COVID + Pathway Learning Network webinar series - OFFICIAL Webinar 12: The Time is Now, Managing Patient Flow beyond COVID- 19 - Better ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Wednesday 15 December, 2021
COVID + Pathway Learning
Network webinar series
Webinar 12: The Time is Now, Managing Patient Flow beyond COVID-
19
OFFICIAL
OFFICIAL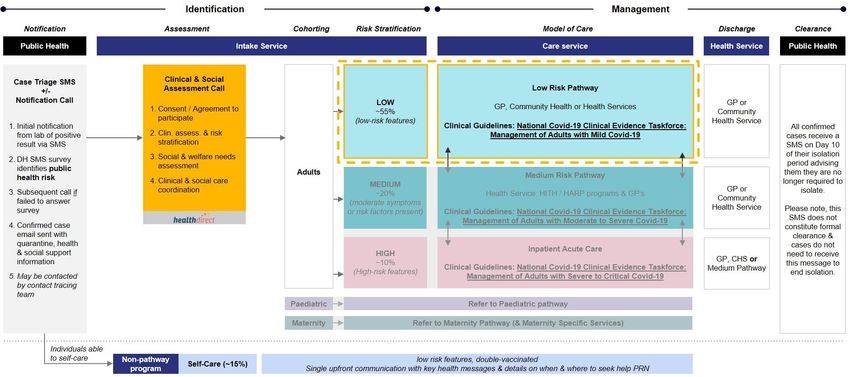
Acknowledgement of
Traditional Owners
I acknowledge the Traditional Custodians of all
the lands in which we live and from where we
join this meeting today. I pay my respects to
the past, present and future Traditional
Custodians and Elders of this nation and the
continuation of cultural, spiritual and
educational practices of Aboriginal and Torres
Strait Islander peoples. I also pay my respects
to the Elders of other communities who may
be joining us today.
Artwork by Anmatyerr woman, Tradara Briscoe
OFFICIAL
Overview
Topic Presenter
COVID + Pathway update Shannon Wight
Executive Lead, COVID + Pathways, Department of Health
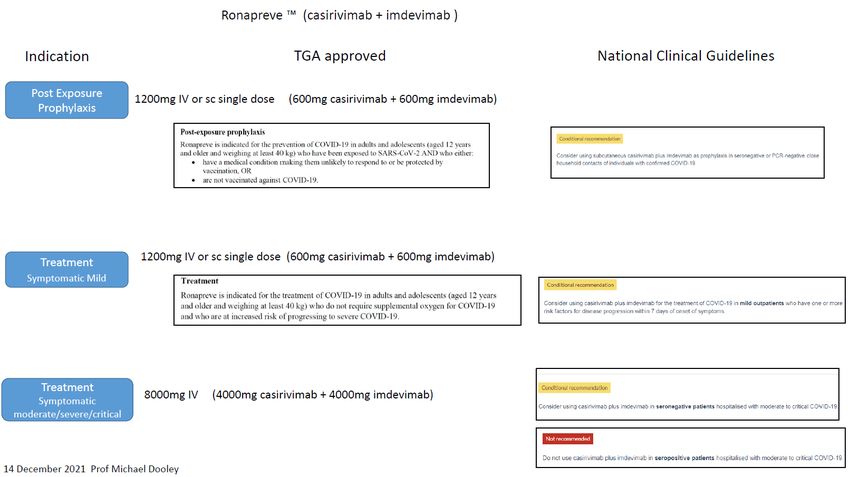
Sotrovimab/Ronapreve update Prof Michael Dooley
Director of Pharmacy, Alfred Health. Professor of Clinical Pharmacy,
Centre for Medicine Use and Safety, Monash University. Adjunct
Professor, Department of Epidemiology and Preventive Medicine, School
of Public Health and Preventive Medicine, Monash University
Questions
The Time is Now, Managing Patient Flow beyond Dean Pritchard
COVID-19 Northern Health/ SCV Faculty Timely Care
Kiri Stuart
Peninsula Health
Dr Amith Shetty
NSW Health
Questions
OFFICIAL
COVID + Pathways update
Shannon Wight – Executive Director, COVID + Pathways Program
& Executive Director Clinical Operations, Eastern Health
OFFICIAL
OFFICIAL
OFFICIAL
Current priorities: Self-care program
C+P key priorities
• Designed for C+ individuals who are considered very low risk and capable of self-managing their own care
• Directs precious resources to those most at risk and promotes self-care,
1 Self-Care Program • Anticipated self-care allocation may grow over time as the risk profile shifts as more Australian’s become double
vaccinated.
