Dietary Supplements and Young Teens: Misinformation and Access Provided by Retailers - American Academy ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Dietary Supplements and Young
Teens: Misinformation and
Access Provided by Retailers
Maguire Herriman, Laura Fletcher, Alexis Tchaconas, Andrew Adesman, MD, Ruth Milanaik, DO
BACKGROUND AND OBJECTIVE: Despite the American Academy of Pediatrics’ recommendations abstract
against pediatric use of creatine and testosterone boosters, research suggests that many
young teenagers take these dietary supplements. Our objective was to determine to what
extent health food stores would recommend and/or sell creatine and testosterone boosters
to a 15-year-old boy customer.
METHODS: Research personnel posing as 15-year-old high school athletes seeking to increase
muscle strength contacted 244 health food stores in the United States via telephone.
Researchers asked the sales attendant what supplements he/she would recommend. If a
sales attendant did not mention creatine or testosterone boosters initially, each of these
supplements was then specifically asked about. Supplement recommendations were
recorded. Sales attendants were also asked if a 15-year-old could purchase these products
on his own in the store.
RESULTS: A total of 67.2% (164/244) of sales attendants recommended creatine: 38.5%
(94/244) recommended creatine without prompting, and an additional 28.7% (70/244)
recommended creatine after being asked specifically about it. A total of 9.8% (24/244)
of sales attendants recommended a testosterone booster. Regarding availability for sale,
74.2% (181/244) of sales attendants stated a 15-year-old was allowed to purchase creatine,
whereas 41.4% (101/244) stated one could purchase a testosterone booster.
CONCLUSIONS: Health food store employees frequently recommend creatine and testosterone
boosters for boy high school athletes. In response to these findings, pediatricians should
inform their teenage patients, especially athletes, about safe, healthy methods to improve
athletic performance and discourage them from using creatine or testosterone boosters.
Retailers and state legislatures should also consider banning the sale of these products to
minors.
Division of Developmental and Behavioral Pediatrics, Steven and Alexandra Cohen Children’s Medical Center of WHAT’S KNOWN ON THIS SUBJECT: Teenage boy
New York, North Shore–Long Island Jewish Health System, Lake Success, New York athletes often take supplements to improve their
Mr Herriman helped conceptualize and design the study, performed the data collection and performance and typically purchase these supplements
analysis, drafted the initial manuscript, and approved the final manuscript; Ms Fletcher helped at health food stores. To date, however, no studies have
design the study, performed the screening calls, edited the initial manuscript, and approved the analyzed the recommendations these stores make to
final manuscript; Ms Tchaconas performed the statistical analysis, edited the initial manuscript, young teenage boys about supplement use.
and approved the final manuscript; Dr Adesman helped conceptualize and design the study,
WHAT THIS STUDY ADDS: This study documents that
guided the data analysis, reviewed the manuscript, and edited the final manuscript; Dr Milanaik
health food stores nationally often recommend age-
helped conceptualize and design the study, guided the data analysis, reviewed the initial
manuscript, and edited the final manuscript. restricted supplements to young boy teenagers. It
highlights the need to review how supplements are
DOI: 10.1542/peds.2016-1257 promoted and the important role pediatricians play in
Accepted for publication Nov 16, 2016 counseling youth about the risks of supplement use.
To cite: Herriman M, Fletcher L, Tchaconas A, et al. Dietary Supplements and
Young Teens: Misinformation and Access Provided by Retailers. Pediatrics.
