Design Characteristics of Worksite Environmental Interventions for Obesity Prevention
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Review
Design Characteristics of Worksite
Environmental Interventions for
Obesity Prevention
Charlotte A. Pratt,* Stephenie C. Lemon,† Isabel Diana Fernandez,‡ Ron Goetzel,§ Shirley A. Beresford,¶
Simone A. French,储 Victor J. Stevens,** Thomas M. Vogt,†† and Larry S. Webber‡‡
Abstract organizational and social contexts. The interventions, which
PRATT, CHARLOTTE A., STEPHENIE C. LEMON, are offered to all employees, include environmental- and
ISABEL DIANA FERNANDEZ, RON GOETZEL, individual-level approaches to improve physical activity
SHIRLEY A. BERESFORD, SIMONE A. FRENCH, and promote healthful eating practices. Environmental strat-
VICTOR J. STEVENS, THOMAS M. VOGT, AND egies include reducing portion sizes, modifying cafeteria
LARRY S. WEBBER. Design characteristics of worksite recipes to lower their fat contents, and increasing the ac-
environmental interventions for obesity prevention. Obesity. cessibility of fitness equipment at the workplace. Across all
2007;15:2171–2180. seven studies about 48% (N ⫽ 23,000) of the population is
Objective: This paper describes the design characteristics of randomly selected for measurements. The primary outcome
the National Heart, Lung, and Blood Institute (NHLBI)- measure is change in BMI or body weight after two years of
funded studies that are testing innovative environmental intervention. Secondary measures include waist circumfer-
interventions for weight control and obesity prevention at ence, objective, and self-report measures of physical activ-
worksites. ity, dietary intake, changes in vending machines and cafe-
teria food offerings, work productivity, healthcare use, and
Research Methods and Procedures: Seven separate studies
return on investment.
that have a total of 114 worksites (⬃48,000 employees)
Discussion: The results of these studies could have impor-
across studies are being conducted. The worksite settings
tant implications for the design and implementation of
include hotels, hospitals, manufacturing facilities, busi-
worksite overweight and obesity control programs.
nesses, schools, and bus garages located across the U.S.
Each study uses its own conceptual model drawn from the Key words: environmental-level interventions, individu-
literature and includes the socio-ecological model for health al-level interventions, physical activity, dietary intake
promotion, the epidemiological triad, and those integrating
Introduction
Received for review March 28, 2006. Overweight and obesity in the U.S. population have
Accepted in final form February 6, 2007.
The costs of publication of this article were defrayed, in part, by the payment of page reached epidemic proportions, with about 66% of U.S.
charges. This article must, therefore, be hereby marked “advertisement” in accordance with adults being overweight or obese (1). The dramatic increase
18 U.S.C. Section 1734 solely to indicate this fact.
*National Heart, Lung, and Blood Institute, Division of Epidemiology and Clinical Appli-
in prevalence of obesity over the past two decades cannot be
cations, Bethesda, Maryland; †University of Massachusetts Medical School, Division of explained by genetic changes, but by environmental factors
Preventive and Behavioral Medicine, Worcester, Massachusetts; ‡Department of Commu- that encourage increased energy intake and decreased en-
nity and Preventive Medicine, University of Rochester School of Medicine, Rochester, New
York; §Institute for Health and Productivity Studies, Cornell University, Washington, ergy expenditure (2). Environmental, community, and soci-
District of Columbia; ¶Fred Hutchinson Cancer Research Center, Seattle, Washington, and etal factors influence dietary and physical activity behaviors
University of Washington, Cancer Prevention Program, Seattle, Washington; 储University of
Minnesota, School of Public Health, Minneapolis, Minnesota; **Kaiser Permanente Center
and may foster a positive energy balance (2,3), suggesting
for Health Research, Portland, Oregon; ††Kaiser Foundation Hospitals, Center for Health that strategies for addressing the obesity epidemic must
Research, Honolulu, Hawaii; and ‡‡Tulane University School of Public Health, New include environmental approaches.
Orleans, Louisiana.
Address correspondence to Charlotte A. Pratt, National Heart, Lung, and Blood Institute, Environmental approaches use policies, programs, or or-
Division of Epidemiology and Clinical Applications, 6701 Rockledge Drive, MSC 7936, ganizational practices to influence behaviors by, for exam-
Room 10118, Bethesda, MD 20892.
