CHIRURGISCHE HERZINSUFFIZIENZ-THERAPIE - Dr. med. Fabian Emrich Klinik für Thorax-, Herz- und thorakale Gefäßchirurgie Herzzentrum ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
CHIRURGISCHE HERZINSUFFIZIENZ-THERAPIE Dr. med. Fabian Emrich Klinik für Thorax-, Herz- und thorakale Gefäßchirurgie Herzzentrum, Universitätsklinikum Frankfurt
Definition der Herzinsuffizienz
„Die Unfähigkeit des Herzens, trotz eines ausreichenden
venösen Rückstroms eine für den Metabolismus der
peripheren Organe ausreichende Menge an Blut durch den
Organismus zu pumpen."
E. Braunwald, Textbook of Heart Disease.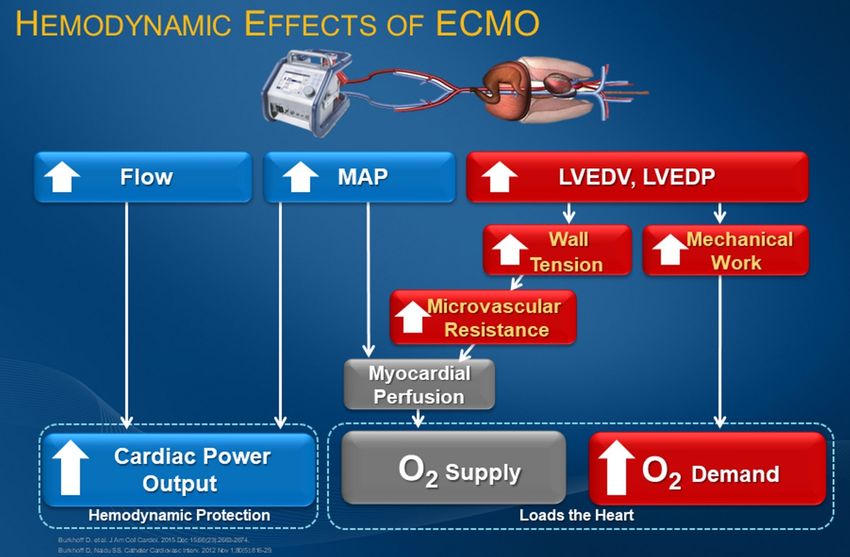
Herzinsuffizienz
Deutscher Herzbericht 2019
Chirurgische Herzinsuffizienztherapie • Optimale medikamentöse Therapie • Koronarchirurgie • Klappenchirurgie • Ventrikelrekonstruktion (Dor-Plastik) • ECMO / Impella • Assistsysteme • Herztransplantation
42 Akute Herzinsuffizienz ESC Guidelines
Management of patients with advanced heart failurea
Downloaded from https://academic.oup.com/eurheartj/advance-article/doi/10.1093/eurheartj/ehab368/6358045 by UB Frankfurt/Main user on 08 Sep
INTERMACS INTERMACS INTERMACS INTERMACS
1 2 3-4 >4 “Stable ambulatory”
Short-term MCS
BTD/BTR/BTB/BTT
(Class IIa)
Persistence of
severe brain Neurological
Cardiac,
damage and and end-organ
neurological Contraindications
severe recovered Y High riskb
and end-organ for HT
irreversible but no cardiac
end-organ
recovered
recovery
damage Y N N
Potentially
N
reversible
Y
LVAD-BTC
(Class IIa)
Contraindication
reversed
List for HT or
de-listing with Advanced HF
N Y very close therapies 2016 ESC guidelines Heart Failure, EHJ 2016; 37:2129-2200
Withdrawal of Weaning from LVAD-DT follow-up in (HT/LVAD) can
MCS support MCS support (Class IIa) case of be deferred.
