to
breaking point while the mortality from COVID-19 has risen healthcare, eye care, and increased efficiency.40,41
steadily.22 With global recognition of the need to suppress spread, In this global health emergency where medical resources
travel restrictions and social distancing were mandated by most outweigh demand, telemedicine has enabled the triaging of at-risk
countries in the world.23 This lock-down of movement has triggered populations (Table 1). Teleconsultations have allowed patients’
widespread acceptance and adoption of digital communication with symptoms to be evaluated for possible COVID-19 infections
the intention of mitigating the social, economic, and political while reducing the risk of exposure to other patients, healthcare
impact of the pandemic.24–26 professionals, and the community.42,43 With the need for rapid
detection of patients with COVID-19, several groups have also
harnessed the automation of artificial intelligence (AI) to enable
DIGITAL TECHNOLOGY DURING THE COVID-19 rapid automated diagnosis of COVID-19 through analysis of
PANDEMIC radiological imaging of the respiratory system.44–46 To enable
Teleconferencing has become an essential daily tool for monitoring and surveillance of this pandemic, public agencies
remote communication for purposes of work, social interaction, have embraced digital technologies such as IoT, big data analyt-
and medical consultations.27 Notably, Zoom Video Communica- ics, AI, and Blockchain.47 Use of digital tools utilizing GPS or
tions’ stock price rose dramatically with the implementation of Bluetooth tracking has been critical to aid contact tracing to
social distancing measures, from US$68.04 on 31 December 2019 identify exposed individuals and sever the chain of transmis-
to $259.51 on 26 June 2020 on the US stock market.13 In addition, sion.21 Easily accessible databases such as “Worldometer” show
the e-commerce giants’ growth during this pandemic is proving to real-time live updates on the global number of positive cases,
be substantial and multifactorial. Amazon’s net sales have deaths, and recovered cases.48 Thermal camera setups at access
increased this year by 26% to US$75.5 billion in the first quarter points also provide fever screening areas, and when coupled with
of 2020 compared to US$59.7 billion in the first quarter of 2019.28 facial recognition software, allows rapid identification of
Alibaba Group’s revenue for this year’s first quarter amounting to COVID-19 suspect individuals in the community.49,50
a total of US$16.1 million compared to its counterpart in 2019
where US$13.9 million revenue was generated.29 This is contrib-
uted by a forced change in consumers’ spending behavior to DIGITAL TECHNOLOGY IN OPHTHALMOLOGY
online retail, which also generates demand for small businesses to Although digitalization has been more widely accepted with
utilize online retail as a platform to overcome financial difficulty recent pressures, this fourth industrial revolution had already begun
during the current economic decline.30 Digital payments have also to transform various sectors with no exception to healthcare.51
gained traction during this period. An analysis by Bain & Com- Ophthalmology has been at the forefront of this foray and with its
pany estimated that there will be a 5% increase in digital payments culture of innovation, it was quick to adopt these novel digital
compared to pre-COVID and e-commerce digital payments will technologies, including virtual health, AI, and digital home-moni-
increase by 1–2%.31 As quarantine orders have eased and people toring applications to aid in improving patient care.52 Telemedicine
have ventured out of their homes, contactless payments have risen has been integral in improving screening programs of ophthalmo-
especially since initial reports from the World Health Organiza- logical diseases.35 As the availability of experienced ophthalmolo-
tion carried warnings to the public that banknotes were capable of gists may be scarce especially in developing countries, telemedicine
carrying and spreading the virus.32,33 Mastercard reacted by may allow for more appropriate distribution of resources.53,54 This is
raising contactless payment limits across 29 countries.34 through more people screened at an early stage of disease by
specialty-trained nurses and graders, allowing ophthalmologists to
focus their efforts toward managing difficult and severe cases.53,54
DIGITAL TECHNOLOGY IN MEDICINE Telemedicine has also facilitated the management of more than
Virtual clinics and teleconsultation frameworks have been 10,000 potentially complex cases in low- and middle-income coun-
the means of provision of acute specialist care to rural areas.35 tries via the Orbis Cyber-Sight telemedicine program.55 The portal
40 | https://journals.lww.com/apjoo ß 2021 Asia-Pacific Academy of Ophthalmology.
Asia-Pacific Journal of Ophthalmology Volume 10, Number 1, January/February 2021 Digital Technology for AMD in the post-COVID-19 New Normal
TABLE 1. Digital Techniques Used by Health Symptoms and Government to Aid in Tackling COVID-19 Pandemic
Strategy to Tackle Digital Tool
COVID-19 Example Employed
Monitoring community cases Thermal cameras with facial recognition software49,50 Thermal imaging, AI, IoT, big data
Contact tracing with digital footprint90 IoT, big data
Real-time live updates of pandemic48 IoT, big data
Reducing spread Virtual clinics for remote consultations to reduce traffic into Videotelephony
hospitals91
Home monitoring of non-urgent diseases92 IoT, big data
Quarantine, remote working27 Blockchain, videotelephony
Delivery of medications47 Blockchain
Triage Teleconsultations for symptomatic individuals with systemic or Videotelephony, AI
respiratory symptoms42
Screening of high-risk individuals based on travel and contact AI, big data
history42
Home monitoring and triage of unstable patients93 IoT, big data
Diagnosis of confirmed cases Automated diagnosis of COVID-19 from chest imaging44,46 AI
Multimodal automated analysis of symptoms, exposure history, AI
laboratory test, and imaging45
Interventions and treatment of Electronic Intensive Care Unit monitoring programs42 IoT
COVID-19 patients
AI indicates artificial intelligence; IoT, internet of things.
