Crisis Standards of Care and COVID-19: What Did We Learn? How Do We Ensure Equity? What Should We Do? - National Academy ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
DISCUSSION PAPER
Crisis Standards of Care and COVID-19: What Did We
Learn? How Do We Ensure Equity? What Should We
Do?
John L. Hick, MD, Hennepin Healthcare and University of Minnesota; Dan
Hanfling, MD, In-Q-Tel and George Washington University; Matthew K. Wynia,
MD, University of Colorado; and Eric Toner, MD, Johns Hopkins Center for
Health Security
August 30, 2021
Authors note: The authors are grateful to have been involved in many conversations with pro-
viders, health care systems, and jurisdictions about crisis standards of care (CSC) issues during
COVID-19. Statements in this paper are often based on or buttressed by these accounts, al-
though the authors are not able to share the specific details, as some of these colleagues have
suffered professional retribution for raising these issues or being willing to have open and
honest discussion of the tactics that were implemented. The authors of this manuscript hope
that discussion about CSC can become akin to root cause analysis and other no-fault learning
environments. Until then, the authors are thankful for our colleagues’ honesty and desire to
clarify and improve our frameworks.
Introduction This paper focuses on hospital application of CSC,
though emergency medical services (EMS) experienced
COVID-19 has fundamentally challenged the delivery
similar issues. EMS and health care planning and re-
of health care services across the world, forcing dif-
sponse must be linked to ensure consistency of ex-
ficult choices on health professionals and laying bare
pectations as well as optimal patient distribution and
many preexisting health, medical, and public health
redistribution. Both EMS and hospital resources and
sector frailties. Extreme shortages of key resources
staff require stewardship during disasters, particu-
and worries that patients would not receive the care
larly ones that are protracted in nature. Recognition
they needed were frequent features of the response
of clinical care interdependency (long-term care, EMS,
beginning in the spring of 2020 and were recurrent
hospitals, outpatient care) in planning and response is
during subsequent regional and national peaks.
critical for avoiding CSC conditions and improving con-
Crisis standards of care (CSC) occur when the degree
sistency across the spectrum of care as well as across
of resource shortage requires decisions that place a
any given geographic region.
patient or provider at risk of a poor outcome. These
Revision of CSC doctrine is needed and should be a
situations arose in most jurisdictions and required a
focus for health care institutions and local, state, and
systematic, coordinated response [1]. Often, state and
federal governments alike to ensure that the best care
health care CSC plans were used or revised, or they
possible is delivered when the next disaster strikes. In
did not apply to the situations encountered. In several
the following sections, the authors discuss some key
critical instances, potentially useful CSC plans were ig-
CSC domains as well as successes, issues, and action
nored or actively subverted. The authors of this paper
steps.
describe some of the successes and shortfalls of CSC
principles and practices during COVID-19 and identify
issues to be addressed for future events.
Perspectives | Expert Voices in Health & Health Care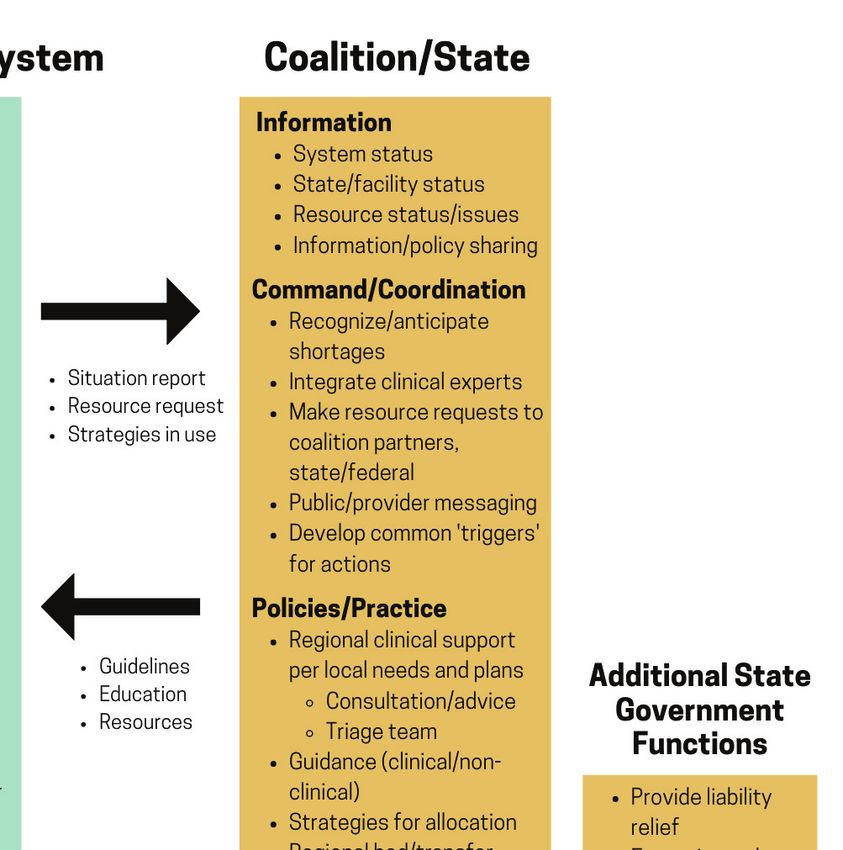
DISCUSSION PAPER
CSC Areas of Focus include race, such as the Centers for Disease Control
and Prevention’s (CDC’s) Social Vulnerability Index, has
Equity been less contentious in theory and has been recom-
CSC planning has been predicated upon the impor- mended by a National Academies of Sciences, Engi-
tance of ensuring unbiased, fair, and consistent tri- neering, and Medicine committee and the CDC’s Advi-
age decisions. However, COVID-19 laid bare the struc- sory Committee on Immunization Practices [13,14,15].
tural inequities of our current health care system that However, such tools have rarely been implemented in
made such aspirational goals largely unachievable practice for vaccine allocation—and where they have
and highlighted that some elements of CSC planning been used, they have sometimes been challenged
may unfairly penalize certain groups [2]. COVID-19 [13,14,15]. Rather, the focus on equity, where it has
disproportionately affected communities of color and been explicitly addressed, has been through strate-
at-risk individuals, such as those in skilled nursing fa- gies like establishing pop-up clinics in churches serving
cilities, detention facilities, and essential workplaces. communities of color and through outreach strategies
Further, preexisting comorbidities, multigenerational targeting underserved communities.
housing, use of public transit, and essential worker oc- The potential for structural racism in CSC plans is
cupations magnified poor outcomes and accelerated not the only concern. Risks of ageism and discrimi-
transmission in historically disadvantaged communi- nation against the disabled must also be addressed
ties [3,4,5,6,7,8]. [16,17,18]. This is especially true given the catastrophic
When resources are in shortage, fairness demands impact on residents of long-term care facilities, whose
extra effort to reach and serve the hardest hit com- life circumstances often present a high risk of implicit
munities, including tailored connection and commu- triage decisions by providers to withhold usual medi-
nication strategies, as many historically marginalized cal care, sometimes cloaked in the language of medical
communities have limited connection with, and sig- futility (i.e., presenting a triage decision, based on a re-
nificant distrust of, the medical system and govern- source shortage, as a decision to withhold the resource
ment initiatives. Unfortunately, for resources such as because it offers no benefit).
