DIABETE: È TEMPO DI RICLASSIFICAZIONE? - DIPARTIMENTO DI MEDICINA CLINICA, SANITÀ PUBBLICA, SCIENZE DELLA VITA E DELL'AMBIENTE (MESVA) UNIVERSITÀ ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Diabete: è tempo di
riclassificazione?
Marco Giorgio Baroni
Dipartimento di Medicina Clinica, Sanità Pubblica,
Scienze della Vita e dell’Ambiente (MeSVA)
Università dell’Aquila
Il Prof Marco Giorgio Baroni dichiara di aver ricevuto negli ultimi due anni compensi o finanziamenti dalle seguenti Aziende Farmaceutiche e/o Diagnostiche: - Novo Nordisk - Sanofi - Lilly - MSD - Boehringer Ingelhaim - Astra Zeneca Dichiara altresì il proprio impegno ad astenersi, nell’ambito dell’evento, dal nominare, in qualsivoglia modo o forma, aziende farmaceutiche e/o denominazione commerciale e di non fare pubblicità di qualsiasi tipo relativamente a specifici prodotti di interesse sanitario (farmaci, strumenti, dispositivi medico-chirurgici, ecc.).
Precision medicine in diabetes
• Precision medicine in diabetes refers to an approach to optimise the
diagnosis, prediction, prevention or treatment of diabetes by integrating
multidimensional data, accounting for individual differences.
• Precision diagnostics: refining the characterisation of diabetes to
optimise therapies and/or prognostication using information about
a person’s unique biology, environment and/or context
Precision medicine in diabetes: a Consensus Report from ADA and EASD. Diabetologia 2020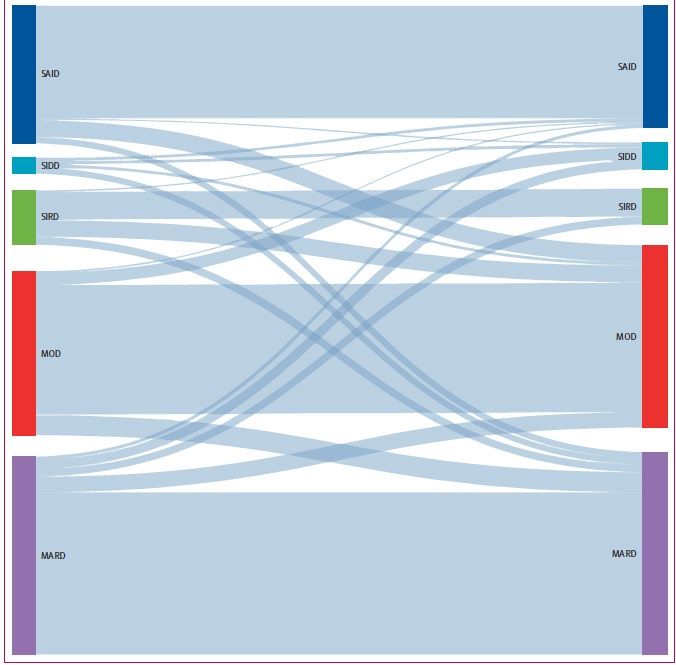

La parola diabete identifica un gruppo di disordini
cronici che condividono la presenza di iperglicemia
L’iperglicemia è il prodotto finale di una serie di
processi.
La sola iperglicemia è sufficiente per caratterizzare
adeguatamente la patologia?