Criteria Model Journey
To be able to self-care, individuals must - Individual consents to self care
meet the following criteria: Individual self-monitors symptoms
- Individual able to self-care receives an
- > 12 and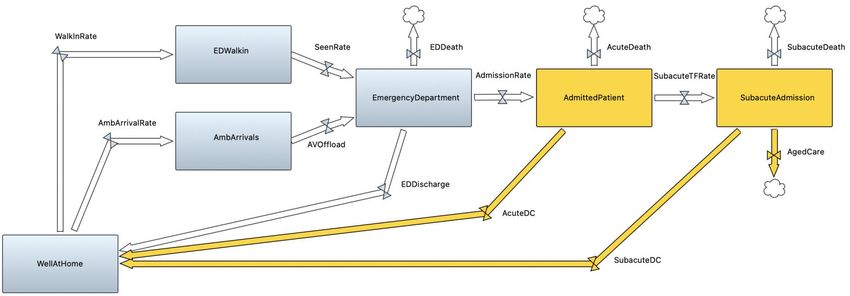
OFFICIAL
OFFICIAL
Current priorities cont’d
C+P key priorities
• Commonwealth, Healthdirect Australia and Victoria are working together to define the national C+P rollout, with Victoria
identified as the leading jurisdiction.
Establishment of • Oversee the pilot project to successfully transition Healthdirect to undertake all GP referrals in the NE, as part of
2
National C+P model the C+P program.
• Enable stakeholder engagement to deliver the pilot project and identify opportunities to ensure future scalability.
• North East leading the pilot site with the North East HSP.
COVID Positive Pathways Program December 2021
Vic Department of Health
OFFICIAL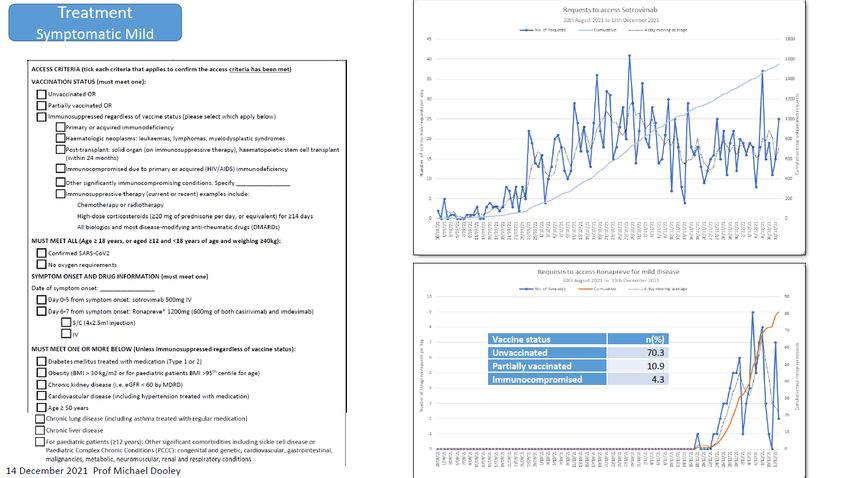
OFFICIAL
OFFICIAL
Current priorities cont’d
C+P key priorities
• Working closely with SRS’s to identify who can be cared for on a pathway
3 Disability • Work underway to review pathway eligibility in order to ensure people living in supported residential services
and disability accommodation settings receive the clinical care they require at the right time, in the right place
throughout the duration of their illness
• Updated, informative messaging and web content to the Victorian community on how to self-care and live with
COVID
4 Public messaging
https://www.coronavirus.vic.gov.au/managing-covid-19-home
https://www.coronavirus.vic.gov.au/covid-positive-pathways
• Consideration to expand the C+P program to support patients with chronic disease/ frequent presenters.
