D-2.4.3. Studies using the German results extended to the partner institutes JRP6 - NOVA - FBZ1 - 1st Call - One Health EJP
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
D-2.4.3. Studies using the German results extended to the partner institutes JRP6 - NOVA - FBZ1 - 1st Call Responsible Partner: SVA
GENERAL INFORMATION
European Joint Programme Promoting One Health in Europe through joint actions on foodborne
full title zoonoses, antimicrobial resistance and emerging microbiological hazards
European Joint Programme One Health EJP
acronym
Funding This project has received funding from the European Union’s Horizon
2020 research and innovation programme under Grant Agreement No
773830.
Grant Agreement Grant agreement n° 773830
Start Date 01/01/2018
Duration 60 Months
DOCUMENT MANAGEMENT
JIP/JRP Deliverable D-2.4.3
Join Integrative/Research JRP6 - NOVA - FBZ1 - 1st Call
Project
JIP/JRP Leader Jenny FROSSLING (SVA)
Other contributors Ides Boone, Hendrik Wilking, Klaus Stark, Sebastian Haller, Tim
Eckmanns (Robert Koch Institute, RKI)
Michele Luca D'Errico, Gaia Scavia, Rosangela Tozzoli (Istituto Superiore
di Sanità, ISS)
Luigi Iannetti (Istituto Zooprofilattico Sperimentale dell’Abruzzo e
Molise, IZSAM)
Due month of the deliverable M24
Actual submission month M24
Type R: report
R: Document, report
DEC: Websites, patent filings,
videos, etc.
OTHER
Dissemination level CO
PU: Public
CO: confidential, only for
members of the consortium
(including the Commission
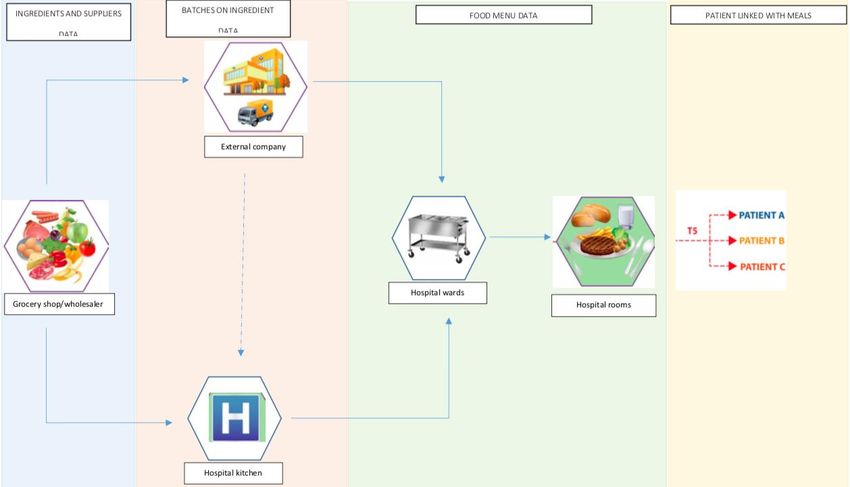
Services)Evaluation of the feasibility of investigating food consumption patterns via electronic data in Italy and Germany Introduction Healthcare associated foodborne outbreaks (HAI-FBO) result from exposure to contaminated food within a healthcare institution. They can cause considerable morbidity and mortality in hospital patients and nursing home residents, especially in highly susceptible populations. They can also affect staff members and cause major disruption of services. In the EU, data on foodborne outbreaks are reported to EFSA in accordance with Directive 2003/99/EC, and include information on causative agents, implicated vehicles and settings including hospitals. Surveillance data and published literature could suggest an underreporting problem of HAI-FBO. This may partly be explained by an underdetection because food vehicles are less frequently analysed as a potential vehicle of outbreaks in healthcare institutions. Timely identification and investigations of HAI-FBO are particularly crucial in order to avoid negative consequences to patients’ and staff members’ health and hospital resources. This requires detailed data of food exposures from patients or residents from healthcare institutions, which is not always easily obtainable. In fact, collecting food exposure history from populations in healthcare settings may be resource-intensive and time-consuming, which slows down outbreak investigations and implementation of effective control measures, especially because different food supply chain types exist in healthcare institutions (Figure 1). This situation has highlighted the need for new ways to obtain such data. For this reason, to enable a more rapid identification of potential food sources associated with a HAI-FBO, stored menu data from healthcare institutions may be used. To examine this further, we performed surveys among health care institutions and here report on the methods, results and conclusions. We plan to present the content of this deliverable as a scientific publication, which is expected to be ready for submission within the first half of 2020.
