COVID-19: Remdesivir for Adults - A Living Review - VA HSRD
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Evidence Synthesis Program
COVID-19: Remdesivir for
Adults – A Living Review
Supplemental Materials
updated August 2021
Prepared for: Authors:
Department of Veterans Affairs Timothy J. Wilt, MD, MPH
Veterans Health Administration Anjum S. Kaka, MD
Health Services Research & Development Service Rod MacDonald, MS
Eric Linskens, BS
Washington, DC 20420 Adam Obley, MD
Kathryn Vela, MLIS
Prepared by: Wei Duan-Porter, MD, PhD
Evidence Synthesis Program (ESP) Center
Minneapolis VA Health Care System
Minneapolis, MN
Timothy J. Wilt, MD, MPH, DirectorCOVID-19: Remdesivir for Adults (updated August 2021) Evidence Synthesis Program Supplemental Materials TABLE OF CONTENTS Supplemental Table 1. Search Strategies ........................................................................................ 1 Supplemental Table 2. GRADE Approach to Rating the Certainty of Evidence ........................... 1 Supplemental Table 3. Study Characteristics ................................................................................. 2 Supplemental Table 4. Outcomes A ............................................................................................... 7 Supplemental Table 5. Outcomes B.............................................................................................. 12 Supplemental Table 6. Viral Load ................................................................................................ 14 Supplemental Table 7. Harms A (based on number of subjects reporting at least 1 event) ......... 15 Supplemental Table 8. Harms B (based on number of subjects reporting at least 1 event) ......... 17 Supplemental Table 9. Risk of Bias – Randomized Controlled Trials ......................................... 19 Supplemental Table 10. COVID-19 Disease Severity .................................................................. 21 Supplemental References .............................................................................................................. 24 Supplemental Figure 1a: Mortality: All Studies (SIMPLE-2 with 5- and 10-day course): Absolute Effects............................................................................................................................. 25 Supplemental Figure 1b: Mortality by Initial Respiratory Status: Absolute Effects ..................... 26 Supplemental Figure 2a: Proportion of Patients Recovered: Absolute Effects ............................. 27 Supplemental Figure 2b: Need for Mechanical Ventilation: All Studies (SIMPLE-2 with 5- and 10-day course): Absolute Effects ............................................................................... 28 Supplemental Figure 2c: Patients With ≥1 Serious Adverse Event: Absolute Effects .................. 29 i
COVID-19: Remdesivir for Adults (updated August 2021) Evidence Synthesis Program
Supplemental Materials
SUPPLEMENTAL TABLE 1. SEARCH STRATEGIES
Source Strategy
MEDLINE and CENTRAL (Cochrane Central Trials 1. exp Coronavirus/ or exp Coronavirus
Register) Infections/
2. (nCoV or 2019-nCoV or ((new or novel or
wuhan) adj3 coronavirus) or covid19 or covid-
19 or SARS-CoV-2 or "Severe Acute
Respiratory Syndrome Coronavirus
2").ti,ab,kw.
3. 1 or 2
4. (remdesivir or Veklury or GS-5734).ti,ab,kw.
5. 3 and 4
WHO Database 1. remdesivir or Veklury or GS-5734
NIH COVID-19 iSearch Portfolio 1. remdesivir or Veklury or GS-5734
Title/Abstract fields only, medRxiv
Journal Tables of Contents (New England Journal of Keyword search: (remdesivir or Veklury or GS-
Medicine, JAMA Network, The Lancet) 5734)
Gilead Sciences, Inc. https://www.gilead.com/science-
and-medicine/research
SUPPLEMENTAL TABLE 2. GRADE APPROACH TO RATING
THE CERTAINTY OF EVIDENCE
The GRADE approach to rating the certainty of evidence for randomized controlled trials is
based on five reasons to possibly rate down the quality of evidence.1
Reason Consequence
Limitations in study design or execution (risk of bias) ↓ 1 or 2 levels
Inconsistency of results ↓ 1 or 2 levels
Indirectness of evidence ↓ 1 or 2 levels
Imprecision ↓ 1 or 2 levels
Publication bias ↓ 1 or 2 levels
1COVID-19: Remdesivir for Adults (updated August 2021) Evidence Synthesis Program
Supplemental Materials
SUPPLEMENTAL TABLE 3. STUDY CHARACTERISTICS
Intervention
Author, Year Country
Comparator
Funding Demographics
Inclusion/exclusion criteria
Risk of Bias
Study Period/Length of Follow-up
Beigel 20202 Intervention: Remdesivir (n=541) 200 mg on day 1 followed by N=1062
Adaptive Covid-19 Treatment Trial 100 mg on days 2–10 (or until hospital discharge or death) in Age (years, mean): 59
(ACTT-1) single daily infusions Gender (male): 64%
Race/Ethnicity:
Multinational (60 sites and 13 Comparator: Placebo (n=521) White 53%
subsites, 45 in the US) Black/African American 21%
Inclusion criteria: 18 years or older and meeting one of the Asian 13%
Design: RCT following criteria suggestive of lower respiratory tract infection at Latino (of any race) 23%
enrollment: radiographic infiltrates by imaging study, peripheral
Funding: Primarily government, oxygen saturation (SpO2) ≤94% on room air, or requiring Time from symptom onset to randomization
other supplemental oxygen, mechanical ventilation, or ECMO; no limit Overall, median [IQR] 9 days [6-12]
to duration of symptoms prior to enrollment; laboratory- Remdesivir median [IQR] 9 days [6-12]
Risk of Bias: Low confirmed SARS-CoV-2 infection as determined by a positive Placebo median [IQR] 9 days [7-13]
RT-PCR assay result from any respiratory specimen collected
5 times the upper limit of the
normal range, impaired renal function as determined by
calculating an eGFR or need for hemodialysis or hemofiltration,
allergy to study product, pregnancy or breast-feeding, and
anticipated discharge from hospital or transfer to another
hospital within 72 hours of enrollment
Study Period/Length of Follow-up: 29 days
Wang 2020 3
Intervention: Remdesivir (n=158; 2:1 ratio) 200 mg on day 1 N=237
China followed by 100 mg on days 2–10 in single daily infusions Age (years, median):
