Demonstration of Tolerability of a Novel Delivery Approach and Secreted Protein Expression Following Intracochlear Delivery of AK-antiVEGF ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Demonstration of Tolerability of a Novel Delivery Approach and
Secreted Protein Expression Following Intracochlear Delivery of
AK-antiVEGF (AAVAnc80-antiVEGF Vector) in Non-Human Primates
John Connelly1, Ivy K. Hughes1, Ann E. Hickox1, Shimon P. Francis1, Christopher A. Shera2, Alec Salt2,
Eric Horowitz1, Kathleen Lennon1, Jean Phillips1, Jenna Soper1, Michelle D. Valero1, Jennifer A. Wellman1,
Gregory S. Robinson1, Emmanuel J. Simons1, William F. Sewell3, Michael J. McKenna1, Eva Andres-Mateos1
1Akouos, Inc., Boston, MA, 2Consultant to Akouos, Inc., 3Co-founder and consultant to Akouos, Inc.
Bellucci Symposia | June 3-4, 2021
1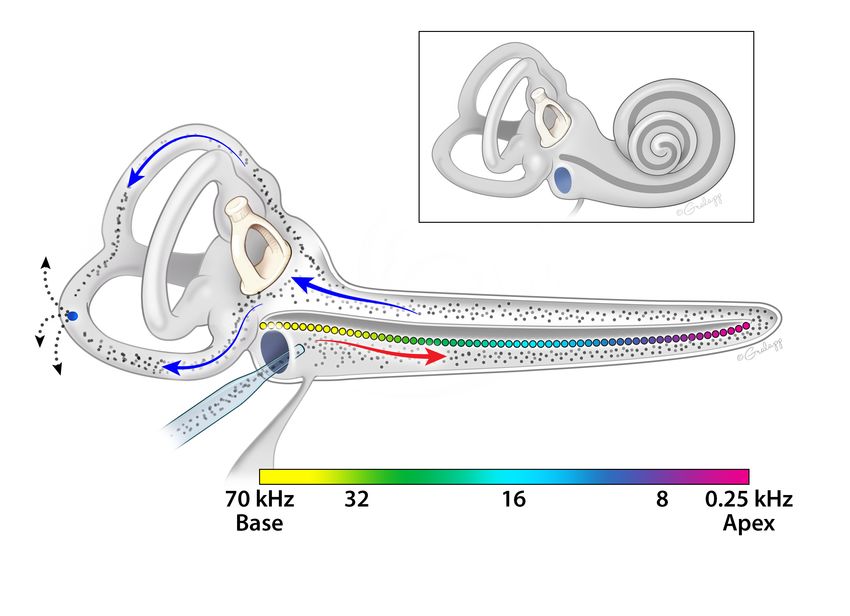
Disclosures
John Connelly is an employee of Akouos, Inc., and has received, and is
receiving, compensation and equity from Akouos, Inc.
2
Forward Looking Statements
This presentation includes “forward-looking statements” within the meaning of the Private Securities Litigation Reform Act of 1995,
including, but not limited to: the ability of our product candidate AK-antiVEGF to potentially treat vestibular schwannoma; statements
relating to the initiation, plans, and timing of our future clinical trials and our research and development programs; and the timing of our
planned IND submission for AK-antiVEGF. These forward-looking statements may be accompanied by such words as “aim,”
“anticipate,” “believe,” “continue,” “could,” “estimate,” “expect,” “forecast,” “goal,” “intend,” “may,” “might,” “plan,” “potential,” “possible,”
“target,” “will,” “would,” and other words and terms of similar meaning. Akouos may not actually achieve the plans, intentions, or
expectations disclosed in these forward-looking statements, and you should not place undue reliance on these forward-looking
statements. Actual results or events could differ materially from the plans, intentions, and expectations disclosed in these forward-looking
statements as a result of various factors, including: our limited operating history; uncertainties inherent in the development of product
candidates, including the initiation and completion of nonclinical studies and clinical trials; the timing of and our ability to submit and
obtain regulatory approval; whether results from nonclinical studies will be predictive of results or success of clinical trials; our ability to
obtain sufficient cash resources to fund our foreseeable and unforeseeable operating expenses and capital expenditure requirements; our
ability to obtain, maintain, and enforce our intellectual property; the impact of the COVID-19 pandemic on our business, results of
operations, and financial condition; the potential that our internal manufacturing capabilities and/or external manufacturing supply may
experience delays; risks related to competitive programs; and the other risks and uncertainties that are described in the Risk Factors
section of the Company's Quarterly Report on Form 10-Q for the quarter ended March 31, 2021, which is on file with the Securities and
Exchange Commission, and in other filings that Akouos may make with the U.S. Securities and Exchange Commission. These statements are
based on our current beliefs and expectations as of the date of this presentation. We do not undertake any obligation to publicly
update any forward-looking statements except as required by law. By attending or receiving this presentation, you acknowledge that: you
are cautioned not to place undue reliance on these forward-looking statements; you will be solely responsible for your own assessment of
the market and our market position; and you will conduct your own analysis and be solely responsible for forming your own view of the
potential future performance of Akouos, Inc.
