DIAGNOSING AN MI ECG: Tips and Tricks - Dr Ahmed Vachiat - SA Heart Congress
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

DIAGNOSING AN MI
ECG: Tips and Tricks
Dr Ahmed Vachiat
MBBCh (Wits) FCP(SA) MMed Cert Cardiology (SA)
Wits Donald Gordon Medical Centre
Sunninghill and Sunward Park Hospitals
CLINICAL CRITERIA FOR MI “The clinical definition of MI denotes the presence of acute myocardial injury detected by abnormal cardiac biomarkers in the setting of evidence of acute myocardial ischaemia”


Fourth Universal definition of myocardial infarction, European Heart Journal 2018

Fourth Universal definition of myocardial infarction, European Heart Journal 2018

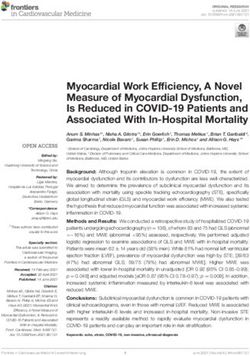
Normal ECG

Normal ≤100ms

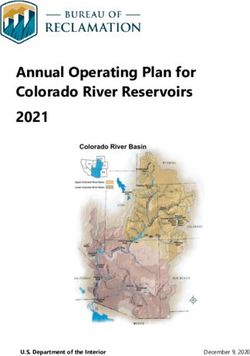
Case Study 1 65y old male patient Typical chest pain at home @ 18h00 Presents to Casualty @ 20h30 Haemodynamically stable

ECG @ 21h00

Thrombolytic? Primary PCI?
Chest pain with ST elevation ▪ Give thrombolytic within 30 minutes (if no contraindications within 12 hours) ▪ Primary PCI (If door to wire time less than 90 minutes)
Tip 1
Look at entire ECG for clues !
• Rate
Massive anterior MI ➔ tachycardia
Pulmonary embolism ➔tachycardia
Inferior MI with heart block ➔ bradycardia
• Rhythm
Arrhythmias can also raise troponin
• Shape of ST elevation
Concave up : myocardial infarction
Convex up : pericarditisDifferential diagnosis of ST elevation
Myocardial infarction
Prinzmetal angina, Takotsubo syndrome
Postmyocardial infarction
Acute pericarditis
Normal variant (“early repolarization”)
LBBB, LVH
Myocardial contusion, Myocarditis
Hypothermia
Post DC cardioversion
Intracranial haemorrhage
Hyperkalaemia
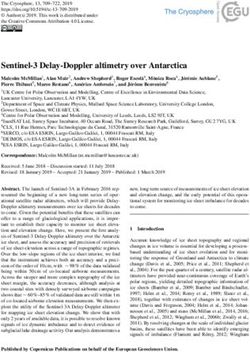
HypercalcaemiaCase Study 2 • 70y old male • Atypical chest pain after collapsing at home @18h00 • Presents to Casualty @ 20h30
ECG Changes : STEMI
All leads 1.0mm (besides Lead V2-3)
Lead V2-3
Male Female
>1.5mm
40y
>2.5mm >2.0mmTip 2 Look at the ECG with the company it keeps! Not all chest pain is myocardial infarction
Case Study 3 • 80y female • Chest pain 1 day after total hip replacement • Diabetic and hypertension
Tip 3
Use other investigations to come to
final diagosis!
Bloods
Exercise stress tests
Echocardiography
CT scans
MRI
Nuclear Medicine studies+ Troponins
2015 ESC Guidelines for the management of ACS in patients without persistent ST-segment elevation
>50% >20%
Anterior STEMI
VERY NB
TIME Goals
First medical contact (FMC) to first ECG ≤ 10 min
FMC to fibrinolysis ≤ 30 min
FMC to PPCI (PCI capable) ≤ 90 min
FMC to PPCI (PCI capable and within 2 hours of symptom onset) ≤ 60 min
Primary PCI rather than fibrinolysis ≤ 120 min
Primary PCI rather than fibrinolysis (if large area at risk) ≤ 90 min
Successful fibrinolysis t0 angiography 3-24hr
ESC STEMI guidelines 2015Atypical presentations that deserve
prompt management
LBBB
Ventricular paced rhythm
Persistent ischaemic symptoms
Posterior MI
ST elevation aVRAnterior STEMI
Acute inferior STEMI
RBBB and anterior MI
Diagnosis of STEMI in the presence of
LBBB (Sgarbossa et al)
ST segment elevation ≥ 1 mm concordant with QRS (5)
ST segment depression ≥ 1 mm in V1, V2 or V3 (3)
ST segment elevation ≥ 5 mm discordant with QRS (2)
Score of ≥ 3 – Spec > 90% and PPV of 88% .LBBB and inferior MI
Acute MI: ECG subsets, correlation with artery and mortality
Category Anatomy of ECG 30 day 1 year
occlusion mortality (%) mortality (%)
Proximal LAD Proximal to first ST ↑ V1-6, I, aVL 19.6 25.6
septal perforator and fasicular or
BBB
Mid LAD Proximal to ST ↑ V1-6, I, aVL 9.2 12.4
diagonal but
distal to first
septal perforator
Distal LAD or Distal to ST ↑ V1-4, or I, 6.8 10.2
diagonal diagonal aVL, V5-6
Moderate to Proximal RCA or ST ↑ II, III, aVF and 6.4 8.4
large inferior cicumflex any below:
(posterior, a. V1, V3R, V4R
lateral, RV) b. V5-6
c. R>S in V1,V2
Small inferior Distal RCA or cx ST ↑ II, III, aVF 4.5 6.7
onlyEchocardiography
Risk scores
Case study 4 55 year old male Coughing for 2 weeks Presents with chest pain for 12 hours
a) Give IV streptokinase b) Do emergency PCI (percutaneous coronary intervention) c) Give paracetamol tablets d) Give sublingual nitrates e) Start antibiotics
Typical ECG for acute pericarditis ◆ PR segment elevation in aVR, ◆ depression in inferior leads ◆ together with widespread ST elevation.
a) Give IV streptokinase b) Do emergency PCI (percutaneous coronary intervention) c) Give paracetamol tablets d) Give sublingual nitrates e) Start antibiotics
ECG Tips for diagnosing myocardial infarction 1) Look at entire ECG for clues 1) Look at the ECG with the company it keeps! 1) Use other investigations to come to final diagosis
You can also read