Remdesivir 66
Design: RCT Comparator: Placebo (n=79) Placebo 64
2COVID-19: Remdesivir for Adults (updated August 2021) Evidence Synthesis Program
Supplemental Materials
Intervention
Author, Year Country
Comparator
Funding Demographics
Inclusion/exclusion criteria
Risk of Bias
Study Period/Length of Follow-up
Gender (male):
Funding: Government, other Inclusion criteria: men and non-pregnant women with COVID- Remdesivir 56%
19, age at least 18 years, RT-PCR positive for SARS-CoV-2, Placebo 65%
Risk of Bias: Low pneumonia confirmed by chest imaging, oxygen saturation of Race: East Asian
94% or lower on room air or a ratio of arterial oxygen partial
pressure to fractional inspired oxygen of 300 mm Hg or less, Time from symptom onset to drug
within 12 days of symptom onset Remdesivir median [IQR] 11 days [9-12]
Placebo median [IQR] 10 days [9-12]
Exclusion criteria: pregnancy or breast feeding; hepatic
cirrhosis; ALT or AST >5 times the upper limit of the normal Oxygen status on admission:
range; known severe renal impairment (estimated eGFRCOVID-19: Remdesivir for Adults (updated August 2021) Evidence Synthesis Program
Supplemental Materials
Intervention
Author, Year Country
Comparator
Funding Demographics
Inclusion/exclusion criteria
Risk of Bias
Study Period/Length of Follow-up
radiographic evidence of pulmonary infiltrates and peripheral Asian 11%
Funding: Industry capillary oxygen saturation (SpO2) ≤ 94% or requiring Other 7%
supplemental oxygen at screening
Risk of Bias: Moderate Time from symptom onset to drug
Exclusion criteria: Pregnant or women who were breast feeding Remdesivir 5-day median [IQR] 8 days [5-11]
infants, ALT or AST >5 times the upper limit of the normal Remdesivir 10-day median [IQR] 9 days [6-12]
range, creatinine clearance < 50 mL/min using the Cockcroft-
Gault formula for participants ≥ 18 years of age and Schwartz Oxygen status on admission:
Formula for participants < 18 years of age; mechanically Percent on no oxygen 14%
ventilated (including V-V ECMO) ≥ 5 days, or any duration of V- Percent on supplemental oxygen 55%
A ECMO; evidence of multiorgan failure; concurrent treatment Percent on non-invasive ventilation 27%
with other agents with actual or possible direct acting antiviral Percent on invasive ventilation 4%
activity against SARS-CoV-2 < 24 hours prior to study drug
dosing; participant in any other clinical trial of an experimental
treatment for COVID-19
Study Period/Length of Follow-up: 14 days (up to 30 days for
adverse events)
Spinner 20205 Intervention 1: Remdesivir, 5-day course (n=199) 200 mg on N=596 randomized (584 analyzed)
GS-US-540-5774 day 1 followed by 100 mg on days 2–5 in single daily infusions Age (years, median):
SIMPLE 2 5-day group 58
Intervention 2: Remdesivir, 10-day course (n=197) 200 mg on 10-day group 56
105 sites in the US, France, day 1 followed by 100 mg on days 2–10 in single daily infusions Standard care 57
Germany, Hong Kong, Italy, Gender (male): 61%
Republic of Korea, The Netherlands, Comparator: Standard care (n=200) Race:
Singapore, Spain, Switzerland, White 58%
Taiwan and the United Kingdom Inclusion criteria: ≥ 18 years (at all sites), or aged ≥ 12 and < 18 Black 18%
years of age weighing ≥ 40 kg (where permitted according to Asian 18%
Design: Randomized, open-label, local law and approved by relevant review boards) currently Other 7%
multi-center Phase 3 clinical trial hospitalized and requiring medical care for COVID-19; SARS- Latino (of any race) 18%
CoV-2 infection confirmed by PCR test ≤ 4 days before
Funding: Industry randomization; moderate COVID-19 pneumonia (peripheral Time from symptom onset to drug
capillary oxygen saturation (SpO2) >94% on room air Remdesivir 5-day median [IQR] 8 days [5-11]
Risk of Bias: Low radiographic evidence of pulmonary infiltrates) Remdesivir 10-day median [IQR] 8 days [5-11]
4COVID-19: Remdesivir for Adults (updated August 2021) Evidence Synthesis Program
Supplemental Materials
Intervention
Author, Year Country
Comparator
Funding Demographics
Inclusion/exclusion criteria
Risk of Bias
Study Period/Length of Follow-up
Exclusion criteria: Women who were pregnant or breast feeding Oxygen status on admission:
infants, ALT or AST >5 times the upper limit of the normal Percent on no oxygen: 84%
range; creatinine clearance < 50 mL/min using the Cockcroft- Percent on supplemental oxygen: 15%
Gault formula for participants ≥ 18 years of age and Schwartz Percent on non-invasive ventilation: NA
Formula for participants < 18 years of age; mechanically Percent on invasive ventilation: NA
ventilated at screening; concurrent treatment or planned
concurrent treatment with other agents with actual or possible
direct acting antiviral activity against SARS-CoV-2; participation
in any other clinical trial of an experimental treatment for
COVID-19
Study Period/Length of Follow-up: 11 days (primary
outcome); final assessment on day 28
WHO Solidarity 20206 Intervention: Remdesivir, intravenous, (n=2750), 200 mg on day N=5475 randomized (5451 analyzed)
0 followed by 100 mg on days 1-9 (treatment stopped at Age (years):
30 countries: Europe (13), Canada, discharge or death)COVID-19: Remdesivir for Adults (updated August 2021) Evidence Synthesis Program
Supplemental Materials
Intervention
Author, Year Country
Comparator
Funding Demographics
Inclusion/exclusion criteria
Risk of Bias
Study Period/Length of Follow-up
Norway Gender (male): 73%
Comparator: No study drug (local standard of care) (n=58 Race: NR
Design: Open-label randomized trial allocated versus remdesivir, 87 total in full analysis set)
Time from symptom onset to drug: mean 7
Funding: National Clinical Therapy Inclusion criteria: (see WHO Solidarity) days
Research in the Specialist Health
Services, Norway Exclusion criteria: severe comorbid conditions Oxygen status on admission: NR
with life expectancy 470 ms, pregnancy,
breastfeeding, acute occurrence of a comorbid condition in a 7-
day period before inclusion, known intolerance to study drugs,
participation in a potentially confounding trial, or concomitant
medications interfering with the study drugs.