meaningful Very close
improvement follow-up
(Class I)
2021 Figure
ESC 4guidelines
Algorithm for theHeart
treatmentFailure, EHJ
of patients with 2021;
advanced 00, BTB
heart failure. 1-128
= bridge to bridge; BTC = bridge to candidacy; BTD = bridge to
decision; BTR = bridge to recovery; BTT = bridge to transplantation; CA = cardiac amyloidosis; DT = destination therapy; ESC = European Society of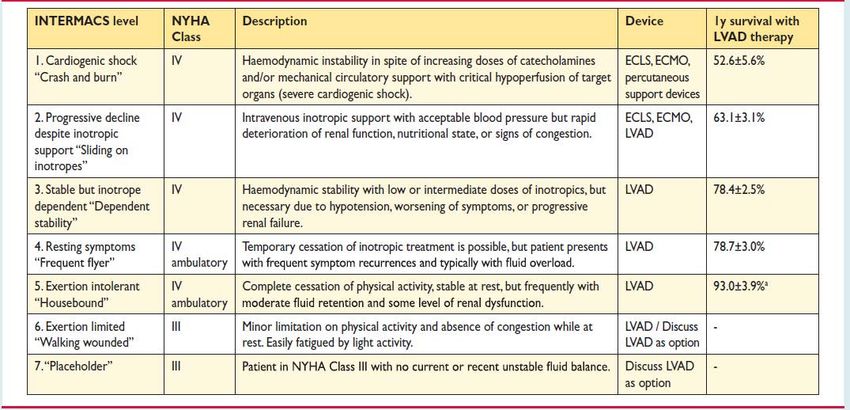
ECMO Zentrifugalpumpe + Oxygenator
ECMO
Abb. 41: Schema einer veno-arteriellen ECMO (ECLS)
37
femo-femoral axillär-femoral
https://www.researchgate.net/figure/Peripheral-veno-arterial-extracorporeal-membrane-oxygenation-with-axillary-artery_fig2_345995444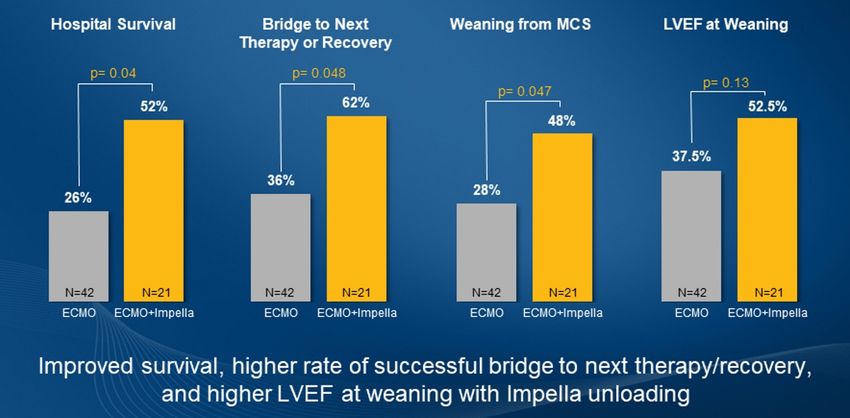
Pulmonary 33,313 22,612 67% 19,734 59%
Cardiac 32,307 19,252 59% 14,378 44%
ECPR ECMO 10,115 4,213 41% 3,030 29%
Total 151,683 105,039 69% 83,333 54%
ECLS Registry Report
Centers International Summary
April, 2021
Centers by year Report data through 2020
600 20000
Overall Outcomes
Total Runs Su
Number of Centers (red)
Number of Runs (blue)
450 Neonatal 15000
Pulmonary 33,400
Cardiac 9,561
300 ECPR 10000 2,244
Pediatric
Pulmonary 11,168
150
Cardiac 5000
13,945
ECPR 5,630
Adult
Pulmonary 33,313
0 0
1990 1991 1992 1993 1994 1995 1996 1997 1998 1999 2000 2001 2002 2003 2004 2005 2006 2007 2008 2009 2010 2011 2012 2013 2014 2015 2016 2017 2018 2019 2020
Cardiac 32,307
Centers 83 86 98 111 112 112 115 112 115 112 115 115 119 117 119 131 132 136 151 164 184 206 247 280 319 347 371 427 463 477 492
Runs 1644 1775 1932 1910 1880 1876 1868 1743 1720 1722 1862 1855 1908 1977 1928 2191 2347 2568 2804 3262 3446 4043 5155 ECPR
6208
7732 9065 10567 12810 14637 16605 16605 10,115
Total 151,683 1
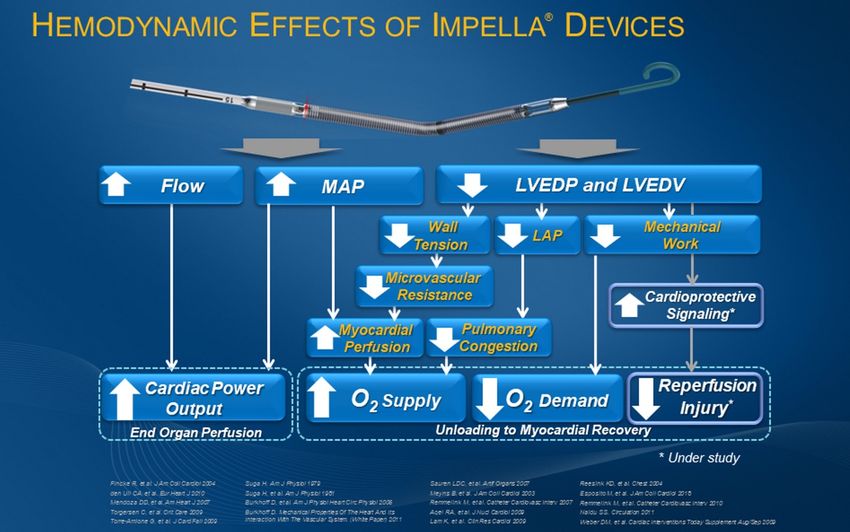
Impella®
bis zu 6 l Fluss
30 Tage zugelassen
ECMO vs. Impella
ECMO vs. Impella
ECMO vs. Impella
ECMO:
Vorteil: Oxygenator, gute RH-Entlastung
Nachteil: keine Entlastung des LV
Impella:
Vorteil: LV-Entlastung
Nachteil: keine Oxygenierung
keine RV-EntlastungECMELLA
Pappalardo et al., European Journal of Heart Failure (2017) 19, 404–412ECMELLA
Eulert-Grehn et al., The Annals of Thoracic Surgery, 2021