E-mail: prattc@nhlbi.nih.gov
ple, increasing the availability of, and providing access to,
Copyright © 2007 NAASO healthful food choices and facilities for physical activity,
OBESITY Vol. 15 No. 9 September 2007 2171Worksite Environmental Interventions, Pratt et al.
and by creating a socially supportive environment. Such months or less). Some had modest but significant interven-
approaches do not require individuals to self-select to de- tion effects on weight after 6 months (7,8). Studies that
fined educational programs (4). Worksites are viable set- addressed environmental influences or psychosocial factors
tings for reaching large numbers of working adults of vary- as mediators or moderators of weight control were rare (8).
ing socioeconomic levels and ethnic backgrounds. A key Most of the studies were conducted in large worksites
hypothesis for research is that interventions to promote (⬎500 employees) with few racial and ethnic minorities,
behavior change in such settings could be generalizable, and a limited number had worksites as units of randomiza-
cost-effective, and sustainable. If proven effective and tion and analysis. The theoretical bases of the interventions
widely implemented, environmental interventions could and studies on cost-effectiveness or benefits were rarely
have a major impact on the health of employees and, thus, reported (8). These gaps suggest a need to determine the
on the health of the nation, as well as provide a positive effects of environmental interventions on weight and
return on corporate investments. weight-related outcomes. Toward this goal, the NHLBI
In September 2004, the National Heart, Lung, and Blood supported seven independent studies for a two-phase, four-
Institute (NHLBI)1 funded seven institutions to collaborate year program. Phase I activities include formative assess-
with worksites across the country to test interventions em- ment using methods such as focus groups, interviews with
phasizing environmental approaches to behavior change for employees and administrators, surveys, assessments of the
overweight and obesity control. These institutions are Cor- worksite environment and pilot testing of intervention com-
nell University, Washington, DC; Kaiser Permanente, Ho- ponents. Phase II includes a two-year intervention study to
nolulu, HI; Tulane University, New Orleans, LA; the Uni- test innovative strategies that have strong theoretical under-
versity of Massachusetts Medical School, Worcester, MA; pinnings, seem to be practical, cost-effective, and sustain-
the University of Minnesota, Minneapolis, MN; the Univer- able without incurring undue costs, and are being refined
sity of Rochester, Rochester, NY; and the University of based on Phase 1 activities and results.
Washington, Seattle, WA. Each study is conducted inde-
pendently under the direction of a local principal investiga-
tor. Unlike multi-site clinical trials, these studies are being Research Methods and Procedures
conducted in different types of worksites (e.g., hotels, hos- Design Characteristics
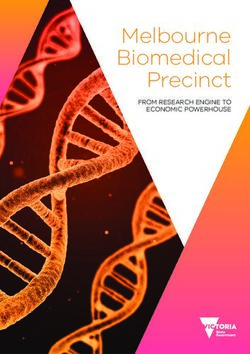
pitals, and businesses) that have diverse employee popula- Table 1 presents the design characteristics of the seven
tions. funded studies. Across the seven studies, there is a total of
The purpose of this paper is to describe these NHLBI- 114 worksites (range, 4 to 30 per study site) with about
supported studies, focusing on their design characteristics, 48,000 employees (range 1200 to 10,600 per study site),
interventions, common measures, and study collaboration. mostly low- to middle-income and from diverse racial and
These are innovative studies that emphasize environmental ethnic groups. A total of about 23,000 employees are ran-
strategies to change or modify behaviors related to diet and domly selected for measurement. Worksites are units of
physical activity for weight control and obesity prevention randomization in all of the studies; they are randomly as-
at worksites as well as examine the economic benefits of signed to intervention or comparison groups, with prior pair
such strategies. Information on the design, implementation, matching used in three studies. In all of the studies, the
and evaluation of worksite obesity management programs inclusion criteria consist of stable worksites (i.e., low turn-
could be useful to researchers designing such programs. over rates) whose administrators agree to 1) have worksites
Also, if found effective, such studies could lead to policies randomly assigned to intervention or comparison groups, 2)
and practices that enhance employee health and contribute allow assessment of consenting employees at various time-
to the financial well being and reduced healthcare needs of points within the worksite, 3) provide space or support for
employees and employers. intervention targeting the employees, and 4) encourage em-
Obesity prevention at various settings, including work- ployee participation. All assessments are being conducted
sites, emerged as a priority during NHLBI strategic plan- on work time or directly before or after shift changes and on
ning meetings held in 2000 and 2002. Documents support- site. Worksites provide time off for measurement. Each
ing worksite intervention studies include the Healthy People study was approved by a local Institutional Review Board
2010 Objectives (5) and the Surgeon General’s Call for and has a data and safety monitoring plan as well as Data
Action (6). A review of published worksite intervention and Safety Monitoring Board or other safety monitoring
studies for overweight and obesity control indicated that entity.