Mahajan 20218 Intervention: Remdesivir, intravenous, (n=41) 200 mg on day 1 N=82 randomized (70 analyzed)
followed by 100 mg once daily on days 2-5. Both treatment Age (years): 58
India groups continued supportive therapy Gender (male): 66%
Race: NR
Design: Open-label randomized trial Comparator: No study drug (local standard of care) (n=41)
Time from symptom onset to drug: mean 7
Funding: No funders Inclusion criteria: 18 to 60 years of age hospitalized with a days
diagnosis of COVID-19 by PCR, radiographic evidence of
Risk of Bias: High pneumonia, respiratory rate >24/min, oxygen saturation ≤94%, Oxygen status on admission:
creatine clearance >40 mL/min Percent on no oxygen: 0%
Percent on low-flow oxygen: 76%
Exclusion criteria: receiving mechanical ventilation, multi organ Percent on high-flow oxygen /non-invasive
failure, AST/ALT >3 times the upper limit of normal ventilation: 24%
Percent on invasive mechanical ventilation: 0%
Study Period/Length of Follow-up: 24 days or until discharge
or death
Abbreviations. ALT = alanine aminotransferase; AST = aspartate aminotransferase; ECMO = extracorporeal membrane oxygenation; eGFR = estimated glomerular filtration
rate; IQR = interquartile range; RT-PCR = reverse transcription, polymerase-chain-reaction; SARS-CoV = Severe Acute Respiratory Syndrome Coronavirus-2 infection
6COVID-19: Remdesivir for Adults (updated August 2021) Evidence Synthesis Program
Supplemental Materials
SUPPLEMENTAL TABLE 4. OUTCOMES A
Recovery or
Length of hospital stay Time to recovery Mortality Combined endpoint
Author, Year “Clinical Improvement”
Remdesivir Placebo Remdesivir Placebo Remdesivir Placebo Remdesivir Placebo
Beigel 2020 2
Median Median Median Median 14-day 14-day Day 29 Day 29
ACTT-1 [IQR] [IQR] [95% CI] [95% CI] 6.5% 11.7% Recovery a Recovery a
12 [6 to 28] 17 [8 to 28] 10 days 15 days (35/541) (61/521) 73.8% 67.6%
[9 to 11] [13 to 18] (399/541) (352/521)
Difference HR 0.55 [95%
-5.0 days [95% CI, 0.36 to Recovery Rate
CI, -7.7 to -2.3] 0.83] Ratio 1.29
(through day [95% CI, 1.12
Median [IQR] 15) to 1.49]
for those who Median [IQR]
did not die for those who 29-day 29-day Recovery
10 [5 to 21] did not die 10.9% 14.8% Mild/mod. Recovery
14 [7 to 27] (59/541) (77/521) Disease b Mild/mod.
Difference 98.2% (54/55) Disease b
-4.0 days [95% HR 0.73 [95% 92.0% (46/50)
CI, -6.0 to -2.0] CI, 0.52 to Severe
1.03] Disease c Severe
71.0% Disease c
(345/486) 65.0%
(306/471)
Wang 20203 Median [IQR] Median [IQR] Time to Clinical Time to Clinical 28-day 28-day Day 28 Day 28
25 days 24 days Improvement Improvement Clinical Clinical
[16 to 38] [18 to 36] Median [IQR] Median [IQR] 13.9% 12.8% improvement d improvement d
21 days 23 days (22/158) (10/78) 65.2% 57.7%
Difference [13 to 28] [15 to 28] (103/158) (45/78)
0.0 days ARD 1.1%
[95% CI, -4.0 [95% CI, -8.1 ARD 7.5%
to 4.0] to 10.3] [95% CI, -5.7
to 20.7]
HR 1·23
[95% CI, 0·87
to 1·75]
7COVID-19: Remdesivir for Adults (updated August 2021) Evidence Synthesis Program
Supplemental Materials
Goldman Remdesivir Remdesivir Remdesivir Remdesivir Remdesivir Remdesivir Remdesivir Remdesivir
20204 5-day 10-day 5-day 10-day 5-day 10-day 5-day 10-day
GS-US-540- NR NR Median [IQR] Median [IQR] 14-day 14-day Day 14 Day 14
5773 10 days 11 days Clinical Clinical
SIMPLE 1 [6 to 18] [7 to not 8.0% 10.7% (21/197) recovery e recovery e
possible to (16/200) 64.5% 53.8%
HR 0.81 estimate] P=.70 (129/200) (106/197)
[95% CI, 0.64 Baseline-
to 1.04] adjusted ARD
and p-value
-6.3%
[95% CI,
-15.4 to 2.8];
P=.17
Clinical
Clinical (≥2-point)
(≥2-point) improvement f
improvement f 54.3%
64.5% (107/197)
(129/200)
Baseline-
adjusted ARD
and P-value
-6.5%
[95% CI, -15.7
to 2.8]; P=.16
8COVID-19: Remdesivir for Adults (updated August 2021) Evidence Synthesis Program
Supplemental Materials
Spinner 20205 Remdesivir Standard Care Remdesivir Standard Care Remdesivir Standard Care Remdesivir Standard Care
GS-US-540-
5774 NR NR Median [IQR] Median [IQR] 11-day 11-day Day 11 Day 11
SIMPLE 2 with 5 day 7 (4-14) Recovery e Recovery e
standard care 6 (5-10) 5-day 2.0% (4/200) 5-day 64.0%
0% (0/191) 73.8% (128/200)
10 day 10-day (141/191)
8 (4-13) 1.0% (2/193) 10-day
HR for 5-day 68.4%
vs. standard (132/193)
care HR for 5-day
0.51 [95% CI, vs. standard
0.09 to 2.80] care
HR for 10-day 1.18 [95% CI,
vs. standard 0.96 to 1.45]
care HR for 10-day
0.76 [95% CI, vs. standard
0.17 to 3.40] care
1.11 [95% CI,
0.90 to 1.36]
Clinical Clinical
(≥2-point) (≥2-point)
improvement f improvement f
5-day 60.5%
70.2% (121/200)
(134/191)
10-day
65.3%
(126/193)
HR for 5-day
vs. standard
care
1.15 [95% CI,
0.93 to 1.42]
HR for 10-day
vs. standard
care
1.16 [95% CI,
0.93 to 1.43]
