Cost-effectiveness of Epinephrine and Dexamethasone in Children With Bronchiolitis - American Academy of Pediatrics
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
ARTICLE
Cost-effectiveness of Epinephrine and Dexamethasone
in Children With Bronchiolitis
AUTHORS: Amanda Sumner, MSc,a Douglas Coyle, PhD,b WHAT’S KNOWN ON THIS SUBJECT: Despite the large economic
Craig Mitton, PhD,c David W. Johnson, MD,d Hema Patel, burden of bronchiolitis, there have been no economic evaluations
MD, MSc,e Terry P. Klassen, MD, MSc,f Rhonda Correll, of the effectiveness of intervention with bronchodilators or
HBScN,a Serge Gouin, MD,g Maala Bhatt, MD, MSc,e Gary steroids.
Joubert, MD,h Karen J. L. Black, MD, MSc,i Troy Turner,
MD,f Sandra Whitehouse, MD, MALS,j and Amy C. Plint, MD,
WHAT THIS STUDY ADDS: Economic analysis reveals that
MSc,k for Pediatric Emergency Research Canada
treatment infants with bronchiolitis with combined epinephrine
aClinical Research Unit, Children’s Hospital of Eastern Ontario
and dexamethasone results in the lowest health care system and
Research Institute, Ottawa, Ontario, Canada; Departments of
bEpidemiology and Community Medicine and kPediatrics and societal costs.
Emergency Medicine, University of Ottawa, Ottawa, Ontario,
Canada; cHealth Studies, University of British Columbia,
Okanagan, British Columbia, Canada; Departments of
dPediatrics and Pharmacology and Therapeutics, University of
Calgary, Calgary, Alberta, Canada; eDepartment of Pediatrics,
McGill University, Montreal, Quebec, Canada; fDepartment of abstract
Pediatrics, University of Alberta, Edmonton, Alberta, Canada;
gDepartment of Pediatrics, University of Montreal, Montreal,
OBJECTIVE: Using data from the Canadian Bronchiolitis Epinephrine
Quebec, Canada; hDepartment of Pediatrics, University of Steroid Trial we assessed the cost-effectiveness of treatments with
Western Ontario, London, Ontario, Canada; Departments of epinephrine and dexamethasone for infants between 6 weeks and 12
iEmergency Medicine and Pediatrics, Dalhousie University,
months of age with bronchiolitis.
Halifax, Nova Scotia, Canada; and jDepartment of Pediatrics,
University of British Columbia, Vancouver, British Columbia, METHODS: An economic evaluation was conducted from both the soci-
Canada etal and health care system perspectives including all costs during 22
Dr Mitton’s current affiliation is Clinical Epidemiology and days after enrollment. The effectiveness of therapy was measured by
Evaluation, Vancouver Coastal Health Research Institute, School
the duration of symptoms of feeding problems, sleeping problems,
of Population and Public Health, University of British Columbia,
Vancouver, British Columbia, Canada. coughing, and noisy breathing. Comparators were nebulized epineph-
KEY WORDS rine plus oral dexamethasone, nebulized epinephrine alone, oral dexa-
children, bronchiolitis, cost-effectiveness, epinephrine, steroids, methasone alone, and no active treatment. Uncertainty around esti-
dexamethasone mates was assessed through nonparametric bootstrapping.
ABBREVIATIONS
RESULTS: The combination of nebulized epinephrine plus oral dexa-
CanBEST—Canadian Bronchiolitis Epinephrine Steroid Trial
ED—emergency department methasone was dominant over the other 3 comparators in that it was
CHEO—Children’s Hospital of Eastern Ontario both the most effective and least costly. Average societal costs were
CI—credible interval $1115 (95% credible interval [CI]: 919 –1325) for the combination ther-
www.pediatrics.org/cgi/doi/10.1542/peds.2009-3663 apy, $1210 (95% CI: 1004 –1441) for no active treatment, $1322 (95% CI:
doi:10.1542/peds.2009-3663 1093–1571) for epinephrine alone, and $1360 (95% CI: 1124 –1624) for
Accepted for publication Jul 27, 2010 dexamethasone alone. The average time to curtailment of all symp-
Address correspondence to Amy C. Plint, MD, MSc, Children’s toms was 12.1 days (95% CI: 11–13) for the combination therapy, 12.7
Hospital of Eastern Ontario, 401 Smyth Ave, Ottawa, Ontario, days (95% CI: 12–13) for no active treatment, 13.0 days (95% CI: 12–14)
Canada K1H 8L1. E-mail: plint@cheo.on.ca
for epinephrine alone, and 12.6 days (95% CI: 12–13) for dexametha-
PEDIATRICS (ISSN Numbers: Print, 0031-4005; Online, 1098-4275).
sone alone.