Volume 111, Issue 2, Pages e135-e137Chronische Herzinsuffizienz • Keine ausreichende Erholung nach ECMO oder Impella • Ischämische Kardiomyopathie (ICM) • Dilatative Kardiomyopathie (DCM)
42 Akute Herzinsuffizienz ESC Guidelines
Management of patients with advanced heart failurea
Downloaded from https://academic.oup.com/eurheartj/advance-article/doi/10.1093/eurheartj/ehab368/6358045 by UB Frankfurt/Main user on 08 Sep
INTERMACS INTERMACS INTERMACS INTERMACS
1 2 3-4 >4 “Stable ambulatory”
Short-term MCS
BTD/BTR/BTB/BTT
(Class IIa)
Persistence of
severe brain Neurological
Cardiac,
damage and and end-organ
neurological Contraindications
severe recovered Y High riskb
and end-organ for HT
irreversible but no cardiac
end-organ
recovered
recovery
damage Y N N
Potentially
N
reversible
Y
LVAD-BTC
(Class IIa)
Contraindication
reversed
List for HT or
de-listing with Advanced HF
N Y very close therapies 2016 ESC guidelines Heart Failure, EHJ 2016; 37:2129-2200
Withdrawal of Weaning from LVAD-DT follow-up in (HT/LVAD) can
MCS support MCS support (Class IIa) case of be deferred.
meaningful Very close
improvement follow-up
(Class I)
2021 Figure
ESC 4guidelines
Algorithm for theHeart
treatmentFailure, EHJ
of patients with 2021;
advanced 00, BTB
heart failure. 1-128
= bridge to bridge; BTC = bridge to candidacy; BTD = bridge to
decision; BTR = bridge to recovery; BTT = bridge to transplantation; CA = cardiac amyloidosis; DT = destination therapy; ESC = European Society ofHerztransplantation
Herztransplantation
Herztransplantation
Quelle: DSO Tätigkeitsbericht 2020Herztransplantation
84 | organtransplantation | herztransplantation
Herztransplantation
47
49 Anmeldungen und Herztransplantationen
Deutschland 2014 bis 2019 | Anzahl
DSO 330
Warteliste Herztransplantation inkl. Anmeldungen und Abgängen 700
Deutschland 2019 | Anzahl
DSO 350 600
Mit 344 Organen im Jahr 2019 stieg die Zahl der du Anmeldungen
geführten Herztransplantationen im Vergleich zum
500
559 Anmeldungen
um 26 Transplantationen. Gleichzeitig stieg die Anz
Anmeldungen zur Herztransplantation. Die Zahl der
400
Herztransplantationen
1.136 Warteliste 31.12.2019 holungsanmeldungen blieb zum Vorjahr gleich. Dies
300
stellt eine erneute Anmeldung eines bereits transpl
transplantabel 722 nicht transplantabel 414 Patienten auf der Warteliste für das gleiche Organ d
200
abb 47.