Consideration/ reform
5 • Work underway between the department and SCV to consider opportunities to integrate long-COVID care into
opportunities
the ‘pathways’ model and consult with primary care in delivering support.
COVID Positive Pathways Program December 2021
Vic Department of Health 7
OFFICIAL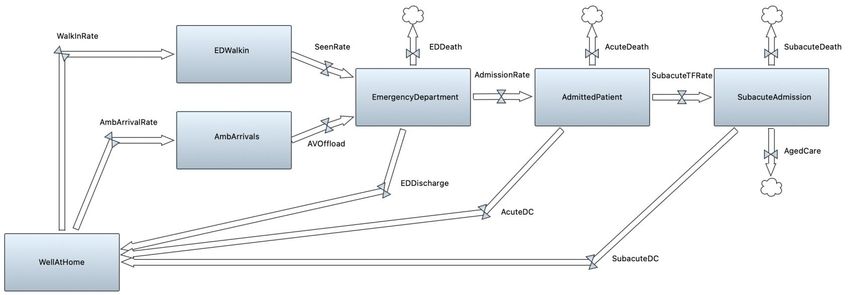
Sotrovimab/Ronapreve update
Prof Michael Dooley
Director of Pharmacy, Alfred Health. Professor of Clinical Pharmacy, Centre for Medicine Use and Safety,
Monash University. Adjunct Professor, Department of Epidemiology and Preventive Medicine, School of
Public Health and Preventive Medicine, Monash University
OFFICIAL
OFFICIAL
OFFICIAL
OFFICIAL
OFFICIAL
OFFICIAL
OFFICIAL
OFFICIAL
OFFICIAL
The time is now: Managing patient flow
beyond COVID-19
OFFICIALHospital Access Block
Raising the bar with COVID…
Picture: The Australian (2021).
OFFICIALThe Whole of System Approach
Unplanned arrivals
OFFICIALThe Whole of System Approach
Unplanned arrivals
OFFICIALTimely Care Collaborative
Kiri Stuart
Dr. Amith Shetty
OFFICIALUsing improvement
science to reduce
unnecessary bed days
December 2021
OFFICIALObjectives
Failing to achieve hospital wide patient flow – the right care, in the right place, at the right time – puts patients
Context at risk for suboptimal care and potential harm. Optimizing flow and improving outcomes for patients requires an
appreciation of the entire system of care.
A hospital wide audit of unnecessary bed days, as part of the Timely Care Collaborative, indicated Residential
Trigger
Aged Care patients may present greatest opportunity to improve flow
Question How can we improve timely care and reduce flow delays for this patient cohort?
This review aims to:
1 Describe the problem we are trying to solve
Describe how improvement science is being used
2
to reduce unnecessary bed days
3 Outline improvement action plan
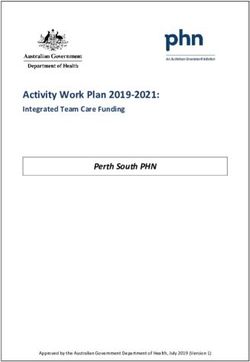
OFFICIAL 23Unnecessary bed days have increased significantly since
2019
Data entry issues
related to new Insights
1,050
C Chart surgical activity at ▪ This measure is derived form our
950 Frankston Private “Countdown to Discharge”
process. Unfortunately the
850 Outbreak
process is inconsistently
at PH
followed, so the data has to be
750
interpreted with caution.
650 ▪ Historically, medical and surgical
units at Frankston Hospital
550 carried between 130 and 150
COVID wave 1, unnecessary bed days per month
450 fewer inpatients 411 (around 5 per day).
354 ▪ This dropped during the first
350
298 wave of covid, with fewer
250 inpatients.