Copyright © 2010 by the American Academy of Pediatrics
CONCLUSION: Treating infants with bronchiolitis with a combination of
FINANCIAL DISCLOSURE: The authors have indicated they have
no financial relationships relevant to this article to disclose. nebulized epinephrine plus oral dexamethasone is the most cost-
effective treatment option, because it is the most effective in control-
ling symptoms and is associated with the least costs. Pediatrics 2010;
126:623–631
PEDIATRICS Volume 126, Number 4, October 2010 623
Downloaded from www.aappublications.org/news by guest on January 18, 2020Bronchiolitis is the most common This multicenter, double-blind, placebo- similar synergy between both epineph-
lower respiratory tract infection in the controlled trial, which enrolled 800 rine and dexamethasone and albuterol
first year of life. Although the mortality patients, was designed to determine and dexamethasone.19–21
rate is low in high-income countries, the effect of nebulized epinephrine Stemming from the CanBEST, the focus
bronchiolitis is an important illness and systemic corticosteroids in the of this study was to assess the cost-
worldwide because of the frequency treatment of outpatients with bron- effectiveness of combined treatment
that affected infants require medical chiolitis. In this trial, combined ther- with epinephrine and dexamethasone
care and hospitalization1–3 and be- apy with epinephrine and dexameth- in the treatment of outpatient infants
cause of the burden on patients and asone, as compared with placebo, with bronchiolitis.
families resulting from the length and seemed to reduce the rate of hospi-
severity of symptoms.4 The number of tal admission in the 7 days after METHODS
hospital admissions for bronchiolitis study enrollment by 9% and showed
a relative risk reduction of 35% (P ⫽ Randomized Controlled Trial
has doubled over the last 10 to 15
years in both Canada and the United .02). Also, infants treated with this This analysis is based on a double-
States.1,2 In 1996, ⬃16% of all US hos- combination seemed to have a blind randomized controlled trial of
pital admissions in the first year of life shorter length of stay, a more rapid 800 infants between 6 weeks and 12
were for bronchiolitis,1 and in 1998, an- return to quiet breathing, and months of age (median age: 5 months
nual hospital charges for respiratory greater improvement in respiratory [interquartile range: 3–7]) with bron-
syncytial virus–associated bronchioli- rate and respiratory clinical score chiolitis who were seen at participat-
tis were estimated at $365 to $691 mil- compared with those who received ing emergency departments (EDs).
lion.5 Canadian statistics show that 35 placebo. In contrast, neither epi- Patients were recruited during 3 bron-
in 1000 infants younger than 1 year are nephrine nor dexamethasone alone chiolitis seasons (December through
admitted annually with bronchiolitis, reduced the admission rate com- April) at 8 Canadian pediatric EDs from
and annual costs were conservatively pared with placebo. The CanBEST re- 2004 through 2007. All participating
estimated 15 years ago at US $18 sults suggest that the combination of hospitals were members of the re-
million.3 nebulized epinephrine and oral ste- search group Pediatric Emergency
roid treatment given to outpatients Research Canada (PERC).
Despite the large economic burden of
with bronchiolitis may reduce rates Written informed consent was ob-
bronchiolitis, only 2 economic analy-
of hospital admission and improve
ses of bronchiolitis management have tained from all parents or guardians of
some symptoms. Synergy between
been published. Respiratory syncytial included infants. The study was ap-
corticosteroids and 2-agonists has
virus immunoprophylaxis in infants at proved by Health Canada and by the
been well documented in the treat-
high risk was examined in 1 of them,6 ethics committee at each site. The re-
ment of asthma.12–16 Although various
and in the other, the utility of chest sults of the study were described
models suggest mechanisms of action
radiographs was examined.7 To our elsewhere.11
for this synergy,16,17 results of in vitro
knowledge, there have been no eco- studies of airway cells have indicated Participants were eligible for inclusion
nomic evaluations of the effectiveness that 2-adrenoceptor agonists can en- in the study if they had a score of 4 to
of bronchodilator or steroid interven- hance the ability of corticosteroids to 15 on the respiratory distress assess-
tion. As highlighted by Tugwell et al8 promote responses via the glucocorti- ment index22 and had a diagnosis of
and Hartling et al,9 economic evalua- coid receptor.18 It is important to note bronchiolitis, defined as the first epi-
tions are an essential step in the over- that these findings reveal that 2- sode of wheezing associated with
all process of establishing whether a adrenoceptor agonists are not only signs of upper respiratory tract infec-
therapy is beneficial. More specifically, steroid-sparing but also enhance the tion. Excluded infants were those who
this type of analysis establishes the maximal efficacy of the response to had received previous bronchodilator
relative efficiencies of therapies in corticosteroids to a level that cannot treatments, had previous episodes of
terms of their costs and effects and be achieved by corticosteroids alone.18 wheezing or a diagnosis of wheezing,
provides decision-makers with cost/ This effect can be said to mimic the any chronic cardiopulmonary disease,
benefit information.10 clinic observations in the context of or immunodeficiency and infants who
Recently, results of the Canadian asthma.15 In the context of wheezing in- were in severe distress.