9COVID-19: Remdesivir for Adults (updated August 2021) Evidence Synthesis Program
Supplemental Materials
WHO Solidarity Remdesivir Standard Care Remdesivir Standard Care Remdesivir Standard Care Remdesivir Standard Care
20206
Still Still NR NR 12.5% 12.7% NR NR
hospitalized at hospitalized at (301/2743) (303/2708)
day 7 day 7
69% 59% Rate Ratio:
0.95 [95% CI,
0.81 to 1.11]
NOR-Solidarity NR NR NR NR In-hospital In-hospital NR NR
20217 7.1% 7.0%
Sub-study of RR 1.0 [95%
WHO Solidarity CI, 0.2 to 4.6]
HR 1.0 [95%
CI, 0.4 to 2.9]
28 day 28 day
2.4% 5.3%
Estimated
Marginal Risk
Difference vs
SC
-2.9% [95% CI,
-10.3 to 4.5]
60 day 60 day
7.1% 5.3%
Estimated
Marginal Risk
Difference vs
SC
1.9% [95% CI,
-7.8 to 11.6]
10COVID-19: Remdesivir for Adults (updated August 2021) Evidence Synthesis Program
Supplemental Materials
Mahajan 20218 NR NR Patients in the remdesivir group All patients All patients NR NR
and standard of care group had 14.6% (6/41) 12.2% (5/41)
an equal time to recovery
between 10 and 20 days (no Per protocol Per Protocol
other data reported) Day 12-24 Day 12-24
14.7% 8.3%
(5/34) (3/36)
Abbreviations. ARD = absolute risk difference; CI =confidence intervals; HR = Hazard ratio; IQR = interquartile range; NR = not reported; RR = relative risk; SC = standard
care
a Defined by either discharge from the hospital or hospitalization extended for purposes of infection-control only with no medical needs.
b Mild/moderate disease was defined by a SpO2 >94% and respiratory rateCOVID-19: Remdesivir for Adults (updated August 2021) Evidence Synthesis Program
Supplemental Materials
SUPPLEMENTAL TABLE 5. OUTCOMES B
Required invasive mechanical ventilation;
Required oxygen;
Duration of invasive mechanical ventilation,
Author, Year Duration of oxygen support, days
days
Remdesivir Placebo Remdesivir Placebo
Beigel 2020 2
17.6% (95/541) at Day 23.2% (121/521) at Day 10.7% (58/541) at 11.5% (60/521) at
ACTT-1 15 visit; 15 visit; Day 15 visit: Day 15 visit;
Length of use if Length of use if receiving Length of use if Length of use if
receiving at baseline, at baseline, receiving at baseline, receiving at baseline,
Median [IQR] Median [IQR] Median [IQR] Median [IQR]
17 days [9 to 28] 20 days [8 to 28] 13 days [5 to 28] 21 days [8 to 28]
Difference Difference
-3.0 days -8.0 days
[95% CI, -9.3 to 3.3] [95% CI, -11.8 to
-4.2]
Length of new use
during study, Length of new use during Length of new use Length of new use
Median [IQR] study, during study, during study,
21.5 days [9 to 28] Median [IQR] Median [IQR] Median [IQR]
Difference 23 days [12 to 28] 4 days [2 to 12] 5.5 days [1 to 15]
1.0 days Difference
[95% CI, -6.0 to 8.0] -1.0 days
[95% CI, -7.6 to 5.6]
Wang 20203 8.2% (13/158) 12.8% (10/78) Median [IQR] Median [IQR]
Median [IQR] Median [IQR] 19.0 days 21.0 days
7.0 days 15.5 days [11 to 30] [14 to 30.5]
[4 to 16] [6 to 21]
Difference Difference
-4.0 days -2.0 days
[95% CI, -14.0 to 2.0] [95% CI, -6.0 to 1.0]
Goldman 20204 Remdesivir Remdesivir Remdesivir Remdesivir
GS-US-540-5773 5-day 10-day 5-day 10-day
SIMPLE 1 8.0% (16/200); 16.8% (33/197); Duration NR NR
Duration NR NR
Spinner 20205 Remdesivir Standard Care Remdesivir Standard Care
GS-US-540-5774 5-day 2.0% (4/200) Time to Room Air 6 (4-14)
SIMPLE 2 with 0% (0/191) Median [IQR]
standard care 5-day
10-day 5 (3-7)
0.5% (1/193) 10-day
4 (2-6)
6.3% (12/191) and 11% (22/200)
6.7% (13/193) required oxygen
required oxygen support on Day 1
support on Day 1
WHO Solidarity Remdesivir Standard Care Remdesivir Standard Care
20206 Initiation of ventilation Initiation of ventilation in NR NR
in those not already those not already
ventilated ventilated
11.9% (295/2489) 11.5% (284/2475)
12COVID-19: Remdesivir for Adults (updated August 2021) Evidence Synthesis Program
Supplemental Materials
NOR-Solidarity 9.5% 7.0% NR NR
20217 Estimated Marginal
Sub-study of WHO Risk
Solidarity Difference vs SC
2.5% [95% CI, -8.6 to
13.6]
Mahajan 20218 Day 12-24 Day 12-24 Day 12-24 Day 12-24
11.8% 5.6% Supplemental O2 Supplemental O2
(4/34) (2/36) 11.8% 16.7%
(4/34) (6/36)
Day 12-24 Day 12-24
High-flow O2 or/ High-flow O2 or/
non-invasive non-invasive
ventilation ventilation
55.9% 61.1%
(19/34) (22/36)
Abbreviations. ECMO = extracorporeal membrane oxygenation; IQR = interquartile range; NR = not reported; SC = standard care
13COVID-19: Remdesivir for Adults (updated August 2021) Evidence Synthesis Program
Supplemental Materials
SUPPLEMENTAL TABLE 6. VIRAL LOAD
Author, Year Pre Post
Viral load definition Remdesivir Placebo Remdesivir Placebo
Beigel 20202 NR NR NR NR
ACTT-1
Wang 20203 4.7 log10 copies/mL 4.7 log10 NR NR
Mean baseline viral load of nasopharyngeal copies per mL
and oropharyngeal swabs
