Community Eye Health - Vision 2020
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Community Eye Health
JOURNAL
Volume 18 | Issue No.54 | June 2005 | INDIAN SUPPLEMENT - Official Publication of the “VISION 2020: The Right to Sight - India Forum”
Indian Supplement Editorial Board Published for “Vision 2020: The Right to Sight - India Forum” from
International Centre for Advancement of Rural Eye Care, L V Prasad
Dr Damodar Bachani Dr Parikshit Gogate Eye Institute, Banjara Hills, Hyderabad 500 034, India. E-mail: JCEH-
Dr GVS Murthy Dr Praveen K Nirmalan India@icare.stph.net
Dr GV Rao Dr BR Shamanna Editorial Assistance: Dr Usha Raman, Mr Sam Balasundaram,
Dr Asim Kumar Sil Ms Sarika Jain Antony
Editorial
An infrastructure model for the implemen-
tation of VISION 2020: The Right to Sight
Gullapalli N. Rao
President-elect of the International Agency for the Prevention of Blindness, L.V. Prasad Eye Institute, Hyderabad, India
Blindness is a serious public health causes of blindness, human resource including comprehensive diagnostic
problem globally. Eighty percent of this development, and development of evaluation, cataract surgical services,
problem is avoidable, i.e., either infrastructure and appropriate technology. other minor surgical procedures, low-vision
preventable or treatable; 90% of the The three components must be developed services, community-based rehabilitation
problem manifests in the developing in parallel to ensure the success of this and an eye donation centre, for a
countries of the world. Over the past 30 program. population unit of 500,000. The initial
years the magnitude of blindness has investment for such a centre in the
steadily increased, with southeast Asia One of the major limiting factors in the developing countries is US$100,000 (20¢
carrying the greatest burden combat against blindness in the per person). The staff required includes
(disproportionate to the size of its developing countries is the lack of one or two ophthalmologists supported by
population), followed by the western appropriate infrastructure for delivery of a team of 25 to 30 people to cover
Pacific region, sub-Saharan Africa, Europe, eye care. The proposed model envisages medical, administrative and other support
Eastern Mediterranean and Latin delivery of comprehensive eye care at all services. These centres may be district
American regions. The risk of blindness levels, namely, primary, secondary, tertiary hospitals in the government sector, rural
increases significantly with poverty and and advanced tertiary, through a pyramidal hospitals run by nongovernmental
older age and in women. structure. organisations or private hospitals. The idea
is to integrate all sectors of eye care
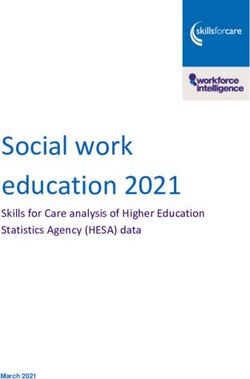
In light of these observations, all the major At the base of the pyramid are vision delivery to bring about a good public–
groups and organisations involved in the centres, which are intended to deliver private partnership for better coordination
prevention of blindness around the world primary eye care to a population unit of and more optimal use of available
realized that a major shift was warranted in 50,000. The functions at this level include resources.
the strategies to control blindness. This screening of the communities to detect
led to the development of the Global potentially blinding diseases, refraction At the third tier in the pyramid are the
Initiative for the Elimination of Avoidable and dispensing services, linkage with all training centres, one for each unit of 5
Blindness, given the name “VISION 2020: community services and appropriate million people. The main functions at this
the Right to Sight.” This is a joint referrals, both horizontally and vertically. level include secondary and basic tertiary
programme of the World Health The problems that can be handled eye care, good-quality residency training,
Organization, which represents the effectively at this level (in collaboration training of all other ophthalmic personnel,
governments of the world, and the with other local primary health care lowvision and rehabilitation services, and
International Agency for the Prevention of organisations) are refractive errors, appropriate clinical research. Essentially at
Blindness, which represents the vitamin A deficiency, trachoma and this level the problems of cataract,
international nongovernmental onchocerciasis. Based on our experience, glaucoma, diabetic retinopathy and corneal
development organisations, professional the initial capital investment required to scar can be handled along with difficult
organizations, institutions and the set up such a centre is around US$10,000 cataracts and refractive errors. The
corporate sector. The goal of this initiative (20¢ per person). The staff required is a dominant activity should be training of eye
is to control blindness and to reverse the vision technician, a high school graduate care personnel. The initial investment for
present trend of increasing global who has undergone a year of special the creation of such a centre is around
blindness. The three strategic components training. At the next level are service US$1 million (20¢ per person). This
of this programme are effective disease centres, whose main purpose is to provide tertiary level could develop on the existing
control aimed at controlling the major predominantly secondary-level eye care, base of departments of ophthalmology in
COMMUNITY EYE HEALTH JOURNAL | VOL 18 NO. 54 | JUNE 2005 S 6 1
these facilities. The main additions will be
Centres of Excellence L V Prasad Eye Institute in terms of focused training and upgrading
the facilities.