Proposed strategies.
provides a platform for ophthalmologists in developing countries to VEGF inhibitor therapy is required. Finally, once stability of the
transmit patient data and images safely, and to consult with expert disease has been achieved, home-monitoring using digital appli-
mentors in the field. With the increasing development of AI, cations or devices can be implemented to avoid unnecessary
automated diagnosis of ophthalmological conditions has helped to hospital visits.
address concerns of limited resources by providing an automated way
of triage common causes of vision-threatening conditions. There is a AI for AMD Screening and Treatment
keen global interest in AI to detect diabetic retinopathy, a major
worldwide cause of preventable blindness. Products of this are Screening
multiple algorithms able to detect not only diabetic retinopathy from In the past few years, several deep learning systems (DLS)
fundus photographs with high sensitivity and specificity, but in have been developed for detecting and classifying the severity of
addition, other related eye conditions such as diabetic macular AMD based on color fundus photographs. Although the majority
edema, glaucoma, and age-related macular degeneration.56 With of these algorithms were built using the Age-related Eye Disease
retinopathy of prematurity being the leading cause of childhood Study (AREDS) materials,60–62 others have come from popula-
blindness causing lifelong morbidity, AI algorithms for retinopathy tion-based studies and diabetic retinopathy screening pro-
of prematurity has been developed to address concerns of reliability grams.56,63 Because the color fundus images in the AREDS
and accuracy of screening of at-risk babies especially in low- or dataset were captured as analog photographs, they were subse-
middle-income countries, usually limited by inadequate equipment, quently digitized. Whether the DLSs trained using digitized
training, and personnel.57 As the retina is the only organ in which images will show similar analyzing capability if presented with
direct observation of blood vessels in vivo is possible, studies have images that were acquired using digital cameras has not yet been
shown correlations with the health of the microvasculature of the established; however, there are available and increasing number
heart and brain. Therefore, future developments in teleophthalmol- of DLS trained to identify AMD from digital camera images.
ogy are likely to provide opportunities to use retinal vascular Most Deep learning (DL) algorithms have demonstrated the
health screening to identify cardiac, neurovascular, and systemic potential to perform different AMD classification tasks at high
diseases.58,59 accuracy and noninferiority when compared with retinal special-
ists or professional human graders.56,60–62 The DLSs utilizing
AREDS dataset for both training and testing purposes obtained
DIGITAL TECHNOLOGY IN AMD high performance. To exemplify, Grassmann et al obtained a
AMD typically affects elderly patients who are also at risk of sensitivity of 84.20% and specificity of 94.30%, and Burlina et al
morbidity and mortality related to COVID-19. We envisage that obtained an area under the curve of receiver operating curve
with current and future digital tools, the management of AMD can (AUC) of 0.94–0.96. Ting et al confirmed these findings in
be streamlined and adapted to reduce patients’ risk of exposure to multiethnic real-world datasets allowing for broader applications
COVID-19. This digital revolution can address all aspects of of this technique.56,60,61
AMD management. First, AMD screening can be readily per- Apart from digital fundus photographs, OCT can also play
formed using fundus and Optical coherence tomography (OCT) an important role in AMD screening. DL algorithms have been
imaging in the community. Next, patients with abnormalities built to deliver automated segmentation and classification tasks
detected can be referred to virtual AMD clinics for expert using OCT images that are key for detecting the new onset of
evaluation and a clinic visit only if treatment with intravitreal nAMD. The clinical application of DL on OCT scans was
ß 2021 Asia-Pacific Academy of Ophthalmology. https://journals.lww.com/apjoo | 41Sim et al Asia-Pacific Journal of Ophthalmology Volume 10, Number 1, January/February 2021
described by De Fauw et al.64 Using 14,884 three-dimensional per patient per year, providing economic rationale to integrate AI
OCT scan volumes, they built a two-stage framework by decou- into the screening program.65
pling the segmentation and classification network, which pro- A recent feasibility study adapted the multimodal retinal
vides 1 of 4 referral suggestions, that is, urgent, semi-urgent, image analysis consisting of fundus photographs, OCT, and OCT
routine, and observation only. This framework was tested for angiography scans. Although the training dataset was relatively
patient triage in an ophthalmology clinic based on more than 50 small (75 participants), Vaghefi et al showed that by combining
common diagnoses that can be derived from OCT, compared with multiple modalities, the DLS accuracy increased from 91% to
retinal specialists and optometrists. The DL algorithm was 96% in detecting intermediate AMD, compared to using OCT
comparable to the decision for “urgent referral” made by 2 expert alone.66 With methods to mitigate the common problem of small
retina specialists and was better in making this decision as datasets required for training of algorithms such as generating
compared to 2 other retinal specialists and 4 optometrists with new images through the use of Generative Adversarial Networks,
an AUC of 0.99. A key advantage of this two-stage framework is further studies could even show improvement in outcomes.
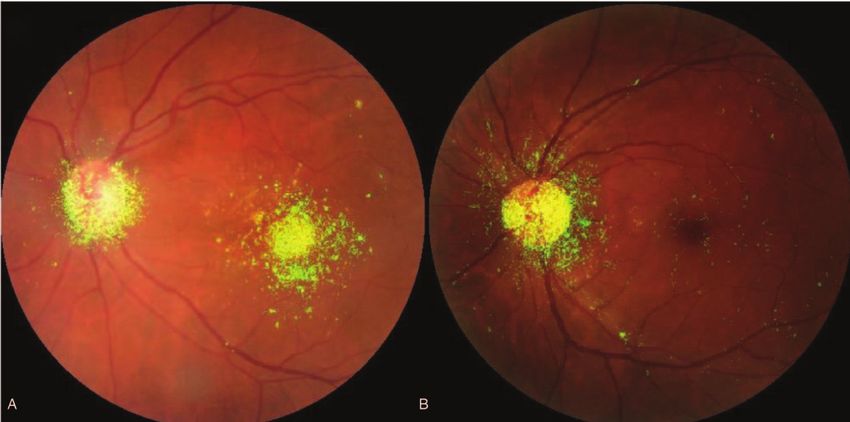
that the model can be generalized to a new OCT device by Figure 2 shows examples of Generative Adversarial Network-
retraining the segmentation stage with manually annotated created images of AMD compared to actual images taken of eyes
slices, whereas the classification network remains unchanged. with AMD, showing the ability for realistic images of AMD to be
The error rate of the framework tested on Spectralis OCT created for the benefit of future studies and DLS development.