COVID-19 diagnostic testing kits and access to vaccines The authors suggest:
and monoclonal antibodies, there was widespread use • CSC protocols that will be used for making ur-
of online registration systems and implementation gent allocation decisions in a disaster cannot
of mass testing or vaccination sites, with the aim of be expected to remedy historic and structural
speeding the process and rapidly making progress, but inequity. However, they should not exacerbate
these choices further disadvantaged those with dimin- underlying disparities. Public and private part-
ished access to information, computers, and transpor- nerships are required to address structural in-
tation [9,10]. equity, trust, and access to care issues prior to
Equity clearly requires that resources be balanced an incident.
in a community to ensure a consistent level of care— • During a disaster, resource allocation for com-
such as patient load-balancing between hospitals (dis- munity-based interventions (such as vaccination
cussed later in this paper). The more difficult task is to clinics and testing sites) should be weighted to
ensure equitable access to information, basic medical ensure equitable access to resources for com-
care, testing, vaccination, and early treatment for un- munities according to their risk of illness and
derserved communities. While several racial and eth- mortality, including access to transportation,
nic minority groups have seen dramatically higher CO- personal protective equipment (PPE), diagnos-
VID-19 infection, hospitalization, and death rates, the tics, safe housing for quarantine, and treatment
direct use of race as a prioritizing factor for resource for those who become ill.
allocation has been controversial, with only Vermont • Ethicists and clinicians should agree concretely
and Montana doing so for vaccination prioritization on priority mechanisms of both allocation (e.g.,
[11]. Arguments against the use of race in medical when random number, lottery, weighted lottery,
resource allocation include operational concerns of or first-come-first-served are most appropriate)
defining members of racial groups, ethical concerns and clinical prioritization (e.g., according to like-
of fairness at the individual level, social concerns of lihood of benefit) when novel therapies are in
stoking racial resentment, and legal concerns of equal shortage (e.g., monoclonal antibodies, vaccine).
protection [12]. The use of multifactor risk tools that Templated baseline strategies and thresholds
Page 2 Published August 30, 2021
Crisis Standards of Care and COVID-19: What Did We Learn? How Do We Ensure Equity? What Should We Do?
for their use would also be helpful, in light of the of a declaration and which were not. Most state plans
apparent reticence of some political and clinical at least tacitly indicate that a declaration would be
leaders to acknowledge crisis conditions (dis- made to support such decisions as ventilator triage in
cussed further later in this paper). a catastrophic situation, but prior guidance has gener-
ally reflected a blanket invocation and not accounted
Politics and Declarations of CSC for more limited declarations or actions. Clearly, crisis
Both the 2009 and 2012 Institute of Medicine (IOM) conditions and the need to make decisions to prioritize
(now National Academy of Medicine) reports on CSC services and asset allocation can arise regardless of
(Guidance for Establishing Crisis Standards of Care for Use any jurisdictional declaration.
in Disaster Situations: A Letter Report and Crisis Standards The authors suggest:
of Care: A Systems Framework for Catastrophic Disaster • State leadership (public health, governors, at-
Response, respectively) defined CSC as requiring a “for- torneys general, and regulatory entities) should
mal declaration,” and, in fact, many hospital and state identify ways in which mitigation and surge strat-
plans rely on a state declaration to trigger CSC proto- egies can be implemented and supported at the
cols [19,20]. This threshold was included largely based state or regional level, including promoting com-
on the assumption that many resources would come munication and coordination of resources to re-
into scarcity at the same time, including ventilators and duce the need for CSC, in addition to regulatory,
other life-saving resources, but it did not consider that administrative, and executive actions to support
some resources might be in sustained shortage, yet providers and facilities and reduce liability.
not require formal state action. For example, during • Offices of governors and state attorneys gener-
the early phase of COVID-19, health care systems expe- al, health care systems, and state health depart-
rienced critical shortages of PPE, requiring implemen- ments should negotiate more explicit expecta-
tation of crisis strategies developed by the CDC—but tions of legal, regulatory, and policy support
usually without required state action. Although short- during crisis conditions, including consideration
ages no longer require crisis strategies, many facilities of specific triggers and requests that would au-
are still not able to use conventional PPE strategies at tomatically invoke CSC legal protections and
the time of this writing [21]. clinical guidance. These should recognize that
Only Arizona and New Mexico formally declared CSC, while a state declaration may be part of support
allowing for triage of ventilators and other intensive for clinical activities, crisis conditions can arise
care resources using state CSC plans. But the decision whether declared or not, and ad hoc clinical
to implement ventilator triage was left to health care problem-solving will likely still be required. Fa-
facilities, none of which apparently did so [39]. Wax- cilities and health care systems must coordinate
ing and waning conditions over time created significant care and mitigate crisis conditions as quickly and
difficulty in determining when a crisis situation began consistently as possible, and states have a duty
or ended for a given resource in a given area. Many to support providers making difficult choices.
jurisdictions reached a point where staff and resources • States should clarify the role of state health de-
such as dialysis were spread critically thin, with con- partment and governors’ offices in the public
fusion as to whether the system was in crisis or not. recognition of the aspects of the health care sys-
Some jurisdictions declared CSC at a county or state tem that are in crisis, the support of strategies
level without having leveraged patient transfer mecha- to mitigate the situation, and the provision of
nisms that could have unloaded their affected facilities best practice guidance when rationing becomes
(in the end, none of these wound up performing overt necessary.
triage). In addition, some areas that were clearly in cri- • Planning efforts should focus on developing and
sis related to ventilators, oxygen, or other resources, promulgating tools for managing specific re-
where painful triage decisions had to be made, never sources that may be in extreme shortage (e.g.,
received a formal declaration authorizing CSC [22,23]. PPE, dialysis, oxygen, sedatives) rather than
It appears that some states ignored their own CSC seeking an overarching declaration of crisis con-
plans to declare crisis conditions. This reticence is ditions. These should include public, patient, and
likely attributable to multiple factors, including politi- family messaging, legal and regulatory tools to
cal concerns as well as practical concerns about scope, support necessary health care rationing actions,
authorities, and liability in addition to issues defining and proactive guidance for those situations.