UCL
CL ▪ A spike during the outbreak at
150 LCL
PH likely reflects increased
50 challenges in discharging
Mar-19
May-19
May-20
Apr-19
Jul-19
Mar-20
Apr-20
Jul-20
Mar-21
May-21
Apr-21
Feb-19
Oct-19
Nov-19
Dec-19
Feb-20
Oct-20
Nov-20
Dec-20
Feb-21
Jan-19
Jun-19
Aug-19
Sep-19
Jan-20
Jun-20
Aug-20
Sep-20
Jan-21
Jun-21
patients, as well a reduced focus
on timely discharges.
▪ The spike in May 2021 likely
reflects teething issues with data
from elective surgery contracted
Definition: All days patients in hospital past their “Day 0” date – the date they are medically clearer for discharge. out to a private hospital.
Included: Acute Medical and Surgical unit, Frankston Hospital
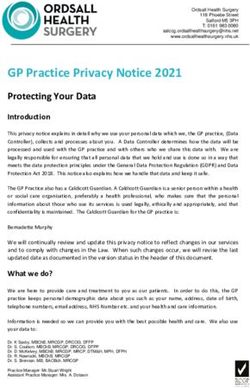
OFFICIAL 24A deeper dive into the data showed almost 99% of UBD’s
came from subacute wards, specifically patients waiting for
t/f to aged care facilities
Patients on medical, surgical and subacute wards over day 0 on discharge readiness whiteboard , Thursday 14 th October 2021,
n = 52 patients & 1,313 UBD’s
700 120%
600 13
100%
99% 99% 99% 100%100%100%
94% 97% TCP 9
500 88% 8
82% 80%
75% NOT SPECIFIED 6
400
60% 4
300 50% HOME 3
40% 2
200
PCU OR GEM 1 RACF cohort may present
100 20% 1
656 334 88 82 70 48 22 4 3 3 3 2 ABI CLINIC CAULFIELD 1
greatest opportunity to reduce
0 0% 1 UBD’s
AWAITING PLACEMENT 1
1
SRS 1
Subacute wards
• 5GS includes 1 patient with 327 UBD’s
Source: Audit of Discharge Readiness whiteboards,
• GLR1 includes 1 patient 348 UBD’s and 125 UBDs
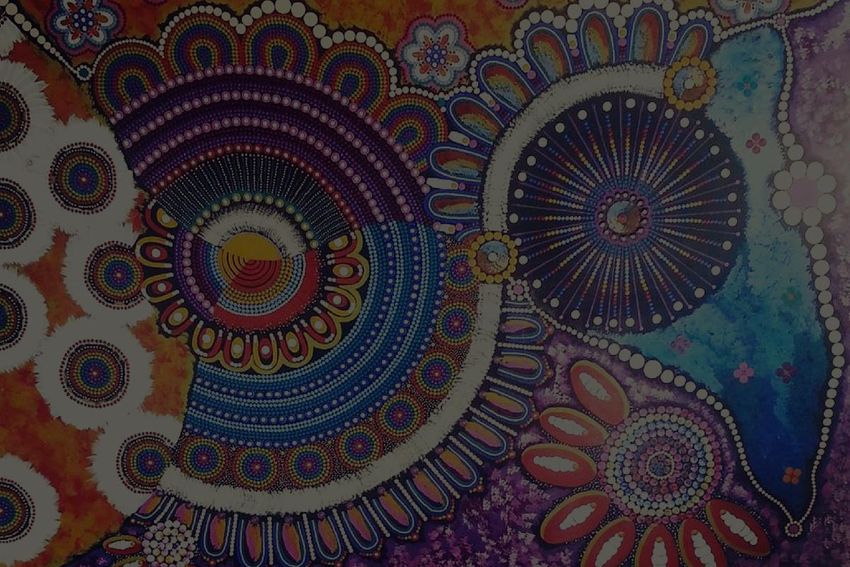
OFFICIAL 25Family deciding on facility and waiting on a bed account for
56% of delays
Insights
Patients being discharged to a RACF with 1 or more
Reason for UBD for patients being discharged to RACF 14th - 1. Flinders and Sorrento had
UBD and cumulative UBD’s 14th - 26th October, n = 18 &
26th October , n = 19 patients
cumulative UBD’s of 251 highest no. of patients being
discharged to a RACF with 1 or
more UBD. Flinders had greatest
6 120% cumulative UBD’s
100%
94% 2. Family deciding on facility and
5 100%
83% waiting on a bed account for
Gunamatta 262
4 72% 80%
56% of delay reasons
56%
Sorento 110 8 3 60%
2 28% 40%
Flinders 115 8
1 20%
5 5 3 2 2 1
Sum of UBD's No of patients 0 0%
1
family waiting change in further dc internal external
deciding on bed med planning ax ax
on facility status required
2
Source: Audit discharge readiness whiteboard
OFFICIAL 26There is a corresponding increase in ALOS for subacute to
aged care transfers by 66 days since 2019
ALOS and separations for RAPPS – RACF patients
1 July 2019 to 30 September 2021, n = 1,084 patients 4
Insights
1. First lockdown in Melbourne Impacts
3 of lockdowns include families unable
2 to view facilities, some facilities not
1
accepting patients until cleared of
COVID, decreased community
supports available i.e. PCA, family
2. Second lock down & 50% reduction
in rehab bed capacity at Golf
Links Road (GLR)