529 Abgänge 100
Die Kardiomyopathie sowie die chronische ischämi
transplantiert 344 sonstiges 84 verstorben 101 Herzkrankheit sind bei insgesamt 22 Hauptdiagnos
jahr 2014 2015 2016 2017 2018 2019
die häufigsten Indikationen, die eine Herztransplant
517 483 458 440 499 559 Anmeldungen
512 477 450 429 493 553 davon Neuanmeldungen
5 6 8 11 6 6 davon Wiederholungsanmeldungen
Quelle: Eurotransplant 304 286 297 257 318 344 Herztransplantationen
notwendig machen. Bei einem Patienten sind mehr Quelle: Eurotransplant
Quelle: DSO Tätigkeitsbericht 2020
Diagnosen möglich. Auf 525 von insgesamt 553 FäMechanische Kreislaufunterstützung
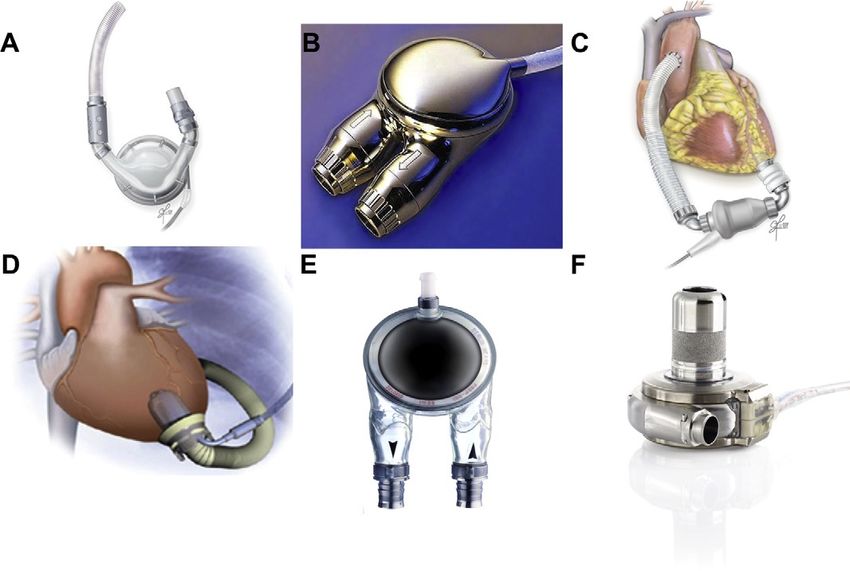
Leftventricular Assist Device (LVAD)
Leftventricular Assist Device (LVAD)
Slaughter et al, NEJM 2009:361:2241Leftventricular Assist Device (LVAD)
HeartWare Heart Mate III
21
20
llt
te
es
ng
EiLVAD-Implantation
LVAD-Implantation
Biventricular Assist Device (BVAD)
Biventricular Assist Device (BVAD)
Clinical Research in Cardiology
https://doi.org/10.1007/s00392-017-1200-4
ORIGINAL PAPER
Successful support of biventricular heart failure patients by new
EXCOR® Adult pumps with bileaflet valves: a prospective study
Bastian Schmack1 · Alexander Weymann1 · Frank Ruschitzka2 · Rüdiger Autschbach3 · Philip W. Raake4 · Clinical Research in Cardiology
Nadine Jurrmann5 · Ares K. Menon5 · Matthias Karck1 · Markus J. Wilhelm6 · Arjang Ruhparwar1
Received: 2 November 2017 / Accepted: 21 December 2017
© Springer-Verlag GmbH Germany, part of Springer Nature 2018
Abstract
Aims The Berlin Heart EXCOR® Adult biventricular assist device (BiVAD) is an approved mechanical circulatory support
for patients with end-stage biventricular heart failure. In this prospective post-market clinical follow-up study, we present
the first clinical experience of the new EXCOR® Adult pump with bileaflet (BL) valves in Europe.