scanner with adapted segmentation network was 3.4%, not Another method to overcome the problem of small datasets is to
significantly different from the error rate of 5.5% on the original adopt “live” clinical databases that will accumulate an increasing
device type.64 amount of datapoint and allow interactive improvement and
Lack of confidence in the feasibility of integration of these refinement of DLS for patients that may have heterogeneous
systems and the “black box” unaccountable nature of DLS factors for genetic and environmental susceptibility. Thus, further
garnered some resistance to adoption during initial proposals. research should note that it is crucial to use large multicenter
However, the development of “heatmaps,” areas of focus of the datasets with various macular diseases and to incorporate a
DLS, provided clinicians and policymakers more understanding multimodal approach with clinical data, color fundus photo-
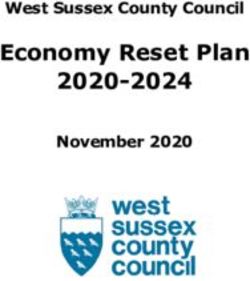
of the neural networks’ learning and decision-making. Figure 1 graphs, and OCT imaging, in order to enhance the generalizability
shows examples of heatmaps of our DLS showing eyes with of the AMD DL framework.
advanced AMD compared to a normal fundus. This demonstrates Although the DLS is able to screen for AMD, there are
that the DLS is able to identify pathology in the macula suggestive potential limitations in its clinical use as a screening tool for some
of AMD and thus classify it to have AMD. The cost-effectiveness ocular conditions as it does not address comorbid conditions or
of integrating AI solutions into screening programs have also been risk factors before the development of ophthalmoscopic findings.
a considerable factor for policymakers determining widespread For example, elevated intraocular pressure before glaucomatous
adoption. Xie et al explored the cost-effectiveness of a fully- optic neuropathy and elevated glycated hemoglobin before wors-
automated, semi-automated model for diabetic retinopathy, a ening diabetic retinopathy. Thus, one would be cautious to
vision-threatening ophthalmological condition with national interpret DLS screening results in the isolation of these
screening in many countries, which demonstrated reduced cost risk factors.
FIGURE 1. Heatmaps of our DLS demonstrating areas of focus of the algorithm determining AMD detection as depicted by the fluorescent green
signals. A, Heatmap of the fundus with AMD showing focus in the macula where the drusen is identified and localized, and the optic disc. B,
Heatmap of the fundus with no AMD demonstrating background detection of the optic disc with no focus of the macula that is non-pathological.
AMD indicates age-related macular degeneration; DLS, deep learning system.
42 | https://journals.lww.com/apjoo ß 2021 Asia-Pacific Academy of Ophthalmology.Asia-Pacific Journal of Ophthalmology Volume 10, Number 1, January/February 2021 Digital Technology for AMD in the post-COVID-19 New Normal
FIGURE 2. Generative Adversarial Network (GAN) created images of AMD compared to real images of AMD. This may represent how we can
circumvent the need for large databases for DLS training by creating new images of AMD. A, This shows an example of a real color photograph with
the focus of an eye with AMD with focus and cropping of the macula. Drusen is noted in the image, suggestive of AMD. B, This shows an example
of a virtual image created using GAN models of an eye with AMD that shows a high resemblance of an actual photograph of macula cropped image
of an eye with AMD as seen in image (A). AMD indicates age-related macular degeneration; DLS, deep learning system.
Treatment Personalized medicine has been highly regarded as the gold
In the management of nAMD, OCT monitoring of morphol- standard of treatment options for an individual where treatment is
ogy of retinal lesions and disease activity forms an integral part of optimized to minimize side effects and maximize efficacy.
monitoring and decision for retreatment. With increasing Development of AI algorithms aiming to predict progression to
demands for effective and accurate OCT monitoring, automated late dry and late wet AMD based on color fundus photographs
techniques have been explored.67,68 These include the Notal OCT allows higher-risk individuals who may benefit from closer follow
Analyzer that reports high-concordance rates when comparing to surveillance and may guide management by advising on better
retinal specialists with an accuracy of 91%, sensitivity of 92%, control of risk factors and for alternative advanced treatment.71,72
and specificity of 91%.68 A recent study utilizing the AREDS2 In the current technological climate, models have been having
10-year Follow-On study (AREDS2-10Y) with 1127 eyes with high-accuracy rates with detection, but accuracy in prediction of
longitudinal data showed that the AI-based algorithm achieved a progression of AMD has not achieved such high rates yet that
higher level of performance at detecting the presence of retinal proves to be a difficult task with few groups attempting this.71 In
fluid than human retinal specialists (accuracy 0.851 versus 0.805, addition, predicting the onset of the disease is currently difficult
sensitivity 0.822 versus 0.468, specificity 0.865 versus 0.970, with limited images of asymptomatic patients. Prognostication of
respectively) when compared to the ground truth of expert graders functional improvement from treatment through algorithms has
at the University of Wisconsin Fundus Photograph Reading been explored to provide predictive information that can assist in
Center.67 patients’ autonomous decision-making. A study utilizing machine
AI has lent its ability to develop further tools to aid the learning to predict visual acuity (VA) after the commencement of
management of nAMD by defining the disease and detection of anti-VEGF treatment at 3- and 12-month intervals showed that the
biomarkers of nAMD. Various algorithms have been developed to difference between algorithmic prediction and actual VA was
monitor nAMD using biomarkers including but not limited to between 0.11 and 0.18 logMAR for 3-month forecast and 0.16 and
intraretinal fluid, subretinal fluid, pigment epithelial detachment, 0.22 logMAR.73 This demonstrates the utility that AI may provide
drusen, and geographical atrophy.69 The development of systems in the creation of personalized medicine.
