Pushing the boundaries: Evidence to support the delivery of good practice in audiology - NHS England
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
NHS
AUDIOLOGY
NHS Improvement
CANCER
DIAGNOSTICS
HEART
LUNG
STROKE
Audiology Improvement Programme
Pushing the boundaries:
Evidence to support the delivery of
good practice in audiology

Pushing the boundaries: Evidence to support the development and implementation of good practice in audiology | 3
Contents
Introduction 4
Age related hearing loss projects 5
Direct access tinnitus patient pathway 12
Balance 17
Collaboratively working with ENT to redesign pathways 22
Adults with complex hearing needs 24
Audiology transition projects 27
Children’s balance 33
Children’s hearing services 40
Central auditory processing disorder 45
Acknowledgement 47
www.improvement.nhs.uk/audiology
4 | Pushing the boundaries: Evidence to support the development and implementation of good practice in audiology
Introduction
During 2009/10 NHS Improvement This report contains information for There are lots of practical examples
worked wih 18 pilot sites across those professionals working in, within this report to support clinical
England as part of the Department of commissioning or interfacing with, teams in delivering quality and
Health (DH) National Audiology audiology services. This will include productivity benefits for our patients
Programme (led by the DH Chief those who are: and a wider range of stakeholders.
Scientific Officer, Profressor Sue Hill), • involved in the care of patients
to identify and share innovative ways who require audiology services Over the next 12 months, the NHS
to improve the quality of patient • responsible for commissioning Improvement Audiology Programme
experience, increase productivity and audiology services will be testing the key principles for
sustain improvements over the long • managing audiology services change in a small number of NHS
term. The pilots covered a diverse • involved in the education and sites, in a similar process to that
range of clinical pathways which training of staff who will be which has established winning
included tinnitus, balance and working with patients who require principles in transforming cardiac and
children’s hearing, as well as age audiology services. cancer care. As this information
related hearing loss and those with emerges it will be shared with
more complex needs The pilot sites were encouraged to audiology services and the wider
employ a range of service NHS.
This publication has been written to improvement techniques as
share the learning from this pilot appropriate to their needs. These
phase of the NHS Improvement included process mapping, capacity Dr Janet Williamson
Audiology Programme. Through a and demand analysis, application of National Director, NHS Improvement
series of case studies and examples, Lean methodology, process redesign
it aims to highlight areas of and workforce/skill mix review. The Professor Sue Hill
innovative and emerging good NHS Improvement team supported Chief Scientific Officer, Department
practice that can be used locally to the testing of new ideas and of Health
deliver improvements for audiology pathways through site visits and by
patients and their carers. One of hosting a number of learning
these successes includes working workshops.
with young people and the voluntary
sector to construct an effective multi-
agency approach to meeting their
needs by providing timely access to
relevant services.
www.improvement.nhs.uk/audiology
Pushing the boundaries: Evidence to support the development and implementation of good practice in audiology | 5
Age related hearing loss projects
Introduction Clinical leaders now need to focus on Summary
Gradual deterioration of the ear how to deliver effective care outside Each of the age related hearing loss
means that for most people, deafness an acute setting and in, or near to, pilot sites sought to move some
is an unwelcome feature of later life. patient’s homes. element of care into the community,
Although the degree of disability reduce the number of steps in the
varies greatly, and some people adjust This has focused audiology patient pathway and provide a more
quite well to the slow decline in their departments’ attention on improving effective and efficient service for
hearing, for many this form of current service provision to patients. They sought to improve the
hearing loss causes frustration, encompass these aspirations through quality of the service provided, whilst
loneliness and depression. getting the systems and processes maintaining or enhancing the patient
It is estimated that the prevalence of right, using the best technology experience.
hearing loss amongst adults in available and planning an effective
England is 20% and the vision for workforce to deliver these improved Moving care into the community and
audiology and adult hearing services services. closer to patients’ homes can throw
is to provide high quality, efficient up unusual and unexpected
services, delivered closer to home, With increasing competition from challenges, especially for hearing
where long waits are a thing of the alternative providers, audiology services, for example, in providing
past and where patients are treated departments need to be continually suitable accommodation and meeting
as individuals with personal needs looking for ways to improve on the the required noise specifications, at a
(Transforming Adult Hearing services services provided by reducing waiting busy health centre.
for Patients with Hearing Difficulties times, enhancing both the patient’s
2007). experience and the quality of care The sites chosen were:
and providing efficient pathways of • University Hospitals of
With the publication of the White care. Leicester NHS Trust
Paper ‘Our Health, Our Care, Our Say‘ (Leicester Royal Infirmary)
(Department of Health 2006) the The aim of this work is to identify the • Nottingham University
vision for people to have greater factors that help or hinder progress in Hospitals NHS Trust
choice, independence, control and moving care into community locations • Trafford Healthcare
empowerment was clearly and to share the lessons learnt with the NHS Trust.
articulated. This intentionally wider NHS.
challenged existing practice.
www.improvement.nhs.uk/audiology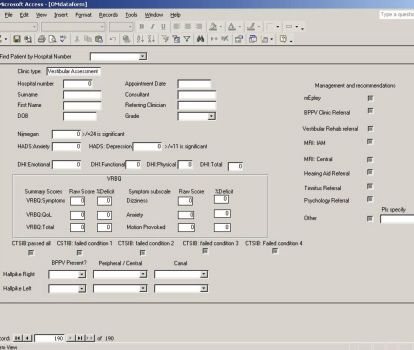
6 | Pushing the boundaries: Evidence to support the development and implementation of good practice in audiology
Initial findings from the pilot projects
have started to indicate that locally
led work, which forms part of the
national priorities, can be achieved by
working in partnership with all
stakeholders. The key to their success
stems from clear local clinical and
managerial leadership and the
application of robust project
management.
