From New Mechanisms to New Standards of Care - Corporate Presentation January 2020
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

From New Mechanisms to New Standards of Care Corporate Presentation January 2020

Forward-Looking Statements Statements in this presentation, other than statements of historical fact, constitute forward-looking statements within the meaning of the safe harbor provisions of the Private Securities Litigation Reform Act of 1995. These forward-looking statements include statements regarding Summit’s clinical trials supporting the safety and efficacy of its product candidates and the potential novelty of such product candidates as treatments for disease, plans and objectives for preclinical studies, clinical trials, product development and regulatory filings, Summit’s collaboration with Eurofarma Laboratorios SA, Summit’s award from BARDA, Summit’s Discuva Platform, strategies, future performance, expectations, assumptions, financial condition, liquidity and capital resources. These forward-looking statements may be preceded by, followed by or otherwise include the words “anticipate,” “believe,” “estimate,” “expect,” “intend,” “may,” “plan,” “predict,” “project,” “target,” “potential,” “will,” “would,” “could,” “should,” “continue,” and similar expressions. Actual results or events may differ materially from those expressed or implied in any forward-looking statements due to various factors, including the risks and uncertainties inherent in clinical trials and product development and commercialization, such as the uncertainty in results of clinical trials for product candidates, the uncertainty of whether the preliminary results from a clinical trial will be predictive of final results of that trial or whether the results of clinical trials will be predictive of results in later stages of product development, the risk of delays or failure to obtain or maintain regulatory approval, the risk of failure of the third parties upon whom Summit relies to conduct its clinical trials and manufacture its product candidates to perform as expected, the risk that any third-party collaborator, including Eurofarma, terminates or fails to meet its obligations to Summit, the risk of the ability of BARDA to terminate our contract for convenience at any time, the risk that Summit’s discovery and development platform may not identify new potential drug development candidates, the risk of increased cost and delays due to delays in the commencement, enrollment, completion or analysis of clinical trials or significant issues regarding the adequacy of clinical trial designs or the execution of clinical trials and the timing, cost and design of future clinical trials and research activities, the timing of expected filings with the FDA or other regulatory agencies; and the other risks and uncertainties described in Summit’s public filings with the Securities and Exchange Commission. Summit may not actually achieve the plans, intentions or expectations disclosed in its forward-looking statements, and you should not place undue reliance on its forward-looking statements. Actual results or events could differ materially from the plans, intentions and expectations disclosed in forward-looking statements. You are cautioned not to place undue reliance on these forward-looking statements, which speak only as of the date hereof. Summit disclaims any intent or obligation to revise or update these forward-looking statements, except as required by applicable law. 2 Company presentation January 2020

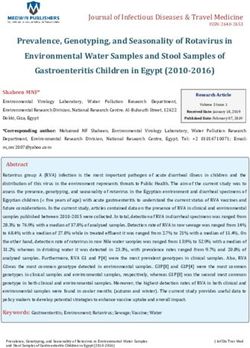