most interventions focused on individual-directed ap-
proaches of minimal intensity and short-term duration (6 Intervention
All of the studies use conceptual frameworks for their
interventions (Table 1), including the socio-ecological
1
Nonstandard abbreviation: NHLBI, National Heart, Lung, and Blood Institute. framework that combined theoretical views of the environ-
2172 OBESITY Vol. 15 No. 9 September 2007Table 1. Characteristics of the national worksite overweight and obesity control studies
Program name, institution
Lighten Up, Cornell Work, Weight and Step Ahead, University ACTION!, Tulane Route H, University of Images of a Healthy PACE Fred Hutchinson
University, Institute Wellness, Kaiser of Massachusetts University, Louisiana Minnesota—Twin Worksite, Univer- Cancer Research
for Health and Permanente, Medical School, Cities sity of Rochester, Center, and the
Productivity Hawaii Massachusetts New York University of
Studies, Washington, Seattle,
Washington DC Washington
Number of worksites, 12 Dow Chemical 30 hotels on the Six hospitals in central 20–23 public elementary Four transit bus garages 12 sites in a large 30 worksites within 40
type, and location Company plants in island of Oahu, Massachusetts schools in Jefferson in the Minneapolis- manufacturing miles of the Seattle
Texas, Louisiana, Hawaii Parish, Louisiana St Paul metropolitan facility in Rochester, metro area
New Jersey, and area New York
West Virginia
Employee population ⬃10,600: 94 to ⬃10,000: 18 to ⬃8400: 350 to 3500 ⬃1500: about 30 ⬃1200–1500: about ⬃13,000: about 1000– ⬃6000: 100 to 350
4202 employees 1800 employees employees per employees per school: 300 employees per 1500 employees per employees per
per worksite: per hotel: 60% hospital: 79% 93% female, 70% garage: 20% female, facility: 20% female, worksite: 33%
18% female, female, 20% female, 87% white, white, 27% black, 64% white, 34% 82% white, 11% female, 80% white,
74% white, white, 50% 6% black, 5% 2.6% Hispanics; age black, 2% Hispanics; black, 6% Hispanics, 3% black, 5%
8% black, Asian, and 30% Hispanics; age 18–65 years age 18–65 years 1% Asian, American Hispanics, 10%
7% Hispanics, Native Pacific 18–65 years (mean 47 years) Indian or Alaskan Asians; age 18 to
Worksite Environmental Interventions, Pratt et al.
11% Asian; age Islanders; age Native; age 18–65 70 years
18–65 years (mean 18–65 years years
44 years)
Number of employees 6000 6000 540 600 1200 4000 3000
randomly selected
for measurement
Study design; primary Three arm design 14 matched pairs 3 matched pairs of Worksites are random- Worksites are random- 6 matched pairs of 15 matched pairs of
outcome with worksites of worksites worksites randomly ized to intervention ized to intervention worksites randomly worksites randomly
measurement; time randomly assigned with each assigned to (N ⫽ 10) or com- (N ⫽ 2) or compari- assigned to inter- assigned to inter-
points to moderate member of a intervention or parison (N ⫽ 10) arm, son (N ⫽ 2) arm; vention or delayed vention or
(N ⫽ 4), intensive pair randomly comparison arm; stratified by East or change in BMI and intervention; change comparison arm;
(N ⫽ 5), or assigned to one change in BMI; West Bank of the body weight; effect in BMI; effect change in BMI;
comparison of two levels of effect size ⫽ 0.5 Mississippi River; size, BMI ⫽ 0.25 size ⫽ 0.8 kg/m2; effect size ⫽ 1.5
2
(N ⫽ 3) arm; intervention; kg/m ; power ⫽ change in BMI; effect kg/m2; power ⫽ power ⫽ 80%; type kg/m2; power ⫽
2
change in BMI, change in BMI, 80%; type 1 error ⫽ size ⫽ 1.0 kg/m ; 80%; type 1 error ⫽ 1 error ⫽ 0.05; 87%; type 1 error ⫽
effect size ⫽ 2.2% effect size ⫽ 0.05; ICC ⫽ 0.015; power ⫽ 80%; type 1 0.05; ICC ⫽ 0.005; ICC ⫽ 0.0005; 0.05; ICC ⫽ 0.04;
points; power ⫽ 0.11 kg/m2; baseline, 12 and error ⫽ 0.05; ICC ⫽ baseline and 24 baseline and 24 baseline and 24
80%; type 1 error power ⫽ 80%; 24 months 0.04; baseline, 12 and months months months
⫽ 0.05; ICC ⫽ type 1 error ⫽ 24 months
0.001; baseline, 0.05; ICC ⫽
12 and 24 months 0.005; baseline,
12 and 24
months
Formative research Focus groups and Quantitative and Key informant Focus groups with Interviews with bus In-depth interviews Interviews and focus