Upper respiratory tract Estimated from graph Estimated from graph Estimated from graph Estimated from graph
specimens 3.7 log10 copies/mL 3.6 log10 copies/mL 0.6 log10 copies/mL 0.1 log10 copies/mL
Lower respiratory tract Estimated from graph Estimated from graph Estimated from graph Estimated from graph
specimens 7.3 log10 copies/mL 6.4 log10 copies/mL 1.4 log10 copies/mL 0.0 log10 copies/mL
Goldman 20204 Remdesivir Remdesivir Remdesivir Remdesivir
GS-US-540-5773 5-day 10-day 5-day 10-day
SIMPLE 1 NR NR NR NR
Spinner 20205 Remdesivir Standard Care Remdesivir Standard Care
GS-US-540-5774 NR NR NR NR
SIMPLE 2 with standard care
WHO Solidarity 20206 Remdesivir Standard Care Remdesivir Standard Care
NR NR NR NR
NOR-Solidarity 20217 1.6 (1.6) 2.3 (1.8) Difference in viral level at day 10,
Sub-study of WHO Solidarity log10 copies/1000 cells log10 copies/1000 cells 0.203 log10 copies/1000 cells
oropharynx [95% CI, -0.348 to 0.754]
Difference in daily viral decrease rate,
0.113 log10 copies/1000 cells
[95% CI, -0.001 to 0.227]
Mahajan 20218 NR NR NR NR
Abbreviations. NR = not reported
14COVID-19: Remdesivir for Adults (updated August 2021) Evidence Synthesis Program
Supplemental Materials
SUPPLEMENTAL TABLE 7. HARMS A (BASED ON NUMBER OF SUBJECTS REPORTING
AT LEAST 1 EVENT)
Author, Year Serious AE AE leading to drug withdrawal Any AE
Remdesivir Placebo Remdesivir Placebo Remdesivir Placebo
Beigel 20202 ACTT-1 24.6% 31.6% 10.7% 14.9% 57.3% (305/532) a
62.6% (323/516)a
(131/532) a (163/516) a (57/532) a (77/516) a
Study-related Study-related
2 events 3 events
Grade 3 or 4 Grade 3 or 4
51.3% (273/532) 57.2% (295/516)
Wang 20203 18.1% 25.6% 11.6% 5.1% 65.8% 64.1%
(28/155) (20/78) (18/155) (4/78) (102/155) (50/78)
Grade 3 or 4 Grade 3 or 4 Grade 3 or 4 Grade 3 or 4
5.8% (9/155) 12.8% (10/78) 8.4% (13/155) 14.1% (11/78)
Goldman 20204 Remdesivir Remdesivir Remdesivir Remdesivir Remdesivir Remdesivir
GS-US-540-5773 5-day 10-day 5-day 10-day 5-day 10-day
SIMPLE 1 21.0% (42/200) 34.5% (68/197) 4.5% 10.2% 70.5% 73.6%
(9/200) (20/197) (141/200) (145/197)
P=.07 P=.86
Grade ≥3 Grade ≥3
30% (60/200) 43% (85/197)
Spinner 20205 Remdesivir Standard Care Remdesivir Standard Care Remdesivir Standard Care
GS-US-540-5774
5-day 9.0% (18/200) 5-day NA 5-day 45.0% (90/200)
SIMPLE 2 with standard
4.7% (9/191) 2.1% (4/191) 51.3% (98/191)
care
10-day 10-day 10-day
5.2% (10/193) 4.1% (8/193) 58.5% (106/193)
Grade ≥3 Grade ≥3
5-day 12.0% (24/200)
10.5% (20/191)
15COVID-19: Remdesivir for Adults (updated August 2021) Evidence Synthesis Program
Supplemental Materials
10-day
10.9% (21/193)
WHO Solidarity 20206 Remdesivir Standard Care Remdesivir Standard Care Remdesivir Standard Care
NR NR NR NR NR NR
NOR-Solidarity 20217 19.0% (8/42) 14.9% (13/87) 0% (0/42) 0% (0/87) 38.5% (20/42) 25.3% (22/87)
Sub-study of WHO
Solidarity
Mahajan 20218 NR NR 7.3% (3/41) due to 0/41 NR NR
abnormal ALT and
AST values
Abbreviations. AE = adverse event; ALT = alanine aminotransferase; AST = aspartate aminotransferase; NR = not reported
a Data for the treated population
16COVID-19: Remdesivir for Adults (updated August 2021) Evidence Synthesis Program
Supplemental Materials
SUPPLEMENTAL TABLE 8. HARMS B (BASED ON NUMBER OF SUBJECTS REPORTING
AT LEAST 1 EVENT)
Respiratory failure or acute respiratory distress
Cardiopulmonary failure
Author, Year syndrome
Remdesivir Placebo Remdesivir Placebo
Beigel 2020 2
Serious respiratory failure Serious respiratory failure NR NR
ACTT-1 7.3% 8.0%
(39/532) a (66/516) a
Respiratory distress Respiratory distress
1.1% (6/532) a 2.1% (11/516) a
Wang 20203 Respiratory failure or acute Respiratory failure or acute 5.2% 9.0%
respiratory distress respiratory distress (8/155) (7/78)
syndrome syndrome
10.3% 7.7%
(16/155) (6/78)
Grade 3 or 4 Grade 3 or 4
2.6% (4/155) 5.1% (4/78)
Goldman 20204 Remdesivir Remdesivir Remdesivir Remdesivir
GS-US-540-5773 5-day 10-day 5-day 10-day
SIMPLE 1 6.0% 10.7% NR NR
(12/200) (21/197)
Spinner 20205 Remdesivir Standard Care Remdesivir Standard Care
GS-US-540-5774 NR NR NR NR
SIMPLE 2 with standard care
WHO Solidarity 20206 Remdesivir Standard Care Remdesivir Standard Care
NR NR NR NR
NOR-Solidarity 20217 NR. Study authors note “Most other serious adverse NR NR
Sub-study of WHO Solidarity events were related to respiratory failure and interpreted
as attributable to disease progression”
Serious respiratory, thoracic, and mediastinal disorders:
Remdesivir 11.9% (5/42)
Standard care 6.9% (6/87)
17COVID-19: Remdesivir for Adults (updated August 2021) Evidence Synthesis Program Supplemental Materials Mahajan 20218 NR NR NR NR Abbreviations. AE = adverse event; NR = not reported a Data for the treated population 18