3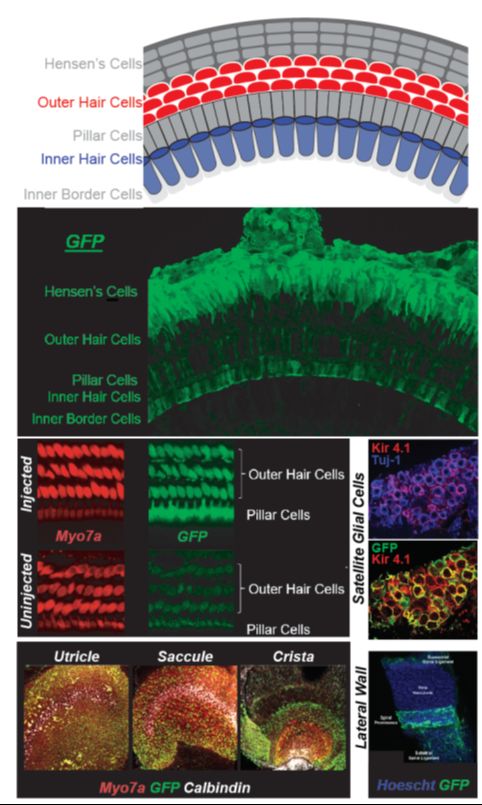
Vestibular Schwannoma
• Vestibular schwannomas (VS) are tumors resulting from neoplasia of
the Schwann cells that ensheathe the vestibulocochlear nerve and is
estimated to affect approximately 200,000 individuals in the United
States and Europe
Site of VS
• VS may result in a variety of symptoms including hearing loss,
tinnitus, headaches, and impaired balance; left untreated, VS can cause
serious neurological problems, including facial paralysis, blindness, and
brain damage severe enough to cause death
• Current standard of care:
• Small or non-growing tumors may be followed by observation only
• Surgical resection and/or radiation therapy are indicated for larger and/or
progressive tumors
• Surgical resection and radiation carry the risk of significant morbidity,
including facial paralysis and hearing loss
• Systemic administration of VEGF inhibitors has shown promising results
in a genetic form of VS (Neurofibromatosis Type 2 [NF2]) in clinical
trials (Plotkin 2009 N Engl J Med; Plotkin 2012 Otol Neurotol; Lu 2019 J Neurooncol) The most common area for VS occurrence is along the vestibulocochlear nerve as it courses through
the internal auditory canal (IAC) to the brainstem. The majority of small, intracanalicular tumors (less
• Vascular endothelial growth factor (VEGF) is upregulated in vestibular than 5 mm width) arise within the lateral third of the IAC, nearest to the cochlea (Koen 2020
Otolaryngol Head Neck Surg).