to better quantify and measure retinal fluid will enable a reliable
assessment of response to anti-VEGF treatment compared to the Virtual AMD Clinics for Diagnosis and Treatment
qualitative evaluation currently used in clinical practice.70 The concept of “virtual” (without actual consultation) medi-
Schmidt-Erfurth et al utilized automated segmentation methods cal retina clinics emerged in 2015.74 In this “virtual” clinic,” all
in deep learning to ascertain volumes of intraretinal fluid, sub- patients had VA tests and OCT scan performed and reviewed
retinal fluid, and pigment epithelial detachment, and applied this asynchronously by the medical team without a face to face
algorithm to a phase III HARBOR clinical trial.70 This study specialist consultation. The implementation of these virtual
demonstrated that the stricter treatment arm with a higher dose AMD clinics not only assisted with a reduction in mean time
and regular monthly dosing of anti-VEGF resulted in the least between consecutive appointments and waiting times, but also
residual fluid, exemplifying how these AI algorithms are enabling resulted in significant visual gains.74 Furthermore, previous stud-
improving therapeutic regimes for nAMD.70 ies have demonstrated high inter-reader and intrareader
ß 2021 Asia-Pacific Academy of Ophthalmology. https://journals.lww.com/apjoo | 43Sim et al Asia-Pacific Journal of Ophthalmology Volume 10, Number 1, January/February 2021
agreement for OCT scans.75,76 In another study, a reduction in The future development of a pandemic-ready, robust clinical
healthcare burden was demonstrated when up to 44% of patients management must address new referrals and follow-up protocols,
were found to be suitable for virtual clinics where only OCT and patient treatment compliance, tracking of clinical outcomes, and
ultra-widefield imaging were performed.77 also data security.
With the advances in imaging coupled with potential AI-
driven decision making, we expect that the monitoring of treat- Digital monitoring devices for
ment response, recurrence during maintenance phase or after AMD – ForeseeHome, myVisionTrack, Alleye
cessation of treatment, and observation of the fellow eye for Since the late 1960s, self-monitoring in AMD patients has
incipient neovascularization can be managed using “virtual” traditionally involved the use of an Amsler chart (grid). The
clinics. This concept adheres to the principles of social distancing, Amsler grid can evaluate the central 208 visual field when used at
which is imperative for the prevention of COVID-19 spread, by a 30-cm testing distance.79 The identification of subtle changes in
allowing the acquisition of images and subsequent decision visual function (such as distortion) may suggest AMD disease
making to be separated in time and space. activity or recurrence. The limitations of the Amsler chart include
By far the largest survey of patients’ attitudes regarding its subjective and qualitative nature, crowding effects, and per-
attending virtual clinics revealed that more than 86% of patients ceptual completion phenomenon, hence limiting its sensitivity in
were supportive of a “virtual” clinic review in place of face-to- detecting AMD-related visual changes.80
face clinic appointments.78 There are several alternatives to the Amsler chart. In an effort
to improve AMD disease monitoring and recurrence preferential
Real-World AMD Retina Clinics hyperacuity perimetry (PHP) was developed by Loewenstein
nAMD is a sight-threatening condition that requires prompt et al.81 The initial technique was more sensitive than the tradi-
and regular intravitreal anti-VEGF injections. Retina subspecial- tional Amsler chart but had a relatively high rate of false positives.
ists treating nAMD have developed various strategies during the Further iterations of PHP was able to differentiate recent-onset
initial “lockdown phase.” The aim was to reduce the contact time nAMD from intermediate AMD with higher sensitivity and
between ophthalmic care providers and patients and congestion specificity.82 Recently, portable home monitoring devices such
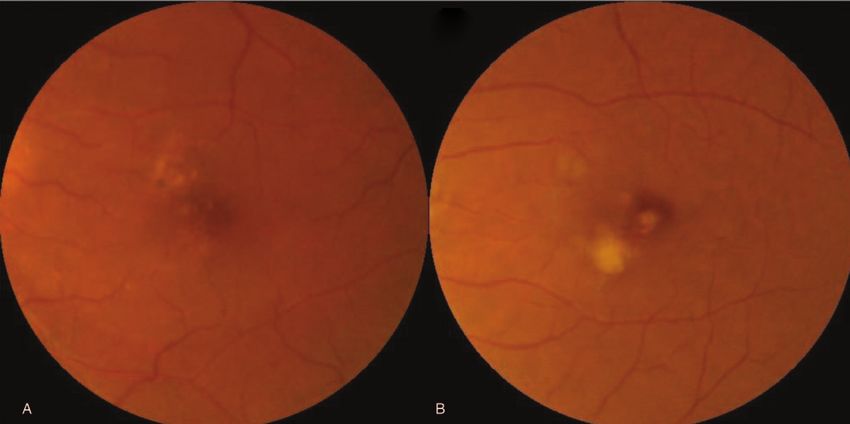
within the clinic, while maintaining visual improvement and/or as the ForeseeHome AMD monitor utilizes PHP testing to detect
visual stability. One of the strategies we implemented (Table 2) new choroidal neovascularization development at an earlier
included a variation of the “Treat-and-Plan” regime as described stage83 (Fig. 3).