By involving the whole team within
the department and getting their
agreement to the proposed change,
ownership was gained and the teams
actively worked together to achieve
the best outcomes for their patients.
The projects demonstrate a
commitment to improving quality, the
use of new technology and increasing
productivity.
By streamlining the pathway and
reducing the number of steps, time
and resources have been released,
without compromising on quality.
Patient satisfaction with the revised
pathways is high, along with staff
fulfilment with the change in working
practice. Extended roles have been
developed and a clear commitment
has been demonstrated to continue
on this improvement journey.
www.improvement.nhs.uk/audiology
Pushing the boundaries: Evidence to support the development and implementation of good practice in audiology | 7
Triage in Primary Care: a new pathway
for hearing aid candidates
Leicester Royal Infirmary
Presenting Issues • Initially trained four GPs to use Benefits
The traditional way to manage screeners and the new referral form
patients who may need a hearing aid • Offered 90 minute appointments to Quality
is to assess at one appointment and those who were appropriate for By using two patient related outcome
fit at another. Recent advances in assess and fit at the same time and measures they have demonstrated
technology mean that, for certain 60 minute assess appointments for that the quality of service has not
patients, the two appointments can those who did not meet the been compromised by the assess and
be combined. criteria, following on with a further fit appointment. For the patients who
60 minute appointment for the only needed to attend once, this
In order to know who would be fitting represents a real increase in quality.
suitable and who would need to • Promoted their early work/findings
attend both appointments, a simple and recruited a further seven GPs Innovation
triage is carried out in primary care, to work with the pilot The utilisation of the screener and the
prior to referral. This enables patients • Recorded all the outcomes from the use of instant fitting technologies has
to go into the correct appointment pilot to enable a full analysis to been an excellent example of the
type for their needs. include a patient satisfaction potential role of innovation in patient
questionnaire. management.
The aim of this project was to pilot
the triage in primary care practices
using a small screening device
Numbers of patients on each pathway
(Siemens Hear Check Screeners)
and a short questionnaire.
The triage is done by either the GP
or the practice nurse/health care
assistant, and includes wax removal,
where necessary.
Pilot work has shown that locally,
approximately 40% of patients are
suitable for ‘assess and fit’ model.
What they did
• Used new technological advances
to enhance the patient’s pathway
• Redesigned the care pathway to
improve the patient’s experience
• Developed clear and consistent
referral criteria for primary care
practitioners
• Developed a direct referral form for
primary care to record screener
outcomes and highlight any
concerns regarding dexterity, poor
vision etc
www.improvement.nhs.uk/audiology
8 | Pushing the boundaries: Evidence to support the development and implementation of good practice in audiology
Productivity
The number of patients who have
completed the pathway through out
the duration of the pilot is 47. Of
those 47, 23 were suitable for the
assess and fit appointment, two out
of the 23 chose not to have the 90
minute appointment.
So 45% of referrals had a 90 minute
appointment, of these 67% had aids
fitted on the day. In terms of net time
saved, based on these relatively small
numbers, 30 minutes time can be
saved in 15% of referrals.
During the last 12 months, 2,420
patients have been directly referred,
even a 30 minute time saving on
15% results in 180 hours of clinical
time being saved.
Identifying the appropriate referral
route may save on the overall number
of referrals and cut costs.
Prevention
By educating GPs patients are more
likely to be referred to hearing
services at their first visit. Also
patients who are being triaged into
the assess and fit pathway are having
a reduced delay in their treatment.
Contact
Pauline Smith
Clinical Scientist - Audiology
pauline.smith15@nhs.net
www.improvement.nhs.uk/audiology
Pushing the boundaries: Evidence to support the development and implementation of good practice in audiology | 9
Developing new pathways for patients requiring
reassessment of hearing needs in Nottingham
Nottingham University Hospitals NHS Trust
Presenting Issues What they did • Achieved a 46% reduction in
Being able to manage the ever • Improved accessibility for patients number of attendances each
increasing demand on local audiology who require reassessment of their patient has to make in the new
services, while maintaining short hearing aid provision pathway and a 43% reduction in
waits and high quality services is • Provided a service that is delivered the time spent in clinic
becoming more difficult. It is safely and effectively at a location • Managed a greater number of
essential that departments look at that is closer to the patient’s home patients within existing resources
different ways of working to meet • Developed clear and consistent • Maintained clinical quality within a
demand within the resources referral criteria shortened appointment
available. • Reduced the number of steps in the • Conducted a comprehensive
patient pathway patient satisfaction survey to assess
This pilot involved redesigning the • Reduced the overall time spent in opinion on the new pathway.
care pathways for patients who the clinic environment
routinely require hearing aid
reassessment, by developing new
protocols and pathways and moving Numbers of appointments in each pathway
the service into a community location
within a local health centre, reducing
the appointment time in the clinic for
the majority of patients. This was
achieved with the introduction of a
‘triaging’ type appointment.
This enabled patients to be assessed
and those who had experienced no
change in hearing, or only a mild
deterioration requiring limited fine
tuning, to be treated separately from
those requiring a full audiological
reassessment.
Those patients assessed as requiring
the full reassessment would then be Numbers of appointments in each pathway
offered a further appointment, more
appropriate to their need. This should
improve the department’s ability to
manage waits by improving capacity
and increasing efficiency within the
service.
www.improvement.nhs.uk/audiology
10 | Pushing the boundaries: Evidence to support the development and implementation of good practice in audiology
Benefits Prevention
• Additional capacity has been
Quality identified to enable patients to be
• Clinical quality is maintained. recalled for reassessment every
• Patient satisfaction is increased. three years.