schwannomas, including non-NF2 (sporadic) tumors (Koutsimpelas 2012 ORL Image modified from: https://commons.wikimedia.org/wiki/File:Anatomy_of_the_Human_Ear.svg
J Otorhinolaryngol Relat Spec)
4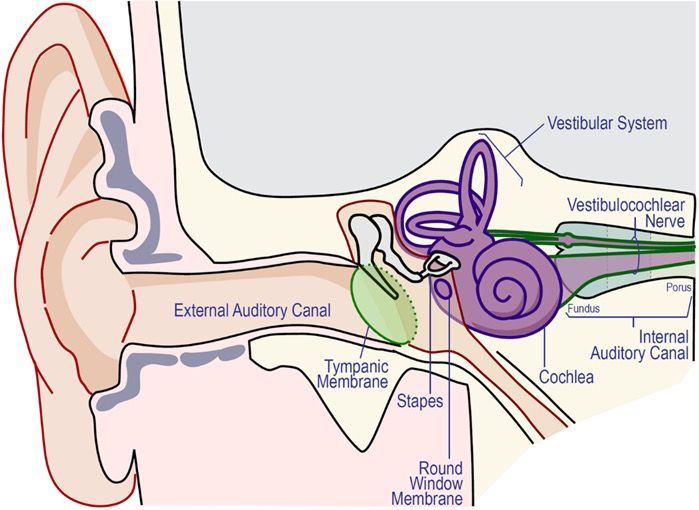
Rationale for AK-antiVEGF (AAVAnc80-antiVEGF) for the Potential
Treatment of Vestibular Schwannoma
• Current standard of care (surgical resection and/or radiation) can have
significant morbidity (e.g., facial paralysis and hearing loss)
• Vascular endothelial growth factor (VEGF) is upregulated in vestibular
schwannomas, including non-NF2 (sporadic) tumors (Koutsimpelas 2012 ORL J
Otorhinolaryngol Relat Spec)
• In clinical trial settings, repeated systemic administration of Avastin®
(bevacizumab, a VEGF inhibitor) has been shown to decrease VS tumor size
and improve hearing in NF2 patients (Plotkin 2009 N Engl J Med; Plotkin 2012 Otol
Neurotol; Lu 2019 J Neurooncol)
• However, long-term systemic use of Avastin® is associated with toxicity
• Alternatively, a local low level of anti-VEGF protein could be efficacious,
potentially reducing need for surgical resection and/or radiation
5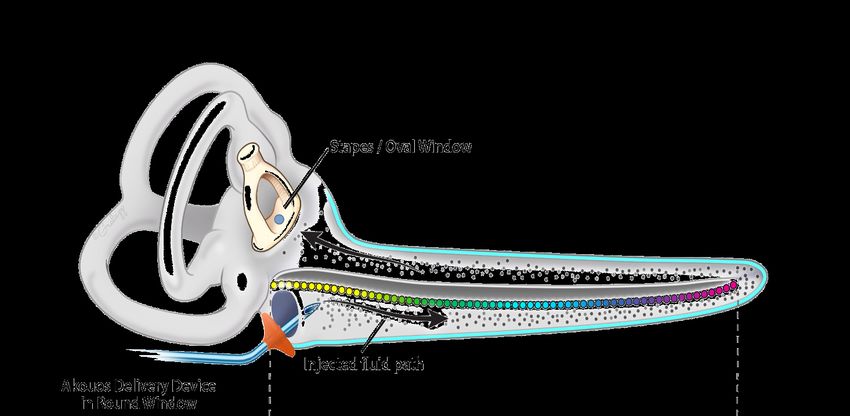
Systemic Administration of VEGF Inhibitor Shows Promise in NF2-related
Vestibular Schwannoma, but Toxicity Limits its Potential as a Viable
Treatment Option
Clinical Trial Data Demonstrate Ability of Systemic VEGF Inhibitor
Meta-analysis: Clinical Trials of Efficacy and Safety
to Improve Hearing and Reduce Tumor Volume
of Bevacizumab in NF2 Patients
in Some Patients
n e w e ng l a nd j o u r na l
The
with Vestibular Schwannoma
m e dic i n e of
The n e w e ng l a nd j o u r na l of m e dic i n e
T he new engl and jour nal o f medicine
original article
original article
original article
Hearing Improvement after Bevacizumab
Hearing Improvement after Bevacizumab
in Patients with Neurofibromatosis Type 2
in Patients with Neurofibromatosis Type 2
Hearing
Fred
ScottG.R.BarkerImprovement
II, M.D., Chris
Plotkin, Ph.D.,Halpin, afterTimothy
Anat O.Ph.D., Bevacizumab
Scott R. Plotkin, M.D., Ph.D., Anat O. Stemmer-Rachamimov, M.D.,
P. Padera,M.D.,
Stemmer-Rachamimov, Ph.D.,
AlexG.
Tyrrell, Ph.D., A. Gregory Sorensen, M.D., Rakesh
P. K. Jain, Ph.D.,
in Alex
Patients with Neurofibromatosis Rakesh K. Jain,Type
Ph.D., 2
Fred Barker II, M.D., Chris Halpin, Ph.D., Timothy Padera, Ph.D.,
Tyrrell, Ph.D.,and
A. Emmanuelle
Gregory di Tomaso,
Sorensen, M.D.,Ph.D.
and Emmanuelle di Tomaso, Ph.D.