by Antaki et al.20 The shape discrimination hyperacuity (SDH) testing is
This involved 3 types of visits, new referral visit, follow-up another method of early identification of AMD and its progres-
assessment visit, and treatment only visits (Table 2). In our sion.84 Wang et al found that a mobile version of the SDH test,
setting, we performed similar tests (VA, dilation, and OCT) myVisionTrack (mVT) developed by Genentech USA, Inc, was
during the new referral visits, with FA, Indocyanine green comparable to the previously established desktop SDH. This
angiography, and Optical coherence tomography angiography provides patients with a new tool that is intuitive and readily
performed only upon request of the treating physician. Patients accessible to monitor macular diseases at home.85 A subsequent
on active treatment who attended follow-up assessment visits had study by the same group also showed that elderly patients were
VA tests with either OCT or dilated fundal examination. If these willing to comply with this novel method of self-monitoring.86
patients were deemed stable by the treating physician the patients Another recently developed novel mobile application, Alleye
then proceeded directly for treatment. However, if vision had developed by Oculocare medical Inc. in Switzerland, uses an
declined by 1 line from the previous visit or the patient reported alignment hyperacuity task (dot alignment) to monitor visual
worse vision, both OCT and dilated fundal examination were function.87 In contrast to mVT that detects and characterizes
required and treatment interval titrated based on activity status. the central 38 of metamorphopsia, Alleye screens 12.7 thus
We also instituted treatment-only visits in which patients on covering almost the entire macular region. The extended area
fixed or regular intervals attended for treatment only without of screening is useful when considering macular pathology typi-
further tests or investigations. Although these measures help cally extends within the vascular arcades (Fig. 4). Further studies
reduce contact time and congestion, a potential downside exists are currently underway for evaluating the reliability of different
for stable patients due to the inability to extend treatment tests for monitoring disease progression and for early detection of
intervals. fellow eye involvement.88,89
TABLE 2. The Clinical Protocol for New Referral Visits Versus Follow-Up Assessment Visits Versus Treatment-Only Visit
Type of Visit New Referral Visit Follow-Up Assessment Visit Treatment-Only Visit
Investigation VA, OCT, DFE - If VA and symptomatically stable: VA, OCT, or DFE None
- If VA and symptomatically worse: VA, OCT, DFE
FA, ICG, OCTA
Treatment Loading dose phase – 3 No disease activity: allocate to fixed-interval regime based For intravitreal
monthly intravitreal on last stable treatment interval injection
injections Presence of disease activity: decrease treatment interval
by 2 weeks
DFE indicates dilated fundal examination; ICG,Indocyanine green angiography; OCT, Optical coherence tomography; OCTA, Optical coherence tomography
angiography; VA, visual acuity.
44 | https://journals.lww.com/apjoo ß 2021 Asia-Pacific Academy of Ophthalmology.Asia-Pacific Journal of Ophthalmology Volume 10, Number 1, January/February 2021 Digital Technology for AMD in the post-COVID-19 New Normal
FIGURE 3. Home monitoring devices for AMD from Notal Vision. A, Notal Vision’s ForeseeHome1 enables patients with intermediate AMD with VA
94
of 20/60 or worse to take daily tests that are subsequently sent to the Notal Vision Data Monitoring Center in which the physician will be notified
when changes are noted from baseline. This machine utilizes a closed viewer and a mouse for patients to click to identify visual distortions
displayed to the patient’s eye. B, Notal Vision’s Home OCT combines OCT imaging technology with artificial intelligence software Notal OCT Analyzer
(NOATM) to enable home-based monitoring of exudative AMD. It is still undergoing FDA approval currently and not available for clinical use as of
yet. AMD indicates age-related macular degeneration; DLS, deep learning system; VA, visual acuity.
Real-World Experience with Alleye Home Monitoring the COVID-19 pandemic lockdown in Singapore. Patients sched-
Application uled for a follow-up in the retina clinic for any condition over the
In Singapore National Eye Center, we deployed the Alleye lockdown period (end April 2020 to middle June 2020) were
application to patients who had their appointments deferred over deferred based on electronic chart review by treating physicians.
FIGURE 4. Alleye phone application that enables home-based self-monitoring of central and paracentral metamorphopsia with existing mobile phone
devices in an at-risk population.95 The figure shows snapshots of the application demonstrating its use. The left image shows easy-to-follow guides
for standardization of the position of the mobile phone to ensure testing of the macula. The middle image shows instructions to the user and
patient on the requirements to place the middle of 3 points on the invisible connecting line between the outer points utilizing controls on the
screen. The right image demonstrates an example of a test of the task previously described.
ß 2021 Asia-Pacific Academy of Ophthalmology. https://journals.lww.com/apjoo | 45Sim et al Asia-Pacific Journal of Ophthalmology Volume 10, Number 1, January/February 2021
All deferred patients were subsequently invited to participate in a 9. Rufai SR, Almuhtaseb H, Paul RM, et al. A systematic review to assess the
pilot test of the Alleye app with an aim to detect early changes in ’treat-and-extend’ dosing regimen for neovascular age-related macular
vision due to reactivation of disease. degeneration using ranibizumab. Eye. 2017;31(9):1337–1344.
10. Zhu N, Zhang D, Wang W, et al. A novel coronavirus from patients with
pneumonia in China, 2019. N Engl J Med. 2020;382(8):727–733.
CONCLUSIONS 11. Sohrabi C, Alsafi Z, O’Neill N, et al. World Health Organization declares
COVID-19 was an unexpected catalyst for digitalization global emergency: a review of the 2019 novel coronavirus (COVID-19). Int
progression in this century and transformation of people’s daily J Surg. 2020;76:71–76.
lives. Although digital strategies were employed to monitor and
12. World Health Organisation WHO Director-General’s opening remarks at
curb the community spread of the virus, these initiatives were also
the media briefing on COVID-19. 2020. https://wwwwhoint/dg/speeches/
extended to address preexisting demands on healthcare. This has
detail/who-director-general-s-opening-remarks-at-the-media-briefing-on-
become part and parcel of our “new normal” in healthcare
covid-19—11-march-2020. Accessed March 29, 2020.
provision and has become essential in the fight against this
13. Nicola M, O’Neill N, Sohrabi C, Khan M, et al. Evidence based
pandemic. In the ophthalmology community, the management
management guideline for the COVID-19 pandemic - review article. Int J
of AMD has been profoundly affected as these patients are not
Surg. 2020;77:206–216.
only most vulnerable to COVID-19 infections but also require
regular monitoring and treatment to slow the progression of the 14. Korobelnik JF, Loewenstein A, Eldem B, et al. Guidance for anti-VEGF
disease. There is an urgent unmet need to transform the way care intravitreal injections during the COVID-19 pandemic. Graefes Arch Clin
is provisioned for AMD during this crisis and beyond. Digital Exp Ophthalmol. 2020;258(6):1149–1156.
transformation may be the solution for ensuring safety in all 15. Teo KYC, Chan RVP, Cheung CMG. Keeping our eyecare providers and
aspects of AMD management. This transformation includes patients safe during the COVID-19 pandemic. Eye. 2020;34(7):1161–1162.
advanced analytic techniques such as AI to detect and screen 16. Lai THT, Tang EWH, Chau SKY, et al. Stepping up infection control
for disease, novel models of care that ensure minimal contact and measures in ophthalmology during the novel coronavirus outbreak: an
social interactions, treatment strategies such as the “Treat-and- experience from Hong Kong. Graefes Arch Clin Exp Ophthalmol.
