(CMML) Chronic myelomonocytic leukemia - Valeria Santini MDS Unit, AOU Careggi, Università di Firenze - Studio ER ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Chronic myelomonocytic leukemia
(CMML)
Valeria Santini
MDS Unit, AOU Careggi, Università di Firenze
CMML: a hybrid disease
Clonal hematologic “overlap”disease
(MDS/MPN) characterized by myeloid
dysplasia, proliferation, and absence of
the molecular lesions BCR/ABL,
PDGFRA, PDGFRB, and FGFR1.
There are currently no FDA or EMA
approved therapies for any MDS/MPN
subtypes, except CMML-dysplastic .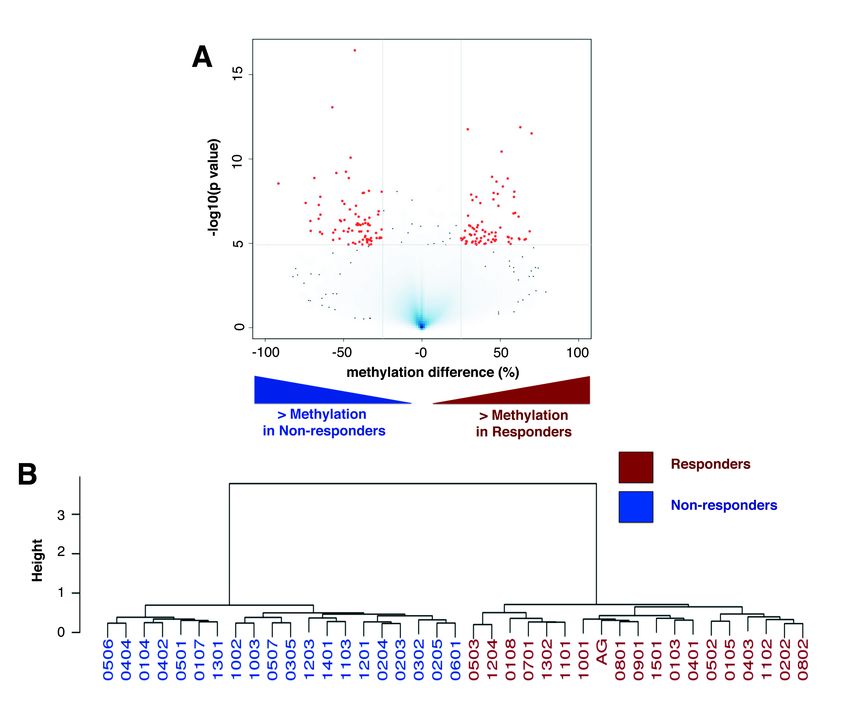
Valent P et al, Haematologica 2019
