Child Torture as a Form of Child Abuse - Alaska Children's ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Journ Child Adol Trauma
DOI 10.1007/s40653-014-0009-9
ORIGINAL ARTICLE
Child Torture as a Form of Child Abuse
Barbara L. Knox & Suzanne P. Starling & Kenneth W. Feldman &
Nancy D. Kellogg & Lori D. Frasier & Suzanna L. Tiapula
# Springer International Publishing 2014
Abstract This paper describes clinical findings and case Ninety-three percent of children were beaten and exhibited
characteristics of children who are victims of severe and cutaneous injury; 21 % had fractures. There were 25 victims
multiple forms of abuse; and proposes clinical criteria that of isolation (89 %), as well as 61 % who were physically
indicate child abuse by torture. Medical records, investigation restrained and 89 % who were restricted from food or water.
records, and transcripts of testimony regarding a non- All of the children were victims of psychological maltreat-
consecutive case series of 28 children with evidence of phys- ment; 75 % were terrorized through threats of harm or death to
ical abuse, neglect, and psychological maltreatment, such as themselves or loved ones and 54 % were degraded and/or
terrorizing and isolation, were reviewed for types of injuries, rejected by caregivers. Nearly all children were medically
duration of maltreatment, medical and physical neglect, social neglected. Half had a history of prior referrals to CPS. The
and family history, and history of prior Child Protective children in this case series were physically abused, isolated,
Services (CPS) involvement. The median age was 7.5 years deprived of basic necessities, terrorized, and neglected. We
(9 months to 14.3 years). Thirty-six percent died. Duration of define child torture as a longitudinal experience characterized
abuse ranged from 3.5 months to 8 years (median 3 years). by at least two physical assaults or one extended assault, two
or more forms of psychological maltreatment, and neglect
resulting in prolonged suffering, permanent disfigurement or
B. L. Knox (*) dysfunction, or death.
Department of Pediatrics, University of Wisconsin School of
Medicine and Public Health, American Family Children’s Hospital,
600 Highland Ave, H4/428 Clinical Science Center, Madison, Keywords Non-accidental trauma . Physical abuse .
WI 53792-4108, USA Psychological maltreatment . Neglect . Starvation
e-mail: blknox@pediatrics.wisc.edu
S. P. Starling
Child abuse pediatrics is an evolving field. Prior to Dr. C.
Eastern Virginia Medical School, Children’s Hospital
of The King’s Daughters, Norfolk, VA, USA Henry Kempe and colleagues analyzing and defining Battered
Child Syndrome in 1962 as physically abusive injuries to one
K. W. Feldman or more body systems culminating in serious injury or death
University of Washington, and Seattle Children’s
Hospital, Seattle, WA, USA
(Kempe et al. 1962) these cases were not recognized or, if
diagnosed, mishandled by the physician. Kempe’s legacy has
N. D. Kellogg been to reshape our understanding of child maltreatment. Due
University of Texas Health Science Center in part to this seminal article, physical abuse of children is now
at San Antonio, San Antonio, TX, USA
diagnosed by clinicians, investigated by social services, and
L. D. Frasier prosecuted in courts. The description of Battered Child
Primary Children’s Medical Center, Syndrome addressed system-wide failures to recognize child
University of Utah, Salt Lake City, UT, USA maltreatment.
As the years progressed, other subcategories of child abuse
S. L. Tiapula
National Center for Prosecution of Child Abuse, emerged including sexual abuse (Kempe 1978), neglect
Alexandria, VA, USA (Cantwell 1980), emotional abuse (Hart et al. 2011; Hibbard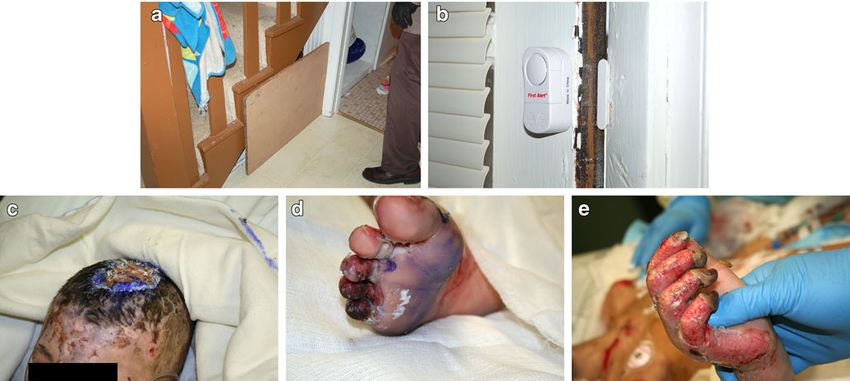
Journ Child Adol Trauma
et al. 2012), abusive head trauma (Christian et al. 2009), victim (Stover and Nightingale 1985), inflict severe pain and
medical child abuse (Roesler and Jenny 2009; Rosenberg suffering, to behave systematically and with purpose, and
1987; Stirling and American Academy of Pediatrics continue or repeat the behaviors over time (Allasio and
Committee on Child Abuse and Neglect 2007), and intention- Fischer 1998). Stover and Nightingale (1985) state:
al child starvation (Kellogg and Lukefahr 2005). Each identi-
fied subcategory of child maltreatment included unique clin- The purpose of torture is to break the will of the victim
ical features which required specific child assessment, diag- and ultimately to break his or her humanity…through
nostic, and treatment approaches. infliction of severe or acute physical pain and mental
Torture is different from other forms of child abuse, but it suffering…and requires that the torturer exert physical
currently lacks medical definitional criteria. As opposed to control over his or her victim. (p. 4–5)
torture, the majority of commonly recognized physically abu-
Campbell (2007) adds: “The act of torture is carried out for
sive acts result from a caregiver’s episodic unchecked anger or
the purpose of physically and psychologically ‘breaking’ an
loss of self-control. Torture is usually prolonged or repeated
individual” (p. 633). Children also have been documented
and includes acts designed to establish the perpetrator’s dom-
victims of political torture (Cohn et al. 1981; den Otter et al.
ination and control over the child’s psyche, actions and access
2013; Green 2007; Welsh 2000). However, descriptions of
to the necessities of life. It employed elements of both physical
manifestations and definitions specific to intra-familial torture,
abuse and psychological cruelty. According to Knox and
without political purpose, have not been described (Allasio
Starling (2012), 1 to 2 % of children being evaluated for abuse
and Fischer 1998; Tournel et al. 2006).
present with such a unique constellation of physical and
psychological injuries which appears to represent torture.