individual interviews qualitative interviews with school employees; operators; employee and focus groups groups with
with employees and assessments of administrative school principal advisory groups; with employees; employees at pilot
managers; “Leading worksite leadership; focus survey; environmental pilot testing of social mapping of worksite to identify
by Example” environments groups with audit completed by instruments, facilities; qualitative key barriers and
organizational and employee employees; study personnel recruitment methods, environmental facilitators to weight
climate survey; weight loss quantitative and intervention assessment loss
analysis of baseline intentions environmental components
medical claims and assessments;
absenteeism data; leadership and
OBESITY Vol. 15 No. 9 September 2007
environmental employee advisory
assessment groups
21732174
Table 1. Continued
Program name, institution
Intervention An integrative organi- Social-ecological Social-ecological Social-ecological model Social-ecological model Epidemiologic triad Conceptual framework
zational model model of health model of health of health behavior; of health behavior; model; employee focusing on the
including work behavior; behavior; a social modification of the increase in the motivation and worksite social and
environment, job education on marketing campaign, physical activity availability of awareness environment con-
demands and worker diet and physical leadership support, environment at healthful vending through social texts, and individual
characteristics; activity directed changes in menu schools, development machine foods and marketing, recipe behavior change;
physical activity and at individuals; options and portion of on-site physical beverages, provision modification, intervention activities
OBESITY Vol. 15 No. 9 September 2007
Worksite Environmental Interventions, Pratt et al.
healthy eating weekly group sizes in cafeteria, activity programs, of snack packs for changes in occur at three levels:
opportunities for instructional changes in vending modifications to the drivers to take along vending machine the worksite environ-
employees, access to modules, and options, a website, cafeteria and vending on their bus route; offerings and ment level, the
fitness equipment, 90-minute weekly email machines, and a social enhancement of subsidies, portion intermediate level,
weight reduction weekly newsletters, marketing campaign fitness rooms at the size reduction at and the individual
classes, healthful “Reinvent organization of promoting healthy diet garages, and reduced prices, level, as is consistent
food choices in Yourself,” a 6- walking groups, pot and increased physical organized outdoor take home with the conceptual
cafeteria and month program luck lunches, social activity; intervention physical activities for healthy meals, framework and
vending machines, for highly activities, and group- schools develop drivers stair use, active include portion size
and engagement of motivated level educational Wellness Committees commute control at cafeteria,
site leadership in employees with programs for health promotion program, active changes in vending
changing worksite BMI ⬎30 travel within machine food
culture company offerings and
instituting employee
advisory groups
Comparison worksite Health risk assessment, Level 1 interven- Pair-matched com- Intervention activities Usual offerings by the Delayed interven- Delayed intervention at
environmental and tion; strategies parison worksites will be disseminated health and fitness tion at conclusion conclusion of the
organizational include educa- continue usual to control schools at provider in the of the study study
climate assessments; tion on diet and policies and the conclusion of the garages (none targets
administrative physical activity activities; study nutrition or physical
medical claims and directed at intervention activity)
absenteeism data individuals after activities will be
completion of disseminated to
the study control hospitals at
the conclusion of the
studyWorksite Environmental Interventions, Pratt et al.