WHO 2016 classification
Blood , April 2016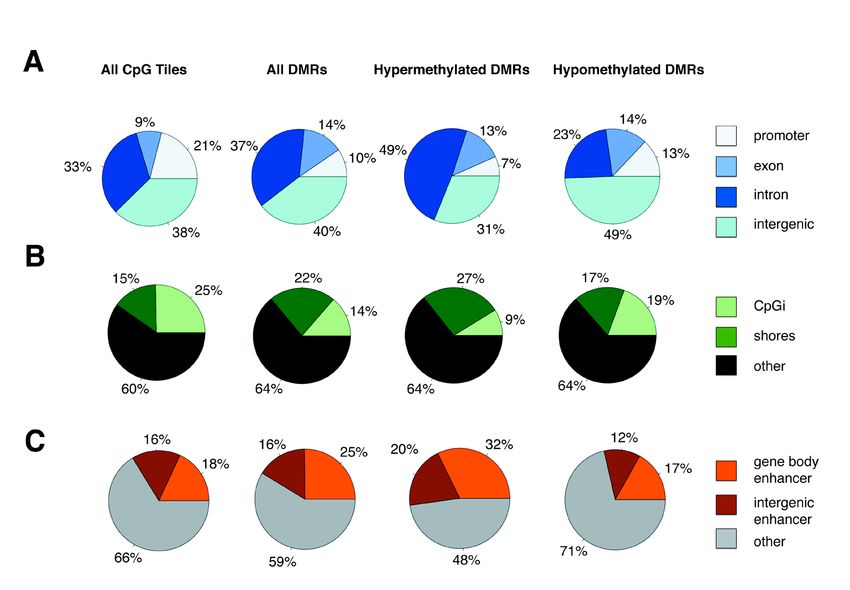
CMML: WHO2016 diagnostic criteria
Overall survival in MDS/MPN
46 mos
18 mos
13 mos
Orazi and Germing, Leukemia (2008) 22,1308-1319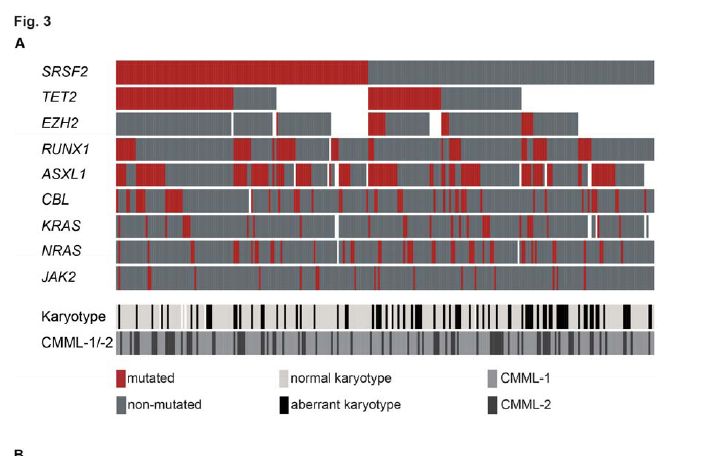
Overall survival in CMML
Median 12 mos
Onida F et al. Blood 2002;99:840-849
©2002 by American Society of Hematology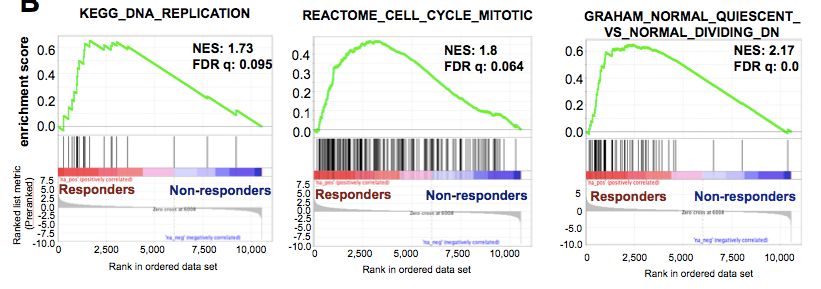
CMML Classifications… the last one
Valent P et al, Haematologica 2019
CMML Classifications… the last one
Valent P et al, Haematologica 2019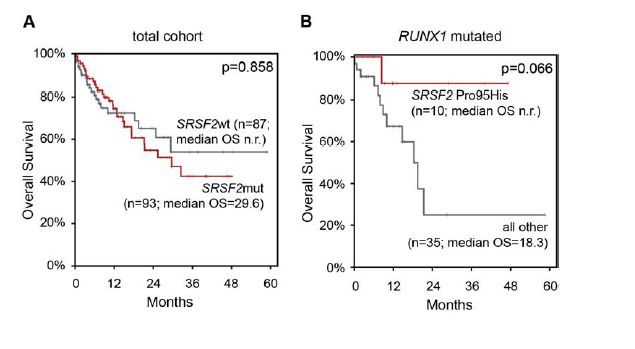
Cytogenetic classification
– Low risk: normal, -Y (unique alteration).