• Patients satisfaction results show
that 97% of patients from the pilot Contact
group would prefer a service local William Brassington
to them. Consultant Audiologist / Head of
Audiology
Innovation William.Brassington@nuh.nhs.uk
• The pathway has been refined,
minimising inefficiencies and
creating a new model of care.
• A benefit to patients is identified by
a 46% reduction in number of
attendances each patient has to
make in the new pathway.
Productivity
• Increased efficiency by reducing the
time spent in clinic by 43% and the
number of appointments required
by 46%.
• A greater number of patients can
be managed within existing
resources which will allow recall for
further reassessment in a more
timely way, working towards the
RNID gold standard of every three
years.
• Patients are managed with the
same clinical quality in a reduced
overall appointment length.
www.improvement.nhs.uk/audiologyPushing the boundaries: Evidence to support the development and implementation of good practice in audiology | 11
Care in the community for those needing
diagnostic assessment
Trafford Healthcare NHS Trust
Presenting Issues • 120 patients have been assessed Innovation
To improve access to hearing across the two new sites during the By moving care into the community
assessments clinics by providing pilot phase and closer to the patient’s home, the
additional community based services • Conducted a patient survey to Trust has responded to the wishes of
The audiology team developed canvas opinion on new pathway. patients. Trafford has the smallest
improved, streamlined pathways for audiology department in the North
adults with hearing loss and Former Manchester City and United West and is one of the first trusts
conducted a thorough review of the legend Denis Law has recently planning to become an integrated
existing skill mix and roles within the travelled the new clinical pathway. care organisation.
department. The revised pathway
was delivered from two community ‘I am more than happy to This means the trust will work in
based sites. partnership with social care to
endorse the new piloted way provide seamless care in the
Trafford Healthcare NHS Trust plans of working. I couldn’t have community for a range of long-term
to become an integrated care wished for a smoother conditions. This pilot model of care
organisation. Part of this project was journey.’ fits perfectly with this vision.
to build upon this intention and to
further enhance the working Productivity
Benefits
relationships between social care and With the additional clinics in place in
the local primary care trust providing the community, patients can now be
Quality
seamless community based care, for seen within two weeks of a referral
This pilot project has reduced the
those in the community who have
need for lengthy journeys for patients
long term conditions or a long term Contact
to travel into the acute trust .A
need. Mike Philbin
patient satisfaction survey was
Specialist Audiologist and
conducted with very positive
What they did Acting Head of Audiology
outcomes and the number of steps in
• Agreed a reduction in the age of Mike.Philbin@trafford.nhs.uk
the pathway have now been reduced.
patients who were able to be seen
Staff satisfaction with their role has
by the audiologist for a diagnostic
increased significantly.
assessment from 60 to 16 years of
age
• Worked in partnership with ENT
colleagues to enable audiologists
to refer for MRI scans as part of the
diagnostic assessment
• Achieved a reduction in the number
of steps in the patient pathway
• Moved care closer to home and
into two community clinics using
test booth facilities.
• Introduced extended roles for
assistant practitioners
www.improvement.nhs.uk/audiology12 | Pushing the boundaries: Evidence to support the development and implementation of good practice in audiology
Direct access tinnitus patient pathway
Introduction patients, tinnitus may be associated Baseline information from surveys
The publication of the DH Good with medical or otological conditions and focus groups illustrated that
Practice Tinnitus Guide, Provision of that need investigation and surgical patients often received limited advice
Services for Adults with Tinnitus, sets management. Consequently, triage on management of tinnitus in
out the vision for services and and differential diagnosis at an early primary care. Lack of awareness of
commissioning pathways. It suggests stage of presenting symptoms is tinnitus management strategies and
that for many patients, the pathways therefore critical, to not only identify knowledge of services available in
for effective care are not always appropriate management but reduce primary and secondary care was also
streamlined or as efficient as they the impact for both the patients recognised. In addition, patients
could be. Tinnitus or perception of quality of life and use of healthcare experienced delays of up to 20 weeks
sound in either one or both ears may resources. Any delay in access to before attending tinnitus
be reported as the only complaint or services can potentially impede the management clinics when referred
it may be a symptom of one or more process of tinnitus management and from ENT outpatients.
underlying pathologies. In the UK, a lead to a greater number of follow
longitudinal study, published by Davis ups by professionals. Early findings from pilot sites suggest
and El Rafaie1 suggests 10.1% of that between 60 to 85% of tinnitus
adults had experienced episodes of Summary referrals could be managed by a
tinnitus lasting more than five Three pilot sites aimed to implement direct access audiology service,
minutes and in 5% the tinnitus was a direct access audiologist/hearing provided that staff have the
moderately or severely annoying. therapist-led clinic to enhance patient appropriate knowledge and skills, are
0.5% of the study population were satisfaction, improve tinnitus deemed as competent, and work
affected severely enough for it to management outcomes and reduce within clinical guidelines and
have a serious impact on their ability referral to treatment times. protocols to enable access to ENT
to lead a normal life. consultants, if required. A reduction
The sites chosen were: in referral to treatment times from 14
The experience of tinnitus can lead to • University Hospitals weeks to less than four weeks has
many complex sets of complaints. Birmingham NHS Foundation been achieved. This efficiency has
Patients may experience distress, Trust – Selly Oak Hospital released up to 85% of tinnitus
helplessness or frustration, depressive • Sherwood Forest Hospitals NHS outpatient capacity, started to reduce
episodes, sleep disturbances, lack of Foundation Trust – Kings Mill follow ups required, and enhanced
concentration and, in a smaller Hospital patient satisfaction. Whilst the
proportion of patients, may be • Newcastle Upon Tyne Hospitals numbers of patients accessing the
chronically disabling. In some NHS Trust – Freeman Hospital direct access service are small, due to
www.improvement.nhs.uk/audiologyPushing the boundaries: Evidence to support the development and implementation of good practice in audiology | 13
the project timescales, further The patients’ story:
monitoring will provide better insight
into clinical advantages, improved ‘To try and speed the process of hospital referral up, that
patient experience and value for
money. certainly would have helped me, I felt I was on my own
and not able to cope.’