2017;139(2):e20161257
Downloaded from www.aappublications.org/news by guest on February 10, 2021
PEDIATRICS Volume 139, number 2, February 2017:e20161257 ARTICLEYoung boy athletes often perceive been associated with an increased the conversion of testosterone to
themselves as less muscular than risk of compartment syndrome, a estrogen. However, the efficacy
their ideal body image, and therefore condition where pressure builds and safety of these products
may take supplements to try to in a muscle compartment and are questionable. Research on
increase their muscle mass.1,2 In prevents bloodlfow.17 Furthermore, supplemental use of testosterone
2005, Field et al3 reported that 12% because dietary supplements are boosters in adults has found that it
of boys reported using supplements subject to little oversight by the can cause polycythemia, increased
to improve appearance, muscle Food and Drug Administration blood viscosity, prostatic hyperplasia,
mass, or strength. More recently, in (FDA), the safety and efficacy of hepatotoxic effects, hepatic
a 2012 study of 2793 adolescents at supplements available on the market neoplasia and dysfunction, and the
20 urban middle and high schools in are not rigorously established.18,19 exacerbation or development of
Minnesota, 34.7% of boys reported Pomeranz et al20 note that dietary sleep apnea.21 In 1 study examining
using protein supplements, 5.9% workout supplements, such as the effectiveness of the purported
used steroids, and 10.5% used some creatine, are often adulterated with testosterone booster N-Methyl-D-
other muscle-enhancing substance.4 pharmaceutical drugs and can lead to aspartate, investigators found it
Similar prevalences were noted in adverse effects, such as hypertension, has no effect on body composition
the recent Growing Up Today study; stroke, and liver injury. or muscle performance for those
in this national cohort, 12% of boys participating in resistance training.22
An additional concern of adolescent
13 to 18 years old reported using Although less well studied, there
creatine use is that teenagers often
muscle-building products (ages are concerns that adolescent use
do not get their information on
13–15 years: 3.2%; ages 16–18 years: of testosterone boosters can also
supplement use from physicians or
9.5%).5 cause the body to shut down its
dieticians, leading to improper usage
natural production of testosterone as
Creatine is one of the most popular against medical recommendations.20
well as increase acne and halt bone
weight gain supplements among Smith and Dahm8 found that 78% of
growth.23,24
this age group; 8.8% to 21% of high school creatine users either did
high school boy athletes report not know how much creatine they
Teens commonly get information
creatine use.6–9 In a study of 37 were taking or were intentionally
about muscle supplements from
public high schools in Wisconsin, taking more than the dose
health food stores and are most
30.1% of high school football recommended on packaging provided
likely to purchase these supplements
players reported creatine use.6 by manufacturers. The same study
from these types of stores.8 Because
Clearly, there is widespread use found that 86% of creatine users
many health food stores present
of creatine among adolescents purchased their creatine at a health
their employees as “expert(s) in
despite the recommendations of the food store and that high school users
health and wellness products”25
American Academy of Pediatrics list friends and health food stores as
(GNC) or “knowledgeable, courteous,
and the American College of Sports their primary sources of information
and extensively trained Health
Medicine against creatine use by on creatine.8 These results suggest a
Enthusiasts ready to help with all
thoseprofessionals and can pose significant eligible national chain stores could be had any products that he/she
health risks. identified. For these states, additional would recommend. Recommended
national chain stores were added products were documented.
from states in the same geographic If the sales attendant did not
METHODS region as the deficient state. The 4 initially mention creatine and/or
Participants geographic regions defined by the a testosterone booster, then the
US Census Bureau (Northeast, South, researcher asked the sales attendant
This study identified 300 health Midwest, and West) were used for for recommendations regarding
food stores in the United States for this purpose. An additional 100 these products. Creatine and
inclusion in this study. Forty-nine nonnational retailers (25 per region) testosterone boosters were asked
states were included in the sample. were identified using the Web site about in separate questions, and the
The institutional review board (IRB) www.VPXSports.com. This Web site sales attendants’ recommendations
required that New Jersey be excluded was used because it offers a registry on each were documented. The
due to pending state legislation that of health food store locations that is researcher also asked whether
would ban the sale of creatine to searchable on a state-by-state basis. he could purchase creatine or a
minors (www.njleg.state.nj.us/2006/ testosterone booster on his own
Bills/S2000/1951_I1.PDF). In each From the initial sample of 300 stores,
in the store. Again, the ability to
of the other states, sale of creatine stores were excluded if they did not
purchase creatine or a testosterone
and testosterone boosters to minors require that all employees were >18
booster without a parent or adult
was legal at the time of the study. years of age. These age requirements
guardian was asked about in separate
Although Massachusetts introduced were introduced at the direction of
questions, and the sales attendant’s
a bill in January 2015 to ban the sale the IRB. The 2 national chain retailers
responses to both questions were
of dietary supplements for weight included in this study require that
documented.