Recognition and management of these cases is problematic
at multiple levels, including medical care, interventions by Exemplary Case Series of Child Abuse Torture
Child Protective Services (CPS), and prosecution by the legal
system. A recent literature review and commentary notes the The goal of this case series is to exemplify and thus define
lack of a formal medical definition of torture in the context of child torture within the context of physical and psychological
child abuse (den Otter et al. 2013); this lack of a definition maltreatment inflicted on children by their caretakers. We
may have reduced the ability of medical and legal authorities sought to identify medical criteria distinguishing these cases
to effectively recognize and address this problem. Although from other forms of child abuse and present reasons for
torture has been described in the context of politically moti- creating a new subcategory of child maltreatment. This case
vated abuse, the torture of children within a familial context series also examines perpetrator characteristics and their
has received little attention. Review of the medical literature implications.
yielded only two isolated case reports of torture that were not
politically motivated (Allasio and Fischer 1998; Tournel et al.
2006). Methods
Child abuse pediatricians from five U.S. medical centers
Definitions of Torture selected cases they considered to represent child torture. The
sites spanned the country, including Virginia, Texas,
Historically, torture in the context of politically or militarily Wisconsin, Utah, and Washington State. These cases included
motivated conduct, often by state actors, is a means of a combination of severe physical and psychological maltreat-
extracting information or controlling populations through in- ment that occurred repeatedly and caused severe physical and
timidation and repression (Stover and Nightingale 1985). psychological injury. This non-consecutive series included
Definitions of torture have been proposed by Amnesty children between ages 9 months and 15-years-old evaluated
International (1975), the World Medical Association (1975), between January 1, 1995 and August 31, 2012. They did not
and the United Nations Convention Against Torture and Other represent all potential cases from any institution. The medical
Cruel, Inhuman, or Degrading Treatment or Punishment records were abstracted for age, sex, relationship to perpetra-
(Burgers and Danelius 1988) to address politically motivated tor, details of the child’s physical and psychological injuries,
conduct and the medical community’s response to torture. reported methods of abuse, the child’s abuse disclosures, the
These definitions include two key components: (1) intentional duration of abuse, and outcomes of the case. Six major types
infliction of severe pain and suffering without regard to the of psychological maltreatment identified for abstraction in-
extent of injury, and (2) for the purpose of obtaining submis- cluded spurning (the emotional rejection/denigration of a
sion or dehumanization. Definitions of political torture gener- child), terrorizing, isolating, exploiting/corrupting, denying
ally require that perpetrators have physical control over the emotional responsiveness, and mental health/medical/Journ Child Adol Trauma
educational neglect (Hart et al. 2011; Hibbard et al. 2012). removed under the auspice of “homeschooling.” This
Cases involving primarily sexual torture were excluded from “homeschooling” appears to have been designed to further
this study based on the authors’ experience that the perpetra- isolate the child and typically occurred after closure of a
tor(s) motivation and relationship to the child were qualita- previously opened CPS case. Review of these cases found
tively different. no true educational efforts were provided to the homeschooled
The Institutional Review Boards (IRB) of the University of children. Their isolation was accompanied by an escalation of
Wisconsin School of Medicine and Public Health and Eastern physically abusive events.
Virginia Medical School approved this study prior to data Every child included in the study was victim of several of
collection. The University of Wisconsin Health Sciences the six major types of psychological maltreatment (as listed in
IRB served as the IRB of record for Seattle Children’s the methodology section). Most of the children were denied
Hospital and the National Center for the Prosecution of emotional responsiveness, in which the caregiver ignored the
Child Abuse. The remainder of the institutions participating child’s attempts and need for social interaction (den Otter et al.
in this study exempted the research. 2013). Threats of death were made to 32 % of the children. Of
known mental health outcomes for the surviving children,
post-traumatic stress disorder (PTSD) was the most common
Results mental health condition.
Half of all cases reviewed had a prior history of 1 to 15
Twenty-eight cases of extreme child abuse were identified. referrals and/or investigations by CPS. These prior CPS refer-
The children’s median age was 7.5 years (range = 9 months- rals had been investigated for intentional food/fluid restriction,
14.5 years). Abuse duration ranged from 3.5 months to 8 years lack of supervision, physical abuse, and neglect. CPS workers
(median = 3 years). Eleven (39 %) children were male and 17 often accepted the caretaker(s) attribution that the child was
(61 %) female. Twelve children were Caucasian (43 %), 10 emotionally/behaviorally disturbed or had an eating disorder.
(36 %) African American, and six (21 %) were Hispanic. If the CPS worker recognized the child to be malnourished,
Forty-five percent of the victims’ siblings had been coerced he/she accepted the caretaker’s agreement to feed the child
into participation in the torture and 65 % of siblings were and closed the case without follow-up.
abuse victims themselves. Ages, physical injuries/outcomes, A clear timeline of abuse could not be established in all
reported methods of torture, and perpetrator(s) for each case cases. However, for cases in which the timeline was known,
are presented in Table 1. Figures 1 and 2, and their individual the shortest period of time between onset of torture and
case data in Table 1 document the abuse of two children and recognition and intervention was 3.5 months, while the lon-
their injury environments. gest period was 8 years. Twenty of 51 perpetrators were either
All study children in this case series were subjected to more biologic mother or father (39.2 %). Females (31 total) were
than one form of egregious physical abuse and neglect, and among the perpetrators in every case. Twelve female perpe-
most children were deprived of basic necessities of life trators were biologic mothers (38.7 %). Stepmothers or girl-
(Table 2). Ninety-three percent of children had cutaneous friends constituted 19.4 %, as did adoptive mothers. Other
evidence of physical abuse at the time of medical intervention female relatives (12.9 %, 4) and unrelated females (9.7 %, 3)
or death. Sixty-one percent had been physically restrained by were also perpetrators. Among the 20 male perpetrators, eight
binding. Ninety-three percent of children had been beaten and (40 %) were the biologic father, five (25 %) were stepfather or
21 % had fractures. They received no medical care for their mother’s boyfriend, four (20 %) were adoptive fathers, one
physical injuries. The fatality rate was high at 36 % (10/28). (5 %) was another relative, and two (10 %) were unrelated
Table 3 lists types of psychological abuse(s) and neglect of males. For all cases, all adults in the home knew of this
child victims. Eighty-nine percent experienced food depriva- extreme abuse and participated to some extent in abusive acts.
tion and 79 % were fluid restricted. Sixty-four percent were Unlike other forms of abuse, most perpetrators of torture
restricted in the performance of normal bodily functions, partially confessed to their crimes; however, they significantly
including toilet access for urination and defecation. The ma- minimized or rationalized their individual involvement.
jority of children (89 %) were isolated from people outside the
immediate family; 75 % experienced solitary confinement. Individual Detailed Case Report
For over half, few individuals outside the abuser(s) knew of
the child’s existence. This social isolation typically involved A 14-year-old girl came to the attention of a county social
preventing the child from attending school or daycare. worker who was notified that the child and her siblings had
Twenty-nine percent of school-age children were not allowed not been attending school. The social worker asked to see the
to attend school; two children, though previous enrolled, were children and was told by their father that they were sleeping.