Figure 1. Food chain from raw material suppliers to the meals distributed to the patients / residents of nursing homes. Objective: To explore the data availability, accessibility, and usefulness of menu/catering data of food served to patients in hospitals and nursing home residents in healthcare institutions, in order to support healthcare associated foodborne outbreak investigations. Material and methods Sampling The sampling was jointly carried out by the NOVA partners in Italy (ISS and IZSAM) and in Germany (RKI). In Italy, this survey has been carried out by the National Institute for Public Health (Istituto Superiore di Sanità, ISS) and the Istituto Zooprofilattico Sperimentale dell’Abruzzo del Molise (IZSAM) among different health-care settings between June and November 2019. A convenience sampling strategy was adopted in Italy. The survey performed by ISS included second- level paediatric hospitals (including special and reference clinical units and branches). In addition, a few general hospitals were also included among the hospitals known to be interested in establishing an active surveillance for hospital-acquired viral infection. This was carried out in connection with an ongoing national project dedicated to viral nosocomial infections. The hospitals were located all over Italy.
The study performed by IZSAM included both general hospitals and nursing homes, all located in the
Teramo province in the Abruzzo region (central Italy). All premises were chosen because directly or
indirectly managed by the Teramo Local Health Unit (public health service).
A concept note (annex 1) describing the field of investigation and the aims of the NOVA survey and
our study, was sent via e-mail to the Medical directorates of the 25 hospitals (14 paediatrics; 11
general hospitals) and of the 4 nursing homes included in the sampling list to support our request for
collaboration and to get a formal partnership agreement. A hard copy of the questionnaire used for
the survey was then delivered only to those hospitals that agreed to collaborate, in order to let the
respondents be aware of the specific questions and be prepared at the time of survey administration.
In Germany, from August to September 2019, the Robert Koch Institute, carried out the survey by
taking a convenience sample from the registered healthcare institutions, consisting of both hospitals
and nursing homes.
Questionnaire
A questionnaire was jointly developed by the RKI, ISS and IZSAM. It consisted of core questions
(shared questions in Italy and Germany) and additional questions administered in Italy or Germany.
Mode of administration was slightly different in Germany and Italy.
In Italy, a semi-structured questionnaire developed by ISS was delivered to participants that accepted
to collaborate (12 paediatric hospitals and 3 general hospitals) using the web platform Lime survey.
Participants were requested to fill in the on-line questionnaire (self-administration) after logging-in,
and to submit the final version to ISS using the web platform. This allowed participants to answer the
questions at different times and to spend the times needed to collect further detail to complete the
questionnaire. A semi-structured questionnaire was also developed by IZSAM and directly
administered to the medical direction of the premises that accepted to collaborate (4 general
hospitals and 2 nursing homes), precisely to the dieticians in charge of deciding the menus to be
proposed to the patients.
The core questions were shared with NOVA partners involved in the same task (RKI, IZSAM) and the
following areas were explored (Annex 2):
Description of the hospital catering service dedicated to patients;
Food menu data availability and traceability;
Food menu data accessibility;
Risky foods (in Italy only by IZSAM).
Beyond the core questions, the Italian questionnaires administered by ISS and IZSAM (Annex 3) were
also aimed at investigating the availability of data on single ingredients, suppliers and batches of
ingredients. In addition, the presence of specific policy for bringing, preparing and storing in the
hospital food from home intended to be consumed by patients was also investigated.