Bronchiolitis Epinephrine Steroid fants and bronchiolitis, 3 small studies The computer-generated randomiza-
Trial (CanBEST) were published.11 in similar populations have revealed tion sequence, stratified according
624 SUMNER et al
Downloaded from www.aappublications.org/news by guest on January 18, 2020ARTICLE
to center, used randomized permuted nebulized epinephrine plus oral dexa- (and repeat ED visits), hospital admis-
blocks of 8 and 12. To conceal the allo- methasone, nebulized epinephrine sions (total cost of length of stay and
cation sequence, the pharmacy at each alone, oral dexamethasone alone, and repeat visits), investigations given in
site prepared patient packets in se- no active treatment (placebo). Pa- the hospital (blood work, cultures, vi-
quentially numbered, visually identical tients received 2 nebulized treatments, ral studies, radiographs, and proce-
packages. The active drugs and pla- administered 30 minutes apart, of 3 dures), and costs of physician assess-
cebo were identical in appearance, vol- mL of generic 1:1000 epinephrine or an ment and reassessments within the ED
ume, weight, odor, and taste. The study equivalent volume of saline. The oral and hospital stay. The prices of all
nurse was responsible for allocating treatments were 1.0 mg/kg of dexa- medications used in hospital were
patients to their treatment groups. methasone (maximum: 10 mg) or pla- taken from CHEO’s in-house pharmacy
Any child with a fever (rectal tempera- cebo given after the first nebulized and included any associated dis-
ture ⬎ 38°C) at presentation in the ED treatment in the ED followed by 5 once- counts; ED visits and hospital admis-
received 15 mg/kg of acetaminophen. daily dexamethasone doses (0.6 mg/ sions costs came from an updated
The only study to show a significant kg; maximum daily dose: 10 mg) or cost model developed for the CHEO to
benefit to dexamethasone for outpa- placebo. The dexamethasone suspen- estimate hospital costs,27 and the cost
tients with bronchiolitis8 was criticized sion consisted of generic dexametha- of assessment and reassessments
for not controlling for the antipyretic sone phosphate injection solution within the ED and hospital stay were
effect of dexamethasone.27 It was pos- mixed with Ora-Plus/Ora-Sweet (Pad- based on the Ontario physician fee
tulated that the antipyretic effect of dock Laboratories, Inc, Minneapolis, schedule.28
dexamethasone may have resulted in a MN). The oral placebo consisted of
The principal resource items of inter-
lowering of respiratory rate in chil- Ora-Plus/Ora-Sweet.
est for follow-up were visits to a health
dren in the dexamethasone group and Data Collection care provider outside of the hospital
influenced clinicians in their admis- (family physician or walk-in clinic), vis-
sion decision. As a result, the treat- Data on resource use and outcomes
its to a specialist, and medications pre-
ment of febrile infants was standard- were derived from the clinical trial.
scribed to the patients on discharge or
ized in our trial. Parents or guardians were contacted
by a health care provider. All health
by telephone using a standardized
care and specialist visits costs were
Form of Analysis telephone follow-up procedure,25,26 and
based on the Ontario physician fee
research nurses obtained data re-
A cost-effectiveness analysis was con- schedule.28 The cost of prescription
garding compliance with administra-
ducted with effectiveness measured medications was based on the Ontario
tion to study medication after dis-
as the time to resolution of individual Drug Benefit Formulary charges plus
charge, health care visits, and details
symptoms (difficulties in infant feed- about the infant’s feeding, sleep, the markup and dispensing fee.29 The
ing, sleeping, coughing, and noisy breathing, and coughing. Follow-up costs for over-the-counter medica-
breathing) and all symptoms. The per- was done daily until day 7, every 2 days tions were obtained from local phar-
spective taken for the economic evalu- until day 14, and then every 3 days until macies. All medications administered
ation was societal, and costs were day 22. A review of the patient’s hospi- in hospital or prescribed by physicians
classified as either payer (costs born tal chart was completed 22 days after were recorded by drug name, volume,
by the province) or nonpayer (costs enrollment. and units, which enabled an accurate
born by the families of children with calculation of costs for each patient.
bronchiolitis). Secondary analysis was Health Care Resource Use and A nasal pharyngeal aspirate for respi-
conducted from the health care sys- Costs ratory syncytial virus testing was ob-
tem perspective. Analysis included all Health care resource use was col- tained from each patient. Therefore, it
health care costs and costs borne by lected for all patients according to the was excluded from analysis because
the family during the 22 days after study protocol. For simplicity we based all patients received it. For any child
enrollment. all of our costs on 1 center in Ontario: with a fever (rectal temperature ⬎
the Children’s Hospital of Eastern On- 38°C) at presentation to the ED, we
Comparators tario (CHEO). The principal resource added the costs of acetaminophen (15
Treatment comparators were based items of interest were the cost of the mg/kg of body weight). All costs are
on the study treatment groups from treatment group medications, medica- presented in 2009 Canadian dollars
the clinical trial. Comparators were tions used in the hospital, ED visits (see Appendix 1; summary in Table 1).