dis-enrolled by their caregiver and received no further school- The worker was eventually allowed into the bedroom where
ing. An additional 47 % who had been enrolled in school were she found the girl and her 8 and 5-year-old siblings hiding inTable 1 Physical injuries/outcomes, reported methods of torture, and perpetrator(s)
Age/sex Physical injury Outcome Reported methods of torture Perpetrator(s)
9 m (a) female Starvation; dehydration; contractures Survived with severe developmental Starved; physically restrained; forced to watch parents Mother & father
Sibling to 9 m (b) case of knees and hips delay and physical disability eat; left home alone for extended periods
9 m (b) female Starvation; dehydration; contractures Died Presented dead on arrival to hospital; starved; physically Mother & father
Sibling to 9 m (a) case of knees and hips restrained; forced to watch parents eat; left home
alone for extended periods
2y 4 m female Bilateral periorbital burns with infection; Survived Chemical burn & blunt trauma to the eyes; blunt trauma Mother’s boyfriend & mother
vitreous hemorrhage; head &facial to the head & teeth; cuts inflicted by a sharp object;
bruising/lacerations; hair loss; dental squeezing & striking of hands; hair pulling
trauma & avulsed teeth; multiple hand
& finger fractures & lacerations
2y 5 m male Patterned bruises/abrasions face & trunk; Died Presented dead on arrival to hospital; multiple beatings Mother’s boyfriend & mother
liver & pancreas laceration; right lung over several weeks witnessed by multiple adults;
contusion & pseudocyst; rib fractures; taunted by dangling him over an angry dog
torn upper labial frenulum; cardiac &
diaphragmatic bruising
2y 6 m female Abusive head trauma & fluid deprivation Survived with partial blindness Multiple witnessed beatings; witnessed being held up Mother’s boyfriend
resulting in SDHa; cerebral venous and severe PTSDb while struck in the abdomen; forced to sit immobile
sinus thrombosis & prolonged coma; under heat lamps for prolonged periods; denied fluids;
lacerations/bruises face & head; regularly threatened, cursed, & denigrated
patterned scars over body; hand burn
2y 10 m male Starvation; dehydration with Survived Starved; physically restrained; locked in bathroom; left Father & father’s girlfriend
hypernatremia; bruises/abrasions alone for extended periods; beaten with a brush & belts
head and chest; patterned injury on
trunk & extremities; pressure
ulceration of extremities
4y 0 m male Strangulation-related neck bruises; Survived Starved; locked in a clothes dryer & tumbled; submerged Mother
truncal bruising; genital injury in freezing water; forced to lick a 9v battery; locked in
closet & end table while siblings taunted him; struck
with hands & objects
4y 1 m male Retinal hemorrhage & optic nerve sheath Died Found buried in a shallow grave; isolated in house; Paternal aunt & paternal
hemorrhage; Impact subgaleal burned; beaten; shaken; no medical care for aunt’s boyfriend
hemorrhage; acute SDH; scleral 4 days; neck snapped
hemorrhage; fracture of T1 spine;
liver laceration; healing deep partial
thickness burns to buttocks, ear, &
hands (covered in duct tape); bruises/
abrasions to trunk & head
4y 4 m male Old subdural hematomas at autopsy; recent Died Found dead at home; starved; physically restrained; Paternal grandmother
impact trauma to scalp; physical signs of beaten; spurned
starvation
4y 6 m female Abusive head trauma; 50 % TBSAc acute Died Found dead in bathtub with extensive burns over lower Maternal aunt & maternal uncle
immersion burns; patterned facial body; older scalp burn treated with alcohol/ulcerating;
contact burns; ulcerating scalp scald whipped on soles of feet with a belt; bound by hands
burn; binding ulcers of wrists and & ankles; slept bound, hanging from a closet rod with
ankles; intra-oral laceration; neck wrists handcuffed behind her back (see Fig. 1)
ligature; diffuse skin scarring
5y 4 m female Abusive head trauma; healed burns; Died Died in intensive care unit; starved; shaken; bound by Father & stepmother
bruises to head, thorax, & extremities; wrists & upper arms and kept in a box; forced pushups
arm ligature marks; perineal laceration
Journ Child Adol TraumaTable 1 (continued)
Age/sex Physical injury Outcome Reported methods of torture Perpetrator(s)
& stair walks; kicked & punched; struck with objects;
burned in shower
6y 11 m male Bruising over most body surfaces; Survived Chronically starved; hyponatremic seizure from forced Adoptive mother
Adoptive sibling of facial burn; lacerated scrotum water intoxication; history of being cut with knife in the
7y 0 m scrotum; adoptive mother reported to school that child
Journ Child Adol Trauma
had a life-threatening medical condition requiring
restrictions of food and water; refeeding syndrome when fed
7y 0 m male Multiple bruises; malnutrition; history Died Dehydration documented at autopsy; chronically starved; Adoptive mother
Adoptive sibling of of spiral fracture of right femur at drank from toilet; clawed through window screen to
6y 11 m 16 months & multiple bruises to face get snow to drink; bound by hands; adoptive mother
and body; dental trauma & extraction reported to school that child had a life-threatening
at 20 months medical condition requiring restrictions of food and
water; adoptive mother had CPS acquire the lock that
kept him from getting food and water
8y 1 m female Severe non-acute genital injuries (fistula) Survived Starved; consumed own urine, feces and vomit; restrained; Mother & stepfather
requiring colostomy beaten; spurned; medical neglect; sexual abuse; kept in
closet, car trunk, & cabinets for 4 years; no school or
human interactions permitted; ridiculed & spurned
by 4 siblings
8y 2 m female Facial laceration; scars on face & trunk; Survived Withheld food & fed spoiled food; beaten; isolated Mother & maternal grandmother
loop mark bruises of chest, back, from siblings & school; scapegoated; made to sleep
& legs; hair cut off in hallway; long hair cut off
8y 5 m female Numerous contusions over body; hair Survived Bound to a chair by hands/mouth/legs; long hair cut Mother & mother’s boyfriend
cut off off; hands burned; beaten for falling asleep
8y 10 m female Medical neglect resulting in critical illness Survived Withheld food and drink; limited toilet access; isolated Stepmother & father
& near fatality; significant bruising; from family & school; repeated spanking & beating;
malnutrition forced sitting for hours
8y 11 m female Abusive head trauma; malnutrition; renal Died Found dead in a bathroom; starved; restrained by wrists Adoptive mother & adoptive
Adoptive sibling of failure; scars/bruises/abrasions on head, & ankles with duct tape around mouth; isolated father
10y 0 m case trunk & extremities; ligatures on wrists from family & school; beaten; no access to toilet;
and elbows; lip laceration; pressure head trauma
ulcers over sacrum, lower back
9y 1 m male Malnutrition; patterned injury on trunk; Died Found dead on bathroom floor; starved; padlocked in Mother & mother’s girlfriend
laceration of lip, trunk, & extremities; room; bound with electric cords to prevent “getting
cauliflower ear; burn on left shoulder; food from the pantry in the middle of the night”;
ligature injuries of elbows, wrists & struck in head with golf club; forced standing for