In addition, the Italian questionnaire was also adapted to investigate how the compliance to the
European regulatory standards ‘hygiene package’ (Reg. (EC) No 852/2004; Reg. (EC) No 853/2004;
Reg. (CE) No 854/2004; Reg. (CE) No 882/2004; Directive2003/99/EC) and to the national guidelines
for hospital and healthcare catering (Ministero della Salute, 2011).In Germany, the questionnaire was designed as a form in Adobe Acrobat in order to facilitate self- administration and coding. The questionnaire was sent by email to the direction of healthcare institutions together with a description of the study, and instructions on how to fill in the questionnaire. Depending on the healthcare institution, questionnaires were forwarded to hospital infection control specialists, kitchen hygiene staff, kitchen manager or hospital caterers. Completed questionnaires were sent back by email. In total, five hospitals (2 general hospitals, 2 university hospitals, 1 specialised hospital), two specialised hospitals combined with nursing homes, and six nursing homes participated in the survey. The German questionnaire included additional questions on the storage of reference food samples (quantity and storage time) of food served in healthcare institutions (Annex 4). Results In total, 33 healthcare institutions (HCI) participated in the survey (Table 1). Table 1. Distribution of healthcare institutions participating in the NOVA survey. Healthcare Setting Germany Italy Total Hospital 5 18 23 Nursing home 6 2 8 Nursing home integrated with hospital 2 2 Total 13 20 33 1. Core questions in Germany and Italy 1.1 Characterisation of healthcare institutions in the survey The distribution of the participating hospitals by bed numbers is represented in Figure 2. In Italy, 11 paediatric hospitals, and 7 general hospitals participated, whereas in Germany, 2 general hospitals, 2 university hospitals and 3 specialised hospitals * (of which 2 were integrated with a nursing home) participated. In Italy, two nursing homes participated (75 and 225 residents), while in Germany, 6 nursing homes, and 2 nursing integrated with a specialised home were included in the German survey totalling 842 residents (range: 19 to 250 residents).
Figure 2. Size of hospitals (number of beds) in the survey. *includes two hospitals integrated with a nursing home. 1.2 Catering systems by healthcare settings, in Italy and Germany The catering system1 in Italy and Germany varied by healthcare setting (Figure 3). A mixed catering type was more frequent in Italian hospitals (12/18 HCI), whereas in German hospitals in-house catering was more frequent. In nursing homes in Germany, the in-house catering type predominated (4/6 nursing homes). Figure 3. Distribution of catering systems of healthcare institution included in the survey, in Italy and in Germany (n=33). *One HCI integrating a hospital and a nursing home, with external catering type for the hospital, and mixed type catering for the nursing home component We did not observe differences in the organisation of catering type (external, in-house, mixed) between different patients/nursing home residents (e.g. immunocompromised patients, patients 1 In-house kitchen: both staff and patients /nursing home residents receive food from the same kitchen managed by the healthcare facility External catering: all the services, preparation and cooking steps are undertaken by an external company outside the hospital Mixed Catering: In-house-Catering, combined with external catering (e.g. external company that works in the hospital kitchen)
with allergies/intolerances, special diets). Catering of hospitals in Italy (Abruzzo region) was part of larger consortia, whereas in Germany, catering for single healthcare hospitals were also represented (n=3) (figure 4). Figure 4. Organisation of catering system in consortiums of HCI. *Only HCI sampled by IZSAM (Abruzzo region) 1.3 Food menu data availability In Germany, three HCI (1 hospital, 1 nursing home and a hospital integrated with a nursing home) did not document what patients ate, except for specific patients or nursing home residents with special needs (e.g. cachexia) (Figure 5). In Figure 6, we illustrate if there are differences of documented food items for each meal (e.g. breakfast, lunch, dinner, snack time). This area of interest was not explored by ISS because, in Italy, food items served at breakfast and snack time are usually considered at very poor risk of contamination. Moreover, it is well known that in Italy it is possible to obtain all the menu data about the possible options for breakfast and snack time but it is not possible to know unequivocally which patient consumed a specific food. Figure 5. Documentation of food menu data in Italy and Germany
Figure 6. Documentation of food menu data for all meals (breakfast, lunch and dinner) in Italy and Germany. *Italy: only HCI from IZSAM, 1 HCI missing. With regard to the possibility of establishing a link between the individual patient/nursing home resident and the meal consumed, in Germany food menu data could be linked for all patients or specific patients in 6/12 HCI* (*1 Missing answer from a hospital). In contrast, in Italy, this link was possible in 18/20 HCI (figure 7). Figure 7. Link of food menu data with individual patients, in Italy and Germany
Figure 8. Access to food menu data by healthcare institution or caterer, in Italy and Germany. Multiple choice question, answers from 4 German HCIs missing. Data storage of menu plans by health care institutions (Figure 9) varied from 2 days to more than 10 years, and in Italian hospitals and in nursing homes, between 1 month and more than one year. In Germany, data storage of menu data ranged from 2 weeks to 3 years in hospitals, and 6 months to 5 years in nursing homes. Figure 9. Distribution of food menu storage type by healthcare setting in Italy and Germany In Italy, the majority of the hospitals (n=15) had a searchable database of patient menu data, whereas searchable database was reported in 3 hospitals in Germany (Figure 10).