PEDIATRICS Volume 126, Number 4, October 2010 625
Downloaded from www.aappublications.org/news by guest on January 18, 2020TABLE 1 Cost Data of bootstrapping (n ⫽ 5000). We calcu-
Item Unit cost, $ Source lated health care costs, societal costs,
ED visit 89.87 CHEO cost model27 and the duration of symptoms for each
Physician fees 15–86.90 Ontario Schedule of Benefits 200828
group, which allowed estimation of the
Hospital admission (per day) 786.87 CHEO cost model27
Investigations 1.55–105.47 Ontario Schedule of Benefits 200827 95% confidence intervals (CIs) around
Radiography 22.25–650.00 Ontario Schedule of Benefits 200827 outcomes. In addition, data from the
Cost for private car, per km 0.45 Canadian Automobile Association, bootstrapping exercise were used to
Driving costs 200830
Ambulance trip 75.00 Ontario Schedule of Benefits 200827 create a cost-effectiveness acceptabil-
Study drug 0.46 (1 mg/mL) CHEO Pharmacy ity curve,33 which provided the proba-
Oral dexamethasone (1 mg/kg) bility that each treatment was the
liquid preparation
Nebulized epinephrine (3 mL; 1:1000) 8.74 (1-mL dose) CHEO Pharmacy most cost-effective given different val-
In-hospital medication Various CHEO Pharmacy ues placed on the relief of symptoms.
Prescription medication Various Ontario Drug Formulary29 Given the stochastic nature of the data,
Over-the-counter medication Various Local pharmacies
probabilistic sensitivity analysis was
Additional details are provided in the Appendix; added to all prescription costs was an 8% markup plus a $6.41 dispensing
fee. the only sensitivity analysis conducted.
Because the purpose of an economic
evaluation is to inform decisions re-
Patient Costs cremental cost-effectiveness ratio
lated to funding of treatments, we have
The principal resource items of inter- (ICER) that corresponded to the differ-
reported estimates of the expected
est for patient costs collected within ence in costs in Canadian dollars be-
values of treatments, not statistical
the randomized controlled trial were tween treatment groups and their as- inferences.
parent or guardian’s lost wages, park- sociated time with symptoms: ICER ⫽
ing expenses, public transportation, (CA ⫺ CB)/ (EB ⫺ EA). RESULTS
ambulance cost, kilometers traveled, Uncertainty around estimates was as- The average societal cost per patient was
out-of-pocket medication, and other
sessed through probabilistic sensitiv- $1210 (95% CI: 1004–1441) for no active
out-of-pocket expenses. The cost of an
ity analysis based on nonparametric treatment, $1360 (95% CI: 1124–1624) for
ambulance was based on Ontario
bootstrapping whereby the original oral dexamethasone, $1323 (95% CI: 1093–
charges. The cost of private car travel
data were resampled to build an em- 1571)fornebulizedepinephrine,and$1115
was the product of the distance trav-
pirical estimate of the sampling distri- (95% CI: 919–1325) for the combination of
eled and national estimates of travel
bution. Bootstrapping methods as- nebulized epinephrine plus oral dexameth-
costs per kilometer.30
sumed that the empirical distribution asone (Table 2).
Analyses of the data was an adequate represen- The average cost per patient from the
All analyses were conducted in SPSS tation of the true distribution of the health care system perspective was
16.0 (SPSS Inc, Chicago, IL) and Mi- data, and statistical analysis was $1019 (95% CI: 826 –1232) for no active
crosoft Excel (Microsoft, Redmond, based on repeatedly sampling from treatment, $1140 (95% CI: 934 –1376) for
WA). If none of the therapies was the observed data.31,32 A random sam- oral dexamethasone, $1090 (95% CI:
shown to be dominant, cost- ple of each group from the original 880 –1329) for nebulized epinephrine,
effectiveness was assessed by the in- data were bootstrapped for each run and $865 (95% CI: 690 –1062) for the
TABLE 2 Average Cost per Patient/Average Length of Symptoms per Patient
Epinephrine and No Treatment Epinephrine Only Dexamethasone Only
Dexamethasone
Average health care costs per patient, $ (95% CI) 865 (690–1062) 1019 (826–1232) 1090 (880–1329) 1140 (934–1376)
Average societal costs per patient, $ (95% CI) 1115 (919–1325) 1210 (1004–1441) 1323 (1093–1571) 1360 (1124–1624)
Average length of symptom per patient, d
Feeding problems 0.62 1.26 0.992 0.55
Sleeping problems 0.89 0.997 1.04 1.03
Coughing 12.08 12.54 12.72 12.37
Noisy breathing 3.83 4.74 4.41 4.38
Any symptom (95% CI) 12.17 (11–13) 12.69 (12–13) 13.02 (12–14) 12.62 (12–13)
Societal costs include health care costs and costs to the patient and their families; the 95% CIs are based on nonparametric bootstrapping.