3. Beginning of Delta outbreak
4. PH became a streaming hospital 1
Acute and RAPPS ALOS for RAPPS – RACF patients October
5. Patient cohort changed when closed
1 July 2019 to 30 September 2021, n = 1,084 patients beds at GLR
50 6. Acute ALOS relatively flat while
RAPPS increased ALOS 8.3 days
40 5 6
30
20 With an increase in UBD in patients
waiting for transfer to residential aged
10 care there is an increase in ALOS
0
Jul-19
Jan-20
Jun-20
Jul-20
Jan-21
Jun-21
Jul-21
Mar-20
Mar-21
Nov-19
Dec-19
Feb-20
Nov-20
Dec-20
Feb-21
Aug-19
Sep-19
Aug-20
Sep-20
Aug-21
Sep-21
Oct-19
Apr-20
May-20
Oct-20
Apr-21
May-21
Acute RAPPS
OFFICIAL 27
Source: Online report A076Workflow mapping showed discharge planning occurs late in
the patient’s journey “These are challenging
“Sub acute often have to be the and life changing
“Transfers and bed bearers of bad news, this conversation to have with
moves for patients with conversation should have families”
delirium and dementia started earlier ”
exacerbate symptoms”
3
1
2
Insights
1. Discharge planning for RACF occurs late in patient stay
2. Family meetings, ACAS, Neuropsychology and POA assessments
often need to occur and can be have significant waits / delays
3. Process relies on families to source and decide on a facility
“For many patients the
discharge destination is not
clear – they want the chance to
try to get home ”
OFFICIAL 28Pressure for acute beds and patient and family expectations
contribute to high unnecessary bed days
If patients require
complex discharge 1
Pressure for Acute beds
planning transfer to
Limited discharge planning subacute
in acute Opportunities:
SW cant see the patient Prioritise other patients ▪ Allow longer acute stay for patients
in acute in acute setting identified as needing RACF in acute
▪ Have conversation in acute where
2 Expectations not appropriate and complete ACAS on
High UBD for High level care at no cost communicated early to the spot in acute wards
RACF patients patient and family
in subacute
No motivating factor to ▪ Embed designated resource to
move on from GEM RACF have bad public manage patient cohort, support
perception following royal families and liaise with facilities
Once a patient in GEM must
commission
to wait for family to make
decisions about facility Challenges
Lack of awareness in 3 Patients and families
aren’t aware of Patients and families often need the
community about RACF
Families don’t have skills system
processes involved with chance to “try” and get home
securing a placement
or time to navigate RACF
Nursing home placement is a very
system Families rely heavily on difficult decision that cant be rushed,
No designated resource to SW’s who are also
4 managing an increasingly feedback from families they are often not
guide and support
demanding caseload ready to have these conversations earlier
Few facilities have
Patients with BOC memory support units
and don’t want to feel pressured.