Figure 10. Format of the food menu data in healthcare institutions in Germany and Italy. Multiple choice question. *Missing answers from 2 HCI. In total, two healthcare institutions (1 nursing home in Italy and one hospital in Germany) have previously used food menu data to investigate a potential foodborne infection in hospital patients or nursing home residents. Documentation of ordering but not eating a meal was carried out in three nursing homes in Germany (out of answers of 8 HCI). In contrast, in Italy*, all healthcare institution documented this information. *In Italy, this question was restricted to the questionnaire from IZSAM (Abruzzo). All food menu data can be made available for outbreak investigation purposes (within 1-2 days) in Germany (n=7 answering this question) and all healthcare institutions sampled in Italy (IZSAM only, n=6).
2. Additional questions (country-specific) 2.1. Food from home (Italy) Figure 11. Availability of policy for food brought from home (n=20) Figure 12. Availability of prescription for sharing food from home among patients in hospitals with policy for food from home (n=11).
Figure 13. Policy for storing and preparing food from home into the hospital (n=20)
2.2. Risky foods available on the menu in healthcare institutions 2.2.1 Germany (n=13) Risky food products including raw sausage products (10/13 HCI), deli-salads, soft cheese and smoked fish were offered in the German HCI (figure 14). Figure 14. Risky food offered in healthcare institutions in Germany 2.2.2 Italy (IZSAM) (n=6) Figure 15. Risky food offered in healthcare institutions in Italy (n=6) 2.3. Storage of food reference samples (Germany) In Germany, food reference samples were taken in all HCI, except in two German nursing homes (2/13). In total 11/13 HCI took these reference samples (at least) for lunch meals. From these, 4 HCI took reference samples from all meals (breakfast, lunch and dinner). Storage time of food reference samples of food offered to HCI varied from 20 days (figure 16).
Figure 16. Storage time of food reference samples of healthcare institutions in Germany
Discussion Study limitations: This pilot study explored nearly which catering resources, food menu data, practices and tools are available at hospital and nursing homes level to support HA-FBO investigation. In order to maximise the participation of hospitals and nursing homes, a convenience sample was taken. Therefore, results are not representative for the whole healthcare setting population, and we should be careful in extrapolation of our results. Nonetheless, the study yielded imported findings for the ‘vulnerable’ population in healthcare setting including hospitals and nursing homes. Our survey results indicated a high variability and variety of catering organisation in healthcare institutions in Germany and in Italy. Similarly, a survey in Germany by DKI (2016) described the variety and trends in catering organisation for hospitals (> 80 beds) between 2006 and 2016. Issues in awareness of risk posed by FBO in healthcare settings were highlighted in this study. In Italy, externalisation of food catering service is frequently associated with a non-optimal awareness about the availability of traceability and menu data. This suggests a possible non-optimal awareness of the risk posed by FBO in hospital settings. Risky foods were offered in hospitals and nursing homes in Germany and in Italy. In Germany, raw pork products, delicatessen salads, soft cheese, smoked fish were common in the menu of hospitals and nursing homes, despite food safety recommendations for highly vulnerable population groups (Federal Institute for Risk Assessment (BfR). 2011). These findings correspond with the results from the food monitoring 2017 of the German Federal Office of Consumer Protection and Food Safety (BVL) stating that in many hospitals and nursing homes in Germany, patients and residents were exposed to the same risky food which may represent an unnecessary risk for highly sensitive populations. Differences in consumption habits were observed between Italy and Germany with regard to food served at breakfast vs other meals. Breakfast are not considered at high risk in Italy because usually it only includes ‘safe’ products (food items include pre-packed cooked products only, such as biscuits and/or similar products, rusks, crackers; pre-packed fruit puree fresh fruits (whole fruits not pre- peeled); pasteurised milk, the, coffee; pre-packed fruit juice. In contrast, in Germany, breakfast is considered as a full meal which may include also risk food products (e.g. raw meat products, soft cheese) for vulnerable populations. The large variance in answers both in Italy and Germany suggests that data access and usefulness of food menu data for healthcare associated foodborne outbreaks (HA-FBO) is currently not optimal and data availability and standardisation/harmonisation should be improved. A large variety was observed in the documentation of meals. In Germany, nearly half of the healthcare institutions (mainly nursing homes) did not document food menu data for all meals (only lunch meals). Furthermore, a lack of harmonisation was identified in Italian and German healthcare institutions with respect to the format of the food menu data, ranging from paper, electronic data (PDF) formats - which are not readily usable - to electronic searchable databases (fit for purpose for HA-FBO). However, electronic searchable databases for food menu was much more common in Italy (present in 11/18 hospitals and 2/2 nursing homes).