which specific conditions or shortages were worthy
NAM.edu/Perspectives Page 3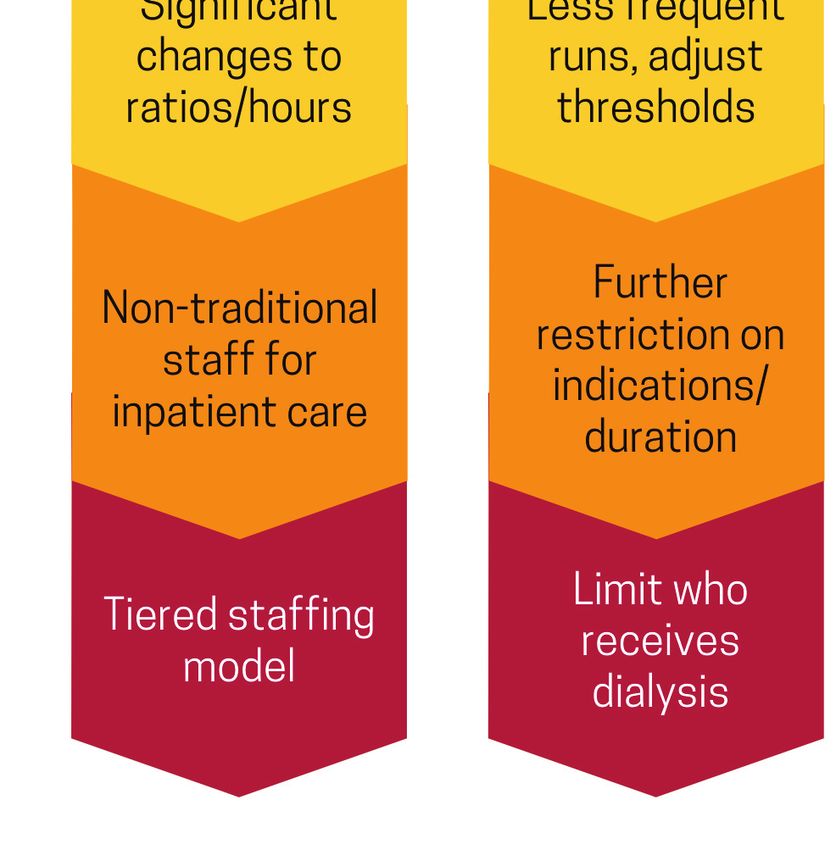
DISCUSSION PAPER
Box 1 | Definitions
• Conventional care: usual resources and level of care provided through maximal use of
the facilities’ usual beds, staff, and resources.
• Contingency care: provision of functionally equivalent care—care provided is adapted
from usual practices (e.g., boarding critical care patients in post-anesthesia care areas).
• Crisis care: inadequate resources are available to provide equivalent care—care is
provided to the level possible given the resource gap. Increased risk of morbidity and
mortality defines the care provided in this phase—this risk can be minimized by imple-
menting consistent proactive resource use strategies.
• Health care facilities and systems should work that health care workers could use bandanas and other
together to agree on information they will share protections of last resort during extreme shortages of
and actions that they will take to avoid crisis situ- PPE resulted in misunderstanding by health care work-
ations as well as coordinate efforts when CSC ers that the CDC considered such protective measures
implementation is unavoidable, regardless of adequate (which was clearly not the case) [23]. This was
governmental action. indicative of a much larger issue—the near-absence of
• When legislative protections are not available, education and training of the US health care workforce
legal protections for providers under executive to operate under disaster conditions. As a result, the
order should be sought but confined to address authors frequently observed an excessive fixation on
the specific issue and time frame (i.e., broad im- worst-case scenarios that generated significant emo-
munity for prolonged periods of time should tional response but that rarely occurred, such as com-
be avoided). If neither legislative nor executive plete absence of PPE, ventilators, or critical medica-
protections are available despite the need to tions. Though this may have resulted in the public and
make triage decisions, professional associations, providers taking precautions more seriously because
hospital associations, health care coalitions, and of the potential extreme consequences, it was not ef-
other entities that span jurisdictional boundar- fective in focusing health care planning.
ies should bring together health care systems, Illustrations of the spectrum of CSC usually repre-
public health departments, EMS, and emergency sent the transition between contingency and crisis as
management agencies to craft guidance, which a sharp vertical line between the two; however, this is
is likely to establish a reasonable provider legal not typically the case. Although some resource short-
standard for the circumstances. ages (e.g., ventilators) pose such a risk as to automati-
• Education should be provided to clinicians about cally represent crisis conditions, incremental changes
the circumstances under which life-saving re- to staffing or the performance of dialysis do not fall
sources may be ethically withheld from patients squarely within either the contingency or crisis cat-
without patient or surrogate consent, and these egory, and the lack of established triggers and proto-
processes must have the support of the provid- cols for allocating these resources created confusion.
ers as well as the state. In prior documents, including the 2012 IOM report,
transitions from conventional to contingency and con-
Categories and Nomenclature tingency to crisis have been described as incremental,
The CSC spectrum of care recognizes that health care but it was difficult for providers to translate this con-
surge occurs on a continuum across conventional, con- cept from graphical representation of a dividing line to
tingency, and crisis response (see Box 1) [20]. This no- knowing when the strategy used crossed the boundary
menclature was generally helpful in surge planning at from contingency to crisis based on the increased risk
the health care facility level and was used early in the to the patient of a given strategy [20]. One way this was
response to COVID-19 by the CDC in its guidance for addressed was to denote the transition from conven-
health care worker PPE [21]. However, problems arose tional care to contingency care as crossing a resource
from the CDC’s use of these categories as the progres- shortage threshold, when a particular resource was
sion across them was unfamiliar to clinicians and health noted to be in short supply. In a sustained or severe
care administrators. For example, a recommendation
Page 4 Published August 30, 2021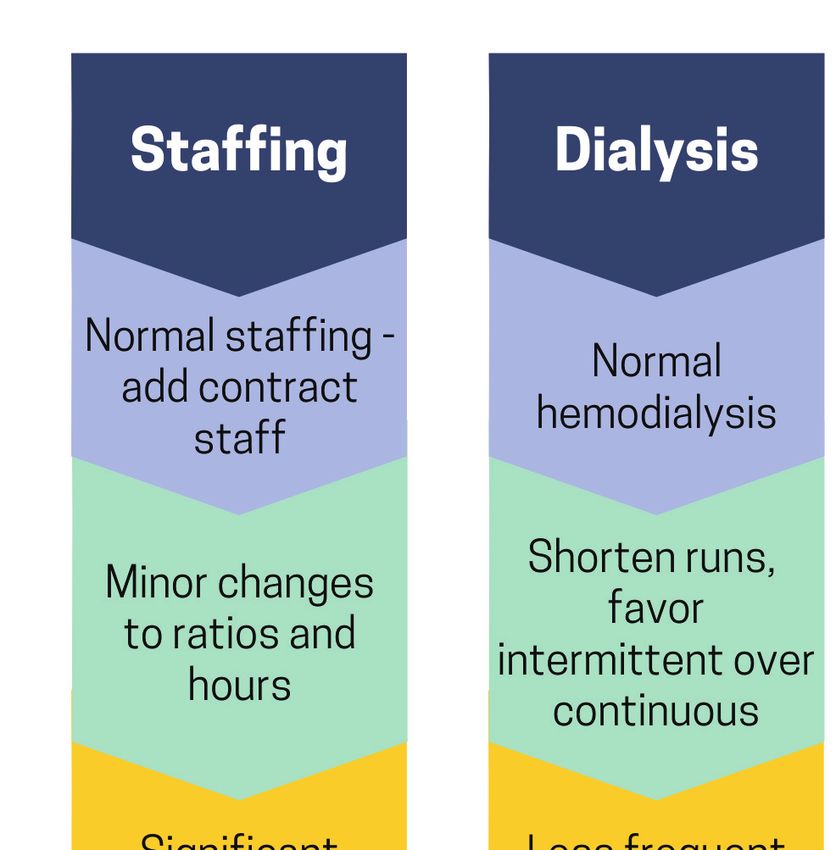
Crisis Standards of Care and COVID-19: What Did We Learn? How Do We Ensure Equity? What Should We Do?