– High risk : +8, -7/del(7q) complex karyotype
• – Intermediate risk: everything else
Intermediate
High
Low Low 78%
Intermediate 9%
High 12%
Such et al., Haematologica 2011CMML-specific prognostic scoring
system (CPSS)
Training cohort: 558 pts (Spanish Group of Myelodysplastic Syndromes)
Validation cohort: 274 pts (Düsseldorf, Pavia)
Such et al. BloodSuch et al.,
2013; Haematologica
121(15): 2011
3005-3015Outcome of CMML pts
according to cytogenetic risk
OS Progression to AML
Probabilidad (%)
Survival
18 mos 37 mosCytogenetic risk groups are predicting
outcome in CMML MD and CMML MP
CMML-MD CMML-MP
Such et al., Haematologica 2011Molecular mutations
in CMML
GENES frequency
TET2 36 - 61%
SRSF2 28 - 47 %
ASXL1 27 - 52%
RUNX1 9 - 37%
CBL 5 - 19%
RAS 11 - 27%
EZH2 6 - 10%
JAK2 1 - 13%
DNMT3A 4 - 10%
IDH1/2 5 - 10%
SF3B1 5%
U2AF1 4 - 8%
Meggendorfer et al. Blood 2012; Grossmann et al. Leukemia 2011Prognostic relevance of different somatic
mutations
ASXL1 CBL
SRSF2
TET2
Meggendorfer et al. Blood 2012
Gelsi-Boyer et al. BJH 2010
Jankowska et al., Blood 2011
Kosmider et al.,Haematologica. 2009
Kohlmann et al, JCO 2010From www.bloodjournal.org by guest on October 4, 2016. For personal use only.
Regular Article
MYELOID NEOPLASIA
Integrating clinical features and genetic lesions in the risk assessment of
patients with chronic myelomonocytic leukemia
Chiara Elena,1,2 Anna Gallı̀,2 Esperanza Such,3 Manja Meggendorfer,4 Ulrich Germing,5 Ettore Rizzo,6 Jose Cervera,3
Elisabetta Molteni,1 Annette Fasan,4 Esther Schuler,5 Ilaria Ambaglio,2 Maria Lopez-Pavia,3 Silvia Zibellini,2
Andrea Kuendgen,5 Erica Travaglino,2 Reyes Sancho-Tello,7 Silvia Catricalà,2 Ana I. Vicente,8 Torsten Haferlach,4
Claudia Haferlach,4 Guillermo F. Sanz,3 Luca Malcovati,1,2,* and Mario Cazzola1,2,*
1
Department of Molecular Medicine, University of Pavia, Pavia, Italy; 2Department of Hematology Oncology, Istituto di Ricovero e Cura a Carattere
Scientifico Fondazione Policlinico San Matteo, Pavia, Italy; 3Department of Hematology, Hospital Universitario y Politecnico La Fe, Valencia, Spain; 4Munich
Leukemia Laboratory GmbH, Munich, Germany; 5Department of Hematology, Oncology and Clinical Immunology, University Hospital Düsseldorf,
« mutations in RUNX1, NRAS, SETBP1, and ASXL1 were
Düsseldorf, Germany; 6Department of Electrical, Computer and Biomedical Engineering, University of Pavia, Pavia, Italy; 7Department of Hematology,
Hospital Arnau de Vilanova, Valencia, Spain; and 8Department of Hematology, Hospital de La Ribera, Alzira, Spain
independently associated with overall survival (OS) »
Chronic myelomonocytic leukemia (CMML) is a myelodysplastic/myeloproliferative neo-
Key Points
plasm with variable clinical course. To predict the clinical outcome, we previously developed
• Risk assessment is crucial in a CMML-specific prognostic scoring system (CPSS) based on clinical parameters and
patients with CMML because cytogenetics. In this work, we tested the hypothesis that accounting for gene mutations
survival may range from a few would further improve risk stratification of CMML patients. We therefore sequenced
months to several years. 38 genes to explore the role of somatic mutations in disease phenotype and clinical
outcome. Overall, 199 of 214 (93%) CMML patients carried at least 1 somatic mutation.
• Integrating clinical features,
Stepwise linear regression models showed that these mutations accounted for 15% to
morphology, and genetic
24% of variability of clinical phenotype. Based on multivariable Cox regression analyses,
lesions significantly improves cytogenetic abnormalities and mutations in RUNX1, NRAS, SETBP1, and ASXL1 were
risk stratification in CMML. independently associated with overall survival (OS). Using these parameters, we defined
a genetic score that identified 4 categories with significantly different OS and cumulative
incidence of leukemic evolution. In multivariable analyses, genetic score, red blood cell transfusion dependency, white blood cell
count, and marrow blasts retained independent prognostic value. These parameters were included into a clinical/molecular CPSSOS according to Prognostic scores
including ASXL1
Molecular Mayo GFM
• Hb < 10 g/dl •Age > 65 yrs
• AMC > 10 x 109/L • Anemia (M < 10 g/dL, F < 11 d/dL)
1 .