Scott R. Plotkin, M.D., Ph.D.,A bs
Anat
trO.
acStemmer-Rachamimov,
t M.D.,
Fred G. Barker II, M.D., ChrisAHalpin,
bs tr ac t Timothy P. Padera, Ph.D.,
Ph.D.,
Alex Tyrrell, Ph.D., A. Gregory Sorensen, M.D., Rakesh K. Jain, Ph.D.,
Background
om the Departments of Neurology Profound hearing loss isand
Background a serious complication
Emmanuelle of neurofibromatosis
di Tomaso, Ph.D. type 2, a ge-
R.P.), Pathology (A.O.S.-R.), and Radia- netic condition associated with bilateral vestibular schwannomas, benign tumors
om the Departments of Neurology
n Oncology (T.P.P., A.T., R.K.J., E.T.); the
Profound hearing loss is a serious complication of neurofibromatosis type 2, a ge-
R.P.), Pathology (A.O.S.-R.), and Radia-
ncer Center (S.R.P.); the Neurosurgical that arise
netic from associated
condition the eighth with
cranial nerve.vestibular
bilateral There is no medical treatment
schwannomas, benignfor such
tumors
n Oncology (T.P.P., A.T., R.K.J., E.T.); the
rvice (F.G.B.); and the A.A. Martinos
ncer Center (S.R.P.); the Neurosurgical
tumors.
that arise from the eighth cranial nerve. There is no medical treatment for such
nter for Biomedical Imaging (A.G.S.)
rvice (F.G.B.); and the A.A. Martinos
all at Massachusetts General Hospi-
tumors. Abstr act
nter for Biomedical Imaging (A.G.S.)
and the Department of Audiology, Methods
all at Massachusetts General Hospi-
assachusetts Eye and Ear Infirmary
and the Department of Audiology,
We determined the expression pattern of vascular endothelial growth factor (VEGF)
Methods
H.) — all in Boston. Address reprint anddetermined
three of itsthe receptors, VEGFR-2, neuropilin-1, and neuropilin-2, in paraffin-
assachusetts Eye and Ear Infirmary
quests to Dr. Plotkin at Yawkey 9E,
We expression pattern of vascular endothelial growth factor (VEGF)
H.) — all in Boston. Address reprint
ssachusetts General Hospital, 55 Fruit embedded
and three of
Background samples from 21VEGFR-2,
its receptors, vestibularneuropilin-1,
schwannomas andassociated with in
neuropilin-2, neurofibro-
paraffin-
quests to Dr. Plotkin at Yawkey 9E,
, Boston, MA 02114, or at splotkin@ matosis type
embedded samples 2 and from 22 sporadic schwannomas. Ten consecutive
21 vestibular schwannomas associated with neurofibro- patients with
om
ssachusetts General Hospital, 55 Fruit
the Departments
rtners.org.
, Boston, MA 02114, orofat Neurology
splotkin@ Profound hearing
neurofibromatosis
matosis type 2 andloss
type
fromis2a22and
serious complication
progressive
sporadic of neurofibromatosis
vestibular
schwannomas. schwannomas
Ten consecutivewhotypewere
2, awith
patients ge-
not
R.P.), Pathology (A.O.S.-R.), and Radia-
rtners.org.
s article (10.1056/NEJMoa0902579) was netic condition
candidates
neurofibromatosis associated
for standard withprogressive
type 2treatment
and bilateral vestibular
were treated with
vestibular schwannomas,
bevacizumab,benign
schwannomas tumors
an anti-VEGF
who were not
n Oncology
blished (T.P.P.,
on July A.T.,atR.K.J.,
8, 2009, E.T.); the
NEJM.org. monoclonalfor
candidates antibody.
standard Antreatment
imaging response was with
were treated defined as a decrease
bevacizumab, of at least
an anti-VEGF
s article (10.1056/NEJMoa0902579) was
ncer Center
blished (S.R.P.);
on July theatNeurosurgical
8, 2009, NEJM.org.
that
20% arise
monoclonal
from
in tumor the eighth
volume,
antibody.
cranial nerve.
as compared
An
There
with baseline.
imaging response
is Anohearing
was defined
medical treatment
as response
a decreasewas
forat such
of defined
least
(F.G.B.); and the A.A. Martinos tumors.
Engl J Med 2009;361:358-67.
rvice
yright © 2009 Massachusetts Medical Society. as a significant
20% increaseasincompared
in tumor volume, the word-recognition score,
with baseline. as compared
A hearing withwas
response baseline.
defined
Engl J Med 2009;361:358-67.
nter for Biomedical Imaging (A.G.S.) as a significant increase in the word-recognition score, as compared with baseline.
yright © 2009 Massachusetts Medical Society.
all at Massachusetts General Hospi- Results
and the Department of Audiology, Methods VEGF was expressed in 100% of vestibular schwannomas and VEGFR-2 in 32% of
Results
assachusetts Eye and Ear Infirmary tumor We
VEGFdetermined
vessels
was onthe expression
in 100% pattern
immunohistochemical
expressed of analysis.