626 SUMNER et al
Downloaded from www.aappublications.org/news by guest on January 18, 2020ARTICLE
1.0
Epinephrine and steroid placebo
0.9
Probability treatment is cost- Effective
Bronchodilator placebo and steroid placebo
Epinephrine and dexamethasone
0.8 Bronchodilator placebo & dexamethasone
0.7
0.6
0.5
0.4
0.3
0.2
0.1
0.0
$0 $100 $200 $300 $400 $500 $600 $700 $800 $900 $1,000
Value of 1 d without symptoms
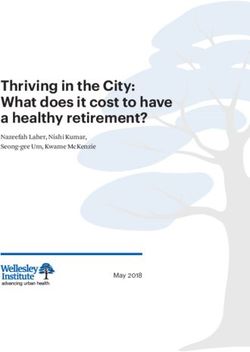
FIGURE 1
Cost-effectiveness acceptability curve.
combination of nebulized epinephrine dexamethasone was the most likely to to consider that within the clinical trial
plus oral dexamethasone (Table 2). be optimal, and the probability of being dexamethasone was not found to re-
In terms of symptoms, the longest-lasting most cost-effective was ⬎75% for all duce the hospitalization rate and only
symptom seemed to be coughing followed scenarios. shortened time to improved feeding
by noisy breathing. The average time to re- when compared with placebo.11
lief of all symptoms was 12.69 days (95% CI: DISCUSSION Economic evaluations conducted
12.00–13.00) for no active treatment, 12.62 In the CanBEST of the treatment of alongside clinical trials are often criti-
days (95% CI: 12.00–13.00) for oral dexa- acute bronchiolitis in infants between cized as not being generalizable on the
methasone, 13.02 (95% CI: 12.00–14.00) for 6 weeks and 12 months of age, com- basis that the trial does not represent
nebulized epinephrine, and 12.17 days bined therapy with epinephrine and the clinical setting in which treatments
(95% CI: 11.00–13.00) for the combination dexamethasone seemed to reduce the would be used in routine clinical prac-
of nebulized epinephrine plus oral dexa- hospital admission rate in the 7 days tice. The design of the CanBEST, as an
methasone (Table 2). after study enrollment by 35% rela- ED-based trial with broad inclusion cri-
Given the information discussed tively and 9% absolutely. In this eco- teria, minimizes this concern.
above, the combination of nebulized nomic analysis, the combination of epi- In economic evaluations, the focus is
epinephrine plus oral dexamethasone nephrine and dexamethasone was on determining the optimal treatment
was dominant over all other treatment also shown to be the most cost- regardless of statistical significance.
options, because it is both least costly effective treatment option in that it Although the results of the clinical
and most effective. In addition, no ac- was both most effective and least evaluation did not show statistical
tive treatment (ie, placebo) was domi- costly. In addition, nebulized epineph- significance for all differences, it is
nant over nebulized epinephrine. rine alone was shown to be both more still necessary to assess the cost-
The cost-effectiveness acceptability costly and no more effective than no effectiveness of the options. The prob-
curve depicts the probability that each active treatment, whereas oral dexa- ability that the combined therapy is the
of the treatment options is cost- methasone alone may be cost-effective most cost-effective treatment option is
effective for values of a day without depending on a decision-maker’s will- at least 75%, which would be consid-
symptoms, ranging from $0 to $1000 ingness to pay to avoid a symptom-day. ered sufficient to determine it to be
(Fig 1). For all values, the combination However, in considering the use of cost-effective. When using economic
of nebulized epinephrine plus oral dexamethasone alone, it is important evaluation to inform decision-making,
PEDIATRICS Volume 126, Number 4, October 2010 627
Downloaded from www.aappublications.org/news by guest on January 18, 2020it is useful to consider the concept of are optimal, which further strengthens common disease of the lower respira-
type 3 error: the probability of doing our conclusion that the combination of tory tract in the first year of life, such
the wrong thing. In the context of this nebulized epinephrine and oral dexa- savings, on a wider scale, would be sig-
study, not funding combined therapy, methasone is the most cost-effective. nificant. As well, this analysis is based
therefore, would have a type 3 error on health care costs within Canada,
CONCLUSIONS which may be lower than costs in the
rate of at least 75%. Thus, to minimize a
type 3 error, the correct funding The results of our economic analysis United States.34 At this point, the choice
choice would be to fund combined show that combined treatment of in- for decision-makers is whether to
therapy. fants with bronchiolitis with epineph- adopt this cost-effective approach now
rine and dexamethasone results in the or await stronger evidence for dexa-
Our analysis had a number of strengths. lowest health care system and societal methasone and epinephrine in the
For example, we incorporated the most costs. Examining only health care sys- treatment of bronchiolitis.
recent standards in the conduct of trial- tem costs, combination therapy re-
based economic evaluations by adopting sults in a cost savings of approxi- ACKNOWLEDGMENTS
a probabilistic approach to analyzing the mately $200 per patient compared The Canadian Institutes of Health Re-
underlying uncertainty. Such uncer- with the costs of no treatment, epi- search and the Alberta Children’s Hos-
tainty is illustrated through CIs and the nephrine alone, or dexamethasone pital Foundation funded this study. Dr
depiction of a cost-effectiveness accept- alone. Although this is not a dramatic Plint was supported by a salary award
ability curve that highlights the probabil- savings on an individual patient basis, from the Canadian Institutes of Health
ity that the various treatment options given that bronchiolitis is the most Research.