COVID-19: Remdesivir for Adults (updated August 2021) Evidence Synthesis Program
Supplemental Materials
SUPPLEMENTAL TABLE 9. RISK OF BIAS – RANDOMIZED CONTROLLED TRIALS
Author, Year Random sequence Allocation Blindinga Incomplete Selective outcome Overall Risk of Biasd
generation concealment outcome datab reportingc
Beigel 20202 Low, adequate, Low, adequate, Low, patient, Low, 1 placebo No Low
ACTT-1 permuted web-based provider patient and 3
randomization remdesivir patients
sequence Follow-up safety excluded due to no
and efficacy data after baseline.
evaluations
performed by
blinded clinic staff
Wang 20203 Low, adequate, Low, adequate, Low, patient, Low, 1 placebo No Low
permuted centralized provider patient withdrew
Note: trial block randomization consent, not in ITT
stopped early sequence analyses.
Three remdesivir
patients did not
take drug and are
not in the safety
analyses.
Goldman 20204 Low, adequate, Low, adequate, Open-label Low,2 patients in No Moderate based on
GS-US-540- computer generated web-based the 5-day group imbalance between
5773 Outcome assessors and 3 in the 10-day groups (patients
SIMPLE 1 were not blinded. group not included randomly assigned to
in analyses the 10-day group had
(withdrawn or significantly worse
randomized in clinical status than
error) those assigned to the
5-day group (P =
0.02)) and open label
nature of study.
Spinner 20205 Low, adequate, Low, adequate, Open-label Low, 8 patients in No Low
GS-US-540- computer generated web-based the 5-day group
5774 Outcome assessors and 4 in the 10-day
SIMPLE 2 with were not blinded. group not included
standard care in analyses (did not
start treatment)
19COVID-19: Remdesivir for Adults (updated August 2021) Evidence Synthesis Program
Supplemental Materials
Author, Year Random sequence Allocation Blindinga Incomplete Selective outcome Overall Risk of Biasd
generation concealment outcome datab reportingc
WHO Solidarity WHO: Unclear, not WHO: Low, WHO and NOR- WHO: Low, 7 WHO: Yes – limited Moderate based on
20206 reported; adequate, cloud- Solidarity: patients in reporting of unclear sequence
(NOR-Solidarity based; Open-label remdesivir and 17 hospitalization generation and
– sub-study)7 NOR-Solidarity: Low, patients in control duration; no selective outcomes
computer NOR-Solidarity: Blinded analyses of group not included adverse event reporting
randomization Low, allocation all relevant in analyses (no or reporting
procedures sequence was data uncertain consent
prepared by an to follow-up) NOR-Solidarity: No,
independent all outcomes were
statistician NOR-Solidarity: 2% reported
patients not
included in full
analysis set, 18%
did not complete 3-
month follow-up
Mahajan 20218 Low, adequate, Unclear, not Open-label High, 8 patients in No High based on not
computer generated reported remdesivir and 5 using ITT analysis,
patients in control attrition, and absence
group not included of information on
in analyses allocation
(Patients who were concealment
discharged when
symptom-free,
withdrawn from
treatment, for had
treatment stopped
due to elevated
ALT or AST levels
were excluded).
16% were excluded
from analyses
Abbreviations. ALT = alanine aminotransferase; AST = aspartate aminotransferase; ITT = intent-to-treat
a For the open-label trial, blinding of study participants and study personnel was not feasible. This element was not considered in rating overall risk of bias.
b Incomplete outcome data was rated high if more than 10% of participants randomized were not included in the analyses.
c Selective reporting was determined by comparing reported outcomes with outcomes specified in the Methods section. If a protocol paper was available, reported
outcomes were compared with outcomes specified in the protocol.
d Studies were rated low risk of bias if at least 3 elements were rated low and no additional elements were rated high. Studies were rated High risk of bias if at least 2
elements were rated high risk of bias. All other studies were rated Moderate risk of bias.
20COVID-19: Remdesivir for Adults (updated August 2021) Evidence Synthesis Program
Supplemental Materials
SUPPLEMENTAL TABLE 10. COVID-19 DISEASE SEVERITY
COVID-19 NIH COVID-19 WHO Clinical Management Food and Drug Administration (FDA)11 Included Studies in
Disease Treatment Guidelines9 of COVID-1910 Evidence Report
Severity
Asymptomatic Individuals who test NA Positive testing by standard reverse NA
or Pre- positive for SARS-CoV- transcription polymerase chain reaction (RT-
symptomatic 2 by virologic testing PCR) assay or equivalent test; no symptoms.
using a molecular
diagnostic (eg,
polymerase chain
reaction) or antigen test,
but have no symptoms.