In addition, the storage time for food menu data greatly varied within hospitals and nursing homes. A possible development of a standard for fast identification of food potentially implicated in an HA-FBO should comply with multiple systems! In Italy, specific food safety guidelines for healthcare catering organisations focusing on the risk of HA-FBO for vulnerable populations have received little attention. In Germany, specific food safety recommendations for vulnerable populations in healthcare institution exist from the hospital hygiene (KRINKO, 2010) and the food safety side (BfR, 2011), but are insufficiently known, as highlighted by the monitoring report from German Federal Office of Consumer Protection and Food Safety (BVL, 2018). In Germany, a minority of healthcare institutions (2 hospitals, 1 nursing home) were able to unequivocally link individual patients with their respective food menu data, whereas in Italy, this link could be established in 17/20 healthcare institutions. Understanding the complexity of the catering management system in healthcare institutions is crucial; terms as Insourcing/outsourcing/in-house/externalisation may create confusion but are essential for HA-FBO investigations. This is important as the subject entitled of the catering service (the hospital or a company) is usually the owner or custodian of the traceability data. An external company may in any case prepare the meals outside the hospital or ‘in-house’ (using the hospital facilities), with consequent different levels of risk. In Italy, in-house is usually associated with better quality of the food served, and in some place, a deliberate choice of the facility for in-house catering was made to improve the food quality in order to discourage food bringing in from home. Concluding recommendations Due to the large variability in accessibility, type and format of food menu/catering data, its usefulness for HA-FBO is currently non-optimal both in Italy and Germany. Individual registration of hospital food menu data should be extended to all meals (not only lunch). Individual registration of food menu data in hospitals and nursing homes using searchable database will increase the usefulness of food menu data for outbreak purposes. Awareness should be raised to avoid risky foods for vulnerable populations in hospitals and nursing homes.
Acknowledgements We thank the healthcare institutions for participating in the survey, and Hans-Peter Blank and Hartwig Wehrmeyer (RKI) for designing the Adobe Acrobat Form and coding of the questionnaires References BfR (Federal Institute for Risk Assessment) (2011). Merkblatt für weitere Berufsgruppen: Sicher verpflegt – Besonders empfindliche Personengruppen in Gemeinschaftseinrichtungen. https://www.bfr.bund.de/cm/350/sicher-verpflegt-besonders-empfindliche-personengruppen-in- gemeinschaftseinrichtungen.pdf. (accessed: 17.12.2019). BVL (Bundesamt für Verbraucherschutz und Lebensmittelsicherheit). (2018). Bundesweiter Überwachungsplan 2017. BVL-Report 13.3. Berichte zur Lebensmittelsicherheit. Available at: https://www.bvl.bund.de/SharedDocs/Berichte/02_BUeP/2017_BUeP_bericht.pdf?__blob=publicati onFile&v=3. (accessed: 17.12.2019). DKI – Deutsches Krankenhausinstitut, K&P Consulting GmbH. Verpflegungsdienstleistungen im Krankenhaus – Studie 2016. Ergebnispräsentation. Available at: https://www.dki.de/sites/default/files/2019-05/Verpflegungsleistungen%20im%20Krankenhaus.pdf. (accessed: 17.12.2019). KRINKO (Kommission für Krankenhaushygiene und Infektionsprävention). (2010). Anforderungen an die Hygiene bei der medizinischen Versorgung von immunsupprimierten Patienten. Bundesgesundheitsblatt, 53, 357–388.
Annex 1. Concept note, survey in Italy (ISS and IZSAM)
Alla cortese attenzione di:
XXXX
Direttore Sanitario del XXXX
XXXX
Oggetto: proposta di collaborazione scientifica per un’indagine promossa dall’Istituto Superiore di
Sanità (ISS) sul rischio epidemico di malattie a trasmissione alimentare in ambito nosocomiale e sulla
ristorazione ospedaliera.
Gentile Dott XXX,
la contatto per chiedere la disponibilità del XXXX, a partecipare ad un’attività di indagine
epidemiologica sugli aspetti relativi al rischio epidemico di malattie a trasmissione alimentare (MTA)
in ambito nosocomiale.