disaster, clinical decision making might further be im- Understanding of Surge
pacted if supplies continue to dwindle, now crossing a Insights gained from the management of a large, sus-
resource triage threshold at which point decisions re- tained flow of patients to U.S. hospitals greatly ad-
lated to their specific allocation were required, denot- vanced understanding of actual surge capacity and
ing the transition from contingency to crisis care [20]. highlighted those factors (e.g., staffing, oxygen supply)
The transition of risk between contingency and crisis is that may limit the expansion of critical care in disas-
a gray area, particularly when a resource is elastic, and ters. If properly documented, this understanding of
is less important than a common understanding of the surge capacity can greatly advance regional and na-
progression of changes that will be made and an ability tional disaster planning. In many cases, hospital surge
to compare those adaptations to the ones required at plans did not reflect a graded progression of strategies
other facilities in the area. across the spectrum of conventional, contingency, and
However, multiple examples (see Figure 1) during crisis. In some cases, crisis surge plans were separate
COVID-19 demonstrated the ability of clinicians to documents.
implement graded changes in services provided, thus The authors suggest:
minimizing risks to patients [20,24]. In many cases, • States, health care systems, public health agen-
these were developed on an ad hoc basis but repre- cies, and health care coalitions capture and
sent examples that need to be preserved. Titrating the share available surge data and capacity data to
minimum change required to the resources available better understand daily system capacity as well
across this continuum satisfies the proportionality te- as for use in future events of all hazard types.
net of CSC. What constitutes significant risk to the pa- Accurate, accessible, relevant data are critical to
tient that indicates a transition to crisis care is often understanding the impact of patient surges and
open to interpretation, but the use of a graduated pro- the need for intervention.
gression ensures that the right thing is done clinically • Health care facilities should update surge capac-
for the circumstances. In general, the setting of triggers ity plans for all-hazards response that include
as a threshold for crisis (e.g., no ICU beds remaining) CSC strategies as part of the spectrum of a grad-
at the state level has failed because when this thresh- ed surge response, not as a separate plan.
old is crossed, either adaptive strategies allow contin- • Future architectural remodeling and health care
gency care beyond that number, or some facilities have facility capital improvement projects, including
crossed that threshold, but others have not. At the co- plans for new building construction, should an-
alition or regional level, agreeing on a threshold (such ticipate and accommodate disaster surge needs.
as staffing ratios) that is recognized as “in crisis” allows
improved communication of circumstances and coor- Coordination of Care and Information Sharing
dination, and can drive additional facility, coalition, and Community and regional (i.e., in a health care catch-
state actions to support the affected facilities. ment area) consistency in the delivery of care is cru-
The authors suggest: cial to avoiding pockets of crisis care and assuring
• Mandatory clinical staff education should be fairness, particularly given recent work illustrating the
provided about the spectrum of disaster care, increased mortality at hospitals experiencing COVID-19
which was a recommendation laid out in prior surge [25]. In many communities, COVID-19 forced
reports related to CSC calling for provider en- health care coalitions, hospital associations, and health
gagement [19,20]. care systems to refine data collection and informa-
• Casebooks with examples of stepwise degrada- tion sharing for system status monitoring. Such data
tion of services should be created (e.g., exten- coordination permitted coalition/state actions such as
sion of dialysis, using transport ventilators for load-balancing (i.e., medical operations coordination
patients with stable respiratory parameters). cells [MOCC]) that contributed greatly in many areas to
• When the significant risk (i.e., crisis) threshold is maximal use of critical care beds by facilitating trans-
not clear, regional definitions should be adopted fers from overwhelmed facilities [26,27]. Some short-
to facilitate resource allocation/movement deci- falls involved patients being refused transfer due to in-
sions—for example, what level of staffing consti- surance status [28,29]. Close coordination with EMS is
tutes crisis vs. contingency. required to ensure that adequate resources are avail-
• Emphasis should be on planning and effort to able for transfers and to maintain emergency response
avoid crisis conditions (i.e., stay in contingency). capacity. Regional and interstate coordination of EMS
assets may be required.
NAM.edu/Perspectives Page 5DISCUSSION PAPER
FIGURE 1 | Examples of Graduated Changes Across the Care Continuum
SOURCE: Developed by authors.
NOTE: Examples only. Does not represent all potential adjustments. Increasing risk for poor patient
outcome as changes implemented from top to bottom. Regional agreement on what constitutes ‘sig-
nificant risk’ and therefore crisis conditions is needed to facilitate communications, resource distri-
bution, and guide response strategy.
Page 6 Published August 30, 2021Crisis Standards of Care and COVID-19: What Did We Learn? How Do We Ensure Equity? What Should We Do?
Additionally, in some areas, health care coalitions including MOCC operations and essential ele-
and state entities were critical in allocating resources ments of information.
to facilities most in need, including PPE, ventilators, • Patient transfer decisions should be made irre-
and staffing. These coordination and prioritization spective to patient insurance status and other
mechanisms have been articulated and encouraged by nonclinical factors and should be based on pa-
the Department of Health and Human Services (HHS) tient loads and clinical needs only.
Office of the Assistant Secretary for Preparedness • A national system for health care system infor-
and Response (ASPR) Hospital Preparedness Program mation sharing in disasters should be developed
(HPP) requirements, which may be refined in future it- and implemented, with consultation from ma-
erations to further support this important role [30]. jor electronic health record (EHR) providers and
Between 2009 and 2020, the U.S. health care system other health care information technology com-
failed to define essential elements of information that panies, coalition leaders, clinicians, state health
could be shared between hospitals, across and be- departments, and health care system stakehold-
tween states, and with federal partners to assess the ers.
impact of an event in real time and to support load- • Passive data collection should be ongoing to es-
balancing of patients, staff, and resources. During the tablish daily and seasonal baselines for health
COVID-19 crisis, this led to implementation of ad hoc care systems (i.e., direct feed from the EHR) that
systems (e.g., awarding of de novo contracts to private will better demonstrate the impact of patient
sector parties), which created full-time obligations at surges on a geographic area when an incident
hospitals to fulfill data requirements, yet often provid- occurs including hospital capacity, morbidity,
ed low visibility on how this data affected federal deci- and, to a degree, mortality [32]. An information
sions [31]. States and health care coalitions also had chain powered by advanced analytics allow-
diverse interpretations of the data points requested, ing for forecasting, modeling, and predictions
which further limited the utility of the data (e.g., criti- should be built into these capabilities.
cal care beds available—some reporting staffed vs. un- • Facilities should create regional indicators of cri-
staffed beds). sis conditions to improve communication and
The authors suggest: coordination (e.g., the health care coalition will
• All jurisdictions should have access to a MOCC consider a facility in crisis and will implement the
[26] that can facilitate patient placement and re- regional MOCC, when patient loads, staffing, or
distribution. All hospitals should be required to restriction of nonemergency procedures differ
participate, and expectations for patient distri- significantly between facilities) that help create
bution/acceptance should be agreed upon prior consistency, direct regional patient movement,
to an incident. or prioritize a facility for resources.