mental, individual, social, cultural, and policy factors that
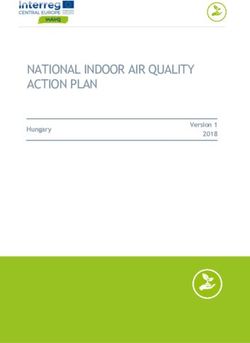
influence behaviors (9). One study uses an integrative Table 2. Examples of promotional activities and
model of worksite health promotion that emphasizes orga- strategies of environmental intervention for physical
nizational and work environmental factors (10). This model, activity and diet
which is based on a systems perspective, argues that work- Promotional activities
place health promotion efforts must address 1) organiza-
Use pamphlets, fliers, posters and signage to “saturate”
tional factors (e.g., socio-cultural, economic), 2) the work
the workplace with messages on physical activity
environment (e.g., physical and structural), and 3) job de-
mands and worker characteristics. Thus, the intervention and healthful eating
targets job demands and worker characteristics, physical Physical activity
work environment, and the socio-organizational environ- Mark walking paths inside and outside buildings and
ment. For example, in some worksites, specific job require- promote their usage
ments or conditions limit or facilitate opportunities for Create more inviting stairwells in buildings with
physical movement. Thus, weight management strategies staircases
address these job demands in such worksites. Another study Facilitate the development of exercise/fitness groups
uses a framework that posits that the obesity epidemic can Offer a pedometer challenge program
best be controlled by targeting the epidemiological triad: Provide fitness equipment at workstations and
hosts, vectors of agents, and environments (11). The study encourage their usage
targets the employee (or host), energy intake and output (or
Facilitate assess to and encourage use of exercise
vectors of the agent, positive energy balance, for example,
equipment and bike racks
energy dense foods, large portion sizes and physical inac-
tivity), and the obesogenic environment (11). Provide discounts to local fitness facilities
Formative research (Phase I) is being used to refine, Provide equipment (e.g., LifeClinic Health Station) for
modify, enhance, or develop the intervention strategies. The measuring body weight and other indicators of health
studies are using combinations of intervention strategies Dietary
that have been shown to be successful in the literature (e.g., Label healthful food choices in vending machines and
vending machines) or were pilot-tested in Phase I. Further, cafeteria
the studies employ employee advisory boards whose mem- Provide preferential pricing for healthful foods
bers suggest additional interventions or modifications to Provide “healthy cupboard” space and snack stations
planned interventions and serve as program champions/ for healthful eating choices
advisors to help implement the intervention. Also, process Coordinate a local Farmers’ Market on site
evaluation data (e.g., number of people who used pedome-
Provide scales to weigh foods and control portion sizes
ters, weighed themselves daily, take the stairs, or read
Require healthful food choices at company-sponsored
study-specific newsletters) are collected and are being used
to improve the intervention (12). Table 2 presents examples meetings, events, and training programs
of environmental strategies addressing diet and physical Encourage consumption of water by placing filtration
activity, and promotional activities used by the studies. The systems near vending machines
environmental intervention strategies include portion size Promote area restaurants that offer healthful food
reduction and recipe modifications of cafeteria foods, pref- choices
erential pricing for healthful foods in vending machines,
and provision of fitness equipment. Individual-level inter-
ventions are also included, for example, group or individual
activity, fast foods and fruit and vegetable consumption
weight loss management programs for highly motivated
questionnaire, the Work Limitations Questionnaire, short
employees with BMI ⬎30 (Work, Weight and Wellness
form, to measure worker productivity, and a healthcare use
Program, Kaiser Permanente, Hawaii) or group-level edu-
and absenteeism survey. The primary outcome measure for
cational programs are being offered to all employees (Step
all studies is change in BMI or body weight. Secondary
Ahead Program, Massachusetts; and the Lighten-Up Pro-
measures include waist circumference, individual dietary
gram, Cornell). All interventions are about two years in
intake, objective measures of physical activity (e.g., accel-
duration (Table 1).
erometry), self-reported measures of physical activity (e.g.,
questionnaires assessing free-time physical activity), work
Measurements productivity, healthcare use, and cost benefit (e.g., return on
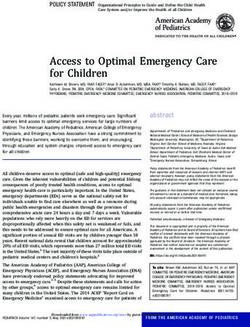
Table 3 presents a list of tools and instruments that are investment and programmatic and medical costs). Study-
being used by the studies. These include weight scales for specific measures include blood pressure, depressive symp-
body weight/BMI, the Godin survey for assessing physical toms, social support, tobacco and alcohol use, and self-
OBESITY Vol. 15 No. 9 September 2007 2175Table 3. List of measures by worksite program
2176
PACE
Work, Fred Hutchinson
Weight and Step Ahead, Route H, Images of a Cancer Research
Lighten Up, Wellness, University of ACTION!, University of Healthy Worksite, Center and the
Cornell Kaiser Massachusetts Tulane Minnesota— University of University of
Measure University Permanente Medical School University Twin Cities Rochester Washington
Weight outcomes
Weight (kg)* X X X X X X X
BMI (kg/m2)* X X X X X X X
Waist circumference (cm) X X X X X
Dietary outcomes
24-hour dietary recall X X X X
OBESITY Vol. 15 No. 9 September 2007
Worksite Environmental Interventions, Pratt et al.