REFERENCES
1. Shay DK, Holman RC, Newman RD, Liu LL, phy in diagnosis of acute bronchiolitis. Pe- erol and Corticosteroids Establishing Ther-
Stout JW, Anderson LJ. Bronchiolitis- diatr Pulmonol. 2009;44(2):122–127 apy (FACET) International Study Group
associated hospitalizations among US chil- 8. Tugwell P, Bennett KJ, Sackett DL, Haynes [published correction appears in N Engl J
dren, 1980 –1996. JAMA. 1999;282(15): RB. The measurement iterative loop: a Med. 1998;338(2):139]. N Engl J Med. 1997;
1440 –1446 framework for the critical appraisal of 337(20):1405–1411
2. Njoo H, Pelletier L, Spika J. Infectious dis- need, benefits and costs of health inter- 14. Barnes PJ. Scientific rationale for using a
ease. In: Canadian Institute for Health Infor- ventions. J Chronic Dis. 1985;38(4): single inhaler for asthma control. Eur Re-
mation, Canadian Lung Association, Health 339 –351 spir J. 2007;29(3):587–595
Canada, Statistics Canada, eds. Respiratory 9. Hartling L, Scott-Findlay S, Johnson D, et al; 15. Giembycz MA, Kaur M, Leigh R, Newton R. A
Disease in Canada. Toronto, Ontario, Canadian Institutes for Health Research Holy Grail of asthma management: toward
Canada: Canadian Institute for Health Team in Pediatric Emergency Medicine. understanding how long-acting beta(2)-
Information; 2001:65– 87 Bridging the gap between clinical research adrenoceptor agonists enhance the clinical
3. Langley JM, Wang EEL, Law BJ, et al. Eco- and knowledge translation in pediatric efficacy of inhaled corticosteroids. Br J
nomic evaluation of respiratory syncytial vi- emergency medicine. Acad Emerg Med. Pharmacol. 2008;153(6):1090 –1104
rus infection in Canadian children: a Pediat- 2007;14(11):968 –977
16. Mak JC, Nishikawa M, Barnes PJ. Glucocor-
ric Investigators Collaborative Network on 10. Klassen TP. Economic evaluations of immu- ticosteroids increase beta 2-adrenergic re-
Infections in Canada (PICNIC) study. J Pedi- noprophylaxis in infants at high risk for re- ceptor transcription in human lung. Am J
atr. 1997;131(1):113–117 spiratory syncytial virus: shedding light or Physiol. 1995;268(1 pt 1):L41–L46
4. Plint AC, Johnson DW, Wiebe N, et al. Prac- creating confusion? Arch Pediatr Adolesc
tice variation among pediatric emergency Med. 2002;156(12):1180 –1181 17. Roth M, Johnson PR, Rudiger JJ, et al. In-
departments in the treatment of bronchioli- teraction between glucocorticoids and
11. Plint AC, Johnson DW, Patel H, et al; Pediatric
tis. Acad Emerg Med. 2004;11(4):353–360 beta2 agonists on bronchial airway
Emergency Research Canada (PERC). Epi-
smooth muscle cells through synchro-
5. Stang P, Brandenburg N, Carter B. The eco- nephrine and dexamethasone in children
nised cellular signalling. Lancet. 2002;
nomic burden of respiratory syncytial with bronchiolitis. N Engl J Med. 2009;
virus-associated bronchiolitis hospitaliza- 360(20):2079 –2089 360(9342):1293–1299
tions. Arch Pediatr Adolesc Med. 2001; 12. Greening AP, Ind PW, Northfield M, Shaw G. 18. Kaur M, Chivers JE, Giembycz MA, Newton R.
155(1):95–96 Added salmeterol versus higher-dose corti- Long-acting beta2-adrenoceptor agonists
6. Kamal-Bahl S, Doshi J, Campbell J. Eco- costeroid in asthma patients with symp- synergistically enhance glucocorticoid-
nomic analyses of respiratory syncytial vi- toms on existing inhaled corticosteroid. dependent transcription in human airway
rus immunoprophylaxis in high-risk in- Allen & Hanburys Limited UK Study Group. epithelial and smooth muscle cells. Mol
fants, a systematic review. Arch Pediatr Lancet. 1994;344(8917):219 –224 Pharmacol. 2008;73(1):203–214
Adolesc Med. 2002;156(10):1034 –1041 13. Pauwels RA, Löfdahl CG, Postma DS, et al. 19. Kuyucu S, Unal S, Kuyucu N, Yilgor E. Additive
7. Yong JH, Schuh S, Rashidi R, et al. A cost Effect of inhaled formoterol and budes- effects of dexamethasone in nebulized sal-
effectiveness analysis of omitting radiogra- onide on exacerbations of asthma. Formot- butamol or L-epinephrine treated infants
628 SUMNER et al
Downloaded from www.aappublications.org/news by guest on January 18, 2020ARTICLE
with acute bronchiolitis. Pediatr Int. 2004; 25. Patel H, Platt RW, Pekeles GS, Ducharme english/providers/program/drugs/odbf_mn.