ankles; sacral decubitus ulcer; various hours; isolated from
ages of contusions, lacerations, & family & school
abrasions of multiple body surfaces
9y 7 m male Malnutrition; dehydration; bruises Survived Food restricted; given caustic substances as “punishment Maternal great aunt & maternal
Sibling of 10y 8 m case food”; deprived of toilet use/bathing; beaten; medical great uncle (adoptive parents)
neglect for severe asthma; withdrawn from school
3 years prior after disagreement with school over
food restriction; locked in garage without air
conditioning or heat
10y 0 m female Starvation; anemia; patterned lesions Survived Starved; restrained by wrists & ankles with duct tape Adoptive mother & adoptive
Adoptive sibling of on trunk and extremities; around mouth & neck; chained to the bed; isolated father
8y 11 m case lacerated toe; ankle edema from family & school; beaten with broken shovel
pole; no access to toiletTable 1 (continued)
Age/sex Physical injury Outcome Reported methods of torture Perpetrator(s)
10y 8 m male Malnutrition; dehydration; bruises Survived Food restricted, given caustic substances as “punishment Maternal great aunt &
Sibling of 9y 7 m case food”; deprived of toilet use/bathing; beaten; medical maternal great uncle
neglect for severe asthma; withdrawn from school (adoptive parents)
3 years prior after disagreement with school over
food restriction; locked in garage without air
conditioning or heat
11y 8 m male Extensive scalp burn; 3 disarticulated Survived with PTSD, depression, Food/water deprivation; confinement in small cubbyhole; 3 unrelated caregivers &
toes; mummification of fingertips; loss of digits forced water intoxication; scalded repetitively; hand mother (who was killed
chronic decubitus ulcers; patterned restrained behind back while submersed in water; by same caregivers)
skin injury; malnutrition; dehydration tied by neck to showerhead and forced to stand
or strangulate if fell; (see Fig. 2)
12y 3 m female Burn scar; patterned skin injuries Survived, with suicidal ideation Forced to sleep unclothed on cold garage floor, Father & stepmother
and PTSD basement floor, & bathtub as punishment for
bedwetting; forced to crawl until hands/feet bled;
forced standing on one leg; threatened to kill child
& throw away belongings
13y 8 m female Malnutrition; bruises Died Found dead by parents; starved; deprived of bathing/toilet; Mother & father
isolated; beaten; parents put garlic, pepper, & vinegar
in child’s drinks to make them taste bad; paper bag
put on head as punishment; child chained; forced
positions for discipline; punished for stealing food;
“homeschooled” for 3 years, but no education provided; no
friend, family, school contact, or medical/mental health
care for 4.5 years
14 y 0 m female Chronic malnutrition; no medical care Survived Withheld food & drink; all bathing & toileting strictly Stepmother & father
for 5 years (lost 23 kg); severe dental supervised to prevent obtaining water; drank from toilet
caries with teeth eroded to gum line when possible; forced to sleep on the bare floor beside
parents’ bed & denied covers; locked in a small unheated
room outside the house; hands taped behind her back
and head was pushed into the toilet; beaten with a shoe
and head slammed into a bed; removed from school to
be “home-schooled” after 1st CPS report; books
restricted as punishment
14y 1 m female Malnutrition; multiple abrasions; Survived Withheld food resulting in food scavenging; chronically Father & stepmother
3 digit fractures starved; all access to food in house locked; isolated
from family & school; slapped/shoved; forced to
sleep naked outdoors without a blanket
14y 4 m female Multiple bruises/lacerations over Survived with PTSD Starved; strangled until unconscious; stabbed with Mother & father
entire body; 3 extremity fractures; knife; forced to eat roaches/spiders; attempted
malnutrition suffocation by plastic bag duct-taped over her head;
struck in head with metal objects & baseball bats
a
SDH subdural hemorrhage; b PTSD post-traumatic stress disorder; c TBSA total body surface area
Journ Child Adol TraumaJourn Child Adol Trauma Fig. 1 A 4 6/12 year-old female was found dead in the bathroom. She had burn. That burn, a grid-like cheek contact burn and multiple sub-acute 50 % TBSA acute immersion burns and an acute subdural hemorrhage. facial injuries are seen in her lateral face view (c). The back of her legs She had been suspended from a closet rod at night by a bent coat hanger shows the immersion burns with popliteal sparing. They overlie pressure (distant and close up images a and b) to prevent her scratching her old scalp ulcerations over her heel cords from prior binding with ligatures (d) the closet. The girl was lying in the fetal position in the back of the child had stated her multiple injuries were self-inflicted, the closet; she had a scalp laceration, bald patches, and dried caused by fighting with other teens. However, during the blood on her head. The social worker called law enforcement, course of her hospitalization, she reported ongoing severe and the child was transported to an academic medical center. physical and psychological abuse. She reported being forced At the hospital, the child was emaciated and had multiple to eat roaches, spiders, and other insects as a form of punish- varying age lacerations and contusions on her body, a bite ment and that her family attempted to force feed her a dead mark on her anterior shin, and numerous healed scars on her mouse. She stated that her father bound her hands behind her face, back, and abdomen. X-rays revealed an acute transverse back, taped plastic bags over her head and torso, and threat- fracture of the right patella, acute fracture of the left 5th ened to drown her in the lake. Her younger sister participated metacarpal bone, and a healing fracture of the left 3rd meta- in her abuse by encouraging their father to place more duct carpal bone. It was later determined that the child had pubertal tape on her mouth and also encouraged their mother to force arrest and regression of breast development. On initial history, the girl’s face into soiled toilet water. She reported digital Fig. 2 Law enforcement scene investigation confirmed the 11-year-old injury from chronic confinement, eroded to the bone (c); burned and child victim’s disclosures that he was forcibly confined in a cubbyhole mummified toes, later spontaneously disarticulated (d); scalded fingers underneath the stairs (a) and in closets. A child alarm was placed on the with mummified tips (e) house door to detect his movement and prevent escape (b). Scalp pressure
Journ Child Adol Trauma
Table 2 Physical injuries (n=28) the knowledge and/or acquiescence of other caregivers and
Physical injuries % Yes % No % Unknown siblings. The role of female perpetrators in all cases is an
atypical finding in most cases of child physical abuse. As
Physical binding 61 21 18 the level of violence and control in the homes increased,
Gagging 25 29 46 perpetrators increased the isolation of the victims from every-
Restriction of bodily function 79 27 14 one but their immediate caretakers. The child’s entire house-
Cutaneous evidence of abuse 93 7 0 hold either participated in or was aware of the child’s abuse.