Methods and results After CE-mark approval in August 2014, a total of 12 patients were enrolled with a mean age of
44 years ± 11 (range 21–58 years). The majority of patients (n = 11) were in INTERMACS level 1 or 2. Eight patients had
a median pre-operative extracorporeal life support (ECLS) of 6 days (range 1–37 days). Primary end point was survival,
either to heart transplantation (HTx), recovery or alive at 12 months on device, whichever occurred first. Secondary end
point was the number of adverse events throughout EXCOR® BiVAD support. Median support time up to last follow-up on
EXCOR® BiVAD device was 248 days (range 57–381 days) and patient survival at 1 year was 92%. Half of the EXCOR®
BiVAD patients (n = 6) were transplanted and five patients were still on support at 1 year post-implantation. Complications
during EXCOR® BiVAD support were thoracic bleeding, exit site infection and ischemic cerebrovascular incidents in three
cases, respectively.
Conclusion The new EXCOR® Adult pump with BL provides pulsatile high cardiac output with excellent outcome and
successful bridging to HTx, particularly in critically ill patients with INTERMACS level 1 or 2 at the time of implantation.
Keywords Biventricular heart failure · Ventricular assist device · Bridge to transplant
Introduction
Fig. 3 The Kaplan–Meier survival (a) and competing outcome results (b) for the patients on BIVAD support
For patients treated with ventricular assist device (VAD)LVAD als BVAD
Total Artificial Heart (TAH)
https://www.dicardiology.com/content/fda-approves-study-syncardia-total-artificial-heart-destination-therapyTotal Artificial Heart (TAH)
https://www.epo.org/news-events/events/european-inventor/finalists/2016/carpentier_de.html
Carpentier et al., The Lancet, 2015, 386 P1556-1563Chirurgische Herzinsuffizienztherapie „Chirurgische Behandlung der Herzinsuffizienz bei koronaren und strukturellen Herzerkrankungen“
Fallbeispiel 1 Koronare Herzerkrankung
• Männlich, 71 Jahre
• ICM EF 20%
• Koronare Dreigefäßerkrankung
- Z.n. NSTEMI 2008
- Z.n. PCI (90% LAD-TAXUS, 80% prox. RD1-PTCA, 75% RCA, 2/09)
- Z.n. PCI (de-novo Stenose prox. RIVA, DES 10.1.12)
- Z.n. PCI (elektiv DES RCA, 10.4.12)
• LSB
• Arterielle Hypertonie
• Persistierendes Vorhofflimmern
• EuroScore II: 3,1%Fallbeispiel 1 Koronare Herzerkrankung
What is new (20)
Recommendations for management of patients with HF and CCS
2021 HF Guidelines Class 2016 HF Guidelines Class
Coronary revascularization should be
considered to relieve persistent
Myocardial revascularization is
symptoms of angina (or an angina
recommended when angina persists
equivalent) in patients with HFrEF, CCS, IIa I
despite treatment with anti-anginal
and coronary anatomy suitable for
drugs.
revascularization, despite OMT including
anti-anginal drugs.
©ESC
2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure
www.escardio.org/guidelines (European Heart Journal 2021 – doi:10.1093/eurheartj/ehab368)Fallbeispiel 1 Koronare Herzerkrankung
Fallbeispiel 1 Koronare Herzerkrankung
ICM, EF 20%, keine relevanten KlappenvitienFallbeispiel 1 Koronare Herzerkrankung
4xOPCAB (LAD, RIM, RMS, RCA)
mit Impella 5.0 über A. axillarisFallbeispiel 1 Koronare Herzerkrankung Zweizeitige Implantation eines CRT-D Systems, EF 30-35%
Fallbeispiel 2 Koronare Herzerkrankung • Männlich, 57 Jahre • NSTEMI, ICM EF 20% • Erstdiagnose einer koronaren Dreigefäßerkrankung • MI II, TI II • Diabetes Mellitus • Nikotinabusus • Schwierige Sozialanamnese (Compliance, Sprachbarriere, kein Telefon) • EuroScore II: 7,65%
Fallbeispiel 2 Koronare Herzerkrankung
What is new (6)
Recommendations for management of patients with HF and CCS Class
CABG should be considered as the first-choice revascularization strategy, in patients
suitable for surgery, especially if they have diabetes and for those with multivessel IIa
disease.