Specific food choices
(e.g., fast foods and
fruits and vegetables)* X X X X X X X
Environmental measures
of diet availability
(e.g., low-fat cafeteria
and vending machine
foods)* X X X X X X X
Physical activity outcomes
Environmental measures
of physical activity
resources (e.g.,
facilities for physical
activity)* X X X X X X X
Physical activity, using
accelerometer X X X X
Selected questions from
the International
Physical Activity
Questionnaire (24) X X X X X
Modified Godin Survey:
Leisure-time Physical
Activity (21)* X X X X X X XTable 3. Continued
PACE
Work, Fred Hutchinson
Weight and Step Ahead, Route H, Images of a Cancer Research
Lighten Up, Wellness, University of ACTION!, University of Healthy Worksite, Center and the
Cornell Kaiser Massachusetts Tulane Minnesota— University of University of
Measure University Permanente Medical School University Twin Cities Rochester Washington
Worksite Environmental Interventions, Pratt et al.
Work productivity, health
utilization, and
economic outcomes
Work productivity (e.g.,
number of days absent
from work, attendance)
(25)* X X X X X X X
Healthcare utilization
(e.g., number of
doctor’s visits,
emergency room
admissions) (26)* X X X X X X X
Economic outcomes (e.g.,
return on investments,
program and medical
costs, cost benefits)
(27)* X X X X X X X
X denotes those tools used by a site. “Other measures” (without asterisks) are those that are used by three or more sites.
* Same instruments used by all sites.
OBESITY Vol. 15 No. 9 September 2007
2177Worksite Environmental Interventions, Pratt et al. report measures of sleep. Lack of sleep has been positively Other study-specific assessments (two studies) include correlated with obesity and could mediate intervention ef- the effects of sleep duration on body weight. The Sleep fects on body weight (13,14). Symptoms Questionnaire has good internal consistency re- Dietary intake is being assessed by 24-hour recalls (2 liabilities, with Cronbach’s ␣ coefficients ranging from 0.91 weekdays and 1 weekend) conducted by three studies. Com- to 0.98 (13). mon questionnaires are being used to assess patterns of In addition to the outcome measures, each study uses intake of specific foods such as fast foods, soft drinks, and process measures to examine intervention dose, fidelity, and fruits and vegetables. Such foods correlate significantly reach (12). Examples include number of promotional activ- with body weight or healthful eating (15–19). Environmen- ities (dose), intervention staff’s delivery of intervention tal measures of diet and physical activity are assessed using according to established protocol (fidelity), and participa- a modified version of the Checklist of Health Promotion at tion in worksite food and physical activity contests (e.g., Worksites (20), which has been found to have reliability percent attending compared with that expected) (reach). coefficients ranging from 0.8 to 1.0. Although the investigators focus on different populations, Physical activities of participants are assessed by the use diverse intervention strategies, and address their own Godin leisure-time physical activity questionnaire, which specific research questions, the studies have similar primary typically has moderate-to-high reliabilities for assessing and secondary outcome measures (Table 3) and similar light, moderate, and strenuous physical activity. The Godin designs, which encourage common statistical analytical ap- questionnaire has Cronbach’s ␣ ranging between 0.62 and proaches. Selected data from two or more studies would be 0.74 (21). For all of the studies, the Godin questionnaire was pooled for secondary analyses to obtain greater statistical modified for clarity by listing the intensity of physical power or to examine age, gender, or racial differences. This activity for days per week, and minutes of activity in 10- to collaborative process has the potential to enhance compa- 15-minute increments, from 0 minutes to 60 minutes. Four rability of results and create a synergy of creative expertise studies use accelerometers to provide objective measures of of investigators to address the obesity problem through physical activity. Physical activity thresholds and imputa- worksite environmental intervention strategies. Despite tion methods are defined by the methods proposed by these benefits, there are challenges in this procedure. For Treuth et al. (22) and Catellier et al. (23). example, all sites must adhere to similar procedures in data Questions from the International Physical Activity Ques- collection and must develop common analytical plans to tionnaire (24) that focus on job-related physical activity are establish comparability and generalization of the results. being used by five of the studies. The International Physical However, successful results from two or more worksites Activity Questionnaire has been tested in 12 countries and have the potential to be translated to other businesses. found to have acceptable measurement properties for use in many settings, including worksites. It has a moderate-to- Study Collaboration