Beating 93 7 0 Nearly all children in this case series presented with cutaneous
Kicking 36 11 54 injury. A significant minority (21 %) had fractures. This is
Burning, contact 43 54 4 different from most forms of physical child abuse, in which
Burning, scald 18 75 27 fractures are common, but are typically limited to infants and
Striking with objects 79 7 14 toddlers (King et al. 1988). The children were denied medical
Stabbing 7 89 4 intervention until fortuitously they were discovered or near
Asphyxiation 14 57 29 fatal or fatal events occurred.
Forced position or standing 68 14 18 Based on the commonalities found among these infants and
Forced exercise 25 39 36 children, we propose defining child torture as a longitudinal
Fractures 21 6 11 period of abuse characterized by at least two physical assaults,
Action to aggravate pain of existing injury 43 29 29 and two or more forms of psychological maltreatment (e.g.,
Sexual abuse 21 64 14 terrorizing, isolating), resulting in prolonged suffering, per-
Permanent loss body part or function 46 21 32 manent disfigurement/dysfunction, or death. Torture usually
Death 36 64 0 includes neglect of obvious medical needs that are often the
result of their abusive injuries or starvation. Multiple episodes
of physical and emotional abuse occur over time or during one
penetration of her vagina by her father who also repeatedly prolonged period of abuse. In most cases, the caretaker(s)
made her stand naked in front of the mirror while fondling her made concerted efforts to isolate the child from outside con-
breasts. Her mother struck her with metal pipes, a skillet, tact or observation. Table 4 outlines the definition and pro-
baseball bats, and a glass candle. She also disclosed being vides examples of common forms of assault experienced by
stabbed in the abdomen and forearm with a kitchen knife, child torture victims.
exposing the bone. No medical care was sought for her inju-
ries. The girl reported she felt certain she would die. Her case Caregiver Motivation and Dynamics
had been reported to social services three prior times in the
same year, one of which had not been accepted for investiga- Definitions of political torture include analysis of the perpe-
tion and the other two were unfounded for abuse. The most trators’ intent to commit torture. Captor/perpetrators are polit-
recent allegation was unfounded because the child attributed ically motivated and are state actors, thus differ from a child’s
her bruises and lacerations to injuries sustained during a gang caretaker in a caregiving setting.
altercation. For our subjects, caregiver statements to medical providers,
CPS, and police were insufficient or incomplete. Thus, the
motivation or intent of the abuser was not analyzed in this case
series. The diagnosis of torture in an intra-familial setting is
Discussion based on the severity, morbidity, and mortality of the physical
and psychological maltreatment inflicted on the child. A sim-
Defining Torture in the Context of Child Abuse ilar focus on the harm the child has suffered, instead of the
perpetrator’s intent, has been used in defining other types of
The children in this case series suffered a severe combined child abuse, including Medical Child Abuse, a reframing of
type of child abuse including extreme physical and psycho- Munchausen Syndrome by Proxy (Stirling and American
logical maltreatment (Table 4). Torture goes beyond simple Academy of Pediatrics Committee on Child Abuse and
polyvictimization in that it includes an increased severity of Neglect 2007).
both physical and psychological maltreatment. It involves
intense humiliation and terrorization (Finkelhor et al. 2011). Household Dynamics
In our case series, common characteristics of child torture
involved multiple abusive physical injuries, deprivation of Several children came into the torturing households through
essential needs, and denigration or dehumanizing the child. informal family arrangements. We observed that 79 % of the
Torture was found to occur over a period of time, often with primary abusers were not the child’s first degree relative; theyJourn Child Adol Trauma
Table 3 Psychological
maltreatment Psychological maltreatment Yes No Unknown
Threat of death 9 (32 %) 4 (14 %) 15 (54 %)
Threat to loved object or pet 4 (14 %) 2 (7 %) 22 (79 %)
Threat to loved people 4 (14 %) 4 (14 %) 20 (71 %)
Threat of further torture 17 (61 %) 0 (0 %) 11 (39 %)
Terrorizing 21 (75 %) 0 (0 %) 7 (25 %)
Solitary confinement 21 (75 %) 5 (18 %) 2 (7 %)
Isolation from peers or other 25 (89 %) 2 (7 %) 1 (4 %)
Not allowed personal hygiene 18 (64 %) 2 (7 %) 8 (29 %)
Not allowed privacy 14 (50 %) 3 (11 %) 11 (39 %)
Food deprivation 25 (89 %) 1 (4 %) 2 (7 %)
Water deprivation 22 (79 %) 1 (4 %) 5 (18 %)
Sleep deprivation 14 (50 %) 0 (0 %) 14 (14 %)
Exposure hot/cold environment 12 (43 %) 4 (14 %) 12 (43 %)
Spurning 15 (54 %) 0 (0 %) 13 (46 %)
Denied emotional responsiveness 22 (79 %) 0 (0 %) 6 (21 %)
Insulted 12 (43 %) 0 (0 %) 16 (57 %)
Mental health neglect 5 (18 %) 14 (50 %) 9 (32 %)
Medical neglect 23 (82 %) 3 (11 %) 2 (7 %)
a Prior CPS history 14 (50 %) 11 (39 %) 3 (11 %)
17 children were old enough to
attend school (ages 6 and above) Educational neglecta (n=17) 14 (82 %) 2 (12 %) 1 (6 %)
b
23 children had known siblings Homeschooleda (n=17) 8 (47 %) 8 (47 %) 1 (6 %)
(three of whom were infants) Never allowed to attend schoola (n=17) 5 (29 %) 11 (65 %) 1 (6 %)
c
20 children had non-infant sib- Sibling also abuse victimb (n=23) 15 (65 %) 8 (35 %) NA
lings capable of acting as an Sibling also an abuserc(n=20) 9 (45 %) 11 (55 %) NA
abuser
included such caregivers as boyfriends, girlfriends, aunts, poor. Safety plans for victims of child torture should rarely, if
uncles, grandparents, adoptive parents, and stepparents. ever, involve plans for family reunification. Identification of the
Most child victims appeared to be scapegoated within their correct diagnosis should facilitate a safe child protection dispo-
family; this is another recognized form of abuse associated sition and appropriate long-term rehabilitative treatment for
with sibling empathy deficits (Hollingsworth et al. 2007). physical and psychological trauma endured by these victims.