Hypoglycaemia
Side effects of
medications
PAD
Obesity
Age Myocardial
ischaemia
High blood
pressure
Dyslypidemia
Retinopathy
Neuropathy Nephropathy
Disease Stroke
duration
Race Gender
Life
expectancy
Modified from De Fronzo RA. Diabetes 2009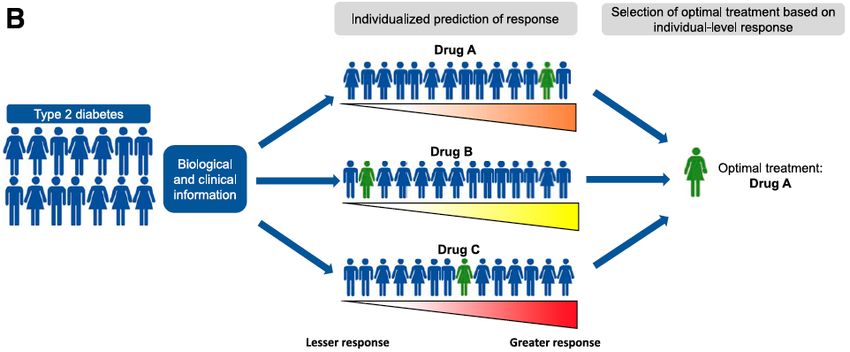
Iperglicemia Biomarkers Clusters Terapia
Subtype A
Disease pathways
Risk of complications
Subtype B
Disease pathways
Risk of complications
Subtype C
Disease pathways
Risk of complications
Subtype D Disease pathways
Risk of complications
Autoimmunity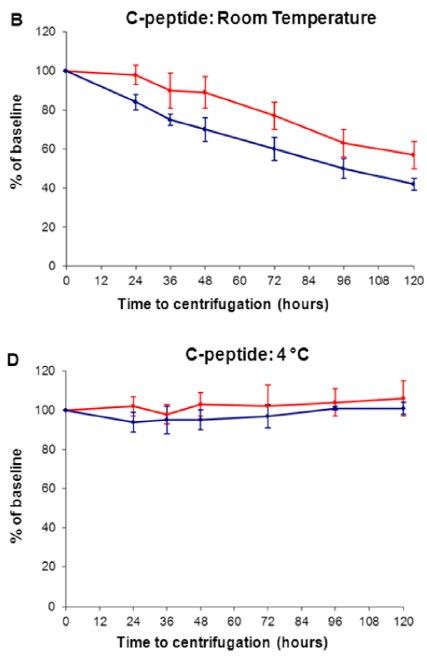
Type 2 diabetes genetic loci* informed by multi-trait
associations point to disease mechanisms and subtypes: A
soft clustering analysis
Udler MS, et al. (2018) PLOS Medicine 15(9): e1002654. *94 T2D-associated variants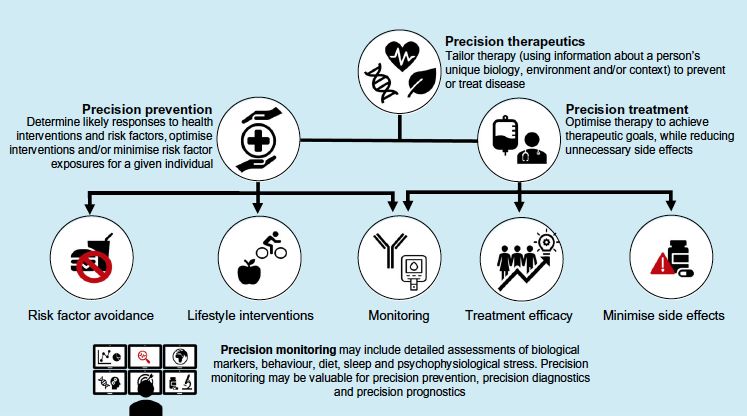
Associations of cluster genetic risk scores and
clinical outcomes from GWAS
Udler MS, et al. (2018) PLOS Medicine 15(9): e1002654.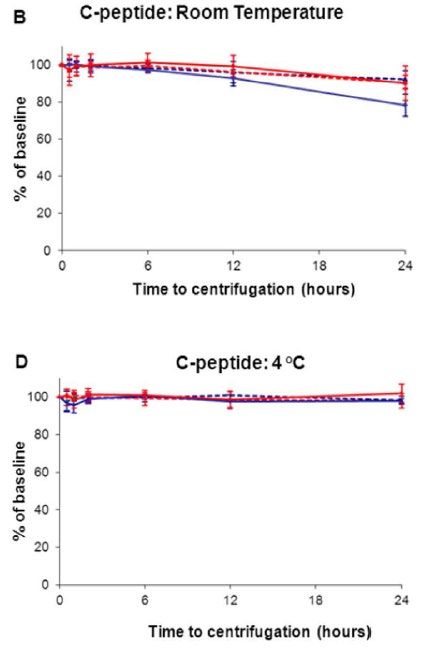
Diabete tipo 2 e fenotipi
Età di
BMI HbA1c GADA HOMA2_B* HOMA2_IR*
esordio
CLUSTER 1 9000 pazienti
Si svedesi con diabete
Severe Autoimmune GADA+
Diabetes (SAID) neo-diagnosticato
No ANDIS cohort
K-means clustering
CLUSTER 2 CLUSTER 3 CLUSTER 4 CLUSTER 5
Severe Insulin-Deficient Severe Insulin-Resistant Mild Obesity-Related Mild Age-Related
Diabetes (SIDD) Diabetes (SIRD) Diabetes (MOD) Diabetes (MARD)
• ↓ Età di esordio • ↑ HOMA2_IR • Lieve HOMA2_IR • Esordio in età avanzata
• ↓ BMI • ↑ BMI • ↑ BMI • Modeste alterazioni
• ↑ HbA1c • ↑ Età di esordio metaboliche
• ↓ HOMA2_B
(*c-peptide)
Ahlqvist E et al., Lancet Diabetes Endocrinol ,2018Clusters e rischio di complicanze
Time to chronic kidney Time to diabetic retinopathy
Time to coronary events
disease (≥stage 3B) (mild-non-proliferative &
proliferative)
SIRD
No differences in age and sex-
SIDD
adjusted model
MARD
SIRD
MARD
SIDD
SAID
MOD
Ahlqvist E et al., Lancet Diabetes Endocrinol 2018Diabetes cluster: comments • This approach cannot be easily implemented in the clinical setting due to the need for elaborate cluster analyses of markers that are not easy to obtain (i.e fasting insulin or C-peptide), especially in healthcare systems with limited resources. • The key