difficult to place
Several projects already completed in the
space
RACF perceive MFW 5 Facilities may not fully
patients as difficult and understand care needs of
maybe reluctant to take patients
OFFICIAL 29Improvement action plan
▪ Acknowledge challenges, continue to engage team to understand
issues
▪ Engage leadership team and broader stakeholder group to
understand implications of longer acute length of stay
▪ Establish a cross continuum team to test and measure PDSA cycles
▪ Continue to track UBD trends across the health service
OFFICIAL 30NSW COVID-19
Care in the
Community
Amith Shetty
Clinical Director, NSW Ministry of Health
31
Classification: FOR OFFICIAL USE ONLYBackground
• In the current surge, as of 16th • On 24th June, NSW had administered
October, there have been 74919 748701 vaccine doses and as of
COVID-19 cases in NSW yesterday, 12,099,297 doses had
• 1633 ICU episodes (2.2%), been administered
• 8354 hospitalisations (11.2%), • The risk to the community has
drastically changed over the last 4
• 12353 ED episodes (16.5%),
months
• 18714 HITH episodes (25%)
• Majority of the care will continue to
• 5089 Medihotel admissions (6.8%) occur in the Community setting
and
• 24674 out of hospital (32.9%)
A tumultuous journey…
32
Classification: FOR OFFICIAL USE ONLYAction Plan and Progress
COVID-19 Care in the Virtual Care Strategy
Community teams
► LHD/ Networks teams ► Patient engagement Apps
development
. ► Virtual Accelerator
achievements.
COVID-19 Care in the
COVID-19 Care in the Community guideline ► Ambulance VCC secondary
triage
Community 7-point ► ACI/MOH/RPA virtual
partnership COVID-19 community care
action plan (Original) clinical pathways
► Paediatric Community care
guideline ► COVID-19 Proactive life
planning
COVID-19 Confirmed
Community Patient tracker ► ED / Hospital avoidance
► PFP live patient tracker ► Ambulance CCC pathway
► ROH-based risk scoring and COVID-19 mental health support
daily severity tracker
► Support resources in isolation
Care in Community Supply – Apps
Chain
► Pathway for patients with
► Modelling-informed Pulse mental illness.
oximeter/ home-monitor
procurement.
33COVID-19 Confirmed Community patient tracker
NCIIMS and Operational Data Store
NCIIMS data (PAS) linkage
feed
Demographics
Automated, real-time – data
management
DATA
PFP Iterative designing and solution delivery
MATCHING
COMMUNITY
COVID-19
Patient list State-wide, all services and
demographics
PATIENT EUID
Location and contact
Ability to share patients list and integrate
PAS Daily with VC platforms, Apps, peripherals
assessment
Risk and
Severity tracking Ability to send SMS/ e-mail notifications
Escalation and
triggers
(under development)
GEOCODING
34COVID-19
Summary
dashboard
35Key components to the strategy
Activity is monitored in real-time through our Ambulance Intensive Care Unit
Arrivals Board, and Patient Flow Portal providing visibility and (ICU)
coordination across system
► Ambulance demand ► Monitoring and coordination of ICU capacity and demand
► Transfer of Care ► Ventilator management and distribution
► Out of Hospital Care activity ► Equipment, consumables, pharmaceutical monitoring and
distribution
► Community COVID-19 cases
► ICU staff deployment
► Emergency Department activity and Short Term Escalation
Plan (STEP) ► ICU Pandemic Short Term Escalation Plan
► Hospital Activity and STEP level ► Intensive Care Advisory Service (ICAS)- virtual support
► ICU Activity and STEP level ► Temporary hospital solutions
Centralised Patient Flow Unit
36SUMMARY WORKFLOW – FUTURE STATE – PATIENT JOURNEY
Identify 1st triage Notify 2nd triage Management
LOW RISK
• < 65 years old SMS Communication
• 2 vaccinations • Nominate GP GP notify / self-care pack /
• < 0.10 ROH (or no score) • Pt Chronic Diseases escalation line
• No Chronic Diseases • Pt Symptoms
GP/PHN
Identified Chronic Diseases
and/or moderate
symptoms
MEDIUM RISK
Apps
Chronic Diseases
SMS
Moderate symptoms
Calls/Checks
Social risk factors
Virtual Care/Pulse oximetry
Covid +ve Call Patient GP/PHN/LHD
patient
Medium Risk identified
after review
HIGH RISK
• > 65 years old Medical Model
• unvaccinated Pulse oximetry
• > 0.10 ROH (any age) Virtual Care
Call Patient LHD
Age < 65, ROHAction Plan and Progress
COVID-19 Care in the Virtual Care Strategy
Community teams
► Baseline composition ► Quality safety frameworks
► Define surge and capacity
limits ► Costing and Evaluation.
