Daptomycin plus Fosfomycin versus Daptomycin alone
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Klinik für Infektiologie & Spitalhygiene
Daptomycin plus Fosfomycin versus Daptomycin alone
for methicillin-resistant Staphylococcus aureus
bacteremia and endocarditis:
a randomized clinical trial
Miquel Pujol et al. for the MRSA Bacteremia (BACSARM) Trial Investigators
CID 2021;72(9):1517–25
Journal Club 31.05.2021
Andreas Neumayr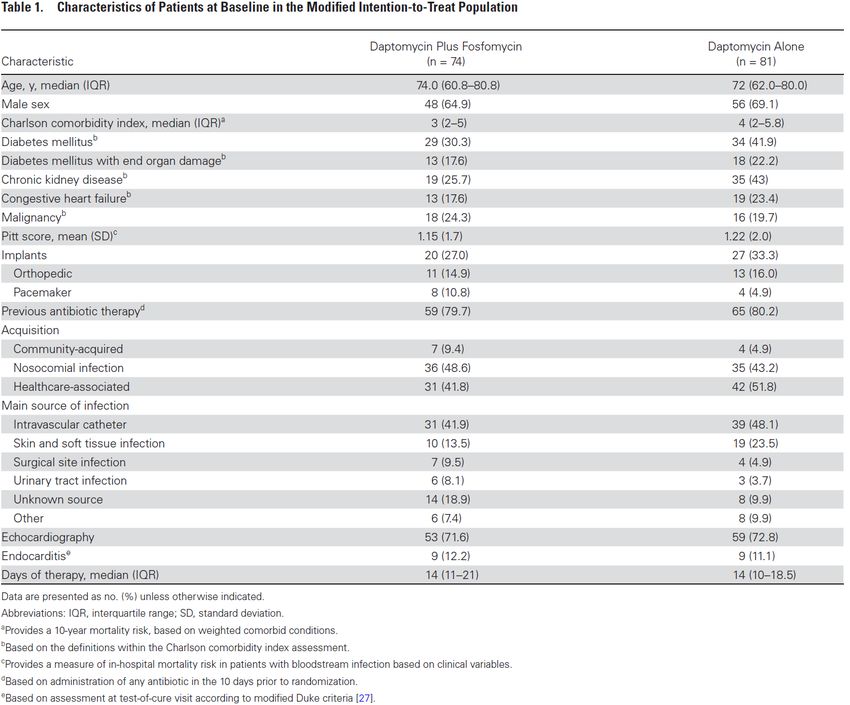
Background:
• Mortality of S. aureus bacteremia is high: 20 – 30%1
• Mortality of MRSA bacteremia is double that of MSSA bacteremia
• Available monotherapies not optimal:
− Vancomycin: slow bactericidal activity, poor tissue penetration,
potential toxicity
− Daptomycin: clin. failure up to 30%2, emergence of resistance
• 2020: CAMERA2: Vanco. or Dapto. monotherapy VS Vanco. or
Dapto. + a β-lactame for MRSA bacteremia3
no mortality benefit of combination therapy
higher rate and more severe AKI with combination therapy
• Daptomycin + fosfomycin is synergistic and rapidly bactericidal
against MRSA in vitro and in the rabbit endocarditis model4
1 Kourtis et al. MMRW 2019;68:214-9. 3 Tong et al. JAMA 2020;doi:10.1001
2 Karchmer. CID 2021;72(9):1526–8. 4 Garcia-de-la-Maria et al. Antimicrob Agents Chemother. 2018;62:e02633-17.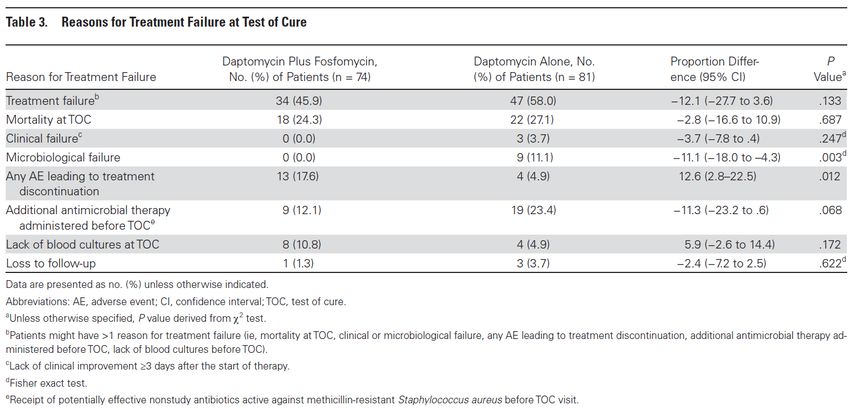
• Study design: Randomized (1:1) phase 3 superiority, open-label trial
• Study sites: 18 Spanish hospitals
• Recruitment: 12/2013 – 11/2017
• Participants: Adult inpatients ≥18y
• Inclusion criteria: MRSA bacteremia (Def.: ≥1 pos. blood culture ≤72 hours)
• Exlusion criteria: Life expectancy ≤24 hours, polymicrobial bacteremia,
pneumonia as a source of bacteremia, prosthetic valve
endocarditis, NYHA III/IV, severe end-stage liver disease
(Child-Pugh C), any clinical condition requiring additional
antibiotics active against MRSA, prior history of eosinoph.
pneumonia, allergy to daptomycin or fosfomycin
• Study arms: I: Daptomycin 1x 10 mg/kg/d i.v.
II: Daptomycin 1x 10mg/kg/d + Fosfomycin 4x 2g/d i.v.