vascular
of vestibular endothelial growth
Before treatment,
schwannomas and factor
the
VEGFR-2 in (VEGF)
median
32%an- of
H.) — all in Boston. Address reprint nual tumor
and volumetric
vessels
three of ongrowth
its rate for 10 index analysis.
immunohistochemical
receptors, VEGFR-2, tumors was
neuropilin-1, 62%.treatment,
Before
and After bevacizumab
thein
neuropilin-2, median treat-
paraffin-an-
quests to Dr. Plotkin at Yawkey 9E, ment
nual in the 10
volumetric patients,
growth tumors
rate for shrank
10 indexin 9 patients,
tumors was and
62%. 6 patients
After had an
bevacizumab imaging
treat-
ssachusetts General Hospital, 55 Fruit embedded
response,
ment in the samples
which wasfrom
10 patients, 21 vestibular
maintained
tumors shrank schwannomas
in 4 patients
in duringand
9 patients, 11associated
to with
16 months
6 patients hadofneurofibro-
anfollow-up.
imaging
, Boston, MA 02114, or at splotkin@ response, matosis
The type
median which2 and
best from
response
was 22tosporadic
maintained treatmentschwannomas.
was aduring
in 4 patients Ten
11 toconsecutive
volumetric reduction
16 months ofpatients
of26%. with
Three
follow-up.
rtners.org. patients
The medianwerebest
not response
eligible for to atreatment
hearing response; of the remaining
was a volumetric reduction seven
of 26%.patients,
Three
neurofibromatosis
four had were
patients a hearing type 2
response,
not eligible
and
fortwo
progressive
had stable
a hearing
vestibular
hearing,
response;
schwannomas
and remaining
of the
who
one had progressive were not
hear-
seven patients,
6
s article (10.1056/NEJMoa0902579) was candidates
ing loss.
four had aTherefor standard
hearingwereresponse,treatment
21 adverse were
twoevents
had of treated
grade
stable 1 with
or 2.
hearing, andbevacizumab, an anti-VEGF
one had progressive hear-
blished on July 8, 2009, at NEJM.org. ing loss. There
monoclonal were 21An
antibody. adverse
imaging events of grade
response was1 ordefined
2. as a decrease of at least
Conclusions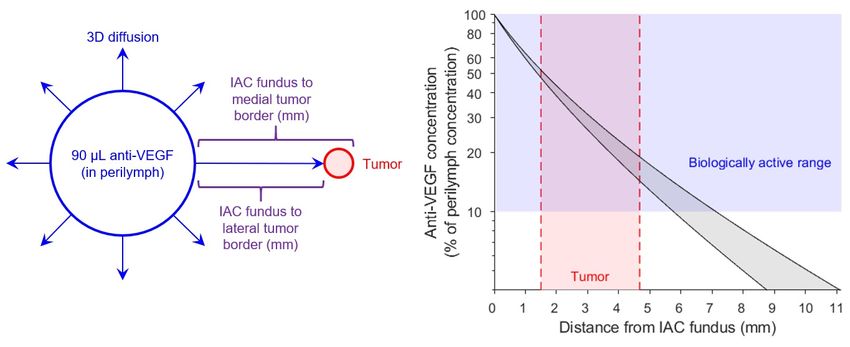
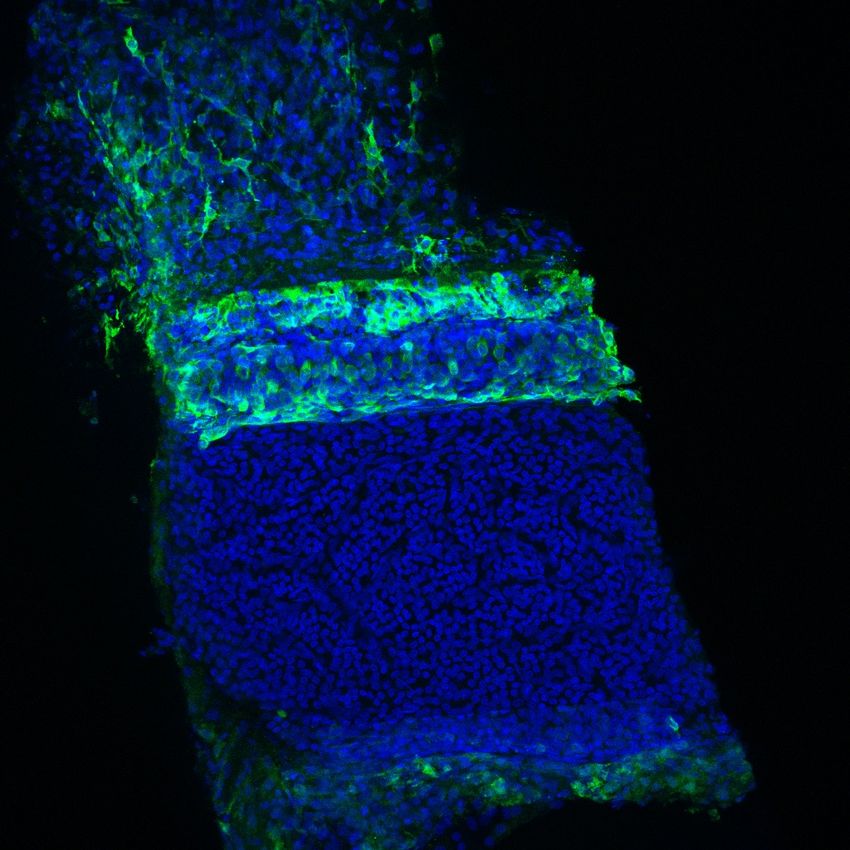
AAVAnc80 Efficiently Transduces Multiple Cell Types in
the Inner Ear
ü Conducted nonclinical studies across three
different species of non-human primates using
GFP as a reporter gene delivered by AAVAnc80
ü AAVAnc80 can efficiently transduce multiple
AAVAnc80-eGFP
target cell populations throughout the cochlea
in the primate inner ear
Negative Control
ü In the planned approach, after administration of
a vector utilizing a ubiquitous promoter, the
cochlear and vestibular cells will produce and
secrete anti-VEGF protein into the perilymph, a
cochlear fluid in diffusional continuity with the
interstitial and perineural spaces of the
vestibulocochlear nerve where vestibular
schwannoma tumors are located GFP: green fluorescent protein; Myo7a: Myosin VII a; Tuj1: class III beta-tubulin
All micrographs are from Study AK-007, with the exception of Satellite Glial Cells
from Study AK-011
7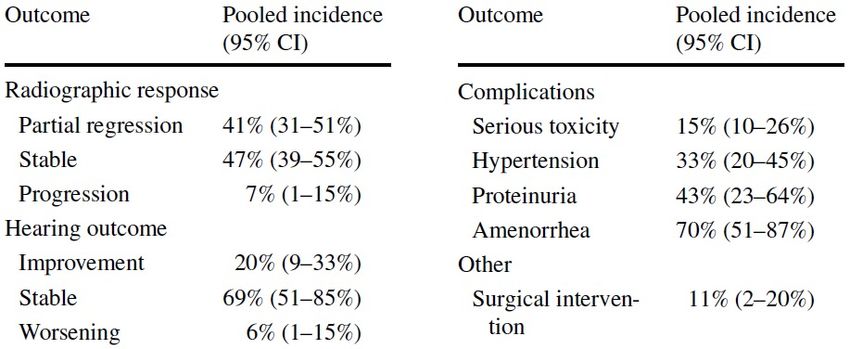