and Monitoring high test-retest reliability coefficient of ⬃0.8. The Center for Health Research of Kaiser Permanente, All of the studies use the Work Limitations Questionnaire Northwest, serves as the coordinating center for the seven to assess work productivity (25). The short, 8-item version projects. It facilitates communication, cooperation and sci- of the Work Limitations Questionnaire is used to measure entific collaboration among the seven projects. To accom- the degree to which health problems interfere with ability to plish study objectives, the NHLBI established a steering perform job roles. It assesses employees’ perceived health committee for the overall research program to facilitate problems, such as physical, mental, and interpersonal de- communication among the scientists and staffs. The overall mands, and how these problems interfere with specific leadership of the research program is the responsibility of aspects of job performance (on-the-job disability) (25). the steering committee consisting of the principal investi- Cronbach’s ␣ statistics are typically between 0.7 and 0.9. gators of each study and the NHLBI Project Scientist. The Employees who have been randomly selected to be mea- coordinating center maintains a program Web site, which sured complete the healthcare use questionnaire, which as- allows secure access to study protocols, procedures for data sesses sick days and doctor’s visits and has been examined collection, assessment tools, and secure transfer and sharing for face validity (26). The studies assess cost benefit by of data among investigators to facilitate across-site data calculating the return on investment, which can be defined analyses. either as net present value (i.e., the ratio of inflation-ad- In summary, the worksite intervention studies program is justed discounted savings to program expenses), or as the a unique collaborative program among seven studies with benefit-to-cost ratio (27,28). All sites collect data on health- the common aim of testing the effectiveness of worksite care use, absenteeism, and presenteeism to estimate pro- environmental strategies to control overweight and obesity gram savings. Data are monetized and savings are compared in adults. with program expenses to calculate return on investment The findings from the studies could be useful to research- (27). ers and employers because they could provide guidance for 2178 OBESITY Vol. 15 No. 9 September 2007
Worksite Environmental Interventions, Pratt et al.
designing, implementing, and evaluating worksite obesity 7. Hennrikus D, Jeffery RW. Worksite interventions for weight
interventions, and for making such interventions an integral control: randomized control trials published in 1968 –1994.
part of employee health promotion. Interventions found to Am J Health Promot. 1996;10:471–98.
be cost-effective and implemented in the worksite setting 8. Katz DL, O’Connell M, Yeh MC, et al. Public health strat-
egies for preventing and controlling overweight and obesity in
have the potential to improve health and reduce medical
school and worksite settings. MMWR Recomm Rep. 2005;
care costs for employers, and could motivate others to
54(RR-10):1–12.
implement such programs within their worksites. Data 9. McLeroy KR, Bibeau D, Steckler A, Glanz K. An ecolog-
pooled from these studies could enhance the translation to, ical perspective on health promotion programs. Health Educ
and data sharing with, other worksites. Findings from this Q. 1988;15:351–77.
program of studies have the potential to guide other work- 10. Dejoy DM, Southern DJ. An integrative perspective on
site obesity interventions and influence worksite policies for worksite health promotion. J Occup Med. 1993;35:1221–30.
overweight and obesity control. The studies could also 11. Egger G, Swinburn B, Rossner S. Dusting off the epidemi-
provide qualitative data on how to secure management ological triad: could it work for obesity? Obes Rev. 2003;4:
support and organizational commitment to conduct scien- 115–9.
tific research in business settings, and methods to encourage 12. Baranowski T, Stables G. Process evaluations in 5-a day
projects. Health Educ Behav. 2003;27:157– 66.
participation of employees.
13. Kump K, Whalen C, Tishler PV, et al. Assessment of the
The emphasis on environmental strategies (or a combi-
validity and utility of a sleep-symptom questionnaire. Am J
nation of environmental and individual strategies) and the Respir Crit Care Med. 1994;150:735– 41.
focus on large-scale changes in dietary and physical activity 14. De la Eva RC, Baur LA, Donaghue KC, Waters KA.
behaviors are promising approaches to improve dietary and Metabolic correlates with obstructive sleep apnea in obese
physical activity behaviors, thereby curtailing the obesity subjects. J Pediatr. 2002;140:654 –9.
epidemic (29,30). 15. Liebman M, Pelican S, Moore SA, et al. Dietary intake,
eating behavior and physical activity-related determinants of
high body mass index in rural communities in Wyoming,
Acknowledgments Montana and Idaho. Int J Obes. 2003;27:684 –92.