Training Centres – 5 million*
Tertiary Eye Care (Eye Hospitals/Medical Colleges) All the various centres of excellence can
then contribute to the development of
Service Centres national and regional programs where
0.5 million – 1 million* common functions, such as program
Secondary Eye Care planning, resource mobilization,
Vision Centres development of curriculum for various
50,000* training programs, distribution of
Primary Eye Care education materials, development of
Vision guardians systems and identification of appropriate
5000* research areas, can be tackled. This will
Community Eye Care
eliminate unnecessary duplication and
help avoid wasteful expenditure.
*Population
It is possible to create this model in most
developing countries with appropriate local
modifications. This then will provide the
medical schools and teaching hospitals as units is around US$10 million (20¢ per
necessary framework for the creation of a
well as tertiary care hospitals in the person). The centre of excellence will be
sustainable eye care delivery system beyond
voluntary and private sectors. staffed by the complete complement of eye
the year 2020 so that everyone in the world
care personnel to cover the entire gamut
At the apex of the pyramid are centres of has that fundamental Right to Sight.
of functions, both medical and
excellence, one for every 50 million people, nonmedical. The total initial investment in
with the functions of advanced tertiary Acknowledgements
setting up this pyramidal infrastructure is
care and new methods of treatment, This editorial was previously published in the
only 80¢ per person. With an additional
training of trainers, appropriate clinical, Saudi Journal of Ophthalmology (2004;18
cost of about 20¢ per person for the
laboratory, public health and operations [Special Issue]:3–4) and is reprinted with
training needed to make this
research, advanced management training, permission from the Saudi Ophthalmological
infrastructure functional, the total cost
low-vision rehabilitation and product Society.
per person is just around US$1. In most
development. In all these areas, service parts of the world, a sizeable portion of the An infrastructure model for the implementation
delivery, training and research will be required infrastructure already exists, and of VISION 2020: The Right to Sight, Can j
emphasized. The total cost of each of these all that is required now is upgrading of Opthalmol; 2004 Oct; 39 (6); 589-90, 593-4.
District Level Eye Care Delivery System
Harsh Goel, MS, DO Despite all these developments, quality eye of eye-care delivery. Through this system
Consultant care still remains beyond the reach of a areas which earlier did not have such
Venu Eye Institute & Research Centre, majority of rural population. In most such services/facilities have now been covered.
New Delhi areas, till recently, the mainstay of eye What follows is a description of the
care service has been through surgical and processes adopted in this endeavor.
screening eye camps. The quality of
Introduction services provided through such camps has Site Identification and Selection
The last couple of decades have been always been questionable. In order to The first step is to identify the area where
witness to tremendous developments provide quality services on a regular, the service is needed; once a site (district)
related to technology, infrastructure and permanent basis to the rural and suburban has been identified as needing service, a
service delivery in eye care globally, and population, it becomes imperative to comprehensive situational analysis is
India has not lagged behind. India can develop such facilities at the district level, done. To estimate the prevalence of
today boast of world class eye care where they can be accessed easily by the blindness and assess its various causes,
services, research and teaching and target beneficiaries. VISION 2020, the either of the following methodologies can
training facilities, as also internationally global initiative to tackle the problem of be adopted:
acclaimed eye care professionals. avoidable blindness by the year 2020,
However, in the not–too–distant past, 1. A Rapid Assessment Survey
recommends that there should be a
such facilities were concentrated in 2. Referring to a previous survey in the
secondary level eye care centre for a
metropolitan and large cities, and catered same area or in an area similar to the
population of approximately 1 million.
to a small percentage of affluent one in question, and extrapolating its
population residing in these cities; these figures to arrive at a rough estimate
Methodology 3. Organising a community-based eye
facilities were not available easily to Venu Eye Institute & Research Centre has
persons residing in rural and suburban care programme like a diagnostic/
been providing quality eye care service screening camp or primary eye care
areas, mainly due to their inaccessibility.
delivery for more than two decades, and in centre or Vision Centre
Fortunately, in recent years, a few state
the past decade, has gained valuable
capitals, industrial townships and some The last of the above listed modalities can
experience in establishing district level
district headquarters have seen the also help in assessing the level of existing
secondary eye care centres in Uttar
establishment of state–of–the–art eye eye care services in the area, their quality
Pradesh, Haryana and Rajasthan, and in
care centres. developing a successful three-tier system and their acceptance in the local
population.