Presenting issues
Traditionally within all sites the ‘The emotional impact of Tinnitus can be extremely
majority of referrals into tinnitus
management clinics were from ENT
destructive, I lost my job, lost a relationship, it was
consultant clinics with a large tough.’
proportion of patients suffering from
bilateral tinnitus with no underlying Focus Group North Tyneside Disability Forum Tinnitus Group
medical condition. Sites were
convinced that many of the adults
being referred to ENT consultants
with tinnitus could have been • Variation in patient satisfaction • Inconsistent information given
managed by audiologists, healthcare levels with speed of access to ENT to patients by different
scientists or hearing therapists with outpatient clinic, explanation of professional groups can lead to
the appropriate level of training. This tinnitus, ability to discuss patients requiring more frequent
was illustrated by a retrospective condition, opportunity to ask follow up visits due to delay in
patient record audit, carried out by questions and helpfulness of acceptance of condition and ability
Newcastle Upon Tyne Hospitals NHS appointment. to adopt self management
Trust, who found that 60% of • Inconvenience for patients strategies due to anxiety and
patients referred to ENT could attending multiple hospital distress.
potentially be seen in a direct access visits prior to being seen by
clinic. This compares with Sherwood tinnitus management clinic – a
Forest Hospitals NHS Foundation Trust potential of five visits to hospital,
who found that 73% of referrals with contact with a variety of
from ENT were for bilateral tinnitus in professionals.
an audit carried out in 2007. All three
pilot sites were therefore interested in
developing a direct access referral University Hospitals Birmingham NHS Foundation Trust
criteria and management pathway. Patient satisfaction levels with traditional Tinnitus pathway
The aims of the projects were to The trust conducted a postal satisfaction survey and 39 responses were analysed.
implement a direct access audiologist/
hearing therapist-led clinic, to
enhance patient satisfaction improve
tinnitus management outcomes and
reduce referral to treatment times.
Baseline information from pilot sites
identified the following key issues:
• Delay in patient access to
tinnitus management clinic of
between 12 and 28 weeks in the
pilot sites.
• Increased emotional impact of
tinnitus, reported by patients
who had a delay in access to
service.
*qualitative data from patient survey
www.improvement.nhs.uk/audiology14 | Pushing the boundaries: Evidence to support the development and implementation of good practice in audiology
What they did University Hospitals Birmingham How they did it
All sites set out to pilot a 'one stop' NHS Foundation Trust set out Pilot sites used a range of
direct access tinnitus service using a initially to triage ENT referrals, prior approaches to achieve goals:-
strict referral criteria. to publishing direct access service via • Set up steering groups and
Choose and Book appointment engaged/ influenced stakeholders
system. An additional 'one stop' including ENT consultants and trust
Direct access tinnitus referral clinic per week was set up to management. Patient
criteria accommodate direct access referrals. representatives attended steering
Adults, over the age of 16, The clinic was managed jointly by group meetings.
complaining of persistent, audiologists and hearing therapists, • Consulted with patients to
troublesome tinnitus should be and in collaboration with twelve ENT provide information about the pilot
referred directly to audiology. consultants. site project and obtain first hand
feedback about the historical
Exclusion criteria Contact pathway.
• Unilateral or asymmetrical Huw Cooper • Process mapped historical
hearing loss. Consultant Clinical Scientist, patient pathways and agreed
• Pulsatile tinnitus or tinnitus Huw.Cooper@uhb.nhs.uk new pathway, in collaboration with
described as a cracking, all stakeholders
popping or clicking noise Sherwood Forest Hospitals NHS • Worked collaboratively, with
• Persistent otalgia or aural Foundation Trust set out to ENT colleagues to agree direct
discharge affecting either ear implement one direct access clinic access referral criteria and safe
• Vertigo per week via Choose and Book. protocol for 'red flagging' those
Commissioners and users of service patients requiring to be seen by
contributed to the steering group. ENT consultant.
A range of different approaches to Following agreement of the new • Agreed protocols for audiology
setting up the service were used; pathway, public, primary and led request for MRI with ENT
secondary care communication consultants and processing via trust
Newcastle Upon Tyne NHS strategies were used to raise clinical governance processes.
Hospitals set out to provide the awareness. The clinic was managed • Reviewed methods of follow up
evidence to support the need for by one audiologist, in collaboration for patients by telephone, email or
change in pathway by a retrospective with three ENT consultants. clinic attendance.
patient record audit and working • Calculated future demand and
collaboratively with the Newcastle Contact capacity for service. Clinic
Upon Tyne Disability Forum Tinnitus Michelle Booth appointments were increased from
Support Group. They set up a focus Audiologist, Chief Audiologist, 45 to 60 minutes to allow more
group to identify the issues with the michelle.booth@sfh-tr.nhs.uk time.
current pathway and consulted with • Raised awareness of new
patients regarding their views on the pathway by effectively engaging
direct access service. They worked with the public, primary and
collaboratively with fifteen ENT secondary care via local community
consultants, to agree pathway, media and communication team
develop criteria for referral and strategies.
protocol for care. • Piloted a 'one stop' clinic for
patients with tinnitus.