Past Commercial Success Associated with Innovation
Macrolides
Glycopeptides, Nitroimidazoles, Streptogramins
Cycloserine, Novobiocin
Pleuromutilins Rifamycins
Trimethoprim
Cephalosporins
Quinolones
Polymyxins, Phenicols
Fosfomycin
Nitrofurans Mupirocin
Tetracyclines
Carbapenems
Aminoglycosides, Bacitracin
Oxazolidinones
Monobactams
Sulfonamides Bedaquiline
Penicillin Lipopeptides
1920s 1930s 1940s 1950s 1960s 1970s 1980s 1990s 2000s 2010s
YEAR ANTIBIOTIC CLASS DISCOVERED
1920s-1980s Since 1990
• Multiple novel mechanisms & classes • Few new mechanisms; only
• Multiple examples of significant commercial incremental benefits
success • Niche market positioning with
• Ciprofloxacin; azithromycin; ceftriaxone low commercial return
• Resistance not clinical issue • Resistance is a clinical issue
3
Company presentation
January 2020
Adapted from ReAct Group 2015
The Summit Opportunity
LARGE INDICATIONS WITH
MEASURABLE UNMET NEEDS
C. difficile infection ~1 million cases Enterobacteriaceae >1 million Gonorrhea ~1.4 million cases per
per year in US and Europe cases per year in US year in US and Europe
NEW CLASSES OF ANTIBIOTICS WITH
DISTINCTIVE FEATURES AND BENEFITS
Targeted to infection/pathogen to work
in harmony with the microbiome
VALUE TO PATIENTS, PHYSICIANS AND PAYORS
DEMONSTRATED IN DEVELOPMENT
Economic outcomes data
Superiority clinical trials
gathered in clinical trials
4
Company presentation
January 2020
Our New Mechanism Antibiotic Pipeline
Discovery Preclinical Phase 1 Phase 2 Phase 3 Threat Status
CDI Urgent
(Ridinilazole)1 (CDC)
Enterobacteriaceae Urgent / High
(DDS-04 Series) (CDC / WHO)
Gonorrhea Urgent / High
(Target #1) (CDC / WHO)
ESKAPE Urgent / High
Program (CDC / WHO)
Gonorrhea Urgent / High
(Target #2) (CDC / WHO)
Discuva Platform
A portfolio created with assistance: BARDA, CARB-X, Innovate UK & Wellcome Trust
5
Company presentation 1. We own worldwide rights to ridinilazole, outside of certain Latin American countries and Caribbean islands.
January 2020About C. difficile Infection (CDI)
>1.0m cases Initial treatment Failure likely
per year in US fails to cure or connected to
and EU1, 29,000 sustain cures in impact on
deaths per year around a third microbiome of
in the US2 of cases standard of care
6
Company presentation 1. Decision Resources, 2015
2. New England Journal of Medicine, 2015
January 2020Importance of the Microbiome in CDI
BROAD-SPECTRUM
NO ANTIBIOTIC NO ANTIBIOTIC NO ANTIBIOTIC
ANTIBIOTIC
Normal Normal
microbiome microbiome
CDI
RISK
Microbiome
disrupted
Low CDI risk Low CDI risk
Patients being treated for CDI
7
Company presentation
Adapted from Rupnik et al., Nat. Rev. 2009
January 2020Increasing Risk of CDI Recurrence Associated with
Broad-Spectrum Treatments
Increasing Risk of Recurrence
Recurrent CDI associated with
increased microbiome damage
Mainstay therapies are broad-spectrum
1st antibiotics that drive microbiome damage
Risk: ~25%
Infection
2nd
Risk: ~45%
Infection
Each additional episode of CDI
associated with increased morbidity and
3rd
Infection
Risk: ~65% mortality and increased healthcare cost
0 20 40 60 80
Risk of Disease Recurrence (%)
8
Company presentation
January 2020 Source: Kelly, Clinical Microbiology & Infection, 2012Current CDI Treatments Damage the Gut Microbiome
ANTIBIOTIC MIC90 µg/mL
Bacteria Vancomycin Metronidazole Fidaxomicin
Bifidobacterium spp. 1 128 0.125
Eggerthella lenta 4 0.5 ≤0.03
Various Gram positive rods 4 2 128
Finegoldia magna 0.5 1 2
Peptostreptococcus anaerobius 0.5 1 ≤0.03
Staphylococcus aureus 1 >512 16
Enterococcus faecalis 4 >512 8
Enterococcus faecium 0.5 >512 128
Streptococcus spp. 1 >512 128