loss or muscle building to minors, sales attendants are at least 18 years
this study was conducted in August old. For the nonnational retailers, This study protocol was approved
2014, before the introduction of a female researcher made initial by the IRB at North Shore–Long
that legislation (https://cdn1.sph. screening calls to the 100 identified Island Jewish Health System. Our
harvard.edu/wp-content/uploads/ locations and asked about the age application to the IRB acknowledged
sites/1267/2015/09/Massachusetts- requirements for employment. Stores the fact that the protocol required
House-Bill-No.-34711.pdf). Both the that employed minors or that were elements of deception and that
New Jersey and Massachusetts bills out of business were excluded. A informed consent could therefore
ultimately failed to be signed into store was considered out of business not be obtained from respondents.
law. if researchers were not able to Protocol modifications were
connect on a screening call after 3 required by the IRB to ensure that
A health food store was defined as
separate attempts during normal all respondents were >18 years
a store that primarily sells dietary
business hours. Sixty-six nonnational of age, that the data would be
supplements. This study divided
retailers were excluded by these de-identified with respect to the
health food stores into 2 categories:
criteria. The final sample consisted of identity of the retailers, and that New
national chain and nonnational
244 health food stores, of which 200 Jersey would be excluded for fear of
retailers. A national chain was
were national chain locations and 44 self-incrimination.
defined as a retailer that operates
were nonnational retailers.
at least 1 store in at least 45 states
Data Handling and Statistical
nationwide. Two national chains of
Procedures Analysis
health food stores were identified
that fit this criterion. A nonnational A 20-year-old male researcher For each retail store location, data for
retailer was any health food store contacted each health food store in creatine and testosterone boosters
that did not fit this criterion. the sample by phone during normal were documented separately. If
Nonnational retailers may operate business hours. All calls were made a sales attendant recommended
regionally or as independently owned during August 2014. Once a sales not using a supplement either
and operated single-store locations. attendant answered the phone, the initially or after prompting, this was
The initial national sample consisted researcher identified himself as a recorded as “recommend against.”
of 200 national chain locations and 15-year-old football player going If a sales attendant recommended
100 nonnational retailers. Although into his sophomore year of high a supplement after initially asking
the intent was to have 4 national school. The researcher then stated for any recommendations, this
chain stores in each state included that he was doing strength training was recorded as “recommend
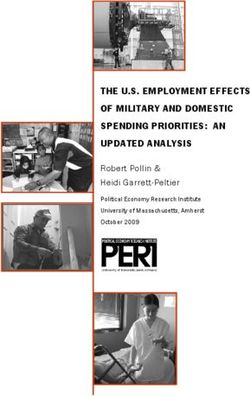
in the study, in some states,TABLE 1 Telephone Recommendations Regarding Creatine and Testosterone Boosters Table 1 summarizes sales attendants’
Testosterone Booster Total recommendations for creatine
Recommend Recommend Recommended Refused to Make (Creatine) and testosterone boosters. Of
Without After Prompt Against Recommendation the 164 sales attendants who
Prompta Over the Phone recommended creatine, only 13.4%
Creatine Recommend 0 15 78 1 94 also recommended testosterone
without prompt boosters. Twenty-two of the 24
Recommend after 1 6 63 0 70 sales attendants who recommended
prompt
testosterone boosters had also
Recommended 1 1 72 0 74
against recommended creatine. Of the 2
Refused to make 0 0 3 3 6 sales attendants who recommended
recommendation a testosterone booster without
over the phone prompting, 1 recommended creatine
Total (testosterone booster) 2 22 216 4 244
after prompting and 1 did not
Recommendations were made by sales attendants at 244 health food stores in the United States to a researcher (MH) recommend creatine.
posing as a 15-year-old high school sophomore who wants to do strength training in preparation for football.
a All units are counts of number of sales attendants (n = 244).