• Circulating IMC • WBC > 15 x 109/L
• Plt < 100 x 109/L ASXL1mut (frameshift and • Platelet < 100 x 109/L
• non sense mutations only ) ASXL1 status = score 2
.8
97 mos
.6
Survival
38.5 mos
.4 59 mos
P=From www.bloodjournal.org by guest on July 7, 2015. For personal use only.
Perspectives
An international consortium proposal of uniform response criteria for
myelodysplastic/myeloproliferative neoplasms (MDS/MPN) in adults
From 1www.bloodjournal.org
Michael R. Savona, by guest
Luca Malcovati,2 Rami Komrokji, 3 on July
Ramon 7, 42015.
V. Tiu, Tariq I.For personal
Mughal, 5
Attiliouse only.
Orazi, 6
Jean-Jacques Kiladjian,7 Eric Padron,3 Eric Solary,8 Raoul Tibes,9 Raphael Itzykson,7 Mario Cazzola,2 Ruben Mesa,9
Jaroslaw Maciejewski,4 Pierre Fenaux,7 Guillermo Garcia-Manero,10 Aaron Gerds,4 Guillermo Sanz,11
BLOOD, 19 Charlotte
MARCH 2015 x VOLUME
M. Niemeyer, 12 125, NUMBER 12
Francisco Cervantes,13 Ulrich Germing,14 Nicholas C.PROPOSED
P. Cross,15 RESPONSE
and Alan F. CRITERIA
List,3 FOR MDS/MPN 1861
on behalf of the MDS/MPN International Working Group
1
Vanderbilt-Ingram Cancer Center/Vanderbilt University Medical Center, TN; 2University of Pavia and Fondazione IRCCS Policlinico San Matteo, Pavia,
Table 2. Proposed
Italy; 3H. Leecriteria for measurement
Moffitt Cancer Center, Tampa, FL; of 4
treatment
Cleveland Clinic response inInstitute,
Taussig Cancer adult Cleveland,
MDS/MPN OH; 5Tufts University Medical Center, Boston, MA;
6 7
Weill Cornell Medical College, New York, NY; Hôpital Saint-Louis, Assistance Publique – Hôpitaux de Paris, Université Paris Diderot, Paris, France;
8
CR (presenceInstitut
of allGustave
of the Roussy, Villejuif,
following France; 9Mayo Clinic Cancer Center, Scottsdale, AZ; 10MD Anderson Cancer Center, Houston, TX; 11Hospital
improvements)*
Universitario y Politecnico La Fe, Valencia, Spain; 12University of Freiburg, Germany; 13The August Pi i Sunyer Biomedical Research Institute, University
Bone marrow: #5% myeloblasts
of Barcelona, (including
Barcelona, Spain; 14 monocytic
University blast equivalent
of Düsseldorf, in case
Düsseldorf, of CMML)
Germany; with normal
and 15University maturation of
of Southampton andallWessex
cell lines and return
Regional to normal
Genetics cellularity*
Osteomyelofibrosis
Laboratory,absent or equal
Salisbury, Unitedto “mild reticulin fibrosis” (#grade 1 fibrosis)†
Kingdom
Peripheral blood‡
WBC #10 3 109 cells/L syndromes (MDS) and
Myelodysplastic is essential to identify meaningful clinical comprising laboratory and clinical experts
Hgb $11myeloproliferative
g/dL neoplasms (MPN) are and biologic end points and standardized in MDS/MPN was established involving 3
hematologically
9 diverse 9stem cell ma- response criteria for clinical trials. The independent academic MDS/MPN work-
Platelets $100 3 10 /L; #450 3 10 /L
lignancies sharing phenotypic features dual dysplastic and proliferative features shops (March 2013, December 2013, and
9
Neutrophils $1.0 3 10 /L
of both myelodysplastic syndromes and in these stem cell malignancies define their June 2014). These recommendations are
Blasts 0%myeloproliferative neoplasms. There are uniqueness and challenges. We propose the result of this collaborative project
currently no standard treatment recom- response assessment guidelines to harmo- sponsored by the MDS Foundation. (Blood.