Study AK-033: Preliminary Evaluation of Tolerability and Exposure of
AK-antiVEGF in NHPs as Part of Overall Development Strategy
Attribute Supporting Data
Historical clinical trial data using Avastin® systemically in NF2 patients
Biological Plausibility (Plotkin 2009 N Engl J Med; Plotkin 2012 Otol Neurotol; Lu 2019 J Neurooncol)
Two- and six-month tolerability assessment in NHPs
• Auditory Brainstem Response
Tolerability
• Otic Histopathology
• Cytocochleograms
Study
Measurement of steady-state anti-VEGF levels in perilymph two months post- AK-033
Local Exposure Levels administration
Measurement of anti-VEGF levels in serum (over 6 months) and terminal CSF
Systemic Exposure (two- or six-months post-administration)
Computational modeling calculating theoretical levels of anti-VEGF at typical
Clinical Translatability site of early vestibular schwannoma
(based on perilymph levels from AK-033)
Abbreviations: CSF: cerebrospinal fluid; NF2: neurofibromatosis type II; NHP: non-human primate
Additional work to further characterize tolerability and exposure is currently underway
8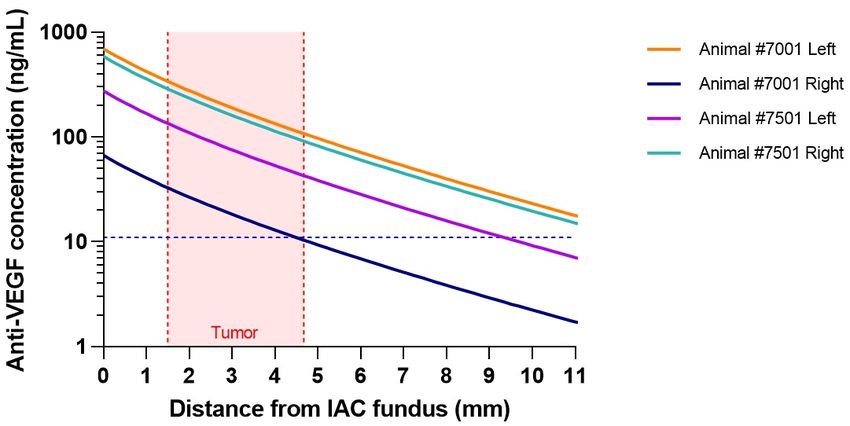
Preliminary Evaluation of Tolerability and Exposure of AK-antiVEGF in
NHPs (Study AK-033) Coiled cochlea
Bilateral auditory function tests (ABR): 1.1, 2.8, 8.0, and 22.6 kHz
Bilateral intracochlear administration of AK-antiVEGF (1X dose or
5X dose) or vehicle control
Uncoiled cochlea
Terminal fluid and unfixed (flash frozen) tissue analysis:
• Perilymph / CSF / serum: measurement of anti-VEGF levels
© Chris Gralapp
• Inner ears and vestibulocochlear nerves (cranial nerve VIII)
• Brain: auditory pathway
• Other major organs
-2 weeks Day 0 1 month 2 months
Bilateral auditory function tests (ABR); and
Groups 6
Terminal fluid and fixed-tissue analyses:
and 7
• Inner ears: otic histopathology (ear 1) or cytocochleogram
analyses (contralateral ear)
Groups 1, 2, • Brain: histopathology, with focus on auditory regions
and 3 • CSF / serum: measurement of anti-VEGF levels
ABR: auditory brainstem response; kHz: kilohertz; CSF: cerebral spinal fluid
3 months 6 months
Groups 4
and 5
9
Physiologic and Histologic Evaluations in NHPs Support Tolerability to
AK-antiVEGF (Study AK-033)
Vehicle 1X Dose 5X Dose
Shifts in ABR thresholds (relative to baseline ABRs acquired in the same ear ~2 weeks prior to intracochlear administration) are shown for 1, 2, 3, and 6 months post-intracochlear administration of
either vehicle or AAVAnc80 vector encoding anti-VEGF at doses of 1X vg/cochlea or 5X vg/cochlea. Group means (±SD) at each timepoint reflect bilateral measurements in each NHP on study.
• Mean ABR thresholds were similar to baseline thresholds across all frequencies following administration of AK-antiVEGF at two doses
• Minimal ABR threshold shifts were likely attributable to the surgical approach used in NHPs, which can affect sound conduction through
the NHP middle ear; evaluations were comparable between animals receiving vehicle and either dose of AK-antiVEGF