10 – 14 days for uncomplicated bacteremia
28 – 42 days for complicated bacteremia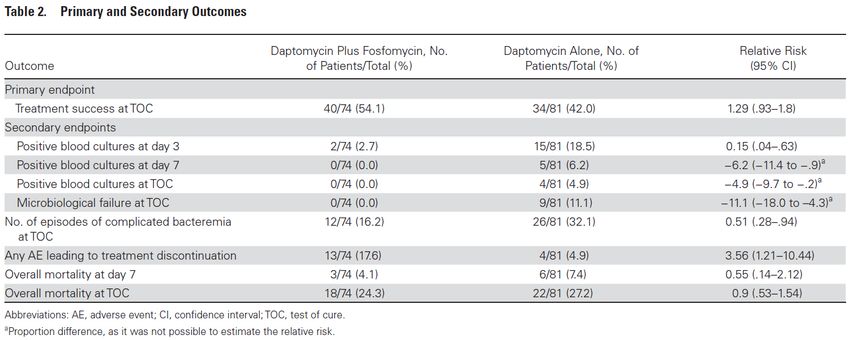
• Sample size calc.: 81 patients per arm to detect a 20% differences between
arms with a power of 80% and an α-level of 0.05
• Primary endpoint: Test of cure (TOC) at 6 weeks after the end of therapy
(Def.: alive + resolution of symptoms + neg. blood cultures)
• 2ndary endpoints: -- bacteremia at day 3, day 7, and at week 6
-- microbiological failure*; complicated bacteremia
-- AEs leading to treatment discontinuation
-- mortality due to any cause at day 7 and at week 6
[* persistent bacteremia, recurrent bacteremia,
emergence of resistance to study drugs]
• Analysis: (i) modified intention-to-treat analysis, including all appropriately
randomized patients who received ≥24h of antibiotic therapy
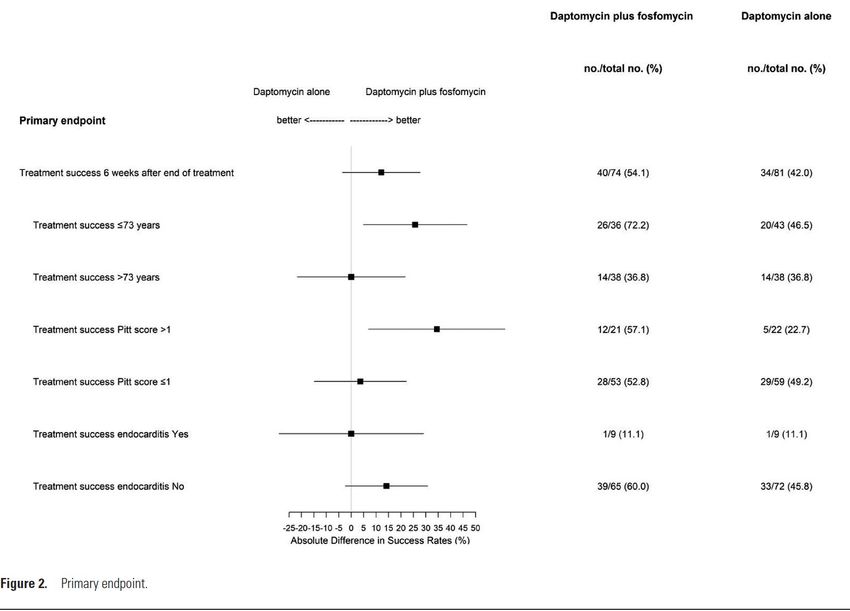
(ii) subgroup homogeneity analysis of the treatment effect
-- age
-- presence of endocarditis
-- Pitt Bacteremia Score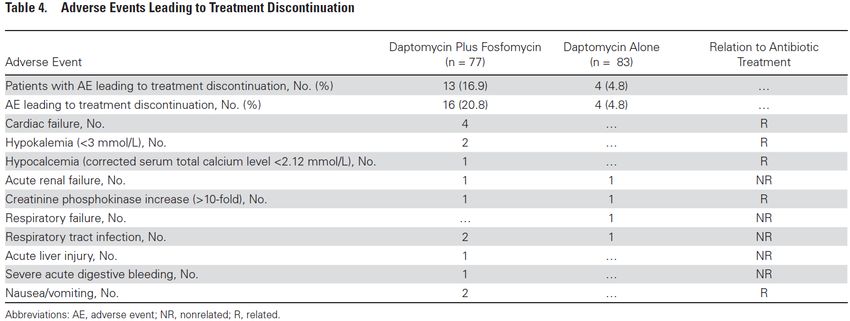
Pitt Bacteremia Score Review on the Pitt Bacteremia Score: Al-Hasan MN , Baddour LM. Resilience of the Pitt Bacteremia Score: 3 Decades and Counting. CID 2020;9:1834–36.
Sample size ~ reached
PBS
p = 0.133
p < 0.001
* p = 0.022
p = 0.012
p = 0.687
* complicated bacteremia:
- spread of infection
- suppurative thrombophlebitis
- endocarditis
- infection involving a foreign material that could not be removed inConclusions:
• The 12% higher treatment success rate did not reach statistical significance
• Combination therapy prevents microbiological failure but is more often
associated with adverse events
• Combination therapy may possibly be more effective than monotherapy in
younger patients and in those with more severe disease
Strengths/limitations:
• Strength: solid design & analysis, low drop-out rate (enrolment challenging)
• Limitation: - no blinding; may have impacted discontinuation due to clinical
worsening or suspected AEs or escalation of treatment
- low number of patients with endocarditis & critically ill patients
Outlook:
• A One-fits-all treatment approach is unlikely: e.g. putative benefit of CT in a
young IVDU with MRSA endocarditis vs. AE-related disadvantage of CT in an
old comorbid patient with catheter-related MRSA bacteremia
• Limiting combination therapy to clearance of bacteremia?Thanks!
You can also read

















