Contact
Tom Davison
Senior Chief Audiologist,
tom.davison@nuth.nhs.uk
www.improvement.nhs.uk/audiologyPushing the boundaries: Evidence to support the development and implementation of good practice in audiology | 15
• Implemented method for using Improved patient experience; What patients said:
individual management plans
(IMP). This defined each patient's 'I understand this is a pilot scheme, it seems really good and
agreed needs and records any
agreed actions as they are
helpful. If at all possible, it should be continued, there is
completed. Patients are issued with more tinnitus out there than maybe is known'.
a written copy of their IMP as well
as information about tinnitus and Sherwood Forest Hospitals NHS Foundation Trust,
local support groups. Patient satisfaction postal survey
• Evaluated impact of service
using patient satisfaction, 'At the clinic they helped me; reassured me and helped me
improvements in tinnitus handicap
inventory, improvement in referral
get all the information I needed. I wish I could have got
to treatment times, number of there sooner. I now have hearing aids and live quite happily
follow ups and requests for MRI with my tinnitus.'
scans.
University Hospitals Birmingham NHS Foundation Trust,
Benefits Patient satisfaction survey
Quality
Improved patient experience -
Both pilot sites have demonstrated
that the direct access service Example of Direct Access Tinnitus pathway at University Hospitals
improved the patients experience and Birmingham NHS Foundation Trust
satisfaction levels of the service.
University Hospital Birmingham NHS
Foundation Trust found that greater
than 90% of patients felt that the
appointment was helpful and they
had to wait less time than expected.
Improved access and treatment
times - Pilot sites have demonstrated
significant improvements in access
and treatment times for patients
suffering from bilateral tinnitus. Both
sites reduced their wait times to less
than four weeks.
More optimum use of staff skills
in the pathway has led to ENT
consultants seeing the right patient University Hospitals Birmingham NHS Foundation Trust
at the right time. Andrew Reid, ENT • 15% (two out of the 13 patients seen) were 'red flagged' as requiring
Consultant, University Hospitals referral to ENT (due to unilateral nature of their tinnitus). One patient
Birmingham NHS Foundation Trust requested to see an ENT consultant for reassurance.
reports. • Potential for 187 ENT outpatient slots released (based on annual
referral demand of 220).
Sherwood Forest Hospitals NHS Foundation Trust
• 20% (Five out of the 25 patients seen) were 'red flagged' as requiring
referral to ENT with one patient requesting to see the consultant. 48%
were seen as one stop service
• Potential for 80 ENT outpatient slots released per annum (based on
annual referral demand of 120).
www.improvement.nhs.uk/audiology16 | Pushing the boundaries: Evidence to support the development and implementation of good practice in audiology
'This new pathway enables Prevention
Improving access and management
more effective access for of tinnitus has the potential to
other patients that require improve the quality of life as patients
may become less prone to sleep
an ENT opinion. Only a small
disturbance, anxiety, depression and
volume of patients with may enable more effective use of
tinnitus need a medical therapeutic drugs or psychological
support for patients. Robust clinical
opinion eg. Objective outcome data will need to be
tinnitus - these are pulsatile collected in order to validate these
assumptions.
tinnitus or complex patients,
of which tinnitus is a
symptom with multiple Commissioner Impact - NHS Nottinghamshire County supports
medical issues.' extension of pilot to gain a better insight into improved patient
experience and value for money of service:
Improved GP and public 'The team have been very enthusiastic and driven in making
awareness to enable more improvements to access and outcomes for adults with
appropriate referrals - Early
tinnitus. Early patient feedback is positive particularly about
findings from Sherwood Forest
Hospitals NHS Foundation Trust early access to the service and the excellent quality of care
suggest that their communication and advice given to them. As numbers of adults accessing
strategies raised both awareness with the service has been understandably small due to the
both GPs and the general public.
project timescales, I would be supportive of the pilot to
Innovation continue a little longer to gain a better insight into the
Direct access services are common clinical advantages, improved patients experience and value
place for hearing loss, however, direct for money of this service.'
access services for tinnitus is evolving.
The pilot sites demonstrate that the Ellie Bevan-Davies, Head of Procurement and Market Management
model of service provision should be at NHS Nottinghamshire County
based around matching the skills of
the professionals to the patient
needs.
Reference
Productivity 1. Davis A and El Rafaie. Epidemiology of tinnitus, In Tinnitus Handbook
Release of ENT outpatient (ed RS Tyler). Singular. Thomsom Learing. San Diego, 1-23. 2000.
appointments - This pathway has
the potential to release between
approximately 60 - 85% of ENT
tinnitus outpatient appointments.
Reduction in audiology/hearing
therapy follow up appointments -
Early findings at Sherwood Forest
Hospitals NHS Foundation Trust
illustrate potential reduction in new
to follow up appointments.
www.improvement.nhs.uk/audiologyPushing the boundaries: Evidence to support the development and implementation of good practice in audiology | 17
Balance
Introduction • Heart of England NHS Foundation • Benefits of supporting information
Community based studies in England Trust, Birmingham - A multi- to meet the individual patient's
and Scotland have suggested that 20- disciplinary team, based in an needs.
25% of the population experience urban area, working together
symptoms of dizziness/vertigo, with providing a joint consultation. Presenting issues
one quarter losing time from work. All three sites highlighted the need to
Summary understand the patient journey and
Referral pathways can be lengthy and In the balance projects, the flow of information. Each had
complex. At Heart of England NHS multidisciplinary teams worked with evidence that a large number of
Foundation Trust in Birmingham, patients to agree protocols and patients had seen several
patients were taking on average just clinical pathways, that improved professionals before being referred to
under five years to receive a diagnosis access to the appropriate the balance clinic.