• Cytocochleogram analyses revealed no signs of ototoxicity related to the test article
• No histopathology findings attributable to the test article
• Initial NHP data supports preliminary tolerability of localized chronic anti-VEGF protein expression
10
ABR: auditory brainstem response; kHz: kilohertz; n: number; SD: standard deviation; NHP: non-human primate; vg: vector genomesIntracochlear Administration of AK-antiVEGF Resulted in Local
Expression of Anti-VEGF Protein in NHP Perilymph (Study AK-033)
Dose Left ear: Right ear:
Animal Test / Control Article In-life Duration CSF Concentration
Group (vg/cochlea Perilymph antiVEGF Perilymph antiVEGF
ID (bilateral administration) (Months) (ng/mL)
) Concentration (ng/mL) Concentration (ng/mL)
6 6101 Vehicle -- 2 BLOD BLOD BLOD
7001 AK-antiVEGF 5X 2 BLOD 694.9 67.0
7
7501 AK-antiVEGF 5X 2 BLOD 275.9 589.2
4 4001 Vehicle -- 6 BLOD
5001 AK-antiVEGF 5X 6 BLOD Perilymph samples were not collected per protocol;
otic histopathology (ear 1) or cytocochleogram
5 5501 AK-antiVEGF 5X 6 BLOD analyses (contralateral ear) were performed
5502 AK-antiVEGF 5X 6 BLOD
Abbreviations: BLOD = below limit of detection (less than 1.7 ng/mL); CSF = cerebrospinal fluid; mL = milliliters; ng = nanograms; NHP: non-human primate; vg = vector genomes
• Two months following intracochlear administration of AK-antiVEGF at 5X dose, anti-VEGF levels in perilymph ranged from 67.0 to 694.9
ng/mL (mean: 406.8 ng/mL)
• No anti-VEGF protein was detected in the perilymph of the vehicle-injected control NHP
• No anti-VEGF protein was detected in CSF, regardless of post-administration duration (2 or 6 months)
• Perilymph samples were tested using the meso scale discovery (MSD) assay; limit of detection (LOD) was 1.7 ng/mL and limit of
quantification (LOQ) was 2.5 ng/mL
11Computational Modeling Supports Biologically Active Levels of
Anti-VEGF at the Tumor Site
1
IAC – internal auditory canal
Image modified from:
https://commons.wikimedia.org/wiki/File:Anatomy_of_the_Human_Ear.svg
1. Range of location of early VS from MRI data (Koen 2020 Otolaryngol Head Neck Surg)
• Anti-VEGF secreted into the perilymph, or into the nerve interstitium, can reach the vestibular schwannoma (VS) passively through simple diffusion, owing
to lack of diffusion barriers from perilymph to the internal auditory canal (IAC)
• Computational diffusional model estimates percent change in a (constant) concentration of anti-VEGF in perilymph as a function of distance to VS, using:
1. Typical location of early VS from MRI data (Koen 2020 Otolaryngol Head Neck Surg)
2. A range of published diffusion coefficients for a representative anti-VEGF molecule
3. Estimated steady-state clearance parameter based on a representative anti-VEGF molecule half-life in vitreous following intraocular injection
4. Conservative assumption of equal 360° diffusion in perilymph (i.e., assumes no anatomical constraints)