In LVAD candidates needing coronary revascularization, CABG should be avoided, if
IIa
possible.
Coronary revascularization may be considered to improve outcomes in patients with
HFrEF, CCS, and coronary anatomy suitable for revascularization, after careful evaluation
of the individual risk to benefit ratio, including coronary anatomy (i.e. proximal stenosis IIb
>90% of large vessels, stenosis of left main or proximal LAD), comorbidities, life
expectancy, and patient’s perspectives.
PCI may be considered as alternative to CABG, based on Heart Team evaluation,
IIb
considering coronary anatomy, comorbidities, and surgical risk.
©ESC
2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure
www.escardio.org/guidelines (European Heart Journal 2021 – doi:10.1093/eurheartj/ehab368)Fallbeispiel 2 Koronare Herzerkrankung
Fallbeispiel 2 Koronare Herzerkrankung
Fallbeispiel 2 Koronare Herzerkrankung
Levosimendan Loading präoperativ
3 x OPCAB (LAD, RMS, RIVP)
Pat. in gutem AZ mit Life-Vest nach Hause entlassenFallbeispiel 2 Koronare Herzerkrankung Weiterhin reduzierte EF 20-25%, Pat. Beschwerdefrei und kompensiert, ICD-Evaluation
Fallbeispiel 3 Aortenklappenvitium
• Männlich, 59 Jahre
• Hochgradige Aortenklappenstenose mit Insuffizienz
Pmax 61 mmHG, Pmean 45 mmHG, AÖF 0.9 cm2
• EF 35%
• Arterielle Hypertonie
• Chronische Niereninsuffizienz
• COPD, Ex-Raucher
• Ausschluss KHK
• EuroScore II: 1,58%Fallbeispiel 3 Aortenklappenvitium
What is new (7)
h!
Recommendations for management of patients with HF and valvular heart disease Class
ac
Aortic valve intervention, TAVI or SAVR is recommended in patients with HF and severe
I
ro
high-gradient aortic stenosis to reduce mortality and improve symptoms.
It is recommended that the choice between TAVI and SAVR be made by the Heart Team,
pp
according to individual patient preference and features including age, surgical risk,
I
A
clinical, anatomical and procedural aspects, weighing the risks and benefits of each
approach.
m
Percutaneous edge-to-edge mitral valve repair should be considered in carefully
a
Te
selected patients with secondary mitral regurgitation, not eligible for surgery and not
needing coronary revascularization, who are symptomatic despite OMT and who fulfil
IIa
rt
criteria to achieve a reduction in HF hospitalizations.
ea
Percutaneous edge-to-edge mitral valve repair may be considered to improve symptoms
in carefully selected patients with secondary mitral regurgitation, not eligible for surgery
H
and not needing coronary revascularization, who are highly symptomatic despite OMT
IIb
©ESC
and who do not fulfil criteria for reducing HF hospitalization.
2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure
www.escardio.org/guidelines (European Heart Journal 2021 – doi:10.1093/eurheartj/ehab368)Fallbeispiel 3 Aortenklappenvitium
What is new (9)
Level of Recommended mode of intervention in patients with aortic stenosis
Data derived from multiple randomized clinical trials or meta-analyses.