S6 2 COMMUNITY EYE HEALTH JOURNAL | VOL 18 NO. 54 | JUNE 2005
Community Based Services participation by sensitizing the community How the Network develops further
Once the site has been selected and the to the problems and needs of persons with (Linkages)
problem identified, primary level disabilities, and helping in their mutual Six to seven of such district level eye
community based eye care services are integration. hospitals can be linked to a tertiary level
organized at various places in the target referral hospital for super-specialty clinical
district. This helps in identifying the Network of Diagnostic Camps and skill upgradation support. To each
pockets of high need where these activities Once the district level centre becomes such district level hospital, 3-4 primary eye
may be repeated; it also helps in functional, besides providing the regular care/Vision centres are linked. Besides
identifying the most suitable place to later OPD, IPD and surgical facilities, these primary level centres, a series of one
on establish the proposed secondary level community-based diagnostic camps are day diagnostic/screening camps are
centre. organized in a series of concentric circles, regularly organised in a designated area
starting from a radius of 20 kilometers around the hospital so as to cover a radius
from the centre, and gradually fanning out
Location of the Secondary to a maximum radius of about 45 to 50
of 35 to 50 km. This kind of networking
Level Centre between primary and secondary levels is
kilometers. This helps not only to raise equipped to tackle 95% of the eye care
The ideal location is one which is needy, awareness about the centre and its related problems at the doorstep if the
accessible from all zones of the target facilities thereby increasing its utilisation patient, who may need to approach the
district and adjoining areas, and is well by the target population, but also helps distant tertiary level centre only for 5% of
connected through public transport identify potential sites for developing his/her needs. Additional facilities listed
system. Besides these, basic civic primary eye care centres/Vision Centres. below assist in increasing uptake of these
amenities like water and electricity supply These peripheral centres, in addition to services, while the schematic diagrams
should also be available. providing primary eye care services, also given below depict the network linkages
serve as focal points for post-operative and the beneficiaries at different levels of
Basic Infrastructure care for surgical patients at their doorstep, service delivery (Fig.).
Ideally, a district level secondary eye care thereby helping ease congestion at the
centre should be a 30 to 40 bed facility hospital. As the centre develops, all its Additional Facilities/Activities
equipped to provide basic ophthalmic OPD activities are regularly monitored for Activities like community based
services and surgical facilities up to quality and viability; any primary/vision rehabilitation, school screening
cataract extraction with intraocular lens centre not proving viable is toned down to programmes and eye donation centres not
(IOL) implantation. Besides tackling act as a screening camp and newer areas only aid in increasing acceptance of the
cataract, this centre would also provide identified for additional centres.
diagnostic, therapeutic and surgical
services for other common ocular
conditions like glaucoma, entropion,
pterygium etc., and would be suitably
equipped to attend to all these problems
efficiently. The support facilities in such a
centre should include 24 hour power
backup, round the clock water supply,
hospital laundry and a hospital kitchen
capable of catering to the patients and
staff, an Optical Dispensing Unit and a
Pharmacy. The centre should also have
spacious and comfortable accommodation
for the resident team of Surgeon(s),
paramedics and support service personnel,
besides (if feasible) a dedicated mobile
unit vehicle for outreach activities.
The ideal situation is to have one’s own
building for such a centre, but this may
not always be feasible. All attempts should
be made to ultimately develop one’s own
infrastructure built according to own
specifications, with potential for future
expansion. If a local partnership is desired,
one could partner with a like-minded NGO
in the area, or a closely knit Trust with
whom an MOU can be arrived at.
Community Participation and
support
Any project designed to operate in a
community at all levels can succeed only
with local community involvement and
support. The attempt to garner this support
begins with the situational analysis.