Mild Individuals who have Symptomatic patients Positive testing by standard RT-PCR assay or ACTT-12: Mild/Moderate
any of the various signs meeting the case definition equivalent test; symptoms of mild illness with disease: confirmed COVID-19
and symptoms of for COVID-19 without COVID-19 that could include fever, cough, positive and hospitalized with
COVID 19 (eg, fever, evidence of viral pneumonia sore throat, malaise, headache, muscle pain, radiographic infiltrates by
cough, sore throat, or hypoxia. gastrointestinal symptoms, without shortness imaging, SpO2 >94% and
malaise, headache, of breath or dyspnea; no clinical signs respiratory rate 94% and
of oxygen (SpO2) ≥94% SpO2 ≥90% on room air OR of moderate illness with COVID-19, such as respiratory rate 93% on room air supplemental oxygen.
(cough or difficulty breathing at sea level, heart rate ≥90 beats per minute; Moderate not further defined.
+ fast breathing and/or chest no clinical signs indicative of Severe or Critical Results for Moderate not
indrawing) and no signs of Illness provided.
severe pneumonia.
SIMPLE 25: Moderate
disease: confirmed COVID-19
positive and hospitalized with
21COVID-19: Remdesivir for Adults (updated August 2021) Evidence Synthesis Program
Supplemental Materials
COVID-19 NIH COVID-19 WHO Clinical Management Food and Drug Administration (FDA)11 Included Studies in
Disease Treatment Guidelines9 of COVID-1910 Evidence Report
Severity
radiographic evidence of
pulmonary infiltrates and
oxygen saturation >94% on
room air.
WHO6: Not defined as
“moderate” but SOLIDARITY
included and provided
mortality data for hospitalized
patients without supplemental
oxygen on study entry.
Severe Individuals who have Adolescent or adult with Positive testing by standard RT-PCR assay or Wang3, ACTT-12, SIMPLE-14,
respiratory frequency clinical signs of pneumonia an equivalent test; symptoms suggestive of Mahajan8: Hospitalized
>30 breaths per minute, (fever, cough, dyspnoea, fast severe systemic illness with COVID-19, which patients meeting one of more
SpO2 30 breaths/min; severe respiratory distress; clinical signs indicative of imaging or clinical assessment
pressure of oxygen to respiratory distress; or SpO2 severe systemic illness with COVID-19, such and an oxygen saturation
fraction of inspiredCOVID-19: Remdesivir for Adults (updated August 2021) Evidence Synthesis Program
Supplemental Materials
COVID-19 NIH COVID-19 WHO Clinical Management Food and Drug Administration (FDA)11 Included Studies in
Disease Treatment Guidelines9 of COVID-1910 Evidence Report
Severity
Critical Individuals who have Individuals who have Positive testing by standard RT-PCR assay or ACTT-12: Not defined as
respiratory failure, septic respiratory failure, septic equivalent test; evidence of critical illness, “critical” but ACTT-1 included
shock, and/or multiple shock, and/or multiple organ defined by at least one of the following: and provided recovery
organ dysfunction. dysfunction respiratory failure defined based on resource outcomes for patients
utilization requiring at least one of the requiring invasive mechanical
following: endotracheal intubation and ventilation or ECMO.
mechanical ventilation, oxygen delivered by
high flow nasal cannula (heated, humidified, WHO6: Not defined as “critical”
oxygen delivered via reinforced nasal cannula but SOLIDARITY included and
at flow rates >20 L/min with fraction of provided mortality data for
delivered oxygen ≥0.5), noninvasive positive hospitalized patients requiring
pressure ventilation, ECMO, or clinical invasive mechanical
diagnosis of respiratory failure (ie, clinical ventilation or ECMO on study
need for one of the preceding therapies, but entry.
preceding therapies not able to be
administered in setting of resource limitation);
shock (defined by systolic blood pressureCOVID-19: Remdesivir for Adults (updated August 2021) Evidence Synthesis Program
Supplemental Materials
SUPPLEMENTAL REFERENCES
1. Schunemann H, Brozek J, Guyatt G, Oxman A. GRADE Working Group. GRADE
handbook for grading quality of evidence and strength of recommendations. Available
from: https://gdt.gradepro.org/app/handbook/handbook.html. Accessed 2 June 2020.
2. Beigel JH, Tomashek KM, Dodd LE, et al. Remdesivir for the treatment of Covid-19 -
final report. N Engl J Med. 2020;383(19):1813-1826.
3. Wang Y, Zhang D, Du G, et al. Remdesivir in adults with severe COVID-19: a
randomised, double-blind, placebo-controlled, multicentre trial. Lancet.
2020;395(10236):1569-1578.
4. Goldman JD, Lye DCB, Hui DS, et al. Remdesivir for 5 or 10 days in patients with
severe Covid-19. N Engl J Med. 2020;383(19):1827-1837.
5. Spinner CD, Gottlieb RL, Criner GJ, et al. Effect of remdesivir vs standard care on
clinical status at 11 days in patients with moderate COVID-19. A randomized clinical
trial. JAMA. 2020;324(11):1048-1057.
6. WHO Solidarity Trial Consortium. Repurposed antiviral drugs for Covid-19 - interim
WHO Solidarity Trial Results. N Engl J Med. 2020.
7. Barratt-Due A, Olsen IC, Nezvalova-Henriksen K, et al. Evaluation of the Effects of
Remdesivir and Hydroxychloroquine on Viral Clearance in COVID-19: A Randomized
Trial. Ann Intern Med. 2021.
8. Mahajan L, Singh AP, Gifty. Clinical outcomes of using remdesivir in patients with
moderate to severe COVID-19: A prospective randomised study. Indian Journal of
Anaesthesia. 2021;65(Suppl 1):S41.