L’Istituto Superiore di Sanità (Dip. di Sicurezza Alimentare, Nutrizione e Sanità Pubblica Veterinaria)
partecipa ad un programma CCM sulla sorveglianza delle infezioni gastroenteriche (GE) da Norovirus
(NoV) e Rotavirus (RV) associate all'assistenza sanitaria e inoltre ha intrapreso un’indagine mirata ad
approfondire gli aspetti relativi al rischio epidemico di malattie a trasmissione alimentare (MTA) in
ambito nosocomiale ed agli aspetti inerenti la ristorazione ospedaliera. Tale progetto nasce dalla
considerazione delle peculiarità specifiche del contesto ospedaliero ed assistenziale, capaci di
influenzare in modo determinante e caratteristico le modalità di manifestazione delle MTA in ambito
nosocomiale, la loro diffusione, l’impatto sulla salute dei pazienti e gli aspetti relativi al controllo.
È noto che l’occorrenza delle epidemie nosocomiali di MTA, cosi come quelle causate da agenti
virali come i Norovirus e/o i Rotavirus, è largamente sottostimata in Italia e nell’UE. I dati di
letteratura e delle fonti informative ufficiali sono infatti assai limitati. Un’identificazione tempestiva
dei focolai epidemici di MTA è essenziale per poter controllarne efficacemente la diffusione.
La sorveglianza delle MTA e delle gastroenteriti acute in ambito nosocomiale, assume caratteri di
particolare importanza in considerazione della vulnerabilità dei pazienti, del contesto ambientale e di
permanenza dei pazienti nonché delle caratteristiche e identità socio-culturali, capaci di influenzare
variabilmente le abitudini alimentari. Vi è da considerare, a tale riguardo, che il recente rapido
sviluppo dei sistemi di sorveglianza molecolare basati sulla caratterizzazione mediante tecniche di
Next Generation Sequencing dei patogeni coinvolti nelle MTA e nei casi di GE virali nocosomiali, apre
nuove possibilità di indagine, caratterizzazione e controllo nella triade uomo-ambiente-alimenti.Immagine: Diagramma di flusso dalla materia prima alla distribuzione del pasto ai pazienti in ambiente ospedaliero L’obiettivo dell’indagine è di raccogliere elementi descrittivi utili alla caratterizzazione della filiera di produzione e consumo di alimenti in ambito ospedaliero, della sorveglianza clinica delle malattie a trasmissione alimentare e del monitoraggio dei pericoli microbiologici negli alimenti. Inoltre si intende raccogliere informazioni utili alla valutazione dell’impatto delle gastroenteriti acute nosocomiali causate da Norovirus e Rotavirus, su pazienti pediatrici e adulti. I risultati dell’indagine verranno utilizzati per i) migliorare la conoscenza del fenomeno; ii) ottimizzare l’approccio metodologico alla sorveglianza e controllo delle MTA in ambito nosocomiale; iii) favorire il ricollegamento con i flussi informativi ufficiali di allerta nell’ambito della sorveglianza epidemiologica della MTA e in sicurezza alimentare. In che cosa consiste l’indagine e che tipo di collaborazione vi chiediamo. L’ISS ha formulato un questionario di indagine che ha come obiettivo la raccolta di informazioni presso la vostra struttura assistenziale, in merito all’occorrenza di focolai epidemici di malattie a trasmissione alimentare e gastroenteriti virali, le modalità organizzative della ristorazione e la somministrazione dei pasti ai pazienti, con particolare riguardo alla disponibilità ed accessibilità ai dati di tracciabilità degli alimenti e dei loro ingredienti. Inoltre sono esplorati alcuni aspetti relativi agli alimenti consumati dai pazienti ma preparati/acquistati in modo autonomo dai pazienti e/o loro familiari. Tali informazioni consentiranno di valutare la fattibilità di studi di tracciabilità a seguito della potenziale esposizione ad un determinato alimento contaminato (trace-forward), anche in collegamento con i sistemi di allerta in sicurezza alimentare o per l’identificazione dei veicoli alimentari implicati e delle sorgenti di contaminazione (trace-back). La vostra struttura è stata selezionata poiché siamo interessati in modo particolare ad approfondire gli aspetti descritti nella popolazione dei pazienti pediatrici. Le chiediamo la disponibilità a collaborare all’indagine indicandoci il riferimento (email e contatto telefonico) di una persona della Direzione Sanitaria a cui rivolgerci per la raccolta delle informazioni attraverso un questionario on-line. L’accesso al questionario avverrà tramite un link che sarà inviato
via email. Per permettervi di visualizzare gli argomenti e le tematiche indagate alleghiamo una copia
.pdf del questionario.