Neutrophil precursors reduced to # 2%
mendations9 for most adult patients with nize future clinical trials with the principal 2015;125(12):1857-1865)
Monocytes #1 3 10To
MDS/MPN. /L optimize efforts to improve objective of establishing suitable treat-
Extramedullary disease: Complete
the management resolution
and disease of extramedullary
outcomes, it mentdisease present
algorithms. Anbefore therapy (eg,
international cutaneous disease, disease-related serous effusions), including
panel
palpableIntroduction
hepatosplenomegaly
Provisional category of CR with resolution of symptoms:‡ CR as described above, and complete9 resolution of disease-related symptoms as noted by the MPN-SAF TSS
Myelodysplastic/myeloproliferative neoplasms (MDS/MPN) comprise ($450 3 10 /L), megakaryocytes with myeloproliferative cytolog-
Persistent low-level dysplasia is permitted given subjectivity of assignment of dysplasia*
a World Health Organization (WHO) category of hematopoietic stem ical features, and, similar to other MDS/MPN or MPN, moderate
Complete cytogenetic sharing morphologic and hematologic features of splenomegaly.3,4 The molecular, diagnostic, and clinical features of
remission
cell malignancies
1 5
Resolution both myelodysplastic
of previously syndromes andabnormality
present chromosomal myeloproliferative neoplasms.
(known to be associatedMDS/MPN have been syndrome
with myelodysplastic, reviewed by this group elsewhere.
myeloproliferative neoplasms, or MDS/MPN), as seen
As characterized by the WHO in 2008, these disorders include chronic
on classic karyotyping with minimal of 20 metaphases or FISH§
Savona M et al; Blood 2015
Currently, few evidence-based recommendations can be made for
myelomonocytic leukemia (CMML), juvenile myelomonocytic leuke- managing patients with MDS/MPN. Overall survival is variable, mea-Therapeutic recommendations for CMML
Patnaik et al; 2016OS in CMML after allogeneic HSCT
overall according spleen size
Park S, et al., Eur J Haematol. 2013OS in CMML after therapy
AZACITIDINE
HU 20 mos 12 mos R ( 15.5)
and NR (9 mos)
VP 9 mos
DECITABINE
AZA 27.7 mos
M 18.6 mos HU 6.9 mos
Costa et al, Cancer 2011;
Wattel et al, Blood 1996
Pleyer et al., Leuk Res 2014
Braun et al., Blood 2011Low-Dose Decitabine or Azacitidine
in MDS/MPN
• Bayesian adaptive randomization: DAC vs. AZA
• Regimens:
− DAC 20 mg/m2 IV D1-3 every 4 weeks
− AZA 75 mg/m2 IV/SC D1-3 every 4 weeks
• Response assessment by modified IWG 2006
Overall DAC AZA
Jabbour et al , Blood. 2017 Sep 28;130(13):1514-1522.Santini et al; Leukemia. 2018 Feb;32(2):413-418.