Other siblings often were coerced to participate in or endorse The dynamic of psychological and physical cruelty used to
the abuse of the index child. In this case series, many of the control a child is similar to the dynamic often observed in
other children in the household were also abuse victims them- intimate partner violence. Perpetrators of child torture exercised
selves, although generally suffering significantly less abuse extreme control over their child victims, inflicting repetitive
than the index child. pain and suffering on these children and dehumanizing them. In
Typically, abusers demonstrated little or no remorse for their some instances torturers may threaten or injure a child’s loved
actions. Many transferred blame for their actions onto others ones or objects such as a family pet or favored toy as a means of
and most perpetrators blamed their victims for precipitating the gaining control over the victim. Denial of necessities, including
abuse or causing abuse to be necessary. Perpetrators seemed to access to food, water, toilet, and sleep were frequently utilized
utilize a framework of necessary discipline and corporal pun- as punishment by the perpetrators. Family members were co-
ishment to justify their abusive acts. In these and other cases we erced into participation in the child’s abuse, possibly out of their
have subsequently evaluated, some perpetrators saw it as a own fear or an inability to escape the situation.
religious duty to discipline their children harshly.
Early identification of perpetrators and their child victims is Effects of Torture
critical as Steele (1987) finds it “extremely difficult, if not
impossible, to rehabilitate perpetrators who torture their off- The long-term effects of child torture as a form of child abuse
spring” (p. 101). The nature of these crimes and the perpetra- are unknown. The medical literature clearly reflects that adult
tor’s self-justification argues against any reunification with torture victims have significant physical and psychological
caretakers and the rehabilitation potential of perpetrators is sequelae (Goldfeld et al. 1988; Herman 1992). AJourn Child Adol Trauma
Table 4 Definition Medical Evaluation
Child torture is defined medically as:
• At least two physical assaults, occurring over at least two incidents or In some cases, health care providers had observed the child for
a single extended incident, which would cause prolonged physical caretaker complaints, but failed to recognize the child’s inju-
pain, emotional distress, bodily injury, or death ries or malnutrition or to accurately diagnose abuse as their
And cause. This subsequently resulted in a continuation of the
• At least two elements of psychological abuse such as isolation, abuse with severe physical and psychological injury to the
intimidation, emotional/psychological maltreatment, terrorizing, child. For example, medical providers frequently based their
spurning, or deprivation
evaluations solely on the history reported by the perpetrator
Inflicted by the child’s caretaker(s)
and failed to consider alternate explanations for malnutrition,
Neglect is usually present, and manifests as failure to seek appropriate
such as intentional starvation. The perpetrators’ explanations
care for injuries and/or malnutrition
that their children were suffering from behavioral or psychi-
Resulting in: prolonged emotional distress, pain and suffering, bodily
injury/disfigurement, permanent bodily dysfunction, and/or death atric issues causing the starvation were initially accepted by
health care practitioners. Many of these children had been
Common Abuse Manifestations Include, But are Not Limited to: bound, confined, or isolated to prevent acquisition of food or
• Physical assaults: hitting, kicking, impacting against objects, beating water; consequently, these children often attempted to steal or
with objects, tying, binding, gagging, stabbing or cutting, burning, otherwise acquire food or water. They were severely punished
breaking bones, exposure to prolonged environmental heat or cold, if caught. A few children had been brought for medical
prolonged forced exercise, forced restraint in or maintenance of an
uncomfortable position, forced ingestion of noxious fluids, evaluations with complaints of “excessive hunger and thirst.”
dangerous materials or excrement, aggravating the pain of prior Physicians evaluating these children did not recognize that the
injuries children’s behavior represented an appropriate response to
• Isolation: removal from school or outside activity, restriction of peer their deprivation. As a result, victims suffered ongoing abuse
contact, hiding from outsiders, imprisoning alone and/or in tightly or death.
confined spaces restricting movement
The victims we saw share some of the characteristics of the
• Intimidation or emotional/psychological maltreatment: Repeated
intimidation or humiliation, cursing, denigration, threatening harm to child starvation cases described by Kellogg and Lukefahr
or harming loved ones, pets or loved objects, spurning, terrorizing (2005), including isolation of the child and hidden or missed
• Deprivation: deprivation of food, water, or sleep, forced to watch malnutrition. They were usually kept at home, or if taken
while others eat or drink, punishment for seeking basic needs, where others could observe them, were clothed to cover their
deprivation of safe and hygienic excretory function, neglect of degree of malnutrition and their physical injuries. Older chil-
medical needs, neglect of mental health needs, deprivation of
education, deprivation of human contact dren were removed from school under the guise of home
Common perpetrator manifestations:
schooling. Although home schooling is a valid form of edu-
• Typically both adult caregivers are involved in the torture to some
cation for many families, these children show no evidence of
extent receiving any education. Their removal from school appears
• Women figure much more prominently as perpetrators of torture than to have been motivated by the need to keep the children
in other forms of physical abuse hidden. Several children had home visits from protective
• Siblings are aware of and may be coerced to participate in the abuse, services or public health nurses or were seen by physicians,
and also may be abused to a lesser degree but their severe malnutrition was missed. Lack of regularly
obtaining and charting growth data appeared contributory.
The evaluation requires a comprehensive, multidisciplinary
psychological syndrome reported in adult torture survivors by approach, including scene investigation, careful questioning
Allodi and Cowgill (1982) includes findings of extreme anx- of the victim, siblings, potential witnesses, and the caregivers.
iety, insomnia, nightmares, suspicious/fearfulness, as well as Medical providers must collaborate with police and protective
somatic symptoms of anxiety and phobias. PTSD is the most services who can evaluate the scene for evidence of confine-
commonly diagnosed psychological disorder among adult ment and past injuries. Photographs should be taken to docu-
torture victims (Allodi and Cowgill 1982; Herman 1992). In ment the availability of sufficient food in the household.