The authors thank Ronald J. Ozminkowski, (Health and 16. Forslund HB, Lindroos AK, Sjöström L, Lissner L. Meal
patterns and obesity in Swedish women: a simple instrument
Productivity Research, Thomson Medstat); Peter Kaufmann,
describing usual meal types, frequency and temporal distribu-
Eva Obarzanek, and Denise Simons-Morton (NHLBI) for re-
tion. Eur J Clin Nutr. 2002;56:740 –7.
viewing the manuscript; and Judy L. Donald (Kaiser Perma- 17. French SA, Harnack L, Jeffery RW. Fast food restaurant
nente, Northwest) for coordinating the study. This study was use among women in the Pound of Prevention study: dietary,
supported by NHLBI Grants R01 HL79478, R01 HL79483, behavioral and demographic correlates. Int J Obes. 2000;24:
R01 HL79491, R01 HL79505, R01 HL79509, R01 HL79511, 1353–9.
and R01 HL79546. 18. Perreira MA, Kartashov AI, Ebbeling CB, et al. Fast-food
habits, weight gain, and insulin resistance (the CARDIA
study): 15-year prospective analysis. Lancet. 2005;365:36 –
References 42.
1. Ogden CL, Carroll MD, Curtin LR, McDowell MA, Tabak 19. Shannon J, Kristal AR, Curry SJ, Beresford SA. Applica-
CJ, Flegal KM. Prevalence of overweight and obesity in the tion of a behavioral approach to measuring dietary change: the
United States, 1999 –2004. JAMA. 2006;295:1549 –55. Fat- and Fiber-related Diet Behavior Questionnaire. Cancer
2. Hill JO, Peters JC. Environmental contributions to the obe- Epidemiol Biol Prev. 1997;6:355– 61.
sity epidemic. Science. 1998;280:1371– 4. 20. Oldenburg B, Sallis JF, Harris D, Owen N. Checklist of
3. Engber LH, van Poppel MN, Chin A, Paw MJ, van Health Promotion Environments at Worksites (CHEW): de-
Mechelen W. Worksite health promotion programs with en- velopment and measurement characteristics. Am J Health Pro-
vironmental changes: a systematic review. Am J Prev Med. mot. 2002;16:288 –99.
2005;29:61–70. 21. Godin G, Shepard RJ. A simple method to assess exercise
4. Glanz K, Mullis RM. Environmental interventions to pro- behavior in the community. Can J Appl Sport Sci. 1985;10:
mote healthy eating: a review of models, programs and evi- 141– 6.
dence. Health Educ Q. 1988;15:395– 415. 22. Treuth MS, Schmitz K, Catellier DJ, et al. Defining accel-
5. United States Department of Health and Human Services. erometer thresholds for activity intensities in adolescent girls.
Healthy People 2010: Understanding and Improving Health. Med Sci Sports Exerc. 2004;36:1259 – 66.
2nd ed. Washington, DC: U.S. Government Printing Office; 23. Catellier DJ, Hannan PJ, Murray DM, et al. Imputation of
2000. missing data when measuring physical activity by accelerom-
6. United States Department of Health and Human Services. etry. Med Sci Sports Exerc. 2005;37(suppl):555– 62.
Surgeon General’s Call to Action to Prevent and Decrease 24. Craig CL, Marshall AL, Sjöström M, et al. International
Overweight and Obesity. Washington, DC: U.S. Public Health Physical Activity Questionnaire (IPAQ): 12-country reliabil-
Service, Office of the Surgeon General; 2001. ity and validity. Med Sci Sports Exerc. 2003;35:1381–95.
OBESITY Vol. 15 No. 9 September 2007 2179Worksite Environmental Interventions, Pratt et al.
25. Lerner DJ, Amick BC III, Rogers WH, Malspeis S, Bun- 28. Gold MR, Siegel JE, Russell LB, Weinstein MC. Cost-
gay K, Cynn D. The Work Limitations Questionnaire. Med Effectiveness in Health and Medicine. New York, NY: Oxford
Care. 2001;39:72– 85. University Press, 1996.
26. Ozminkowski RJ, Goetzel RZ, Chang S, Long SR. 29. Institute of Medicine. Health and Behavior: The Interplay of
The application of two health and productivity instruments Biological, Behavioral and Societal Influences. Washington,
at a large employer. J Occup Environ Med. 2004;46:635– DC: National Academy Press; 2001.
48. 30. United States Department of Health and Human Services.
27. Goetzel RZ, Ozminkowski RJ, Baase CM, Billotti GM. Think tank on enhancing obesity research at the National
Estimating the return on investment from changes in employee Heart, Lung, and Blood Institute [NIH Publication No. 04-
health risks on the Dow chemical company’s health care costs. 5249]. Washington, DC: U.S. Department of Health and Hu-
J Occup Environ Med. 2005;47:759 – 68. man Services; 2004.
2180 OBESITY Vol. 15 No. 9 September 2007You can also read