Plan” regime, and digital home monitoring initiatives that can 2020;258(5):1049–1055.
detect early changes of AMD. In the post-COVID-19 new normal, 17. Wilder-Smith A, Freedman DO. Isolation, quarantine, social distancing
we may see these strategies become more prevalent as evidence of and community containment: pivotal role for old-style public health
their effectiveness to provide safe care materializes. With the measures in the novel coronavirus (2019-nCoV) outbreak. J Travel Med.
continued evolution and improvement of digitalization, we will be 2020;27(2).
better equipped to face the next challenge.
18. Ahmed F, Zviedrite N, Uzicanin A. Effectiveness of workplace social
distancing measures in reducing influenza transmission: a systematic
review. BMC Public Health. 2018;18(1):518.
REFERENCES
19. Koh A, Chen Y. Perspective from Singapore and China on the COVID-19
1. Pennington KL, DeAngelis MM. Epidemiology of age-related macular
pandemic: the new world order for ophthalmic practice. Ophthalmology.
degeneration (AMD): associations with cardiovascular disease phenotypes
2020;127(8):e49–e50.
and lipid factors. Eye Vis. 2016;3:34.
20. Antaki F, Dirani A. Treating neovascular age-related macular degeneration
2. Wong WL, Su X, Li X, et al. Global prevalence of age-related macular
in the era of COVID-19. Graefes Arch Clin Exp Ophthalmol.
degeneration and disease burden projection for 2020 and 2040: a systematic
2020;258(7):1567–1569.
review and meta-analysis. Lancet Glob Health. 2014;2(2):e106–e116.
21. WHO. Situation Report – 194. WHO; 2020.
3. Pascolini D, Mariotti SP. Global estimates of visual impairment: 2010. Br J
Ophthalmol. 2012;96(5):614–618. 22. Gates B. Responding to Covid-19—a once-in-a-century pandemic? New
England Journal of Medicine. 2020;382(18):1677–1679.
4. Sources for Macular Degeneration: Facts & Figures. http://
wwwbrightfocusorg/sources-macular-degeneration-facts-figures. Accessed 23. Organisation ICA, Organisation WH. Joint ICAO-WHO Statement on
August 2020. COVID-19. 2020.
5. Rosenfeld PJ, Brown DM, Heier JS, et al. Ranibizumab for neovascular age- 24. Economist T. The changes covid-19 is forcing on to business. 2020. https://
related macular degeneration. N Engl J Med. 2006;355(14):1419–1431. www.economist.com/briefing/2020/04/11/the-changes-covid-19-is-forcing-
on-to-business. Accessed July 19, 2020.
6. Brown DM, Michels M, Kaiser PK, et al. Ranibizumab versus verteporfin
photodynamic therapy for neovascular age-related macular degeneration: 25. Whitelaw S, Mamas MA, Topol E, et al. Applications of digital technology
two-year results of the ANCHOR study. Ophthalmology. 2009;116(1):57– in COVID-19 pandemic planning and response. Lancet Digit Health.
65.e5. 2020;2:e435–e440.
7. Comparison of Age-related Macular Degeneration Treatments Trials 26. Baig A, Hall B, Jenkins P, et al. The COVID-19 recovery will be digital:
Research G, Martin DF, Maguire MG, et al. Ranibizumab and bevacizumab A plan for the first 90 days. 2020. https://www.mckinsey.com/business-
for treatment of neovascular age-related macular degeneration: two-year functions/mckinsey-digital/our-insights/the-covid-19-recovery-will-be-
results. Ophthalmology. 2012;119(7):1388–1398. digital-a-plan-for-the-first-90-days#. Accessed 18 July 2020.
8. Wykoff CC, Croft DE, Brown DM, et al. Prospective trial of treat-and- 27. Drake Bennett NG. Zoom Goes From Conferencing App to the Pandemic’s
extend versus monthly dosing for neovascular age-related macular Social Network. 2020. https://www.bloomberg.com/news/features/2020-04-
degeneration: TREX-AMD 1-year results. Ophthalmology. 09/zoom-goes-from-conferencing-app-to-the-pandemic-s-social-network.
2015;122(12):2514–2522. 28. Amazon. Amazon.com Announces First Quarter Results. Amazon; 2020.
46 | https://journals.lww.com/apjoo ß 2021 Asia-Pacific Academy of Ophthalmology.Asia-Pacific Journal of Ophthalmology Volume 10, Number 1, January/February 2021 Digital Technology for AMD in the post-COVID-19 New Normal
29. Alibaba. March quarter 2020 and full fiscal year 2020 results. Alibaba 50. Borak M. Beijing considers using facial recognition to fight a new Covid-
Group. 2020. 19 outbreak. 2020. https://www.scmp.com/abacus/tech/article/3089378/
30. Monica P. The way we shop has fundamentally changed. That’s good news beijing-considers-using-facial-recognition-fight-new-covid-19-outbreak.
for Alibaba. CNN Business. 2020. Accessed June 27, 2020.
31. Gringoli V, Williams G, Ott J, et al. The Covid-19 Tipping Point for 51. Jayanthi P, Iyyanki M, Mothkuri A, et al. Fourth industrial revolution: an
Digital Payments. 2020. https://www.bain.com/insights/the-covid-19- impact on health care industry. International Conference on Applied
tipping-point-for-digital-payments/. Accessed June 29, 2020. Human Factors and Ergonomics. Springer; 2019
32. Walden S. Banking After COVID-19: The Rise of Contactless Payments in 52. Ting DS, Lin H, Ruamviboonsuk P, et al. Artificial intelligence, the
the U.S. 2020. https://www.forbes.com/advisor/banking/banking-after- internet of things, and virtual clinics: ophthalmology at the digital
covid-19-the-rise-of-contactless-payments-in-the-u-s/. Accessed June 29, translation forefront. Lancet Digit Health. 2020;2(1):e8–e9.