and subsequent management of their professionals and investigations and
balance problem (HEFT Balance therefore led to earlier diagnosis and The teams wanted to develop and
Service Audit 2007). This is typical to treatment. Each of the three balance validate clear pathways, ensuring the
that found by other specialist balance sites developed a more coherent patient is seen by the most
services in the UK, with patients approach, providing consistent appropriate professional in a timely
seeing on average 4.5 specialists information to meet the needs of the way, removing steps that did not add
before receiving a diagnosis. individual. Patients with a better value. They were keen to involve all
understanding of their condition are the stakeholders and to develop a
Balance projects were undertaken by more likely to adopt recommended multidisciplinary service model.
three very different services; changes and agreed management
• The National Hospital for Neurology plans. Early management may prevent All of the sites struggled to obtain
and Neurosurgery, Queen Square, falls and development of associated robust data, as very little useful
London - a tertiary service led by conditions, such as depression. vestibular specific data had been
audio-vestibular medicine based at collected by the trusts. The use of
the National Hospital for Neurology The projects highlighted the outcome measures to monitor an
• Cambridge University Hospitals following emerging themes; individual's progress was inconsistent
NHS Foundation Trust (CUH) - a • Good clearly-communicated referral and the aggregated departmental
well established audio-vestibular protocols and pathways. data was not collected. This made
diagnostic and rehabilitation service • Opportunities for inter-professional collection of baseline data and
working in partnership with learning and extended roles. projection of potential benefits
otology/neurotology in a large • Patient engagement events difficult.
teaching hospital. The local highlighted the importance of early
catchment area is both rural and diagnosis and intervention.
suburban
www.improvement.nhs.uk/audiology18 | Pushing the boundaries: Evidence to support the development and implementation of good practice in audiology
What they did
Queens Square
• Introduced a one-stop balance
clinic with same day testing,
diagnosis, physiotherapy and
cognitive behavioural therapy (CBT)
• Implemented new patient triage
into uncomplicated and complex
balance patients, with experienced
audiologists assessing the
uncomplicated balance patients
using a red flag system
• Extended the use of outcome
measures and patient evaluation
forms and collated the results of
these to drive service improvement
• Production of patient information Laminated test information sheet developed at Queens Square
sheets on inner ear balance
problems, benign paraxysmal
positional vertigo (BPPV) and Cambridge University Hospitals Heart of England
migraine associated dizziness • Built upon existing clinical • Developed an improved network of
• Streamlining administrative partnerships (otology/neurotology) stakeholders by reviewing pathways
processes, as a result of the and consolidated a thriving and developing relationships with
process mapping session, the multidisciplinary team those who contributed to it
administration procedures were • Created a service topography data- • Used a range of innovative ways to
adjusted. set to be collected monthly and consult patients and involve them
reported back to the team in service developments
Contact • Produced a written patient pathway • Worked in partnership with local
Dr Rosalyn Davies and information leaflets for the commissioners and gained a better
Consultant in Audio-vestibular service understanding of costing the multi-
Medicine • Introduced written individual disciplinary joint consultation
rosalyn.davies@uclh.nhs.uk management plans (IMP) for service model
patients and made them available • Changed the pathway to enable
electronically to other professionals patients to access other specialist
• Implemented a patient outcome services without having to return to
measures protocol and established their GP for a new referral
a database to collate results • Agreed referral criteria for access to
• Enabled patient involvement in the services and for onward referrals
service and better communication into acute or specialist balance
between local professionals service.
managing balance patients.
Contact
Contact Amanda Casey
Katy Butler Hearing Therapist,
Clinical Scientist (Audiology), amanda.casey@heartofengland.
katy.butler@addenbrookes.nhs.uk nhs.uk
www.improvement.nhs.uk/audiologyPushing the boundaries: Evidence to support the development and implementation of good practice in audiology | 19
How they did it straightforward GP referrals in place thus the consultant was available to
Key stakeholders were identified and of audio-vestibular medicine (AVM). provide guidance and see patients. To
project teams established at each site, Taking detailed medical histories, ensure safe clinical practice, the
all included a physiotherapist. Each of examining patients, undertaking or consultant audited the 16 patients
the sites looked at demand and held arranging appropriate investigations, seen on this new pathway against a
process mapping sessions with making a diagnosis and agreeing red flag questionnaire developed by
stakeholders, then identified the appropriate management. This was the team.
steps in the process that were done in parallel with AVM clinics,
unnecessary and did not add value
(value stream analysis). Heart of
England included a patient
representative and her husband in Validation of triage of new patient referrals for
the session. She was able to articulate balance assessment and management
her experiences and feelings as she
travelled along the pathway in a
positive and constructive fashion. All
the stakeholders were then able to
collectively address any issues
identified and develop improved
processes and pathways. At Queens
Square the secretarial staff
highlighted duplication of work and
several systems being used to book
follow-up appointments, leading to
additional checking.
Each of the teams developed new
multidisciplinary pathways, to get the
patients to see the most appropriate
professionals at the right time,
reducing the number of visits. This
involved reviewing the skill set of the
team; at Queens Square the
experienced band 7/8 audiologists
received additional training so they
were able to see some
www.improvement.nhs.uk/audiology20 | Pushing the boundaries: Evidence to support the development and implementation of good practice in audiology
Patient and Public Involvement ‘The exercises I was given helped greatly
Each site wanted to improve the
quality of information provided to to give me confidence.’
patients and their families. This
Focus Group Patient
involved consulting with patients and
GPs, developing individual
management plans, new patient
information leaflets and diagnostic
test information cards. Benefits Sites are now using outcome
measures, although only small
The sites worked with reader panels Quality numbers were available at the time of
and produced a range of balance The enhanced quality is reflected in writing, they are able to demonstrate
related information leaflets. The title the quality enhancement tools (QET) improvements.