question for any subgroup analysis is the clinical utility of the subgroups, and in particular whether the proposed subgroups differ in response to therapy, which could help to inform treatment strategies • The clinical relevance of these approaches to dissect type 2 diabetes heterogeneity, in terms of guiding personalization of diagnosis and of therapeutic decisions, remainsd to be determined, although it seems so far rather limited
C-peptide blood sample handling
• C-peptide in whole blood collected in EDTA and measured
using modern immunoassay analysers is stable at room
temperature for at least 24h
• C-peptide in blood collected into serum gel or plain sample
tubes is stable for 6h, but shows marked degradation by
24h at room temperature
Centrifuged Whole blood
serum gel
K+-EDTA
McDonald TJ et al., PlosOne 2012In conclusion, our data confirms that blood glucose levels modulate the pancreatic insulin secretion; glycemic normalization significantly reduced both basal and post-glucagon C- peptide release J. Endocrinol. Invest. 15: 143-146,1992
Unità di misura, indicazioni e cut off nella
pratica clinica
1 ng/ml = 1 μg/l = 0.333 nmol/l
1 nmol/l = 1000 pmol/l = 3 ng/ml
Jones AG & Hattersley AT, Diab Med 2013Fasting, random or post-stimulation?
• While formal stimulation tests are most accurate and reproducible for
research purposes, a fasting or non-fasting (‘random’) sample is
usually suitable in clinical practice if the sampling conditions (timing
relative to food and concurrent glucose over 8 mmol/l ) are known.
•
Jones AG & Hattersley AT, Diabet Med 2013Inquadramento ambulatoriale: nel primo approccio al
paziente di quali elementi disponiamo?
Raccolta
anamnestica Misure Dati di
• Familiarità antropometriche laboratorio:
• Età e modalità • Body Mass • HbA1c
di esordio Index (BMI) • glicemia
• Complicanze • Circonferenza • esame urine
• Terapia vita • funzione
farmacologica renale etcApproccio basato sui clusters o su semplici caratteristiche
cliniche?
• Riproducibilità dei clusters nella
popolazione del trial ADOPT e
RECORD
• ADOPT trial of glycaemic
durability, randomly assigned to
metformin, sulfonylurea
(glibenclamide), or
thiazolidinedione (rosiglitazone)
monotherapy for up to 5 years
(n=4351).