Bacteroides fragilis 64 2 >512
Bacteroides ovatus 256 2 >512
Bacteroides thetaiotaomicron 128 2 >512
Bacteroides vulgatus 128 1 >512
Parabacteroides spp. 128 2 >512
Fusobacterium nucleatum 512 0.25 >512
Fusobacterium spp. >512 0.5 >512
Prevotella spp. 512 1 >512
Veillonella spp. >512 2 256
Lactobacilus spp. >512 >512 >512
9
C. diff Foundation MIC90 value: the minimum concentration of the antibiotic at which 90% of the microbial activity is inhibited
November 6-7, 2019 Source: Goldstein et al: Antimicrob Agents Chemother. 2013Microbiome Plays an Important Role in Bile Salt Metabolism
(the Metabolome) to Protect Against C. difficile Infection
Liver
Gut
Gut microbiota-mediated bile salts transformation
Cholesterol
Conjugated bile Primary bile Secondary bile
salts salts salts
Bile salt hydrolase 7-Dehydroxylase
Taurocholate Taurocholate
Cholate Deoxycholate
Glycocholate Glycocholate
Glycine
Taurine
+
+
+ -
C. diff spore germination Vegetative cell growth
10
C. diff Foundation
Adapted from Ridlon et al., Gut Microbes 2016
November 6-7, 2019
and Winston and Theriot, Anaerobe, 2016Microbiome Damage Results in Imbalance of Bile Salts that
Favor C. difficile Growth
Liver
Gut
Cholesterol
Conjugated bile Primary bile Secondary bile
salts salts salts
Bile salt hydrolase
Taurocholate Taurocholate
Cholate Deoxycholate
Glycocholate Glycocholate
Glycine
Taurine
+ + -
+
C. diff spore germination Vegetative cell growth
11
C. diff Foundation
Adapted from Ridlon et al., Gut Microbes 2016
November 6-7, 2019
and Winston and Theriot, Anaerobe, 2016Ridinilazole Designed to be Patient-Friendly
Clear Phase 2 trial differentiation supports new standard of care potential
Cured CDI and sustained cures
over 40 days
60% reduction in recurrences, the key unmet need
Superiority over standard of care vancomycin in
sustained cures
Discharged from hospital earlier
Gut-friendly
Improved physical & mental Treatment preserved
effects of CDI compared to VAN
microbiome and allowed
Resolved diarrhea earlier good bacteria to recover
Significantly reduced pain/discomfort Well-tolerated, as
Significantly reduced anxiety/depression treatment targeted to gut
Initiated global Phase 3 clinical trials Feb. 2019
Expect top-line data H2 2021
With positive results, expect NDA filing 2022
12
Company presentation Source: CoDIFy Phase 2 clinical trial
January 2020Ridinilazole has a Highly Targeted Spectrum of Activity
ANTIBIOTIC MIC90 µg/mL
Bacteria Ridinilazole Vancomycin Metronidazole Fidaxomicin
Clostridium difficile 0.25 4 2 0.5
Bifidobacterium spp. >512 1 128 0.125
Eggerthella lenta >512 4 0.5 ≤0.03
Various Gram positive rods >512 4 2 128
Finegoldia magna 64 0.5 1 2
Peptostreptococcus anaerobius 64 0.5 1 ≤0.03
Staphylococcus aureus >512 1 >512 16
Enterococcus faecalis >512 4 >512 8
Enterococcus faecium 128 0.5 >512 128
Streptococcus spp. >512 1 >512 128
Bacteroides fragilis >512 64 2 >512
Bacteroides ovatus >512 256 2 >512
Bacteroides thetaiotaomicron >512 128 2 >512
Bacteroides vulgatus >512 128 1 >512
Parabacteroides spp. >512 128 2 >512
Fusobacterium nucleatum 64 512 0.25 >512
Fusobacterium spp. >512 >512 0.5 >512
Prevotella spp. >512 512 1 >512
Veillonella spp. >512 >512 2 256
Lactobacilus spp. >512 >512 >512 >512
13
Company presentation MIC90 value: the minimum concentration of the antibiotic at which 90% of the microbial activity is inhibited
January 2020 Source: Goldstein et al: Antimicrob Agents Chemother. 2013, 57: 4872–4876Ridinilazole Highly Preserving of Patients’ Microbiomes
Compared to Vancomycin in Phase 2 CoDIFy Trial
Cladograms Showing Changes in Relative Abundance of Microbiome Following 10 Days Dosing