• HHS should better define opportunities and
expectations for interstate coordination of in- Alternate Care Sites
formation sharing and patient movement. A Prior to COVID-19, many jurisdictions did not have ro-
process for interstate regional prioritization bust plans for establishing community-based alternate
of transportation and other assets to support care sites (ACS). This was a focus across the nation
these activities should be in place. during the early months of the pandemic for the U.S.
• Each state should have documented processes Army Corps of Engineers and FEMA [33]. Yet, very few
to reallocate available staff and material re- of these sites contributed significantly to the overall
sources and compare relevant indicators of im- number of patients cared for, and they often wound
pact and need across requesting facilities (e.g., up with disproportionate numbers of uninsured and
percent usual occupancy in addition to staffing difficult-to-place long-term care patients, suggesting
strategies implemented). dumping practices by hospitals onto publicly funded
• Essential elements of information with standard sites [34]. Staffing was a pervasive problem for these
definitions that support system monitoring and facilities, and most of the larger facilities were staffed
load-balancing should be developed and adopt- with federal resources, which is not an option for a ma-
ed by all states. jority of jurisdictions in most disasters. Often, success-
• Federal grant programs should adopt specific ful ACS were in jurisdictions that did not have robust
requirements for patient transfer coordination, inpatient resources or were geographically isolated
NAM.edu/Perspectives Page 7DISCUSSION PAPER
[35]. ACS may also be helpful in specific types of events circumstances. Many such decisions were not within
when local health care infrastructure is damaged or their usual scope of practice, though clinicians rarely
insufficient, and COVID-19 significantly advanced this felt they rose to the level of needing to consult a triage
planning. team as outlined in the 2012 CSC guidance [20]. There
Planning for hospital-based ACS (e.g., tents in a park- was often a disconnect between “bedside and board-
ing lot near the emergency department (ED) with ser- room,” as senior leaders were not always aware of the
vices limited to assessment and triage, or utilization decisions clinical staff were being forced to make, while
of non-patient care areas for inpatient care) may offer clinical staff were not well integrated into command-
significant advantages compared to community-based level decisions and did not receive adequate informa-
sites, due to proximity to medical resources and per- tion about available resources.
sonnel. Many hospitals developed plans and set aside A key way to avoid or minimize the need for resource
assets to ensure maximal care expansion on their cam- triage is to minimize resources expended on unwant-
puses prior to activating community-based sites. ed care, including for those who might altruistically
The authors suggest: decline services in the event of an extreme shortage.
• ACS plans should be updated based on best However, typical do not resuscitate (DNR) discussions
practices from COVID-19. rarely capture these issues. More nuanced discussion
• Hospitals should plan to maximize alternate and documentation of the wishes of patients, includ-
care areas at their facilities, as this can often be ing those around prolonged ventilation, tracheostomy,
done more quickly and effectively than opening feeding, renal replacement therapy, and overall goals
a community site. of care were critical to helping clinicians understand
• Each state should have defined thresholds for what the patient and family prioritize and helping ori-
when a community ACS would be opened and ent and reorient care during hospitalizations for severe
how it will be staffed, licensed (if applicable), and COVID-19. Engagement of family members using digi-
operated. This should assume that all available tal technology promoted frequent conversation about
hospital beds will be used first, elective proce- these issues during COVID-19 but, on the other hand,
dures will be halted, and hospitals will have drastically hampered the development of trust and un-
maximized on-site alternate care areas on their derstanding between family and health professionals
campuses. that these encounters usually rely on. There is ongoing
ethical debate on whether and how to engage patients
Clinical Decision Making or family members in conversations about altruistically
Unfortunately, clinicians experienced multiple informa- forgoing services voluntarily in the event of a severe
tion deficits throughout the pandemic, including lack shortage [36,37,38].
of knowledge of the status of their facility, their roles The authors suggest:
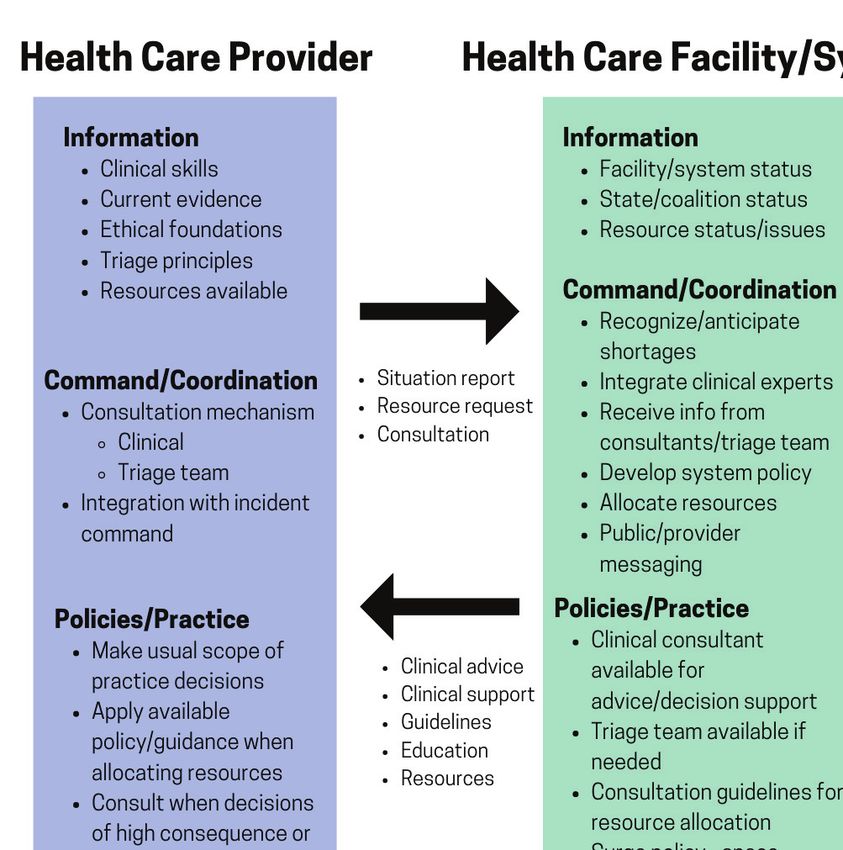
and responsibilities during a disaster, when and how to • Health care systems should develop clearer un-
seek consultations, and an understanding of the foun- derstandings of the required elements of CSC
dational elements of CSC and principles of ethical deci- that cover three levels of activity—from the cli-
sion making in disasters. nician at the bedside, to the health care facil-
Though many of these issues were addressed by ity, and finally the coordination level (coalition/
just-in-time education, in many cases clinicians felt state). These levels share requirements across
disconnected from the formal incident response and three domains in CSC: information, command/
felt forced to make ad hoc decisions at the bedside. coordination, and policy/practice.