Community based activities like
rehabilitation and eye donation
programmes help enhance community
COMMUNITY EYE HEALTH JOURNAL | VOL 18 NO. 54 | JUNE 2005 S 6 3
project in the target community, but also approximately 50-60,000
help in increasing awareness towards OPD patients and 2500 to
these issues and sensitize the community 3000 surgeries annually.
to the special needs of people with These figures are based on
incurable disabilities. Multi-disability the assumption that at
rehabilitation schemes are an add-on optimum utilization,
facility. Regular activities like public surgeries per bed per year
awareness talks for the local community should be around 100, and
and involvement of school children and a single ophthalmologist
NCC / NSS volunteers in such activities should be able to perform
helps in facilitating the bonding between around 1500 or more
the project and the local community. Super surgeries annually.
specialty consultation for conditions
related to low vision, corneal diseases, Outcome of the eye care
paediatric ophthalmic problems and service delivery in such
diabetic eye diseases are initially provided models is assessed in
terms of post operative Operation theatre in a district level hospital
in the district level centre at monthly
intervals; the frequency of such super visual gain, measured as
specialty clinics may be increased in a patients’ post operative visual acuity at a
need based fashion. specified point of time. Such medical activities like higher end surgical facilities
audits are meant to be an integral part of like phacoemulsification for cataract, a
Facility Upgradation this system, constantly monitoring the pharmacy and optical dispensing units at
With passage of time, the need to add quality of services, and up grading the secondary level hospital and Vision
more diagnostic and therapeutic facilities clinical processes and protocols. Centres help achieve sustainability.
is felt; these are added in due course of
time, and include services like YAG laser Self Sustainability Training Centres! The future . . .
unit, automated perimeters, vitrectomy Since these centres are situated in rural/ On the job skill upgradation is necessary
units, etc. In due course, different such suburban areas, a major chunk of the for development of such projects, as also
centres in contiguous (adjoining) districts clientele is usually from the weaker socio- for the morale and personal and
may be identified for development as economic strata. This segment of the professional growth of skilled personnel;
centres for super specialty care. As a population would for obvious reasons find providing these persons advanced
matter of routine, such services are it difficult to afford the cost of treatment, trainings in various fields according to
otherwise provided through the tertiary and would be provided these services at their attitude and aptitude results in such
centre which has highly skilled, dedicated subsidized rates or even free. Such a growth. Such centres later on also serve as
super specialists. scenario casts a shadow over the training centres for both in house as well
sustainability of such a venture. However, as external candidates in surgical skills,
from our experience, we have concluded community based rehabilitation concepts
that such a centre, despite treating 70% and practices etc.
patients at subsidized rates/ free, usually
breaks even financially within 3 to 5 years Conclusion
of its establishment as far as its running The methodology of establishing a district
costs are concerned. Output wise, a level eye care system connected to a
secondary level eye care centre needs to tertiary referral centre has been
perform 1500 to 2000 surgeries per successfully implemented by Venu Eye
annum to become self sustainable. In Institute & Research Centre in various
order to achieve this, one of the districts of the Northern states mentioned
methodologies adopted is of cross earlier, and is replicable and reproducible
subsidization; an example: if 25% surgical almost everywhere. This system provides a
patients pay about USD 80 or more, cost effective methodology of providing
another 50% pay subsidized price of quality eye care services at grassroots
approximately USD 22 and the rest pay level, where they are required the most,
Outpatients in a District Level Hospital nothing, even then the hospital achieves that too at very affordable costs to the
self sustainability within the time frame target population, or, quite frequently, even
Human Resources mentioned, after which the centre usually free of cost. At the same time, this system
requires only capital grants for further attains self sustainability within an
Initially, because the workload is expected
service up gradation and development. acceptable time frame. These services
to be less, the human resources dedicated
Projects situated in remote areas may then become available, accessible,
to the system would be less; two qualified
need 2-3 more years to achieve affordable and accountable, the four A’s
ophthalmologists assisted by 2-3
sustainability. Revenue generation through important for any service delivery system.
paramedics, and support staff comprising
a driver for the vehicle, a cook and
housekeeping personnel are adequate. In
initial stages, multiple roles are assigned L V Prasad Eye Institute
to the paramedics and support staff. The Hyderabad, India
team is augmented in a need -based
manner as the workload increases.
Output and Outcome Supported by ORBIS International
This model of a district level eye care
service delivery can achieve an output of
India Country Office
S6 4 COMMUNITY EYE HEALTH JOURNAL | VOL 18 NO. 54 | JUNE 2005
You can also read