RIDINILAZOLE VANCOMYCIN
C. difficile
C. difficile
Reduced relative abundance Increased relative abundance
14
Company presentation Source: Thorpe et al., PLOS ONE, 2018
January 2020Ridinilazole is Preserving of Patients’ Metabolome
in Phase 2 CoDIFy Trial
Following ridinilazole treatment, there is normalization of bile acid composition
Vancomycin Ridinilazole Healthy
100%
75%
Percentage
50%
25%
0%
D1 D10 D25 D40 D1 D10 D25 D40
Day
Primary Bile Acids Conjugated Primary BileAcids
Secondary Bile Acids Conjugated Secondary BileAcids
15
C. diff Foundation Source: X. Qian et al., ID Week 2019
November 6-7, 2019Ridinilazole: Similar Cure Rates to Vancomycin
in Phase 2 CoDIFy Trial
Cure at End of Treatment
Ridinilazole 77.8%
Vancomycin 69.7%
0 25 50 75 100
16
Company presentation Primary analysis conducted on the mITT group; n=36 in ridinilazole arm and n=33 in vancomycin arm
January 2020 Source: Vickers et al, Lancet ID, 2017Ridinilazole: Statistical Superiority Over Vancomycin in
Phase 2 CoDIFy Trial in Sustained Clinical Response (SCR)
Cure at End of Treatment Sustained Clinical Response (SCR)
Ridinilazole 77.8% 100
Vancomycin 69.7%
75
Δ 24.3
0 25 50 75 100
66.7%
50
Recurrence 30 Days Post Treatment
42.4%
25
Ridinilazole 14.3%
Vancomycin 34.8%
0
Vancomycin Ridinilazole
0 25 50 75 100
(90% CI 3.1–39.1)
17
Company presentation Primary analysis conducted on the mITT group; n=36 in ridinilazole arm and n=33 in vancomycin arm
January 2020 Source: Vickers et al, Lancet ID, 2017Short and Long-Term Improvements Seen in
Patient Quality of Life in Phase 2 CoDIFy Trial
• Patients’ quality of life assessed during the course of the study using the EQ-5D
• 5 domain questionnaire assessing patients’ welfare
EQ-5D-3L – Pain/Discomfort EQ-5D-3L – Anxiety/Depression
80 60
Reporting Problem (%)
Reporting Problem (%)
Proportion of Patients
Proportion of Patients
70 50
60
40
50
40 30
30
20
20
10
10
0 0
Baseline Day 5 Day 10 (EOT) Day 12 Day 40 Baseline Day 5 Day 10 (EOT)Day 12 (AOC) Day 40
(AOC)
Ridinilazole Vancomycin
18
C. diff Foundation
November 6-7, 2019
Source: S. Paul et al., ID Week 2019Ri-CoDIFy: Landmark Clinical Program
Aiming for clear differentiation to support switch from current therapies
SUPERIORITY TRIALS ECONOMIC DATA MICROBIOME
Aim to show Inclusion of health Comprehensive
ridinilazole is better economic measures analysis of impact of
than vancomycin at to support ridinilazole on the
sustaining patient commercialization microbiome
cures
Top line data expected in H2 2021
19
Company presentation
January 2020Phase 3 Clinical Trials Designed to
Evaluate Clinical and Economic Evidence
Group Design for Each Trial
Primary Endpoint
Group N Agent Regimen
• SCR to 30 days after end of therapy (EOT)
• Test for superiority (>95% power) 200mg
1 340 Ridinilazole
BID10 days
Important Secondary Endpoint 125mg
2 340 Vancomycin
QID 10 days
• Clinical cure at AOC
Screening Treatment Follow-Up
• Test for non-inferiority (90% power)
Ridinilazole
200 mg BID
//
Secondary & Exploratory Endpoints Vancomycin
125 mg QID
• SCR rates to 60 and 90 days post EOT //
• Impact on microbiome/metabolome D1 D10 D100
Randomisation EOT EOS
• Safety and tolerability
D12 (AOC): Key 2° Endpoint
Clinical Response at theAOC Visit
Health Economic Outcomes Endpoints
• Include readmission rates, length of hospital stay D40 (AOC): 1° Endpoint
SCR to 30 days post EOT
D70: 2° Endpoint
SCR to 60 days post EOT
Global Studies
• North & South America, Europe, Asia Pacific D100 (EOS): 2° Endpoint
SCR to 90 Days Post EOT
20
Company presentation
January 2020Phase 3 Clinical Trials Powered to
Test for Superiority in SCR