addition to torture, polyvictimization has been recognized to Additionally, photographs should also be taken of any objects
be associated with worse mental health outcomes in child of value in the home (e.g., mobile technologies, gaming
abuse victims (Finkelhor et al. 2011). By definition, all of technologies, alcohol, expensive accessories) to document
our children have suffered polyvictimization as defined by the availability of resources in the home that could have been
Finkelhor. Although mental health evaluations were not al- used to purchase food for the children. Investigators should
ways done or accessible to us, the victims in our case series interview leaders of the perpetrator(s) faith community to
commonly were diagnosed with PTSD. Formal psychiatric determine whether their actions represent idiosyncratic reli-
evaluation is recommended for all victims. gious beliefs. This could defend against claims that theJourn Child Adol Trauma perpetrator(s) abuses of the child fell within the range of acts child victims, allowing earlier intervention by authorities. sanctioned by doctrine of faith. Medically defining child torture also would invite child pro- In cases involving starvation, it is important to obtain tective services, law enforcement, and legal professionals to laboratory studies for dehydration and nutritional status as better recognize the full extent of the injuries suffered by these soon as possible after the child presents for care. If the case children, understand the possible outcomes, and allow them to enters the court system, serial photographs of the victim from more effectively protect victims and prosecute perpetrators. the time of presentation until nutritional recovery are compel- We noted that siblings are also frequently recruited to assist ling illustrations of the severity of nutritional deprivation, in abusing the index child, but also are abuse victims to a supplementing the growth curves. Likewise, these children’s lesser degree themselves. At the very least, they sustain the voracious appetites and rapid weight gain after they are harms of witnesses of violence and abuse (Finkelhor et al. allowed food and fluids belie allegations that they suffer from 2009). As such, both their safety and mental health needs also eating disorders, unusual endocrine disorders, or metabolic must be considered. Both victims and siblings will likely disorders as a cause of starvation (Kellogg and Lukefahr require therapeutic foster care placement and long-term men- 2005). Starved children risk re-feeding syndrome if their tal health services (Anda et al. 2006). malnutrition has been prolonged. The legal landscape for addressing torture varies widely by The cases we observed reflect systematic attempts by the jurisdiction (Tiapula and Applebaum 2011). Statutes caregiver(s) to cause physical and psychological pain and referencing torture reflect a range of legislative responses, suffering to the child. The dynamic of domination and control including both criminal and civil statutes. Criminal laws pro- over the necessities of life is uniquely different from other hibit and penalize both physical and sexual torture while civil forms of physical abuse, which usually result from caretaker statutes reference torture in matters of family law, employment anger and loss of control (Schmitt 1987). The extent to which law, and public health law. Both physical and sexual torture these caregivers have created a system of rules, boundaries, are explicitly addressed by some states in a range of criminal and patterns for managing the targeted children is unique. and child protection statutes and legal precedents, often these Forced position holding, such as standing with arms stretched include specific provisions related to the extent of the injury or out holding phone books for hours, was a common form of pain suffered by the victim (Tiapula and Applebaum 2011). discipline. Medical, child protection, or criminal justice pro- Thus, medical providers should be careful to document the fessionals often failed to note these rules or rituals or under- child’s pain and suffering in cases involving child torture. A stand their abusive significance. Thus the psychological mal- medical definition of torture might stimulate other states to treatment of these children often was overlooked. adopt explicit torture statutes and those with current statues to When extreme discipline is accepted as the norm by a child, update them. Emerging recognition of torture as a distinct the child may not disclose to a medical provider the abuse they medical diagnosis would enable legislative responses that experienced unless specifically asked. Open-ended questions reflect the severity of injury. It would enable courts to focus such as “tell me about meal time,” “tell me about going to the on many of the factors that are often not addressed in existing bathroom,” or “what are the rules about sleep or potty” can be statutes. For example, medical issues include restraint, isola- very helpful in eliciting otherwise normalized punishments, tion, and withholding of necessities and psychological mal- such as food withholding or forced excrement ingestion. treatment. Criminal prosecution and sentencing in cases of Often disclosures only gradually come forth after the child child torture reflect the uneven outcomes associated with has been stabilized in a safe setting. Professionals involved in institutional failures by law enforcement, prosecutors, and these cases may not be aware of the existence of or recognize the courts to recognize and validate the emotional and psy- the significance of extreme forms of discipline, including chological injuries linked to torture. Data not available to the limited access to toilet, food, sleep, or other necessities which current researchers included the prior criminal history of each dehumanize or demean the child. defendant; a factor often weighed heavily in sentencing out- Fifty percent of the children in this case series had been comes. Another significant factor in sentencing would be the previously reported to child protective services for maltreat- relative culpability of each defendant in cases with multiple ment, including psychological maltreatment and starvation. perpetrators torturing or participating in the torture of the child However, there was poor coordination between the medical victim(s). The criminal sentences the perpetrators received providers and the child protection system to identify and ranged from probation to life in prison. manage torture as an unique form of injury. Cases involving This series and paper is limited in that it is a select and by withholding of food were not recognized as a form of abuse. no means, inclusive series, of abuse cases. They have been Cases of unusual punishment, such as prolonged forced exer- chosen to be illustrative of the phenomenon of torture, but cise, also were dismissed and not further pursued. Ultimately a cannot be considered a consecutive case series for statistical medical definition of child torture would provide the medical analysis. Likewise, the information available to us was that profession a framework to make an appropriate diagnosis of primarily available through our consultations. In particular,
Journ Child Adol Trauma
detailed medical and psychiatric follow-up information was Cantwell, H. B. (1980). Child neglect. In R. E. Helfer & H. C. Henry
Kempe (Eds.), The battered child (3rd ed., pp. 183–197). Chicago:
usually unavailable to us.
University of Chicago Press.
Christian, C. W., Block, R., & Committee on Child Abuse and Neglect,
American Academy of Pediatrics. (2009). Abusive head trauma in
infants and children. Pediatrics, 123(5), 1409–1411. doi:10.1542/
Conclusions peds.2009-0408.
Cohn, J., Holzer, K. M. H., & Kock, L. (1981). Torture of children: an
investigation of Chilean immigrant children in Denmark. Child
This case series identified specific components common to 28 Abuse & Neglect, 5(2), 201–203. doi:10.1016/0145-2134(81)
children and infants who were considered victims of torture. 90042.
These commonalities indicate that torture can be defined as at den Otter, J. J., Smit, Y., dela Cruz, L. B., Ozkalipci, O., & Oral, R.
(2013). Documentation of torture and cruel, inhuman or degrading
least two physical assaults (or a single extended incident) and treatment of children: a review of existing guidelines and tools.
two or more elements of psychological maltreatment. Neglect Forensic Science International, 224(1–3), 27–32. doi:10.1016/j.
is often present, generally manifesting as failure to seek ap- forsciint.2012.11.003.
propriate care for injuries and/or malnutrition. The combina- Finkelhor, D., Turner, H., Ormrod, R., & Hamby, S. L. (2009). Violence,
abuse, and crime exposure in a national sample of children and youth.
tion of physical and psychological maltreatment results in Pediatrics, 124(5), 1411–1423. doi:10.1001/jamapediatrics.2013.42.
severe child trauma, including prolonged emotional distress, Finkelhor, D., Shattuck, A., Turner, H. A., Ormrod, R., & Hamby, S. L.
pain and suffering, bodily injury/disfigurement, permanent (2011). Polyvictimization in developmental context. Journal of
bodily dysfunction, and/or death. Victims of torture were Child & Adolescent Trauma, 4(4), 291–300. doi:10.1080/
19361521.2011.610432.
isolated, terrorized, neglected, deprived of basic necessities, Goldfeld, A. E., Mollica, R. F., Pesavento, B. H., & Faraone, S. V. (1988).
as well as physically and psychologically maltreated. Their The physical and psychological sequelae of torture.
abuse appears to represent caretaker efforts to crush the child’s Symptomatology and diagnosis. JAMA, 259(18), 2725–2729. doi:
spirit and humanity. Recognizing early signs of torture, such 10.1001/jama.1988.03720180051032.