evidence2017
A VHD Guidelines Class 2021 VHD Guidelines Class
SAVR
Level is
ofrecommended in patients
Data derived SAVR clinical
from aatsingle randomized is recommended
trial or largein younger
non-
low surgical
evidence B risk (STS or EuroSCORE
randomized studies. II patients who are low risk for surgeryFallbeispiel 3 Aortenklappenvitium
2018 Aortenklappenersatz
Intraoperativ, EF 10%, Kein HLM-Weaning möglich, ECMOFallbeispiel 3 Aortenklappenvitium
Fallbeispiel 3 Aortenklappenvitium
2020
2 Jahre post AKE+LVAD, Komplettes Reverse Remodeling, EF 65%Fallbeispiel 4 Mitralklappenvitium • Weiblich, 63 Jahre • DCM EF 35%, Hochgradige Mitralinsuffizienz • Z.n. CRT-Implant 2013 • Paroxysmales VHF • Z.n. mehrfacher kardialer Dekompensation
Fallbeispiel 4 Mitralklappenvitium
What is new (7)
Recommendations for management of patients with HF and valvular heart disease Class
Aortic valve intervention, TAVI or SAVR is recommended in patients with HF and severe
I
high-gradient aortic stenosis to reduce mortality and improve symptoms.
It is recommended that the choice between TAVI and SAVR be made by the Heart Team,
according to individual patient preference and features including age, surgical risk,
I
clinical, anatomical and procedural aspects, weighing the risks and benefits of each
approach.
Percutaneous edge-to-edge mitral valve repair should be considered in carefully
selected patients with secondary mitral regurgitation, not eligible for surgery and not
IIa
needing coronary revascularization, who are symptomatic despite OMT and who fulfil
criteria to achieve a reduction in HF hospitalizations.
Percutaneous edge-to-edge mitral valve repair may be considered to improve symptoms
in carefully selected patients with secondary mitral regurgitation, not eligible for surgery
IIb
and not needing coronary revascularization, who are highly symptomatic despite OMT
©ESC
and who do not fulfil criteria for reducing HF hospitalization.
2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure
www.escardio.org/guidelines (European Heart Journal 2021 – doi:10.1093/eurheartj/ehab368)Fallbeispiel 4 Mitralklappenvitium
What is new (16)
Indications
Level of for mitral valve intervention in chronic severe secondary mitral regurgitation
Data derived from multiple randomized clinical trials or meta-analyses.
evidence2017
A VHD Guidelines Class 2021 VHD Guidelines Class
Patients
Level of without concomitant coronary
Data derived from artery
a single or other
randomized cardiac
clinical trialdisease
or largerequiring
non- treatment
When revascularization
evidence B is notstudies.
randomized indicated TEER should be considered in selected
and surgical risk is not low, a symptomatic patients, not eligible for
Level of Consensus of opinion of the experts and/or small studies, retrospective
percutaneous edge-to-edge procedure surgery and fulfilling criteria suggesting
evidence C studies, registries.
may be considered in patients with an increased chance of responding to
severe secondary mitral regurgitation the therapy.
and LVEF >30% who remain IIb IIa
symptomatic despite optimal medical
management (including CRT if
indicated) and who have a suitable
©ESC/EACTS
valve morphology by
echocardiography, avoiding futility.
2021 ESC/EACTS Guidelines for the management of valvular heart disease
www.escardio.org/guidelines (European Heart Journal; 2021 – doi: 10.1093/eurheartj/ehab395; European Journal of Cardio-Thoracic Surgery; 2021 – doi: 10.1093/ejcts/ezab389)Fallbeispiel 4 Mitralklappenvitium
What is new (17)
Indications
Level of for mitral valve intervention in chronic severe secondary mitral regurgitation
Data derived from multiple randomized clinical trials or meta-analyses.
evidence2017
A VHD Guidelines Class 2021 VHD Guidelines Class
Patients
Level of without concomitant coronary
Data derived from artery
a single or other
randomized cardiac
clinical trialdisease
or largerequiring
non- treatment
Inevidence
patientsB with severe
randomized
SMR andstudies.