Primary endpoint: SCR Key secondary endpoint: clinical
Test for superiority; >95% power, 2- cure at assessment of cure
sided test, 5% significance level Test for non-inferiority; 90% power,
Assumes 55% SCR rate for 1-sided test, 2.5% significance level
vancomycin & a 15% improvement Established non-inferiority margin of
with ridinilazole 10%
Consistent trend on SCR to 60 and Assumes conservative 80% cure
90 days post end of treatment rate for vancomycin and ridinilazole
(EOT) required
21
Company presentation
January 2020Aiming for Dominant Position in Front-Line Treatment
Goal of Phase 3 clinical trials is to show clear benefits of ridinilazole
• A more effective treatment option
PATIENT • High cure rate with low recurrence
• Well tolerated with preservation of the microbiome
• A more effective treatment option
PHYSICIAN • Statistical superiority over vancomycin, the standard of care
• High cure rates with low recurrence
• Premium pricing supported by total cost of care savings
PAYOR • Fewer expensive recurrences
• Fewer readmissions help meet CMS targets ESTIMATED
SAVINGS OF
~$6,000
Compelling data to support potential switch to PER PATIENT
front-line use of ridinilazole IN THE US1
22 1 - Costs adjusted to 2023 pricing using US CPI for years to 2018 and assumed 2% inflation 2019-2023, based on NNT of 6.7
Company presentation associated with 15% recurrence delta and on front-line population per Lessa et al, 2015
January 2020About Enterobacteriaceae
Gram-negative More than 1m Approaching
family of bacteria, cases1 in US crisis, with
includes E. coli, K. across three growing cases of
pneumoniae infection sites: resistance to last
lung, bloodstream, resort antibiotics
urinary tract
23
Company presentation 1. Summit estimate based on Flores-Morales, 2015
January 2020DDS-04 Series: Targeting Enterobacteriaceae Infections
Potential to treat three major infection sites: bloodstream, lungs and urinary tract
DDS-04 series designed to Percent of resistant isolates
100
address unmet need
80
Enterobacteriaceae specific targeting through LolCDE
In vivo proof of concept established 60
Exposure observed across key infection sites in vivo
40
Low propensity for resistance
No cross resistance to other major antibiotic classes 20
Could replace reliance on antibiotics w/toxicity concerns
0
Discovered and optimized using Discuva Platform China Greece India Italy Russia Turkey US
E. coli carbapenem E. coli cephalosporin
Currently in lead optimization K. pneumoniae carbapenem K. pneumoniae cephalosporin
Healthcare Associated Infection EU Incidence US Incidence % Enterobacteriaceae
Pneumonia/LRT 861,000 250,000 27-30 a,b
Bloodstream 313,000 249,000 19-20 c,d
Urinary Tract 888,000 562,000 62-75 e-h
24 Sources: (a) Sader et al, JAC, 2018; (b) Cilloniz et al, Int J Mol Sci, 2016; (c) NHSN 2014; (d) Magill,
Company presentation NEJM, 2018; (e) Flores-Mireles et al, Nat Rev Microbiol, 2015; (f) Wagenlehner et al., WJU, 2012; (g)
January 2020 Magill et al, NEJM 2014; (h) Koningstein et al, PLOS One, 2014. CDDEP Resistance Map 2017.About Gonorrhea
1.4m cases in N. Gonorrhoeae Clinicians are
US & EU has consistently using the last CDC
78m worldwide1 developed recommended
resistance to treatment option;
known classes no new treatment
of antibiotics options available
25
Company presentation 1. World Health Organization, July 2017 press release
January 2020Potential Front-Line Treatment for Gonorrhea
Addressing the emergence of extensively- and multi-drug resistant gonorrhea
Countries
Resistance of
Designed to address the (%) reporting
Americas
gonococcal
SE Asia
resistance/
Europe
E Med.