Pubblicazione dei risultati e riconoscimento del contributo
Questa indagine conoscitiva rientra nell’attività di ricerca intrapresa dall’ISS nell’ambito del progetto
NOVA (Novel approaches for design and evaluation of cost-effective surveillance across the food
chain) del Joint Programme europeo One Health EJP (https://onehealthejp.eu/) e del progetto CCM
(Sorveglianza delle infezioni gastroenteriche da Norovirus e Rotavirus associate all’assistenza
sanitaria). Le informazioni, raccolte in modo armonizzato anche da parte dell’Istituto Zooprofilattico
Sperimentale G. Caporale (Teramo) e in Germania nell’ambito di uno studio parallelo coordinato dal
Robert Koch Institute, saranno analizzate dall’ISS e restituite in modo aggregato ai partecipanti, per
un ulteriore analisi critica da parte delle strutture ospedaliere/assistenziali coinvolte. È prevista la
pubblicazione dei risultati finali nell’ambito del progetto e attraverso articoli su riviste scientifiche
del settore, in cui sarà attivamente riconosciuto nell’authorship il contributo dei partecipanti.
Per qualsiasi informazione o chiarimento inerente l’indagine vi preghiamo di contattare:
XXXX
Ringraziandola anticipatamente per la disponibilità, rimaniamo in attesa di un Suo cortese riscontro.
Cordiali salutiAnnex 2. Questionnaire - Core Questions in Italy and Germany
CATERING
1. Type of healthcare facility (HCF)
a. Hospital
30 - 200 beds □
201–800 beds □
>800 beds □
1. Primary ‘district hospital’ or ‘first-level referral’
2. Secondary ‘provincial hospital’ or ‘second-level referral’
3. Tertiary ‘central’, ‘regional’ or ‘tertiary-level’ hospital (e.g.university hospital)
4. Specialised hospital. Single clinical specialty...........................................................□
Number of beds?.............................
b. Nursing home □
Number of residents?......................
2. How is the food supply for the majority of the patients in the healthcare facility organised?
a. External catering company
b. In-house kitchen
c. Mixed
Describe briefly your mixed system.……………………………………….......................
External catering: all the services, preparation and cooking are undertaken by an external company
In-house kitchen: both staff and patients / nursing home residents receive food from the same kitchen
managed by the healthcare facility3. In case of a mixed catering system, please specify for each category of patients / nursing home
residents below, the catering system you are relying on:
CATERING
i. In-house External Mixed
a. Immunocompromised patients/nursing home
residents
b. Patients/nursing home residents with food
allergies/intolerances (e.g. gluten or lactose
intolerance/allergy)
c. Patients/nursing home residents with special diets for
physiological and/or pathological status (e.g. low
calories diet, low-protein diet, etc.)
d. Patients/nursing home residents with special diets
(vegetarian, vegan or respectful of different ethnic
groups or religious beliefs menus)
e. Patients/nursing home residents who do not need to
follow a specific diet
4. In case you rely on an external company for hospital catering, does your external company supply
food only in your hospital or in a network of healthcare facilities?
a. Only in our hospital
b. In a network of healthcare facilities
c. I don’t know
FOOD MENU DATA AVAILABILITY
5. Do you document what the patients or nursing home residents eat/have eaten?
Y. Yes please specify................................................................................................
N. No
6. If yes, are all food items documented for each of the meals (i.e. breakfast, lunch, dinner) or only
for specific meals?
Yes, documented for all meals □
Only for certain meals:
a. Breakfast
b. Lunch
c. Dinner
d. Other: please specify..................................................................7. Can you link the food menu data to the individual patient ID (patient number) or individual
nursing home resident?
a. No
b. Yes, can be linked for all patients / nursing home residents
c. Yes, but only for specific patients, or wards
Please specify,.................................................................................
8. Is the level of detail for menu data different according to the meals? (e.g. breakfast only
available as buffet, lunch menu data is detailed)
a. No, the level of detail is the same for all meals
b. Yes, there are differences between the level of detail for the different meals
Please specify....................................................................................