9. NIH COVID-19 Treatment Guidelines. Available from:
https://files.covid19treatmentguidelines.nih.gov/guidelines/covid19treatmentguidelines.p
df. Accessed 24 July 2020.
10. WHO Clinical Management of COVID-19. Available from:
https://www.who.int/publications/i/item/clinical-management-of-covid-19. Accessed 24
July 2020.
11. US Food and Drug Administration. Fact Sheet for Health Care Providers: Emergency
Use Authorization (EUA) of Remdesivir (GS-5734™).
https://www.fda.gov/media/137926/download. Accessed 24 July 2020.
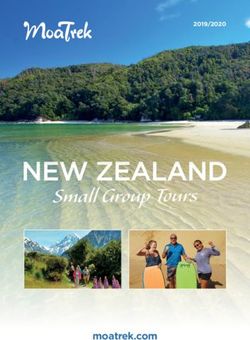
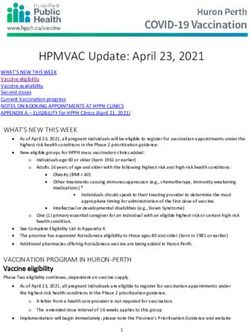
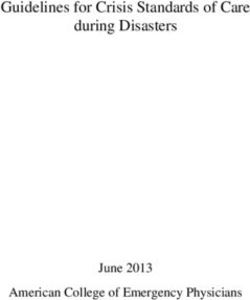
24COVID-19: Remdesivir for Adults (updated August 2021) Evidence Synthesis Program Supplemental Materials SUPPLEMENTAL FIGURE 1A: MORTALITY: ALL STUDIES (SIMPLE-2 WITH 5- AND 10- DAY COURSE): ABSOLUTE EFFECTS Abbreviations. ARD=absolute risk difference; CI=confidence interval 25
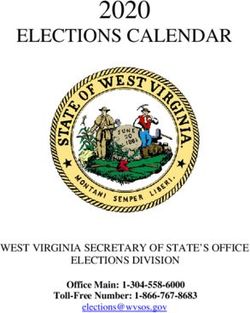
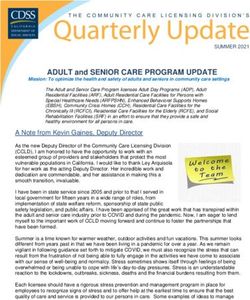
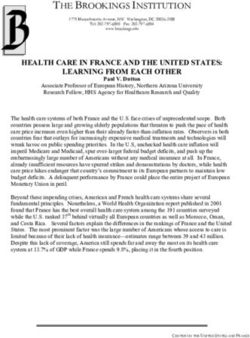
COVID-19: Remdesivir for Adults (updated August 2021) Evidence Synthesis Program Supplemental Materials SUPPLEMENTAL FIGURE 1B: MORTALITY BY INITIAL RESPIRATORY STATUS: ABSOLUTE EFFECTS Abbreviations. ARD=absolute risk difference; CI=confidence interval; ECMO=extracorporeal membrane oxygenation 26
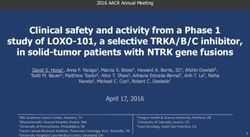
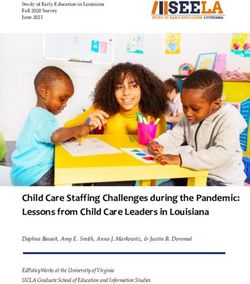
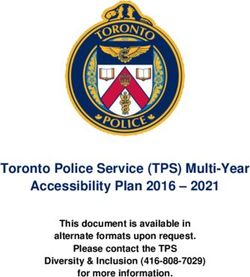
COVID-19: Remdesivir for Adults (updated August 2021) Evidence Synthesis Program Supplemental Materials SUPPLEMENTAL FIGURE 2A: PROPORTION OF PATIENTS RECOVERED: ABSOLUTE EFFECTS Abbreviations. ARD=absolute risk difference; CI=confidence interval 27
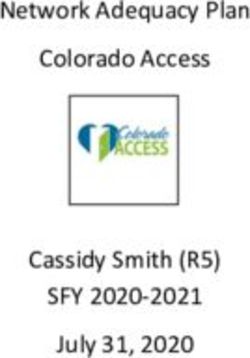
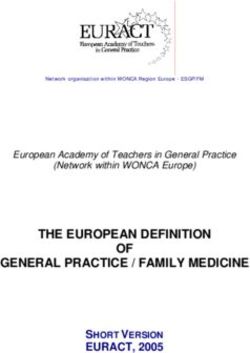
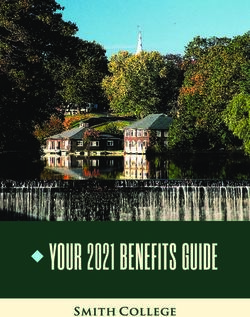
COVID-19: Remdesivir for Adults (updated August 2021) Evidence Synthesis Program Supplemental Materials SUPPLEMENTAL FIGURE 2B: NEED FOR MECHANICAL VENTILATION: ALL STUDIES (SIMPLE-2 WITH 5- AND 10-DAY COURSE): ABSOLUTE EFFECTS Abbreviations. ARD=absolute risk difference; CI=confidence interval; ECMO=extracorporeal membrane oxygenation * For the pooled trials, defined as: proportion on invasive ventilation/ECMO (new vs continued from baseline) at follow up (ACTT-1 on day 15, Wang on day 14, and SIMPLE-2 on day 11). † Unpooled Solidarity trial, defined as: subsequent need for ventilation in those not ventilated at baseline (through day 28) 28
COVID-19: Remdesivir for Adults (updated August 2021) Evidence Synthesis Program Supplemental Materials SUPPLEMENTAL FIGURE 2C: PATIENTS WITH ≥1 SERIOUS ADVERSE EVENT: ABSOLUTE EFFECTS Abbreviations. ARD=absolute risk difference; CI=confidence interval 29
You can also read