Although male sales attendants
were significantly more likely
attendant did not spontaneously a 15-year-old boy. A total of 38.5% to recommend creatine without
suggest a supplement initially, (94/244) recommended creatine prompting than female sales
but then recommended it when without prompting. An additional attendants (χ2 = 7.81, P = .005),
asked specifically about it, this was 28.7% (70/244) recommended no sex difference was found for
recorded as “recommend after creatine after prompting. A total of creatine recommendation after
prompting.” Sales attendants who 30.3% (74/244) of sale attendants prompting (χ2 = 0.33, P = .57). No sex
refused to make a recommendation recommended against creatine, difference was noted for testosterone
over the phone were recorded as “no whereas 2.5% (6/244) refused to booster recommendation. No other
recommendation offered.” make a recommendation on creatine significant differences were found for
use over the phone. A total of 74.2% either supplement when comparing
For both creatine and testosterone
(181/244) of sales attendants stated results by region or store type.
boosters, the percentage of sales
that a 15-year-old could purchase
attendants in each of the 4 response Research personnel noted that
creatine on his/her own, whereas
categories detailed above was in many instances, when asked
22.5% (55/244) stated one had to
calculated. The percentage of sales if the teen caller could purchase
be ≥18 years of age to purchase
attendants who stated that a 15-year- either product independently, sales
creatine.
old could purchase each supplement attendants reviewed the labels of
was also calculated. Responses were Overall, 9.8% (24/244) of all the actual products or scanned the
analyzed by region (Northeast, South, sales attendants recommended products at their checkout counter
Midwest, or West), sex of the sales a testosterone booster. Only 2 looking for additional information.
attendant (male or female), and type sales attendants recommended Many sales attendants stated
of store (national chain or nonnational a testosterone booster without that although the label stated the
retailer) using a difference in prompting, but 9.0% (22/244) supplement was not recommended
proportions hypothesis test. Results recommended one after prompting. for thoseat health food stores.4,8 Despite the Just as health food stores were FDA can take actions only after a
American Academy of Pediatrics’ more likely to recommend creatine product is on the market in cases
and the American College of Sports for use by teens compared with where the dietary supplement is
Medicine’s recommendations testosterone boosters, sales staff adulterated (eg, unsafe), misbranded
against adolescent use of creatine were far more likely to state that (eg, misrepresentations are made on
and testosterone boosters, most a 15-year-old could purchase the product labeling), or cannot be
health food stores recommended creatine than a testosterone booster marketed as a dietary supplement
≥1 of these products to a young without an accompanying adult. (eg, an unapproved new drug).29
teenage boy. Specifically, more than Although product labels provided Thus, under its current mandate,
two-thirds of sales attendants in by supplement manufacturers often the FDA’s role with respect to
this study recommended creatine state the products are recommended dietary supplements is reactive,
to a 15-year-old, and nearly 10% for use only by adults, it is worth not proactive, thereby allowing
recommended a testosterone noting that there currently are no for unprecedented growth in the
booster. More than one-third of sales legal restrictions limiting sales of development and marketing of these
attendants recommended creatine to these supplements to minors. One untested products. Because of the
young customers even without their sales attendant highlighted this lack limited power of federal regulation,
expressing interest in it. Given that of legal restrictions by comparing the Pomeranz et al20 have suggested that
many health food stores claim that sale of dietary supplements to other individual states implement more