‘Migraine Associated Dizziness’ for scores, Cambridge University
one leaflet was a suggestion from a Hospitals NHS Trust used the relevant At Cambridge University Hospitals
member of the reader panel. QET sections to assess the quality of NHS Trust 80% of patients have
the balance service alone, in just nine individual management plans (IMPs)
All of the teams used patient months they managed to increase the completed within 48 hours of their
questionnaires, at Queens Square this number of sections achieving level A appointment. These are stored on the
highlighted issues with the waiting by 19%. trust patient management system
area, the audiologists are now along with vestibular assessment
feeding this back and working with MDT brings together specialists in reports, allowing the relevant
the architects designing the new managing balance focusing on the professionals trust wide access.
department. patients needs, providing evidence
based care that delivers the desired
Cambridge University Hospitals NHS outcomes.
Trust held a facilitated patient forum
to probe the issues important to their
users and changes made as a result
of their comments will be fed back.
Heart of England had an experienced
interviewer record a Discovery
Interview; they were able to share the
learning from this with the team and
other stakeholders. The team found
this very powerful, it highlighted the
importance of planning and training
in this technique, as the emotional
impact on the patients can be
profound.
www.improvement.nhs.uk/audiologyPushing the boundaries: Evidence to support the development and implementation of good practice in audiology | 21
An increased range of informative All sites anticipate a reduction in did
and up to date patient information not attend (DNA) rates, Heart of
leaflets are now available. England has been able to
demonstrate a drop in DNA rate for
Innovation vestibular function testing from 50%
Implemented joint patient to 5%.
consultations with MDT.
• Development of new pathways and Prevention
extended roles, ensuring a clinically • Patients able to return to work
effective and safe pathway. sooner and may be less prone to
• Consulted with and involved falls and chronic depression, more
patients in service review and evidence is needed to verify this.
development.
Productivity
The improved understanding and
data collection at the sites is to be
maintained and used to:
• understand and monitor demand
and activity
• facilitate service developments
• collate patient outcome measures
• communicate progress effectively
• support audit and research
• develop robust business cases
• determine cost of service.
• Clear protocols and use of red flags
resulted in more appropriate and
better quality referrals to the
correct professionals.
• Reduced costs as patients seen
sooner by the correct professionals
leads to less duplication of work
and unnecessary investigations.
• Reduced number of appointments
in the new pathways.
www.improvement.nhs.uk/audiology22 | Pushing the boundaries: Evidence to support the development and implementation of good practice in audiology
Collaboratively working with ENT to
redesign pathways
Introduction Summary providers who may have concerns
The Royal National Throat, Nose and Initial findings suggest that 75% of regarding the expansion of direct
Ear Hospital (RNTNE), at Royal Free ENT otological referrals did not meet access audiology services.
Hampstead NHS Trust, set out to pilot 'red flag criteria' and could
an audiologist-led triage assessment potentially be managed by the Presenting issues
clinic for new outpatient ENT diagnostic audiology department in a Traditionally, the majority of patients
referrals. Whilst RNTNE is a tertiary direct access service, by staff with the suffering from otological conditions
centre, a large proportion of work is appropriate skills and the ability to are referred to ENT and are seen in
also for the local population. The request MRI scans. This efficiency any of the 14 consultant clinics.
Trust also has a well-established could result in shorter waiting times Patients return for a further visit for
Audiovestibular Medical Department. for ENT. In 95% of cases, audiologists any tests and may either be followed
and ENT were in agreement as to the up by ENT or referred to
Patients referred to RNTNE may have referral pathway to audiovestibular audiovestibular medicine (AVM).
multiple appointments from ENT, medicine or ENT. AVM is not accessible via Choose and
audiology, ENT follow up Book.
appointments to referral to the This project demonstrates how
audiovestibular team to enable audiologists and ENT consultants Key issues identified with ENT
management of condition. This delay worked collaboratively to develop a audiology pathways were:-
in access can lead to considerable robust method to validate the • Delays in access to ENT and
distress for patients and impact on knowledge and skills of audiology threshold for referral on
their of quality of life. staff. This approach may be useful for to AVM
Traditional pathway for ENT otological referrals
www.improvement.nhs.uk/audiologyPushing the boundaries: Evidence to support the development and implementation of good practice in audiology | 23
• Inconvenience for patients as How they did it Benefits
multiple steps in pathway eg tests • Process mapped patient
often carried out after ENT pathways and agreed a new Quality
appointment pathway, in collaboration with all This pilot provides evidence for
• Perception that audiologists skills stakeholders optimum use of staff skills to enable
not utilised to full potential. • Conducted a prospective patient patients to be seen by the right
record audit to determine which person at the right time, enhancing
What they did otological referrals met 'red flag' the patient experience.
The overall aim of the project was to criteria for referral to ENT
streamline hearing, balance and • Set up an audiologist-led triage Innovation
tinnitus pathways using effective assessment clinic The approach to this pilot provides a
triage of ENT referrals by audiologists. • Developed a clinical assessment robust method to validate the
The team determined the number of proforma knowledge and skills of audiology
suitable referrals (i.e. did not meet • Developed a system for staff, where providers may be
any red flag criteria indicating referral recording outcome and cautious.
to ENT), and to validate skills of evaluating the assessment
senior audiologists to assess and process Productivity
make decisions regarding appropriate • Developed questionnaires to The new model would potentially
management. evaluate patient and staff release approximately 45 RNTNE
satisfaction with service. outpatient appointments with ENT
per week.