46(5):539 –544 FM. A randomized, controlled trial of the html (search: www.healthinfo.moh.gov.on.ca/
20. Bentur L, Shoseyov D, Feigenbaum D, Gori- effectiveness of nebulized therapy with formulary). Accessed March 10, 2009
chovsky Y, Bibi H. Dexamethasone inhala- epinephrine compared with albuterol and 30. Canadian Automobile Association. Driving
tions in RSV bronchiolitis: a double-blind, saline in infants hospitalized for acute vi- costs. Available at: www.smartcommuteexpo.
placebo-controlled study. Acta Paediatr. ral bronchiolitis. J Pediatr. 2002;141(6): ca/DrivingCostsBrochure08.pdf. Accessed
818 – 824 March 10, 2009
2005;94(7):866 – 871
26. Patel H, Gouin S, Platt RW. Randomized, 31. Campbell MK, Torgerson DJ. Bootstrapping:
21. Tal A, Bavilski C, Yohai D, Bearman JE,
double-blind, placebo-controlled trial of estimating confidence intervals for cost-
Gorodischer R, Moses SW. Dexametha-
oral albuterol in infants with mild-to- effectiveness ratios. QJM. 1999;92(3):
sone and salbutamol in the treatment of
moderate acute viral bronchiolitis. J Pedi- 177–182
acute wheezing in infants. Pediatrics.
atr. 2003;142(5):509 –514 32. Glick H, Doshi JA, Sonnad SS, Polsky D. Eco-
1983;71(1):13–18
27. Gaboury I, O’Grady K, Coyle D, Le Saux N. nomic Evaluation in Clinical Trials. Oxford,
22. Lowell DI, Lister G, Von Koss H, McCarthy P. Treatment cost-effectiveness in acute otitis England: Oxford University Press; 2007
Wheezing in infants: the response to epi- media: watch-and-wait versus amoxicillin. 33. Fenwick E, Claxton K, Sculpher M. Repre-
nephrine. Pediatrics. 1987;79(6):939 –945 Paediatr Child Health. 2010; In press senting uncertainty: the role of cost-
23. Schuh S, Coates AL, Binnie R, et al. Efficacy of 28. Ministry of Health and Long-term Care. effectiveness acceptability curves. Health
oral dexamethasone in outpatients with Available at: www.health.gov.on.ca/english/ Econ. 2001;10(8):779 –787
acute bronchiolitis. J Pediatr. 2002;140(1): providers/program/ohip/sob/sob_mn. 34. Eisenberg MJ, Filion KB, Azoulay A, Brox AC,
27–32 html. Accessed March 10, 2009 Haider S, Pilote L. Outcomes and cost of cor-
24. McBride JT. Dexamethasone and bronchioli- 29. Ministry of Health and Long-term Care. On- onary artery bypass graft surgery in the
tis: a new look at an old therapy? J Pediatr. tario drug benefit formulary/comparative United States and Canada. Arch Intern Med.
2002;140(1):8 –9 drug index. Available at: www.health.gov.on.ca/ 2005;165(13):1506 –1513
PEDIATRICS Volume 126, Number 4, October 2010 629
Downloaded from www.aappublications.org/news by guest on January 18, 2020APPENDIX ED and Hospital Cost Data
Item Cost per Reference
Visit/Test, $
ED visit 89.87 CHEO
Subsequent ED visits 89.87
Comprehensive assessment and care, Monday 37.20 Ontario Schedule of Benefits 2008
through Friday, daytime (8:00 AM to 5:00 PM)
Multiple systems assessment 32.25
Reassessment and minor assessment 15.00
Comprehensive assessment and care, Monday 46.30
through Friday, evenings (5:00 PM to 12:00 AM)
Multiple systems assessment 40.10
Reassessment and minor assessment 18.70
Comprehensive assessment and care, Saturdays, 63.30
Sundays, and Holidays, daytime and evenings
Multiple systems assessment 53.80
Reassessment and minor assessment 25.50
Comprehensive assessment and care, nights 73.90
(12:00 AM to 8:00 AM)
Multiple systems assessment 62.30
Reassessment and minor assessment 29.80
Hospital admission 786.87 CHEO RIW’s
Reassessment 55.45 Ontario Schedule of Benefits 2008
Discharge day 55.45
Subsequent visits 29.20
Visit to a health care provider outside of hospital Ontario Schedule of Benefits 2008
Doctor’s visit, own doctor (limited consultation) 44.65
Walk-in clinic 44.65
Reassessment, family physician 42.35
Specialists
Neurology 82.90 Ontario Schedule of Benefits 2008
Dermatology 66.15
Radiology 82.90
Anesthesiology 103.85
Nephrology 82.90
Gastroenterology 82.90
Urology 71.30
Orthopedic surgery 71.30
Respirology 82.90
Ophthalmology 71.30
General surgery 86.90