• RECORD study (n=4447), a
cardiovascular outcomes trial in
individuals with established type 2
diabetes, initiating the same drug
classes as in ADOPT
(Sulfonylurea and rosiglitazone)
but as dual second-line therapy,
for up to 6 years.
Dennis J.M et al, Lancet Diabetes Endocrinol, 2019 ANDIS cohortApproccio basato sui clusters o su semplici caratteristiche
cliniche?
L’utilizzo di un modello basato su semplici caratteristiche cliniche,ottiene risultati sovrapponibili rispetto ai clusters
nella predizione delle complicanze (età all’esordio per la progressione del diabete)
Dennis J.M et al, Lancet Diabetes Endocrinol, 2019Renal progression by cluster in ADOPT over 5 years In ADOPT and RECORD, baseline eGFR explained a greater proportion of variation than did the clusters Estimated glomerular filtration rate at baseline was a better predictor of time to chronic kidney disease Dennis J.M et al, Lancet Diabetes Endocrinol, 2019
Approccio basato sui clusters o su semplici caratteristiche
cliniche*?
Change in HbA1c over 3 years
in concordant and discordant
treatment selection groups
• (A) ADOPT development
cohort (n=3785), clusters
strategy (left panel) and clinical
features strategy (right panel).
• (B) RECORD validation
cohort(n=4057), clusters
strategy (left panel) and clinical
features strategy (right panel).
* [four simple clinical measures
(age, sex, baseline HbA1c,and
BMI)]
Dennis J.M et al, Lancet Diabetes Endocrinol, 2019Approccio basato sui clusters o su semplici caratteristiche
cliniche?
• We found differences in incidence of chronic kidney disease between
clusters; however, estimated glomerular filtration rate at baseline was a
better predictor of time to chronic kidney disease.
• Clusters differed in glycaemic response, with a particular benefit for
thiazolidinediones in patients in the severe insulin-resistant diabetes cluster
and for sulfonylureas in patients in the mild age-related diabetes cluster.
• However, simple clinical features outperformed clusters to select therapy for
individual patients.
• The proposed data-driven clusters differ in diabetes progression and
treatment response, but models that are based on simple continuous clinical
features are more useful to stratify patients
Dennis J.M et al, Lancet Diabetes Endocrinol, 2019Polemiche!! • The study by Ahlqvist and colleagues and other attempts to characterise the heterogeneity in type 2 diabetes have identified clusters with poor clinical utility because the clusters are non-aetiological, overlapping, highly dependent on the variables used to classify them, and cannot be robustly defined at an individual level (Denis et al. 2019) • Our study provided a wealth of information beyond that of Dennis and colleagues’ study, primarily insights into the pathogenesis of type 2 diabetes and information on disease progression and outcomes. (Ahltqvist et al 2018) • The potential insights into the pathophysiology of complications in type 2 diabetes are exciting and we look forward to hearing more about this in future publications. We accept that the models we propose are constructed to accurately predict clinical outcomes and do not readily lead to pathophysiological insights. (Denis et al. 2019)
Validazioni e conferme
• We assigned participants from recent global outcomes trials (DEVOTE [n =
7637], LEADER [n = 9340] and SUSTAIN-6 [n = 3297]) to the previously
defined clusters according to age at diabetes diagnosis, baseline glycated
haemoglobin (HbA1c) and body mass index (BMI).
• No GADA, HOMA-B and HOMA-IR
• Cluster A, severe insulin-deficient diabetes (ANDIS cluster 2); Cluster B,
severe insulin-resistant diabetes (cluster 3); Cluster C, mild obesity-related
diabetes (cluster 4); and Cluster D, mild age-related diabetes (cluster 5).
Kahkoksa AR et al Diabetes Obes Metab. 2020;22:1537–1547Cumulative risk of a major adverse cardiovascular event (MACE),
cardiovascular (CV) death and all-cause death by cluster
Conclusions: Previously identified clusters can be replicated in
three geographically diverse cohorts of long-standing T2D and are
associated with cluster-specific risk profiles for additional clinical
and survival outcomes, providing further validation of the
clustering methodology.