isolates to
W Pac
unmet need
Africa
decreased
Total
antibiotics
susceptibility
Novel mechanism, targeted
Countries 9 16 3 27 6 16 77
spectrum
≥5% 1 0 0 15 4 6 26
Potent in vitro activity against over 51 (66%)
200 clinical isolates, including CeftriaxonePlanned Upcoming Milestones & Newsflow
2020 2021 2022
• H1 2020: planned • H1 2021: complete • 2022: with positive
Phase 3 sites active Phase 3 recruitment Phase 3 results,
• H2 2020: 50% • H2 2021: expect expect to file NDA
enrollment complete topline Phase 3 data for FDA approval of
in Phase 3 trials for ridinilazole ridinilazole
• 2020: pipeline
progress
27
Company presentation
January 2020Antibiotic Experience at Summit
David Roblin, MD, President of R&D
Previous antibiotic experience at Pfizer and Bayer
Richard Vickers, PhD, CSO
Discovered ridinilazole Brought
8 antibiotics
Dave Powell, PhD, SVP, Research to market
Previous antibiotic experience at GSK
Nawaz Khan, VP, Anti-infectives Discovery
Discovered SMT-571
Clive Mason, Senior Director, Platform Discovery
Discovered SMT-571
28
Company presentation
January 2020Summary Financials
Key Items Amount
Nasdaq Share Price (Jan. 7, 2020): $1.50
Issued Share Capital O/S(1): 67.2M
Market Cap (Jan. 7, 2020): $100M SYMBOL: SMMT
Cash Balance (Oct. 31, 2019)(2): $17.6M
Pro-Forma Cash Balance (Oct. 31, 2019)(3) $66.9M
Debt: $0
29 (1) Based on total Ordinary Shares outstanding; Ordinary Shares outstanding as of Dec. 31, 2019,
were 335.9 million; one ADS is equivalent to five Ordinary Shares
Company presentation
(2) Assumes an exchange rate of $1.2939 to £1.00
January 2020 (3) Pro forma figure includes net proceeds of $49.3 million related to Summit’s placement that closed
Dec. 24, 2019.Contact Details investors@summitplc.com Twitter: @summitplc 136a Eastern Avenue Milton Park Oxfordshire UK One Broadway Cambridge Massachusetts US 30 Company presentation January 2020
Avoidable Economic Burden
COST OF CDI
~$34,000 RECURRENCE OVER
ONE YEAR
~$40,000, 20231 2013 DATA
Rodrigues et al.
What if ALL front-line patients receive an agent that reduces recurrence by 15%?
Number
Needed to
Treat = 6.7
~$6,000 saving per treated patient2
US Healthcare
~$2.7B saving3 System, 2023
31
Company presentation 1 - Costs adjusted to 2023 pricing using US CPI for years to 2018 and assumed 2% inflation 2019-2023
January 2020 2 - Based on NNT of 6.7 associated with 15% recurrence delta; 3 – Based on front-line population per Lessa et al, 2015You can also read