Investigations
Blood work Ontario Schedule of Benefits 2008
Complete blood count 8.27
Reticulocyte count 6.72
Blood culture 15.51
Sickle cell screen 2.59
Hemoglobulin electrophoresis 17.58
Prothrombin time and partial thromboplastin time 13.44
Erythrocyte sedimentation rate 1.55
Serum amino acids 105.47
Bilirubin 2.59
Thyroid-stimulating hormone/thyrotropin 9.48
␥-Glutamyl transpeptidase 2.59
Aspartate aminotransferase 2.59
Alanine transaminase 2.59
Electrolytes 7.93
Urea 2.59
Creatinine 2.59
Glucose 2.59
Phosphate 2.59
Albumin 2.59
Magnesium 2.59
Transferrin 12.25
Ferritin 9.31
630 SUMNER et al
Downloaded from www.aappublications.org/news by guest on January 18, 2020ARTICLE
APPENDIX Continued
Item Cost per Reference
Visit/Test, $
Total iron-binding capacity 17.93
Calcium 2.59
Blood gas 10.54
Phenobarbital level 18.46
Urine tests
Urine routine and microscopic 2.89
Urine culture 12.93
Cultures/screening Ontario Schedule of Benefits 2008
Nasal swab for methicillin-resistant 12.93
Staphylococcus aureus
Swab for culture (eye) 12.93
Stool culture for bacteria 17.58
CSF bacterial culture (including Gram-stain) 14.48
Stool culture for rotavirus 70.00
Stool culture for vancomycin-resistant Enterococcus 12.93
Polymerase chain reaction testing for pertussis 60.00
CSF analysis Ontario Schedule of Benefits 2008
CSF cell count 9.31
CSF protein, glucose 2.59
CSF Gram-stain 2.59
Radiologic investigations Ontario Schedule of Benefits 2008
Radiograph, abdomen (ⱖ2 views) 32.90
Radiograph, soft tissue of neck (2 views) 22.25
Computed tomography of the head 650.00
Cranial ultrasound 78.95
Other investigations
Electrocardiogram 16.50
Procedure costs
Lumbar puncture 77.25
Travel-related costs
Kilometers traveled 0.45 Canadian Automobile Association,
Driving costs 2008
Ambulance 75.00 Ontario Health Insurance Plan
CSF indicates cerebrospinal fluid.
PEDIATRICS Volume 126, Number 4, October 2010 631
Downloaded from www.aappublications.org/news by guest on January 18, 2020Cost-effectiveness of Epinephrine and Dexamethasone in Children With
Bronchiolitis
Amanda Sumner, Douglas Coyle, Craig Mitton, David W. Johnson, Hema Patel, Terry
P. Klassen, Rhonda Correll, Serge Gouin, Maala Bhatt, Gary Joubert, Karen J. L.
Black, Troy Turner, Sandra Whitehouse, Amy C. Plint and for Pediatric Emergency
Research Canada
Pediatrics originally published online September 27, 2010;
Updated Information & including high resolution figures, can be found at:
Services http://pediatrics.aappublications.org/content/early/2010/09/27/peds.2
009-3663
Permissions & Licensing Information about reproducing this article in parts (figures, tables) or
in its entirety can be found online at:
http://www.aappublications.org/site/misc/Permissions.xhtml
Reprints Information about ordering reprints can be found online:
http://www.aappublications.org/site/misc/reprints.xhtml
Downloaded from www.aappublications.org/news by guest on January 18, 2020Cost-effectiveness of Epinephrine and Dexamethasone in Children With
Bronchiolitis
Amanda Sumner, Douglas Coyle, Craig Mitton, David W. Johnson, Hema Patel, Terry
P. Klassen, Rhonda Correll, Serge Gouin, Maala Bhatt, Gary Joubert, Karen J. L.
Black, Troy Turner, Sandra Whitehouse, Amy C. Plint and for Pediatric Emergency
Research Canada
Pediatrics originally published online September 27, 2010;
The online version of this article, along with updated information and services, is
located on the World Wide Web at:
http://pediatrics.aappublications.org/content/early/2010/09/27/peds.2009-3663
Pediatrics is the official journal of the American Academy of Pediatrics. A monthly publication, it
has been published continuously since 1948. Pediatrics is owned, published, and trademarked by
the American Academy of Pediatrics, 141 Northwest Point Boulevard, Elk Grove Village, Illinois,
60007. Copyright © 2010 by the American Academy of Pediatrics. All rights reserved. Print ISSN:
1073-0397.
Downloaded from www.aappublications.org/news by guest on January 18, 2020You can also read