In some cases, lack of communication about plans or • If the required information is not available, or if
recommendations from the facility level resulted in clinical practice, policy, and system components
implicit or covert triage decisions being made by cli- are not aligned, it is not possible to provide re-
nicians who believed that the resource situation was gionally consistent care or to mitigate the crisis
worse than it was, and/or determined on their own ac- effectively (see Figure 2). Planning, education,
cord that a patient should not be offered certain inter- and exercises are needed to ensure that the re-
ventions. Some of these ad hoc triage decisions were quired elements are in place and interface suc-
conflated with thinking on medical futility, (i.e., that the cessfully with each other.
treatment would not benefit the patient) though the • Critical care and other specialty physicians (e.g.,
interventions would have been offered under usual burn, pediatric, infectious disease, trauma sur-
Page 8 Published August 30, 2021Crisis Standards of Care and COVID-19: What Did We Learn? How Do We Ensure Equity? What Should We Do?
FIGURE 2 | Key Domains and Requirements in Crisis Standards of Care
SOURCE: Developed by authors.
geons) should be involved in both planning for • Clinicians should promote discussion of end-of-
and response to disasters, as well as integrating life wishes with patients and their families, in-
directly with the incident command system so cluding the completion of formal advance direc-
that clinical and administrative decisions can be tives before critical events arise. Health systems
informed together. should support these conversations through ap-
• Incident command should be aware of all cur- propriate financing, EHR supports, and fostering
rent or impending rationing decisions and work a culture of routine advance directive conversa-
directly with clinical staff and appropriate re- tions with all adult patients.
gional/coalition entities on mitigation strategies • Clinicians should discuss with patients and fami-
and creation of proactive guidance. lies the consequences of potential interventions,
• Critical care and other physicians should be en- including an honest assessment of likely out-
couraged to share information in structured and comes, as best they can be ascertained. These
informal communications with clinicians at oth- assessments should include details such as how
er facilities to share situational and best practice likely the patient is to return to baseline func-
information. tioning, and to elicit what tradeoffs of interven-
• All clinicians should receive real-time informa- tion/discomfort/rehabilitation the patient and
tion that is sufficient to understand whether or family feel would be appropriate. The patient’s
not they should be triaging specific resources. wishes should be documented in the EHR and
• All health care practitioners should receive train- reassessed as the clinical situation changes.
ing in basic disaster ethics and decision making, • Patients that voluntarily raise the possibility of
including an understanding of implicit bias. foregoing services or resources that are in short-
NAM.edu/Perspectives Page 9DISCUSSION PAPER
age have the legal and ethical right to decline which multiple ventilators had just been delivered by
services, but extreme caution must be exercised the state to the facility, but the provider was unaware
not to pressure patients into “altruistic” acts that of the delivery. Fortunately, the provider was alerted
are not consistent with their underlying values. to this availability in time to prevent potentially tragic
• Facilities should ensure that their legal counsel decisions.
supports the CSC processes and procedures and Triaging patients for critical care interventions some-
understands when and how they will be used. times reflects failures at the provider, facility, health
This should include a commitment to providers care coalition, or government levels. Often, it suggests
that they will be legally defended by the health the need to plan and coordinate better, and CSC im-
care entity if they are following the facility pro- plementation should be limited to situations where no
cesses. other options exist. In some cases during the COVID-19
• Legal and medical associations, as well as pub- pandemic, unfortunately, the solutions either chosen
lic agencies such as the Assistant Secretary for or available to clinicians facing immediate bedside re-
Preparedness and Response should provide source shortages resulted in morally injurious bedside
education about the increased legal risk for ad decisions—the opposite of the proactive, consistent
hoc rationing decisions versus creating plans approach advocated by CSC guidance. Rationing ac-
and expectations for how the health care system cess to extracorporeal membrane oxygenation (ECMO)
adapts to increased demand, how help is ob- provides an example of a uniquely limited resource
tained, and how services will be rationed when with high staffing demands, and this intervention may
necessary. require rationing even under routine system condi-
• Health care systems should maintain multimod- tions (or seasonal conditions such as influenza) [39].
al and transparent communication to staff, par- Regional systems for ECMO prioritization have been
ticularly nurses and physicians, about the cur- described in at least one jurisdiction [40].
rent situation, resources, strategies, trends, and During the COVID-19 pandemic, triage of critical care
coordination with outside agencies/coalitions, resources more often involved not initiating ICU-level
including what steps are being taken to address care rather than withdrawing or reallocating services.
current and future issues. This resulted in higher acuity care sometimes being
• Professional and specialty groups should de- provided in non-ICU environments or, at an extreme,
velop brief, targeted educational materials on not receiving usual interventions, such as a ventilator.
ethical and procedural CSC principles to be in- A reallocation decision (taking a needed resource from
tegrated into teaching curricula and adapted by a patient to give to another) is different than not initiat-
facilities with their specific information embed- ing care. Reallocation is so clinically, emotionally, and
ded. These professional standards can provide ethically challenging, that those decisions should be
both clinical and ethical guidance and may offer made by agreement of multiple providers that the de-
some legal protection to practitioners adher- gree of difference in prognosis warrants the realloca-
ing to professional standards in an emergency, tion, and only if the initial patient has had appropriate
even if CSC has not been formally declared by duration of therapy to demonstrate a lack of benefit.
the state. The CSC triage team approach in this case continues to
have relevance. However, concerns have been raised
Triage that the triage team construct espoused in previous
Though no health care facility was forced to triage IOM/NAM publications was too limited in scope and
ventilators proactively and overtly, many examples of too restrictive for dynamic environments, and that the
implicit or covert triage were communicated to the described appeals process would not be achievable
authors in confidence, in which physicians decided, [20,41]. There is agreement that triage decisions likely
based on their assessment, that they would not offer to result in death should not be made by a single pro-
mechanical ventilation to patients who would have vider, particularly when there is no accepted guidance
been offered this resource under non-crisis conditions. for the situation.
These decisions were often based on limited initial Even if statewide CSC plans had been implemented,
data suggesting extremely high mortality in the elderly many contained outdated triage tools. Very few encour-
from COVID-19 or limited ventilator resources at the aged consideration of disease-/condition-specific prog-
facility. One example highlighting this issue is a case in
Page 10 Published August 30, 2021Crisis Standards of Care and COVID-19: What Did We Learn? How Do We Ensure Equity? What Should We Do?
nostic variables, and many relied heavily on Sequential for disabilities. The notion of life-cycle prioritization of
Organ Failure Assessment (SOFA) scores. Limitations of younger patients over older is controversial because
the SOFA score have been recognized and publicized it is based on ethical norms not held by all cultural
prior to COVID-19 [42,43,44]. The SOFA score should groups, and it is not supported by current OCR direc-
not be used as a significant variable for COVID-19 or tives.
other primarily respiratory diseases, as scores are sig- Prioritization of specific social groups for critical care
nificantly lower than for disease states such as sepsis triage is highly controversial. Some states include es-
[45,46,47]. The assignment of points based on the cre- sential worker status in tiebreaking situations (e.g.,
atinine measurement does not differentiate between Colorado), and some did not include them after de-
preexisting and acute renal disease, particularly penal- bate (e.g., Minnesota). Others (e.g., Pennsylvania) have
izes renal failure/dialysis patients, and can exacerbate considered including geographic deprivation indices in
racial disparities even if race corrections for creatinine tiebreakers despite these being based on community
are not used [48]. Though the SOFA score may be help- and not individual factors. No triage process is value-
ful to compare relative acuity between patients or criti- neutral, and all may have effects on underlying so-
cal care units, it should play a very limited role in tri- cial, economic, and health disparities. Though there is
age methods compared to disease- or injury-specific broad agreement that saving lives is an important goal
knowledge. At present, there is no widely available of triage systems, there remains debate on how best to
prognostic tool that is reliable enough to exclude in- optimize overall benefits while prioritizing attention to
dividuals from critical care [47,48], and in any event, those hardest hit in a disaster [46,53].