their sales attendants are experts in substances, stating, “It’s not like I'm proactive policies to keep children
health and wellness products and selling alcohol.” safe, such as imposing minimal
emphasize the ability of their staff age requirements on the purchase
The comparison with alcohol is
to provide consumer education, it is of dietary workout supplements
striking because, although state and
likely these recommendations will similar to those placed on alcohol
federal laws regulate the sale of
be accepted. Thus, recommendations and cigarettes. Given that annual
alcohol, cigarettes, and spray paint
from sales staff that run counter to sales of dietary supplements in the
to minors, no regulation is placed on
product labeling and expert medical United States have risen sixfold since
the sale of dietary supplements to
opinion pose potentially significant 1994 from $5.8 billion to about $35
minors. Supplements do not require
health risks to young teenagers who billion, greater consideration needs
safety approval by the FDA or other
use creatine and/or testosterone to be given to how these products are
agencies before reaching store
boosters. labeled and marketed to children and
shelves, and the process of removing
young adolescents.30
a dangerous supplement from the
Not only are many health food
market is reactionary and delayed.18,20
stores making recommendations
Furthermore, advertisements for
contrary to expert medical opinion, CONCLUSIONS
supplements often fail to include
but pediatricians themselves rarely
required disclaimers and, when
discuss supplements, such as Supplements, such as creatine and
present, they are “often presented in
creatine, with their patients. In a testosterone boosters, can pose
a hard-to-find way, whether through
2001 cross-sectional survey of 37 significant health risks if used by
tiny type or (on television) a fleeting
public high schools in Wisconsin, young adolescents. These products
appearance.”27,28 Inadequate product
12% to 13% of football players are not recommended by some
labeling, in conjunction with the fact
reported that their physicians product manufacturers for anyone
that the majority of sales personnel
recommended against creatine use,to revising their policies regarding products by minors, and conducting safeguards are introduced by retailers,
recommending products like these audits to verify compliance with states, or the FDA, pediatricians
to minors. This is especially true these policies. Furthermore, although should counsel all adolescents, not
for the national retail chains, given the Massachusetts and New Jersey just teen athletes, about the risks
their professed expertise and stated bills mentioned above that would associated with supplement use.
concern for consumer health and have restricted the sale of creatine
safety. Simple solutions could include and other supplements to minors ABBREVIATIONS
improving the knowledge of their staff both failed to gain the power of law,
FDA: Food and Drug
about supplements not recommended states should consider introducing
Administration
for youth, enabling their point-of-sale and passing similar legislation to
IRB: institutional review board
software to caution about use of these address this problem. Until additional
Address correspondence to Ruth Milanaik, DO, Division of Developmental and Behavioral Pediatrics, Steven and Alexandra Cohen Children’s Medical Center of New
York, 1983 Marcus Ave, Suite 130, Lake Success, NY 11042. E-mail: rmilanai@northwell.edu
PEDIATRICS (ISSN Numbers: Print, 0031-4005; Online, 1098-4275).
Copyright © 2017 by the American Academy of Pediatrics
FINANCIAL DISCLOSURE: The authors have indicated they have no financial relationships relevant to this article to disclose.
FUNDING: No external funding.
POTENTIAL CONFLICT OF INTEREST: The authors have indicated they have no potential conflicts of interest to disclose.
REFERENCES
1. Raudenbush B, Meyer B. Muscular 7. Metzl JD, Small E, Levine SR, Gershel Available at: www.pediatrics.org/cgi/
dissatisfaction and supplement JC. Creatine use among young athletes. content/full/117/3/e577
use among male intercollegiate Pediatrics. 2001;108(2):421–425
14. Laos C, Metzl JD. Performance-
athletes. J Sport Exerc Psychol.