LVEF In high-risk symptomatic patients notFallbeispiel 4 Mitralklappenvitium
2015
Hochgradige Mitralklappeninsuffizienz, EF 35%Fallbeispiel 4 Mitralklappenvitium
Fallbeispiel 4 Mitralklappenvitium
Pat. im Follow-Up in klinisch
sehr gutem Zustand mit
subjektiv guter LebensqualitätIndikationen zur LVAD-Implantation
European Journal of Heart Failure (2018) 20, 152–160 RESEARCH ARTICLE
doi:10.1002/ejhf.975
Screening for heart transplantation and left
ventricular assist system: results from
the ScrEEning for advanced Heart Failure
treatment (SEE-HF) study
Lars H. Lund1,2*†, Jean-Noel Trochu3†, Bart Meyns4, Kadir Caliskan5, Steven Shaw6,
Jan D. Schmitto7, David Schibilsky8, Laura Damme9†, Jerry Heatley9, and
Finn Gustafsson10†
1 Department of Medicine, Karolinska Institutet, Stockholm, Sweden; 2 Department of Cardiology, Karolinska University Hospital, Stockholm, Sweden; 3 Institut du Thorax, Inserm
UMR 1087-CIC1413, Centre Hospitalier Universaire de Nantes, Nantes, France; 4 UZ Leuven, Leuven, Belgium; 5 Erasmus MC University Medical Center, Rotterdam, The
Netherlands; 6 University Hospital of S. Manchester NHS Trust, Manchester, UK; 7 Department of Cardiac, Thoracic, Transplantation and Vascular Surgery, Hannover Medical
School, Hannover, Germany; 8 German Heart Competance Center, University Clinical Center Tuebingen, Tuebingen, Germany; 9 St Jude Medical, Minneapolis, MN, USA; and
10 Department of Cardiology, Copenhagen University Hospital Rigshospitalet, Copenhagen, Denmark
Received 12 April 2017; revised 22 July 2017; accepted 25 July 2017 ; online publish-ahead-of-print 27 September 2017
Background
Patients with CRT and/or ICD + NYHA III-IV + EFFrühzeitige Patienten-Identifikation Klinische Zeichen die zu einer LVAD-Evaluation führen sollten: • Hospitalisation innerhalb von 6 Monaten ohne reversiblen Grund • End-Organ Dysfunktion (meist renal, aber auch hepatisch und cerebral) • Intoleranz gegenüber ACE-Inh., Sartan, Betablocker, etc. (Hypotension) • Hoch-Dosis Diuretika • Rhythmusstörungen / Defibrillatorschocks • Inotropikabedarf • Verschlechterung der RH-Funktion
Zeitpunkt der LVAD Implantation
Hospitalizations because of heart failure
reduce the lifetime
deco
mpe
nsat
ions
Median survival (years)
Cardiac output
Massie BM, Am Heart J 1997; 133: 703–712 Modified from:
Boyko WL, AM Heart J 1999; 137: 115–119 Gheorghiade et al, Am J Cardiol 2005
Setoguchi S et al, Am Heart J 2007Zeitpunkt der LVAD Implantation
Katherine Lietz, 2008Zeitpunkt
O U T C O M E Cder
L I N I CLVAD
A L P R O FImplantation
ILE
Kirklin JK et al. J Heart Lung Transplant 2017Survival
Quelle: Kirklin et al., J Heart Lung Transplant 2018;37:685-691Quality of Life
NYHA-Stadium 6-min Gehtest
Krabatsch T et al. J Cardiothorac Surg. 2017 Apr 4;12(1):23.39
,
..
Home Monitoring
Thus, non-invasive HTM may be considered for patients with HF
..
s .. in order to reduce the risk of recurrent CV and HF hospitalizations
..
r .. and CV death; further evidence on management guided by implanted
- .. systems is awaited.374
..
, ..
Downloaded from https://academic.oup.com/eurheartj/advance-article/doi/10.1093/eur
- ...
- .. Recommendations for telemonitoring Connecting patient & physician
..
e ..
.. Recommendations Classa Levelb
..
e .. Non-invasive HTM may be considered for
, ..
.. patients with HF in order to reduce the risk of augmented
, .. recurrent CV and HF hospitalizations and CV IIb B
g ..
.. death. 374
- ..
.
.. Monitoring of pulmonary artery pressure using a intelligence
.. wireless haemodynamic monitoring system may
e ..
.. be considered in symptomatic patients with IIb B
ESC 2021
t .. HFrEF (LVEFVielen Dank! fabian.emrich@kgu.de
You can also read

















