9. Where is the food preference list of individual patients/residents stored?
a. Individual health care institutions
b. Consortium of health care institutions
c. Kitchen
d. Catering company/companies
e. Other, namely …………………......................................
10. How long are the data stored?
Please detail: ...................................... (weeks/months/years)
11. What is the format of the food menu data?
a. Paper
b. PDF/Word files
c. Electronic searchable database (Information system)
If “b” or “c”,
Please detail what format of electronic data or the type of information system:
.............................................................
12. Have you ever used in your institution food menu data in relation with patients / nursing home
residents who had possibly eaten a contaminated food product?
No
Yes
Please describe under which circumstances....................................................................
13. Is it documented when individual patients/residents do not eat a meal ordered?
No...............................................□
Yes..............................................□14. Would it be possible to make these data available for surveillance purposes? 1-2 days
a. yes, all
b. yes, all but only if made anonymous
c. only some data
d. No
15. Are following food items offered to patients/nursing home residents in your healthcare
institution?
Yes No Don’t know
a. Delicatessen salads (meat, fish, egg, potato)
b. Spreadable raw sausage
c. soft cheese
d. smoked fish
e. unheated frozen berries
f. pre sliced cooked meat products
g. cooked meat products not pre sliced
h. cured meat
i. shell eggs Annex 3 – Additional questions in the survey in Italy (ISS and
IZSAM)
1. The aim of the following questions is to identify who, between the hospital ("H") or the catering
outside the hospital ("C"), keeps information on the traceability of food consumed by the patients
I DON’T
H C
KNOW
a. Who keeps the information about which SUPPLIERS provided the food
ingredients used for food preparation?
b. Who keeps the information about which INGREDIENTS were used for food
preparation?
c. Who keeps the information about which BATCH OF PRODUCTION of the raw
materials/ingredients were used for the preparation of each food item served to
the patients?
d. Who keeps the information about the single plates or trays served to by
patients?
2. How do you judge the ease of access to the information on plates or trays booked by patients in
hospital for each meal?
PLEASE CHOOSE ONE OPTION
Good, the information is directly accessible to the hospital staff
Satisfactory, It is possible to obtain the information after request to the catering company that
manages the hospital catering
Other (describe briefly): ………
This information cannot be accessed by the hospital staff (MOVE ON TO QUESTION 9)
a. In which format is this information available?
MULTIPLE ANSWER ARE POSSIBLE
Paper format PDF/Word file Digital (Searchable database)
Other, specify: ………………………………………………………..
b. How long is this information stored?
Specify: ………………………………………………………… (weeks/months/years)
3. Is it possible to link unequivocally each patient to the plates they consumed or the trays they were
given while hospitalised (picture 2: T5)?
Yes
No4. Is it possible to establish the same link for patients that could not book the meal in advance (e.g.
patients in day-hospital, emergency)?
Yes
No
5. Is it possible to know unequivocally which production batches of raw materials/ingredients have
been used for the preparation of the plates or the trays they were given for each meal (picture 2: T1,
T2)?
Yes
Not sure, It must be verified with the catering company that manages the hospital catering
No
I don’t know
BRINGING FOOD INTO HOSPITAL POLICY
6. Is in this hospital in place any policies about bringing food10 from home intended to be consumed by
patients?
Yes, describe briefly: ……………………………
No (MOVE ON TO QUESTION 29)
GLOSSARY
10FOOD: do not consider chewing gum, bottled drinks or packaged food (e.g. snacks).
7. Is in this hospital in place any indications aiming at controlling the possibility of patient sharing food
brought from home or cooked/heated in the hospital?
Yes
No
8. Is in this hospital or at least in some hospital departments possible to prepare and heat food brought
from home intended to be consumed by patient?
Yes
No
9. Is in this hospital or at least in some hospital departments possible to store food brought from home
(e.g. refrigerator, freezer, etc.) intended to be consumed by patients?
Yes
NoAnnex 4. Additional question in the survey in Germany (RKI) 18. Of which meals, reference samples are taken? □ a. Breakfast □ b. Lunch □ c. Dinner □ d. Other □ Please specify: ............................................. □ e. No reference samples taken 19. What is the storage time of the reference samples? < 7 days □ 7 – 13 days □ 14–20 days □ >20 days □
You can also read

















