2020. 53. Skalet AH, Quinn GE, Ying G-S, et al. Telemedicine screening for
33. Tsang W. Mastercard study shows consumers globally make the move to retinopathy of prematurity in developing countries using digital retinal
contactless payments for everyday purchases. Seeking Touch-Free Payment images: a feasibility project. J AAPOS. 2008;12(3):252–258.
Experiences Mastercard. 2020. 54. Ells AL, Holmes JM, Astle WF, et al. Telemedicine approach to screening
34. Mastercard. Mastercard enables Contactless limit raise across 29 countrise; for severe retinopathy of prematurity: a pilot study. Ophthalmology.
and champions permanent increase. 2020. https:// 2003;110(11):2113–2117.
newsroom.mastercard.com/eu/press-releases/mastercard-enables-contactless- 55. Cyber-Sight: Existing or expanding (post-pilot). Botswana: Center for
limit-raise-across-29-countries-and-champions-permanent-increase/. Health Market Innovations; 2002. http://healthmarketinnovations.org/
Accessed June 29, 2020. program/cyber-sight.
35. Li HK. Telemedicine and ophthalmology. Surv Ophthalmol. 56. Ting DSW, Cheung CY-L, Lim G, et al. Development and validation of a
1999;44(1):61–72. deep learning system for diabetic retinopathy and related eye diseases using
36. Baldwin C, Simpson A. A Brief History of NASA’s Contributions to retinal images from multiethnic populations with diabetes. JAMA.
Telemedicine. 2013. https://www.nasa.gov/content/a-brief-history-of-nasa-s- 2017;318(22):2211–2223.
contributions-to-telemedicine. Accessed July 29, 2020. 57. Gensure RH, Chiang MF, Campbell JP. Artificial intelligence for
37. Blackwell NA, Kelly GJ, Lenton LM. Telemedicine ophthalmology retinopathy of prematurity. Curr Opin Ophthalmol. 2020;31(5):312–317.
consultation in remote Queensland. Med J Aust. 1997;167(11–12):583– 58. Wong TY, Klein R, Klein BE, et al. Retinal microvascular abnormalities
586. and their relationship with hypertension, cardiovascular disease, and
38. Rosengren D, Blackwell N, Kelly G, et al. The use of telemedicine to treat mortality. Surv Ophthalmol. 2001;46(1):59–80.
ophthalmological emergencies in rural Australia. J Telemed Telecare. 59. Wang JJ, Liew G, Wong TY, et al. Retinal vascular calibre and the risk of
1998;4(suppl 1):97–99. coronary heart disease-related death. Heart. 2006;92(11):1583–1587.
39. Clarke J, Puertas R, Kotecha A, et al. Virtual clinics in glaucoma care: 60. Burlina PM, Joshi N, Pekala M, et al. Automated grading of age-related
face-to-face versus remote decision-making. Br J Ophthalmol. macular degeneration from color fundus images using deep convolutional
2017;101(7):892–895. neural networks. JAMA Ophthalmol. 2017;135(11):1170–1176.
40. Perednia DA, Allen A. Telemedicine technology and clinical applications. 61. Grassmann F, Mengelkamp J, Brandl C, et al. A deep learning algorithm
JAMA. 1995;273(6):483–488. for prediction of age-related eye disease study severity scale for age-related
macular degeneration from color fundus photography. Ophthalmology.
41. Wootton R, Craig J, Patterson V. Introduction to Telemedicine. CRC Press;
2018;125(9):1410–1420.
2017
62. Peng Y, Dharssi S, Chen Q, et al. DeepSeeNet: a deep learning model for
42. Hollander JE, Carr BG. Virtually perfect? Telemedicine for COVID-19. N
automated classification of patient-based age-related macular degeneration
Engl J Med. 2020;382(18):1679–1681.
severity from color fundus photographs. Ophthalmology. 2019;126(4):565–
43. Economist T. Telemedicine is essential amid the covid-19 crisis and after
575.
it. 2020. https://www.economist.com/open-future/2020/03/31/telemedicine-
63. Liefers B, Colijn JM, González-Gonzalo C, et al. A deep learning model
is-essential-amid-the-covid-19-crisis-and-after-it. Accessed July 15, 2020.
for segmentation of geographic atrophy to study its long-term natural
44. Murphy K, Smits H, Knoops AJ, et al. COVID-19 on the chest radiograph:
history. Ophthalmology. 2020;127:1086–1096.
a multi-reader evaluation of an AI system. Radiology. 2020;201874.
64. De Fauw J, Ledsam JR, Romera-Paredes B, et al. Clinically applicable
45. Mei X, Lee H-C, Diao KY. et al. Artificial intelligence – enabled
deep learning for diagnosis and referral in retinal disease. Nat Med.
rapid diagnosis of patients with COVID-19. Nat Med. 2020;26:1224 –
2018;24(9):1342–1350.
1228.
65. Xie Y, Nguyen QD, Hamzah H, et al. Artificial intelligence for
46. Ghinai I, McPherson TD, Hunter JC, et al. First known person-to-person teleophthalmology-based diabetic retinopathy screening in a national
transmission of severe acute respiratory syndrome coronavirus 2 (SARS- programme: an economic analysis modelling study. Lancet Digit Health. 2020.
CoV-2) in the USA. Lancet. 2020;395:1137–1144.
66. Vaghefi E, Hill S, Kersten HM, et al. Multimodal retinal image analysis
47. Ting DSW, Carin L, Dzau V, et al. Digital technology and COVID-19. Nat via deep learning for the diagnosis of intermediate dry age-related macular
Med. 2020;26(4):459–461. degeneration: a feasibility study. J Ophthalmol. 2020;2020:7493419.
48. Worldometer. https://www.worldometers.info/coronavirus/. Accessed June 67. Keenan TD, Clemons TE, Domalpally A, et al. Retinal specialist versus
27, 2020. artificial intelligence detection of retinal fluid from OCT: age-related eye
49. Imaging V. https://www.viperimaging.com. Accessed June 27, 2020. disease study 2: 10-year follow-on study. Ophthalmology. 2020.