The external validity and stability of clusters across cohorts
provides a premise for future work to optimize the clustering
approach to yield T2D subgroups with maximum predictive validity
who may benefit from subtype-specific treatment paradigms
Kahkoksa AR et al Diabetes Obes Metab. 2020Cluster redistribution at 5-year follow-up Cluster reproducibility at follow-up (ie, the proportion of patients allocated to the same cluster at baseline and follow up) was 20% SIDD, 82% SAID, 51% SIRD, 79% MOD, and 82% MARD (1105 patients with newly diagnosed type 1 or type 2 diabetes) Zaharia OP et al. Lancet Diabetes Endocrinol 2019
DCS GoDARTS ANDIS
MARD Mild age-related diabetes
• MD Mild diabetes
• MDH Mild diabetes with high
HDL-cholesterol
MOD Mild obesity-related diabetes
SIDD Severe insulin-deficient diabetes
SIRD Severe insulin-resistant diabetes
total 15,940 individuals from 3 cohorts, DCS (Netherlands),
Slieker RC et al. Diabetologia (2021) 64 september
GoDARTS (Scotland) and ANDIS (Sweden)Characteristics of the five clusters across the three cohorts; DCS (a–e), GoDARTS (g–k) and ANDIS (m–q) Slieker RC et al. Diabetologia (2021) 64 september
Meta-analysis results for time to insulin requirement Slieker RC et al. Diabetologia (2021) 64 september
Lugner M et al. Diabetologia (2021) 64 september
Diabete: è tempo di riclassificazione?
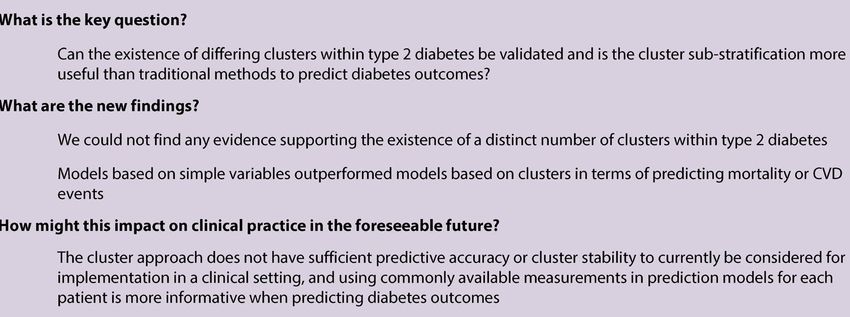
Clustering or individual prediction?
The aim of precision medicine in type 2 diabetes is to
identify people who are likely to have a greater relative
benefit from one drug class over another.• Recent demonstration of robust, clinically relevant differences in glycemic response suggest that a precision medicine approach to selecting optimal type 2 diabetes treatment will soon be possible. • The most practical way to implement this in the near future will be to focus on routine clinical markers, and the most accurate approach will be integration of continuous features into individualized, probabilistic prediction models that can be deployed at the point a decision to escalate treatment is made, rather than subtyping. • Estimates of differences in treatment response can augment the limited existing stratification of people with type 2 diabetes based on cardiovascular and renal comorbidity
Subgrouping patients diagnosed with type 2
diabetes in the routine clinical setting
Easy-to-use clinical data, such as age at diabetes onset, familial history, and
BMI
(65y)
Trischitta V et al. Current Opinion in Pharmacology 2020Subgrouping patients diagnosed with type 2 diabetes in the routine clinical setting • Hba1c at diagnosis • Creatinine and GFR • Lipid profile
Conclusioni • Il diabete è un disordine complesso con numerose manifestazioni cliniche ed una grande varietà di opzioni terapeutiche. • Le evidenze suggeriscono che la fenotipizzazione dei pazienti aiuta a predire le complicanze, comprendere ulteriori aspetti patogenetici e personalizzare la terapia • La migliore fenotipizzazione sembre essere quella basato sui parametri clinici, ma necessitiamo di ulteriori markers e modelli per i vari outcomes. • Sono necessari studi sulla risposta terapeutica alla fenotipizzazione dei pazienti.
You can also read