Response to decitabine in CMML patients
(7% ORR in TP53 mut)
Santini et al, Leukemia 2017Overall survival according to
Response to DACMutational profiles do not correlate
with response to DAC
Omar Waab
Santini et al, Leukemia 2017
Meldi et al; J Clin Invest. 2015Distinct DNA methylation profiles at diagnosis is
associated with response to DAC
167 DMRs
ME Figueroa
Michigan University
( now Miami U )
Meldi, et al. JCI 2015Differentially methylated regions are enriched at
distal intergenic regions and enhancers
Background All DMRs HYPER HYPO
Meldi, et al. JCI 2015Differential gene expression at diagnosis associated
with response to DAC
Expression
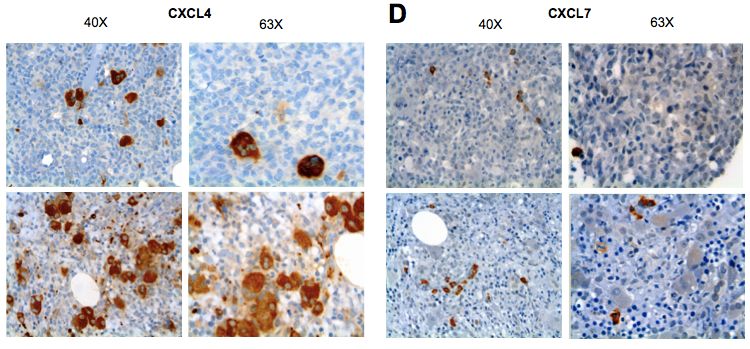
Meldi, et al. JCI 2015CXCL4 and CXCL7 are up-regulated in the bone marrow of
non-responders
Expression
CXCL4 CXCL7
R
N
R
Meldi, et al. JCI 2015Response to DAC is associated with reversal of
hypermethylation
Before DAC – After DAC
CHROMOSOMES
Non-
Responders Responders
• Loss of mC ≥ 25% after DAC
• Gain of mC ≥25% after DAC
Merlevede et al Nat Commun. 2016 Feb 24;7:10767.Response to DAC is associated with reversal
of hypermethylation
Before DAC – After DAC
CHROMOSOMES
Responders
• Loss of mC ≥ 25% after DAC
• Gain of mC ≥25% after DAC
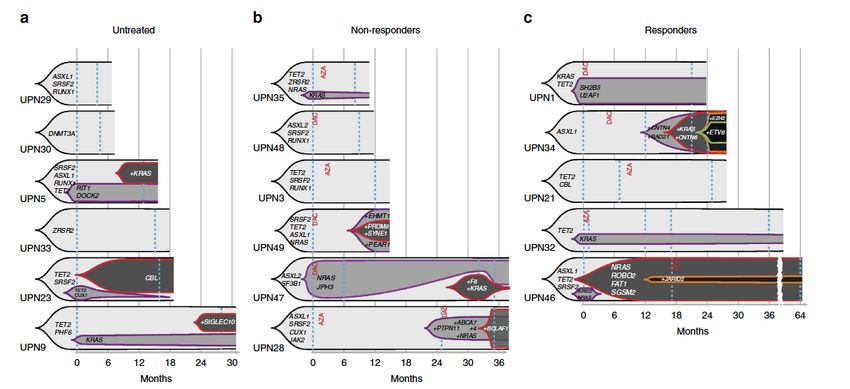
Merlevede et al Nat Commun. 2016 Feb 24;7:10767.Mutation allele burden remains
unchanged after DAC
Merlevede et al Nat Commun. 2016 Feb 24;7:10767.DACOTA trial
Primary Objective
Event free survival DAC 20 mg/m2 x 5 days
every 28 days
Patient Randomized into Study
N = 168 1:1
Minimum 6 month treatment & follow-up
HU
Patient Population:
Advanced proliferative CMML
Centrally confirmed diagnosisParticipants:
EHA CMML panel
•E Solary
•E Padron
•G F Sanz
•R Itzykson
•V Santini
•T de Witte
•U Platzbecker
•J Cortes
•A van de Loosdrecht
•F Onida
• U Germing
•D Bowen
• N Cross
•L Malcovati,
•P Fenaux, Steering Committee Chair
EHA Executive Office:
•C Smand
•G RojkováBernardino Allione
Ana Valencia Monia Lunghi
Alessandro Sanna Antonella Poloni
Valeria Santini Emanuele Angelucci
Carlo Finelli
Alessandro Levis
Omar Abdel-Wahab
Institute Gustave Roussy,
Paris
Eric Solary
Maria E.Figueroa Nathalie Droin
Tingting Qin Dorothée Selimoglu-Buet
Kristen MeldiValeria Santini UF Ematologia, Università di Firenze
You can also read

















