ß 2021 Asia-Pacific Academy of Ophthalmology. https://journals.lww.com/apjoo | 47Sim et al Asia-Pacific Journal of Ophthalmology Volume 10, Number 1, January/February 2021
68. Chakravarthy U, Goldenberg D, Young G, et al. Automated identification related macular degeneration. Ophthalmology. 2003;110(5):
of lesion activity in neovascular age-related macular degeneration. 966 –970.
Ophthalmology. 2016;123(8):1731–1736. 82. Alster Y, Bressler NM, Bressler SB, et al. Preferential hyperacuity
69. Wintergerst MW, Schultz T, Birtel J, et al. Algorithms for the automated perimeter (PreView PHP) for detecting choroidal neovascularization study.
analysis of age-related macular degeneration biomarkers on optical Ophthalmology. 2005;112(10):1758–1765.
coherence tomography: a systematic review. Transl Vis Sci Technol. 83. Group AHSR, Chew EY, Clemons TE, et al. Randomized trial of a home
2017;6(4):10. monitoring system for early detection of choroidal neovascularization home
70. Schmidt-Erfurth U, Vogl W-D, Jampol LM, et al. Application of automated monitoring of the eye (HOME) study. Ophthalmology. 2014;121(2):535–
quantification of fluid volumes to anti-VEGF therapy of neovascular age- 544.
related macular degeneration. Ophthalmology. 2020;127:1211–1219. 84. Wang YZ, Wilson E, Locke KG, et al. Shape discrimination in age-related
71. Bhuiyan A, Wong TY, Ting DSW, et al. Artificial intelligence to stratify macular degeneration. Invest Ophthalmol Vis Sci. 2002;43(6):2055–2062.
severity of age-related macular degeneration (AMD) and predict risk of 85. Wang YZ, He YG, Mitzel G, et al. Handheld shape discrimination
progression to late AMD. Transl Vis Sci Technol. 2020;9(2):25. hyperacuity test on a mobile device for remote monitoring of visual
72. Schmidt-Erfurth U, Waldstein SM, Klimscha S, et al. Prediction of function in maculopathy. Invest Ophthalmol Vis Sci. 2013;54(8):5497–
individual disease conversion in early AMD using artificial intelligence. 5505.
Invest Ophthalmol Vis Sci. 2018;59(8):3199–3208. 86. Kaiser PK, Wang YZ, He YG, et al. Feasibility of a novel remote daily
73. Rohm M, Tresp V, Müller M, et al. Predicting visual acuity by using monitoring system for age-related macular degeneration using mobile
machine learning in patients treated for neovascular age-related macular handheld devices: results of a pilot study. Retina. 2013;33(9):1863–1870.
degeneration. Ophthalmology. 2018;125(7):1028–1036. 87. Schmid MK, Thiel MA, Lienhard K, et al. Reliability and diagnostic
74. Tsaousis KT, Empeslidis T, Konidaris VE, et al. The concept of virtual performance of a novel mobile app for hyperacuity self-monitoring in
clinics in monitoring patients with age-related macular degeneration. Acta patients with age-related macular degeneration. Eye. 2019;33(10):1584–
Ophthalmol. 2016;94(5):e353–e355. 1589.
75. Zhang N, Hoffmeyer GC, Young ES, et al. Optical coherence tomography 88. Ward E, Wickens RA, O’Connell A, et al. Monitoring for neovascular age-
reader agreement in neovascular age-related macular degeneration. Am J related macular degeneration (AMD) reactivation at home: the MONARCH
Ophthalmol. 2007;144(1):37–44. study. Eye (Lond). 2020.
76. Ritter M, Elledge J, Simader C, et al. Evaluation of optical coherence 89. https://njl-admin.nihr.ac.uk/document/download/2007200. EDNA: Early
tomography findings in age-related macular degeneration: a reproducibility Detection of Neovascular Age-related macular degeneration protocol. 2015.
study of two independent reading centres. Br J Ophthalmol. 90. Hellewell J, Abbott S, Gimma A, et al. Feasibility of controlling COVID-
2011;95(3):381–385. 19 outbreaks by isolation of cases and contacts. Lancet Glob Health.
77. Lee JX, Manjunath V, Talks SJ. Expanding the role of medical retina 2020;8:e488–e496.
virtual clinics using multimodal ultra-widefield and optical coherence 91. Saleem SM, Pasquale LR, Sidoti PA, et al. Virtual ophthalmology:
tomography imaging. Clin Ophthalmol. 2018;12:2337–2345. telemedicine in a Covid-19 era. Am J Ophthalmol. 2020;216:237–242.
78. Ahnood D, Souriti A, Williams GS. Assessing patient acceptance of virtual 92. Shehav-Zaltzman G, Segal G, Konvalina N, et al. Remote glucose
clinics for diabetic retinopathy: a large scale postal survey. Can J monitoring of hospitalized, quarantined patients with diabetes and COVID-
Ophthalmol. 2018;53(3):207–209. 19. Diabetes Care. 2020;43(7):e75–e76.
79. Crossland M, Rubin G. The Amsler chart: absence of evidence is not 93. Annis T, Pleasants S, Hultman G, et al. Rapid implementation of a
evidence of absence. Br J Ophthalmol. 2007;91(3):391–393. COVID-19 remote patient monitoring program. J Am Med Inform Assoc.
80. Trevino R. Recent progress in macular function self-assessment. 2020;27:1326–1330.
Ophthalmic Physiol Opt. 2008;28(3):183–192. 94. Vision N. Notal Vision Technology. 2020. https://notalvision.com/
81. Loewenstein A, Malach R, Goldstein M, et al. Replacing the technology/home-oct. Accessed August 26, 2020.
Amsler grid: a new method for monitoring patients with age- 95. Alleye. Alleye. 2020. https://alleye.io/user. Accessed August 26, 2020.
48 | https://journals.lww.com/apjoo ß 2021 Asia-Pacific Academy of Ophthalmology.You can also read