8. Smith J, Dahm DL. Creatine use enhancing drug use in young athletes.
2003;25(2):161–170
among a select population of high Adolesc Med Clin. 2006;17(3):719–731,
2. Alves C, Lima RVB. Dietary supplement school athletes. Mayo Clin Proc. abstract xii
use by adolescents. J Pediatr (Rio J). 2000;75(12):1257–1263
15. Souza RA, Miranda H, Xavier M, et
2009;85(4):287–294 9. Kayton S, Cullen RW, Memken JA, Rutter al. Effects of high-dose creatine
3. Field AE, Austin SB, Camargo CA Jr, R. Supplementation and ergogenic aid supplementation on kidney and
et al. Exposure to the mass media, use by competitive male and female liver responses in sedentary and
body shape concerns, and use of high school athletes. Med Sci Sports exercised rats. J Sports Sci Med.
supplements to improve weight Exerc. 2002;34(5):S193 2009;8(4):672–681
and shape among male and female 10. Gomez J; American Academy of 16. Lopez RM, Casa DJ, McDermott BP,
adolescents. Pediatrics. 2005;116(2). Pediatrics Committee on Sports Ganio MS, Armstrong LE, Maresh
Available at: www.pediatrics.org/cgi/ Medicine and Fitness. Use of CM. Does creatine supplementation
content/full/116/2/e214 performance-enhancing substances. hinder exercise heat tolerance or
4. Eisenberg ME, Wall M, Neumark- Pediatrics. 2005;115(4):1103–1106 hydration status? A systematic review
Sztainer D. Muscle-enhancing 11. Terjung RL, Clarkson P, Eichner ER, with meta-analyses. J Athl Train.
behaviors among adolescent et al; American College of Sports 2009;44(2):215–223
girls and boys. Pediatrics. Medicine. American College of Sports 17. Hile AM, Anderson JM, Fiala KA,
2012;130(6):1019–1026 Medicine roundtable. The physiological Stevenson JH, Casa DJ, Maresh CM.
5. Calzo JP, Sonneville KR, Scherer and health effects of oral creatine Creatine supplementation and anterior
EA, Jackson B, Austin SB. Gender supplementation. Med Sci Sports compartment pressure during
conformity and use of laxatives Exerc. 2000;32(3):706–717 exercise in the heat in dehydrated
and muscle-building products in 12. Grunewald KK, Bailey RS. Commercially men. J Athl Train. 2006;41(1):30–35
adolescents and young adults. marketed supplements for
18. Rodriguez NR, Di Marco NM, Langley
Pediatrics. 2016;138(2):e20154073 bodybuilding athletes. Sports Med.
S; American Dietetic Association;
1993;15(2):90–103
6. McGuine TA, Sullivan JC, Bernhardt Dietitians of Canada; American
DT. Creatine supplementation in high 13. Calfee R, Fadale P. Popular ergogenic College of Sports Medicine. American
school football players. Clin J Sport drugs and supplements in young College of Sports Medicine position
Med. 2001;11(4):247–253 athletes. Pediatrics. 2006;117(3). stand. Nutrition and athletic
Downloaded from www.aappublications.org/news by guest on February 10, 2021
6 HERRIMAN et alperformance. Med Sci Sports Exerc. supplementation with the alleged 27. Giasone F. The Vitamin Shoppe opens
2009;41(3):709–731 testosterone booster Nmda has no its doors on route 23. Patch. August 11,
19. Cohen PA. Hazards of hindsight-- effect on body composition, muscle 2011. Available at: http://patch.com/
monitoring the safety of nutritional performance, and serum hormones new-jersey/triboro/the-vitamin-shoppe-
supplements. N Engl J Med. associated with the hypothalamo- opens-its-doors-on-route-23. Accessed
2014;370(14):1277–1280 pituitary-gonadal axis in resistance- February 10, 2016
trained males. J Sports Sci Med. 28. Morris CA, Avorn J. Internet
20. Pomeranz JL, Barbosa G, Killian C, 2014;13(1):192–199 marketing of herbal products. JAMA.
Austin SB. The dangerous mix of
24. Ahrendt DM. Ergogenic aids: 2003;290(11):1505–1509
adolescents and dietary supplements
counseling the athlete. Am Fam 29. Kesselheim AS, Connolly J, Rogers
for weight loss and muscle building:
Physician. 2001;63(5):913–922 J, Avorn J. Mandatory disclaimers
legal strategies for state action.