Green, C. (2007). Politically-motivated torture and child survivors.
as malnutrition, injuries suspicious for physical abuse, and Pediatric Nursing, 33(3), 267–270.
lack of emotional responsiveness has significant potential to Hart, S. N., Brassard, M. R., Davidson, H. A., Rivelis, E., Diaz, V., &
reduce the significant morbidity and mortality associated with Binggeli, N. J. (2011). Psychological maltreatment. In J. E. B.
this type of child abuse. The prevention of torture also de- Myers (Ed.), The APSAC handbook on child maltreatment (pp.
79–102). Thousand Oaks: Sage.
pends on an effective child protection and criminal justice
Herman, J. L. (1992). Complex PTSD: a syndrome in survivors of
response requiring education and coordination among medical prolonged and repeated trauma. Journal of Traumatic Stress, 5(3),
professionals, child protection workers, law enforcement, and 377–391. doi:10.1007/BF00977235.
the legal community. Hibbard, R., Barlow, J., Macmillan, H., Child, A., & Committee on Child
Abuse and Neglect American Academy of Pediatrics. (2012).
Psychological maltreatment. Pediatrics, 130(2), 372–378. doi:10.
1542/peds.2012-1552.
Hollingsworth, J., Glass, J., & Heisler, K. W. (2007). Empathy deficits in
siblings of severely scapegoated children: a conceptual model.
References Journal of Emotional Abuse, 7(4), 69–88.
Kellogg, N. D., & Lukefahr, J. L. (2005). Criminally prosecuted cases of
child starvation. Pediatrics, 116(6), 1309–1316. doi:10.1542/peds.
Allasio, D., & Fischer, H. (1998). Torture versus child abuse: what’s the 2004-2616.
difference? Clinical Pediatrics, 37(4), 269–271. doi:10.1177/ Kempe, C. H. (1978). Sexual abuse, another hidden pediatric problem: the
000992289803700410. 1977C. Anderson Aldrich lecture. Pediatrics, 62(3), 382–389.
Allodi, F., & Cowgill, G. (1982). Ethical and psychiatric aspects of Retrieved from http://pediatrics.aappublications.org/content/62/3/382.
torture: a Canadian study. Canadian Journal of Psychiatry, 27(2), Kempe, C. H., Silverman, F. N., Steele, B. F., Droegemueller, W., &
98–102. Silver, H. K. (1962). The battered-child syndrome. JAMA, 181, 17–
Amnesty International. (1975). Report on torture. New York: Farrar, 24. doi:10.1001/jama.1962.03050270019004.
Straus and Giroux. King, J., Diefendorf, D., Apthorp, J., Negrete, V. F., & Carlson, M.
Anda, R. F., Feletti, V. J., Bremner, J. D., Walker, J. D., Whitfield, C., (1988). Analysis of 429 fractures in 189 battered children. Journal
Perry, B. D., . . . Giles, W. H. (2006). The enduring effects of abuse of Pediatric Orthopedics, 8(5), 585–589.
and related adverse experiences in childhood—a convergence of Knox, B. L., & Starling, S. (November 27, 2012). Child torture: Case
evidence from neurobiology and epidemiology. European Archives reviews and analysis of institutional responses. Paper presented at
of Psychiatry and Clinical Neuroscience, 256, 174–186. doi:10. the National District Attorneys Association National Center for the
1007/s00406-005-0624-4. Prosecution of Child Abuse Investigation and Prosecution of Child
Burgers, J. H., & Danelius, H. (1988). The United Nations Convention Fatalities and Physical Abuse Conference, Honolulu, Hawaii.
Against Torture: A handbook on the convention against torture and Roesler, T., & Jenny, C. (2009). Medical child abuse: Beyond
other cruel, inhuman or degrading treatment or punishment. Munchausen syndrome by proxy. Elk Grove Village: American
Dordrecht: Martinus Nijhoff. Academy of Pediatrics. doi:10.1016/B978-1-4160-6393-3.00061-0.
Campbell, T. A. (2007). Psychological assessment, diagnosis, and treat- Rosenberg, D. A. (1987). Web of deceit: a literature review of
ment of torture survivors: a review. Clinical Psychology Review, 27, Munchausen syndrome by proxy. Child Abuse & Neglect, 11(4),
628–641. doi:10.1016/j.cpr.2007.02.003. 547–563. doi:10.1016/0145-2134(87)90081-0.Journ Child Adol Trauma
Schmitt, B. D. (1987). Seven deadly sins of childhood: advising parents Tiapula, S., & Applebaum, A. (2011). Criminal justice and child protec-
about difficult developmental phases. Child Abuse & Neglect, 11(3), tion responses to cases of severe child abuse: existing statutory
421–432. doi:10.1011/0145-2134(87)90015-9. frameworks for torture. National Center for the Prosecuton of
Steele, B. (1987). Psychodynamic factors in child abuse. In R. Child Abuse Update, 23(1), 1–8.
Helfer, C. H. Kempe, & R. S. Krugman (Eds.), The battered Tournel, G., Desurmont, M., Becart, A., Hedouin, V., & Gosset, D.
child (4th ed., pp. 81–114). Chicago: University of Chicago (2006). Child barbarity and torture: a case report. The American
Press. Journal of Forensic Medicine and Pathology, 27(3), 263–265. doi:
Stirling, J., Jr., & American Academy of Pediatrics Committee on 10.1097/01.paf.0000233532.18076.14.
Child Abuse & Neglect. (2007). Beyond Munchausen syn- Welsh, J. (2000). Children and torture. Lancet, 356(9247), 2093. doi:10.
drome by proxy: identification and treatment of child abuse 1016/S0140-6736(00)03414-0.
in a medical setting. Pediatrics, 119(5), 1026–1030. doi:10. World Medical Association (1975, revised 2006). Declaration of Tokyo-
1542/peds.2007-0563. guidelines for physicians concerning torture and other cruel, inhu-
Stover, E., & Nightingale, E. (1985). Introduction: The breaking of bodies man or degrading treatment or punishment in relation to detention
and minds. In E. Stover & E. Nightingale (Eds.), Breaking of bodies and imprisonment. Retrieved from World Medical Association
and minds: Torture, psychiatric abuse, and the health professions website: http://www.wma.net/en/30publications/10policies/c18/
(pp. 1–26). New York: Freeman. index.html.You can also read