the need to use such a tool should only apply to binary The authors suggest:
resources such as ECMO and mechanical ventilation. • The availability of rapid expert consultation
Such tools are of limited or no utility when considering must be ensured for rationing decisions outside
allocation of elastic resources like medications and di- of the provider’s normal practice for which there
alysis that can be titrated, substituted, and more grace- is no practice guideline. This expert or group
fully degraded. should have visibility on hospital and regional
In many cases, clinicians made decisions to with- resources and be able to push the decision and
hold interventions based on the patient’s age and as- the consequences up to incident command to
sumed COVID-19 mortality risk. Even though age has facilitate both optimal decision making and de-
direct correlation with risk of death from COVID-19 velopment of proactive strategies to avoid the
[51], the initial assessment of that risk was far more ongoing need for triage.
grim than later data revealed [52], particularly in the • Improved prognostic tools should be prioritized
60- to 70-year-old age group—illustrating the need to for use and widespread deployment. These
have the best available data possible and make it rap- should be both generic systems for organ failure
idly available to clinicians. Some of the very high early assessment as well as condition-specific assess-
mortality rates among older patients during surge con- ment tools. The marked improvements in data
ditions may have been influenced by implicit or covert science, including the application of artificial in-
triage decisions, raising mortality rates among patients telligence (AI) and machine learning to improve
from whom resources were withheld. Monitoring and predictive analytics, should be leveraged to cre-
updating practice guidelines with the latest informa- ate more accurate triage scoring systems, while
tion can help ensure consistency of decision making monitoring closely for inadvertent creation or
and avoid incorporation of age-related and other bias. exacerbation of inequities (a recognized ethical
Discrimination against people with disabilities was risk of AI risk prediction algorithms) [54].
found in several clinical situations and state CSC plans. • In the absence of more accurate scoring systems,
The HHS Office of Civil Rights (OCR) created guidance state and coalition CSC plans should emphasize
that patients needed to be assessed as individuals and coordination of care, access to rapid expert con-
that providers could only use age in determining re- sultation, and situational awareness rather than
source allocation when there were no better measures score-based triage. There should be a review of
available to assess mortality risk and when there was state triage decision tools, and scoring systems
a clear correlation of age with mortality for the specific that do not perform well at the individual patient
condition [16,17,18]. The same considerations apply level should be eliminated or minimized. Scoring
NAM.edu/Perspectives Page 11DISCUSSION PAPER
systems should be used only as a contributing • Plans should specify that the threshold for re-
factor in an individualized assessment process, allocating lifesaving resources should not be
and they should use disease- and injury-specific merely a “possible better chance of survival,” as
factors rather than using a generic scoring sys- might be appropriate during an allocation be-
tem. These plans should incorporate routine re- tween two patients not yet receiving the inter-
gional coordination for therapies such as ECMO vention. There should be a significant difference
that may require rationing in non-disaster situ- in likelihood of survival agreed upon by more
ations. than one expert provider.
• The triage process should specifically exclude • Health care facilities should define the situations
consideration of age, race, gender, disability, and in which an appeals process may be reasonable
other inappropriate discriminators, and those and develop a different model to ensure that
conducting triage should be trained on implicit bias is avoided when time-sensitive decisions
bias with the aim of mitigating the inadvertent are needed— particularly if multiple appeals are
exacerbation of disparities. occurring simultaneously. Ensure appropriate
• The state or region’s attorney general’s office documentation to support quality assurance re-
should review the state plans with specific atten- view, including by the consulting provider.
tion to civil rights protections. • Hospitals and health systems should develop
• The critical care triage processes should exclude policies and processes for discontinuation of
factors not related to medical prognosis or re- potentially non-beneficial therapies. These
source utilization (e.g., status as a health care should explicitly address resources that may be
worker, location of residence, status as a parent, in shortage, such as ECMO, and should empha-
status as an essential worker, status as a child) size accurate and complete communication with
unless these are shown to be socially and legally patients and families when a resource is being
accepted by the community and supported by provided as a trial of therapy rather than as a
the state. resource indefinitely assigned to a patient.
• Social factor incorporation must be procedurally
sound, address the target goal, and be easily ad- Supplies
dressed and implemented by the bedside clini- COVID-19 illustrated in graphic fashion that a just-in-
cian. Geographical and other population-based time supply chain struggles in the face of global de-
determinants of impact have significant value mand. Some of the biggest supply problems faced
for prioritizing interventions prior to hospitaliza- could have been anticipated based on the 2009 H1N1
tion but are controversial to use in prioritizing experience, but solutions were often avoided because
assignment of critical care resources, as there is they involved too much perceived effort, lacked market
no assurance that the goals of the intended cor- drivers (e.g., reusable PPE would generate less revenue
rection are met at the individual level. That is, a than disposable), or were judged too expensive (e.g.,
privileged resident of an area scoring high on a extra ventilators). Shortages of PPE were a known risk
social vulnerability index may be inappropriately after the 2009 H1N1 pandemic, so the scope and the
prioritized over a disadvantaged individual that duration of shortages and their effects on provider
lives outside a prioritized area. This is not an is- health, well-being, and workplace morale should have
sue in community-based interventions where been no surprise during the COVID-19 pandemic. Also,
the community at large benefits from targeted not surprisingly, nations (including the United States)
assignment of assets but is problematic when often prevented export of PPE, medications, and vac-
assigning life-saving resources [55,56]. cines, keeping these for domestic use regardless of in-
• Plans and education should acknowledge that ternational contracts and obligations, and sometimes
withholding usual interventions is triage and against public health best practices to stop the pan-
should only be performed in circumstances that demic most efficiently worldwide.
require such restrictions. Providers must be In some cases, there were problems with both re-
transparent with patients and family members source availability and distribution. For instance, high-
when a care decision is being made because the flow nasal cannula oxygen emerged as a key therapy
therapy will confer no benefit (i.e., futility) ver- for COVID-19 but placed extraordinary demands on
sus when resource triage is required based on hospital oxygen systems. Flow limitations for existing
scarcity. oxygen plumbing, freezing of vaporizers, and inability
Page 12 Published August 30, 2021Crisis Standards of Care and COVID-19: What Did We Learn? How Do We Ensure Equity? What Should We Do?