► Funding models.
► Capacity and sourcing
COVID-19 Care in the COVID-19 Care in the
COVID-19 community care
Community 7-point action Community guideline
models
plan (Current) ► ACI adult V3 and Pediatric
► COVID-19 Proactive life
planning
► Co-designing healthpathways
and transition workflows
► ED / Hospital avoidance
COVID-19 Confirmed
► Post/Long- COVID
Community Patient tracker
► Transition to Primary care
► De-isolation
COVID-19 Psychosocial
► Auto-triaging for primary care
Wellbeing support
transition
► Mapping and cleansing
► Technical integration
► Redesign – central versus
Analytics-driven Supply Chain
local models
Management
► Equipment and Therapeutics.
38What could the one-system environment look like?
Regional partnerships will design and commission services appropriate for their local needs,
leveraging their existing services and providers
Notify 2nd triage Management
Collaborative Commissioned local services (PHN-LHD)
Clinical
LOW RISK
Self care information Assessment & GP led clinical
SMS Communication
• Nominate GP GP notify / self-care pack / F/U call / contact
Triage service management
• Pt Chronic Diseases escalation line Connection to GP (if
• Pt Symptoms required)
GP/PHN Outcome monitoring
Identified Chronic Diseases Escalation Patient
and/or Moderate ESCALATION / DE-ESCALATION
symptoms & transfer education &
MEDIUM RISK to acute onboarding
Apps
Chronic Diseases
Moderate symptoms
SMS care
Calls/Checks
Social risk factors
Virtual Care/Pulse oximetry
Call Patient
GP/PHN/LHD
Medium Risk identified
after review Patient
monitoring
HIGH RISK Specialist
Systems and Medical Model
Pulse oximetry Health supported Patient 7
and support
Virtual Care
Pathways telehealth
Call Patient technology LHD
enablers
LHD services Regional
providers Virtual Care,
APPs, remote
Patient Flow monitoring
24 access
Portal service
LUMOS Phone
Aged Care consults and
Community
services follow-up
care visits
PRMs* (nursing, AH,
MH, social
39
care) 39
*For further developmentThe Third COVID Wave
3000 70
60
2500
50
2000
New cases
40
Deaths 1500
30
1000
20
500
10
0 0
OFFICIALOFFICIAL
The End of a Tough Year…
Picture: Sunset over Bolte Bridge, Melbourne / DocklandsTony / creativecommons
OFFICIALQuestions
Please type your question in the chat
OFFICIALMerry Christmas/Happy New Year
This is the final COVID + Pathway Learning Network webinar for
2021. We will resume on 19 January 2022.
OFFICIALResources
1. Learning Network webinar recordings and slides
https://www.bettersafercare.vic.gov.au/support-training/learning-networks/covid-pathways
2. COVID Clinical Shared Resources SharePoint page - Secure site for sharing, with
permission, health service developed COVID-19 resources.
o To register for access and to share resources contact
centresofclinicalexcellence@safercare.vic.gov.au
3. Department of Health COVID-19 clinical guidance and resources
https://www.health.vic.gov.au/covid-19/for-health-services-and-professionals-covid-19
OFFICIALGet in contact
• Please complete our short survey
• To register for future webinars email us:
centresofclinicalexcellence@safercare.vic.gov.au
• If you have specific questions relating to the COVID+ Pathways
please email the Department of Health at
covid+pathways@health.vic.gov.au
OFFICIALYou can also read