• Estimates of anti-VEGF concentration in the immediate vicinity of the VS in the internal auditory canal are well within the reported biologically active range
12Levels of Anti-VEGF are Modelled to Be Above Biologically
Active Threshold Concentration Across Range of Reported VS
Locations
• Anti-VEGF levels in perilymph were measured in NHPs two months following intracochlear administration of AK-antiVEGF
• Computational modeling was used to assess approximate anti-VEGF levels at reported VS locations
• Using empirically determined anti-VEGF levels in the perilymph of NHP and conservative modeling assumptions, estimated
anti-VEGF levels exceeded the biologically active threshold concentration within the reported range of early VS locations
(Koen 2020 Otolaryngol Head Neck Surg)
Reported biologically active
threshold concentration
1 1. Range of location of early VS from MRI data
(Koen 2020 Otolaryngol Head Neck Surg)
VS = vestibular schwannoma;
NHP: non-human primate 13Anti-VEGF Protein Expression Largely Confined to Inner Ear
(Study AK-033)
• NHPs on study were evaluated for circulating anti-VEGF levels in serum at Baseline, Day 14, Month 1,
and Month 2; animals in the 6-month groups were also evaluated at Month 3 and Month 6
• 36 out of 44 (82%) post-administration serum samples were below the limit of detection (LOD) for anti-
VEGF protein in both the 1X and 5X doses
• Anti-VEGF was detected in serum at biologically relevant levels in only one high-dose animal, and only
at Day 14 and Month 1; the Month 2 serum sample from this animal was below biologically relevant
levels
• Anti-VEGF was not detected in any CSF samples
• Anti-VEGF was not detected in any non-cochlear tissues evaluated, including liver, spleen, brainstem,
auditory cortex, or mandibular lymph nodes
• Serum, CSF, and tissue samples were tested using the meso scale discovery (MSD) assay; LOD was 1.7
ng/mL and limit of quantification (LOQ) was 2.5 ng/mL
CSF: cerebrospinal fluid
14Conclusions
• There remains a high unmet need for alternative treatments for patients with vestibular schwannoma (VS)
• Previous published clinical trial data (Plotkin 2009 N Engl J Med; Plotkin 2012 Otol Neurotol; Lu 2019 J
Neurooncol) support the potential for VEGF inhibitors to be efficacious in treating VS when delivered
systemically
• However, associated toxicity limits the chronic systemic administration of VEGF inhibitors as a viable treatment option for VS
• Long-term, local expression of anti-VEGF protein following intracochlear administration of AK-antiVEGF is
robust and well tolerated in NHPs, an anatomically relevant model for evaluating delivery parameters
• Computational modelling supports the potential for diffusion of biologically active anti-VEGF protein levels
to site of tumor
• Together, these data support the future clinical development of AK-antiVEGF for the treatment of VS
• IND filing for AK-antiVEGF is expected in 2022
1516
You can also read

















