J Public Health Manag Pract. 25. Giorgi A, Weatherby RP, Murphy PW. on dietary supplements do not
2015;21(5):496–503 Muscular strength, body composition reliably communicate the intended
and health responses to the use of issues. Health Aff (Millwood).
21. Lattavo A, Kopperud A, Rogers PD.
testosterone enanthate: a double 2015;34(3):438–446
Creatine and other supplements. Pediatr
blind study. J Sci Med Sport. 30. Ostroff S. Making progress
Clin North Am. 2007;54(4):735–760, xi
1999;2(4):341–355 in protecting consumers from
22. Rhoden EL, Morgentaler A. Risks of
26. GNC. GNC sales associate, retail unsafe supplements. Available at:
testosterone-replacement therapy and
part time in New York, NY. Available http://blogs.fda.gov/fdavoice/index.
recommendations for monitoring. N
at: http://gnc.jobs/new-york-ny/ php/2016/01/making-progress-in-
Engl J Med. 2004;350(5):482–492
sales-associate-retail-part-time/ protecting-consumers-from-unsafe-
23. Willoughby DS, Spillane M, Schwarz FC3E8B47A17E44CFA7231F51B5341DFE/ supplements/. Accessed January 22,
N. Heavy resistance training and job/. Accessed February 10, 2016 2016
Downloaded from www.aappublications.org/news by guest on February 10, 2021
PEDIATRICS Volume 139, number 2, February 2017 7Dietary Supplements and Young Teens: Misinformation and Access Provided by
Retailers
Maguire Herriman, Laura Fletcher, Alexis Tchaconas, Andrew Adesman and Ruth
Milanaik
Pediatrics originally published online January 2, 2017;
Updated Information & including high resolution figures, can be found at:
Services http://pediatrics.aappublications.org/content/early/2016/12/29/peds.2
016-1257
References This article cites 27 articles, 6 of which you can access for free at:
http://pediatrics.aappublications.org/content/early/2016/12/29/peds.2
016-1257#BIBL
Subspecialty Collections This article, along with others on similar topics, appears in the
following collection(s):
Adolescent Health/Medicine
http://www.aappublications.org/cgi/collection/adolescent_health:med
icine_sub
Sports Medicine/Physical Fitness
http://www.aappublications.org/cgi/collection/sports_medicine:physi
cal_fitness_sub
Permissions & Licensing Information about reproducing this article in parts (figures, tables) or
in its entirety can be found online at:
http://www.aappublications.org/site/misc/Permissions.xhtml
Reprints Information about ordering reprints can be found online:
http://www.aappublications.org/site/misc/reprints.xhtml
Downloaded from www.aappublications.org/news by guest on February 10, 2021Dietary Supplements and Young Teens: Misinformation and Access Provided by
Retailers
Maguire Herriman, Laura Fletcher, Alexis Tchaconas, Andrew Adesman and Ruth
Milanaik
Pediatrics originally published online January 2, 2017;
The online version of this article, along with updated information and services, is
located on the World Wide Web at:
http://pediatrics.aappublications.org/content/early/2016/12/29/peds.2016-1257
Pediatrics is the official journal of the American Academy of Pediatrics. A monthly publication, it
has been published continuously since 1948. Pediatrics is owned, published, and trademarked by
the American Academy of Pediatrics, 345 Park Avenue, Itasca, Illinois, 60143. Copyright © 2017
by the American Academy of Pediatrics. All rights reserved. Print ISSN: 1073-0397.
Downloaded from www.aappublications.org/news by guest on February 10, 2021You can also read