to obtain timely delivery created numerous problems. Nurse-to-patient ratios often remained stretched for
In some cases, oxygen conservation strategies were months at a time, contributing to burnout. Ironically,
not enacted in facilities despite low pressure alarms. at the same time, many health professionals involved
The authors suggest: in outpatient and surgical care were furloughed or laid
• A systematic examination of U.S. medical sup- off, though some transitioned from surgical and out-
ply chain resiliency, with a focus on disasters patient roles to inpatient roles. Some hospitals used
and likely shortages during disasters, what can nontraditional staff to provide care in intensive care
be learned from routine medication shortages environments, supervised by critical care staff and
to inform disaster preparedness and response, nurses in ratios that expanded and contracted to meet
and strategies for prevention and mitigation of the demands with available staff. Many states and fa-
supply disruptions. This should include an anal- cilities made requests for staffing assistance that were
ysis of U.S. reliance on international resources, difficult to prioritize without shared data on the types
and reliance of our international partners on of staffing contingencies invoked (e.g., facilities pro-
U.S. resources to fully assess the benefits and nounced themselves in crisis to seek assistance de-
risks of the current push for onshoring medical spite wildly different availability of staff).
supply manufacturing. Just-in-time training and mentoring helped provid-
• A new approach to PPE development, design, ers adjust to new roles, but the mental health impacts
and willingness to use, including respirators of high acuity, contagion, long duration surges, and
with cleanable surfaces, elastomeric models de- often new or expanded responsibilities was immense
signed specifically for health care markets, stan- and likely will cause workforce repercussions for years.
dardizing the testing and assessment of simple Staff are not infinitely expandable, and in some cases,
masks, and refining categorization of barrier states inferred that triage of patients would occur (or
materials. did occur) due to staffing issues, but binary types of
• Improving caches of materials (including agree- triage (e.g., critical care vs. palliative care) should be
ing on reasonable surplus stocks of ventilators, avoided when staffing is the limiting factor [57]. In-
PPE, and medications to support all-hazards crit- stead, prioritization of the sickest patients to be cared
ical care) at the facility, health system, state, and for by the staff with the highest level of training/com-
federal level. petency is appropriate, as are other strategies to try
• Dedicated planning around oxygen, as it repre- to match staff to patient needs when staffing is con-
sents a key vulnerability for hospitals, including strained.
changes to hospital design to allow higher vol- The authors suggest:
ume delivery to inpatient units, developing strat- • Hospitals should include the possibility of ex-
egies for emergency conservation measures treme staffing shortages in their surge capacity
when demand is high, and explicit triggers for and CSC planning, and educate staff about the
implementation of specific conservation strate- plans, new roles, and necessary competencies.
gies. • Health care facilities should ensure dialogue
with their unions and appropriate flexibility in
Staffing collective bargaining agreements to allow a safe
Availability of staff, particularly nursing and respira- and flexible disaster response.
tory therapy, to support expanded COVID-19 critical • National curricula should be refined and imple-
care was a pervasive issue and the subject of a rapid mented by hospitals to improve nursing and
expert consultation by the National Academies of Sci- physician staff comfort in stepping up to provide
ences, Engineering, and Medicine [57]. In many cases, a higher level of care in contingency or crisis sce-
contract personnel, federal and state disaster team narios. This should be reinforced by just-in-time
members, and others played a crucial role enabling training.
care expansion. Severe financial impact on health care • Health care coalitions and states should agree
systems was not an expected consequence of a pan- on commonly accepted definitions for crisis
demic but resulted in widespread furloughs and lay- staffing (e.g., use of nontraditional providers in
offs driven by reduced ED, outpatient, and procedural critical care environments, increase in nurse-to-
visits. [58]. patient ratios beyond a particular percentage,
use of tiered supervised staffing) to enable bet-
NAM.edu/Perspectives Page 13DISCUSSION PAPER
ter situational awareness and improved load- mendously to improve consistency and reduce provid-
balancing of patients and allocation of available er moral distress.
staff. The authors believe that specialty societies, major
health care systems, and private sector health infor-
Concluding Suggestions mation technology partners should work together to
The prior CSC work and its contributions during CO- leverage AI to assist in developing better prognostic
VID-19 to policy and practice should be revisited and tools for critical illness in general, as well as for disease-
updated in collaboration with national experts in medi- and injury-specific situations, and to develop systems
cine, ethics, law, and other disciplines, with an empha- for tracking the effects of using these algorithms on
sis on the need to avoid crisis conditions by planning key measures of equity. The ability to leverage AI will
for systems of care that maintain consistency across also offer opportunity during a novel event to deter-
regions through patient and resource movement. mine risk factors and treatment efficacy, as well as to
Documents such as this one and those that result improve supply chain decision making, including the
from future workshops and committees should be proactive steps necessary to supplement resources an-
used as discussion drivers at the hospital, health care ticipated to be in short supply.
system, health care coalition, state, and federal levels The authors hope that technological advances will
to change policy and process, and optimally be writ- result in meaningful improvements to PPE and will also
ten into federal preparedness program expectations drive changes in critical medical equipment. Ventila-
(e.g., requirements of facilities and coalitions under the tors will be cheaper and easier to use, with standard
HHS/ASPR Hospital Preparedness Program). There is circuits and next generation autonomous systems that
also a clear need to include public health departments can augment the role of respiratory therapists by using
and officials, as well as state governors, in discussions machine-learning algorithms to adjust ventilator set-
to understand when CSC may be invoked and what the tings. Both software and hardware changes to devices
state role is relative to declarations, legal protections, as well as increased integration of remote patient mon-
best practices, and other CSC domains. The actions of itoring, the use of wearables, sensors, and other means
the states during COVID-19 were diverse and varied, of virtual health care could help reduce the strain on
from overly broad declarations of CSC with long-dura- overburdened health care facilities by honing decision-
tion immunity for providers, to no action or acknowl- making skills about who needs to seek care and when.
edgment of the situation in the face of overwhelming The use of such tools can also help to standardize care
patient volumes that required triage of resources such (through greater use of checklists and care plans), re-
as dialysis. In many states, no specific legal protection duce nursing workload (by allowing medication drips
was afforded to physicians forced to make triage deci- and ventilators to integrate with patient monitoring
sions, which contributed to opaque decision process- and auto-titrate within specified ranges of hemody-
es. States and health care systems should emphasize namic or respiratory parameters), and prioritize atten-
transparency and facilitate better decision making by tion in busy units by having graded alarms and notifica-
providing consultation and clinical advice in scarce re- tions, among other improvements.
source situations. When the initial CSC recommendations were first
Prior to COVID-19 there was a recognized gap in cli- created in anticipation of the second wave of the 2009
nician (physician, advanced practice providers, nursing H1N1 influenza pandemic, the authors recognized that
staff) understanding of the ethics and process around future events and learnings would surely result in im-
resource triage and allocation. Building off scarcity provements and revisions to those initial recommen-
thinking and everyday challenges around medication dations [19]. While there have been some incremental
shortages, providers should receive foundational edu- changes made in the ensuing eleven years, informed
cation on the basics of rationing, triage, the shared duty by research as well as discrete events such as the
to steward resources, and current weaknesses in as- Haiti earthquake, COVID-19 provides the emergency
sessing individual prognosis (with limited disease- and preparedness and response community a distillation
injury-specific exceptions). The total time commitment of experiences that allows health care planners and
should be relatively small, but a shared understanding providers to systematically incorporate CSC learnings,
of health care workers’ obligations, limitations, plans, successes, and failures. Unless the time is dedicated
and processes to address shortages would help tre- to engage the providers, do the planning, perform the
Page 14 Published August 30, 2021You can also read