Findings from patients seen in the triage assessment clinic
22 patients seen in clinic - 20 % could potentially be seen and managed by
audiologist. An additional 55% could be seen if staff had the ability to request MRIs.
www.improvement.nhs.uk/audiology24 | Pushing the boundaries: Evidence to support the development and implementation of good practice in audiology
Adults with complex hearing needs
Introduction symptoms for, on average, 12 years Presenting issues
Referral of adults, with complex before being referred for the most Central Manchester University
hearing needs, from secondary care appropriate treatment. Hospitals NHS Foundation Trust,
providers to specialist tertiary centres audiology department at Manchester
is often dependent on knowledge Summary Royal Infirmary, provides
and skills of referring providers and Central Manchester University comprehensive secondary and tertiary
resources available for testing and Hospital NHS Foundation Trust, aimed services to patients. Much of the
management. Adults with complex to develop a service for adults with tertiary work arises from specialist
hearing needs may have undergone complex hearing needs which has referrals to the ENT department, and
several hospital visits prior to referral flexible yet clearly defined, pathways many of these referrals are patients
to a specialist centre for a of assessment and rehabilitation for with complex hearing needs.
comprehensive assessment. Whilst patients referred from providers
there are many providers with throughout the northwest region. The audiology team were interested
designated clinics for patients with in developing a service for adults with
learning disabilities there is a need to Initial findings from the pilot site complex hearing needs, which has
ensure that other patients with suggests delays in referral for optimal flexible, yet clearly defined, pathways
complex needs receive adequate management of patients with of assessment and rehabilitation for
appointment time and expertise to complex hearing needs. A key issue patients referred from the north west
meet their needs, in a timely manner. was the difficulty assessing demand region. Designated clinics for patients
for the service, due to varying with auditory processing disorders
It is vital that referrers are aware of management of patients by referring (APD) and learning disabilities were
specialist services to ensure patients providers. well established within the
receive prompt appropriate treatment department.
and to minimise any delays in their The project highlights the importance
pathway. Central Manchester of referring providers being aware of
University Hospital NHS Foundation specialist services to ensure patients
Trust found evidence to support that receive prompt appropriate treatment
there was variation in thresholds from and to minimise any delays in their
referring providers to specialist pathway. The development of a
services. For example, an audit of regional complex hearing needs
referrals to the Manchester cochlear network enables providers to achieve
implant programme indicated that this by working collaboratively to
patients with a severe to profound enable patients to receive the most
hearing loss had lived with their appropriate care.
www.improvement.nhs.uk/audiologyPushing the boundaries: Evidence to support the development and implementation of good practice in audiology | 25
Definition of Complex Hearing Need Assessment procedures set
Fluctuating hearing loss (e.g. Meniere's Disease) up in clinic room
• Pure Tone Audiometry (PTA)
Acoustic Neuroma (diagnosed) • Aided and unaided CUNY
NF2 (diagnosed) sentences (speech
Auditory neuropathy spectrum disorder (ANSD) discrimination with lip
Ski-slope audiogram reading)
≥50 dB octave difference between 0.5 and 4 kHz • Aided and unaided BKB
sentences (speech
Severe-profound hearing loss discrimination in quiet and
≥80 dB HL at 2 and 4 kHz noise)
Not CI candidates • Threshold Equalising Noise
Conductive hearing loss (TEN) test (for dead regions)
BC ≤20 dB HL with air-bone gap of ≥50 dB • Evoked potentials
Not BAHA/VSB candidates • Otoacoustic Emissions (OAEs)
Mixed hearing loss • Tympanometry and acoustic
AC ≥60 dB HL with air-bone gap of ≥30 dB reflexes.
Not BAHA/VSB candidates
Frequent (≥3) follow up/fine tune attendees
Suspected non-organic hearing loss • Evaluated impact of service by
patient satisfaction level, clinical
outcome measures and case studies
• Conducted an online survey of
There are some important issues that How they did it
local provider departments
need to be addressed when dealing • Set up steering group
• Set up a complex hearing needs
with this patient group and staff will • Agreed criteria for referral to
network.
need advanced diagnostic and clinic
hearing technology skills and • Process mapped historical
Benefits
equipment. patient pathways and agreed
The development of this clinic
new pathway, in collaboration with
provides many benefits in terms of
The team identified a need for a all stakeholders
clinical effectiveness and the
designated regional clinic for complex • Estimated demand for pathway
opportunity for professionals to learn
hearing needs patients and a regional • Piloted clinic 'Specialist Hearing
from peer review case studies.
network to agree referral criteria and and Rehabilitation Clinic
share learning from clinic. (SHARC)' for three months
Quality
• More clearly defined pathway and
What they did
continuity of care for patients.
• Defined complex hearing needs
• 66% of patients reported improved
• Piloted a Specialist Hearing and
level of satisfaction compared with
Rehabilitation Clinic (SHARC)
previous experience.
initially with internal hospital
referrals
• Conducted a survey of local
providers to determine service
provision for this patient group
• Developed a complex hearing need
network group for professionals
www.improvement.nhs.uk/audiology26 | Pushing the boundaries: Evidence to support the development and implementation of good practice in audiology
Innovation
Introduction of a designated clinic for ‘Being able to have a designated clinic for patients who
patients with complex hearing needs.
The establishment of a regional require more complex testing has allowed me as a clinician
complex needs hearing network is an to ensure I am giving my patient the best possible care in
example of how both secondary and the best environment. As we progress with our experience
tertiary providers can work
collaboratively. of non-routine testing we will be able to offer patients a
level of specialism and care more appropriate to their
Productivity needs. I envisage development of 'gold' standard testing
The development and agreement of
referral guidelines for local providers, and care pathways for these patients. I look forward to
via the regional network, will developing my clinical skills and shared learning with my
potentially lead to adults with colleagues’
complex needs being referred more
appropriately, at the right time, to the
right service to receive early ‘SHARC gives the audiologist the time and resources to
assessment and hearing intervention. help patients with non-routine hearing problems. The
It is anticipated that this will lead to a
reduction in the number of close links it has with other specialist services, such as
appointments offered either in local implants, means that patients can receive the most
provider or tertiary centre, with a effective treatment for them sooner and, therefore
consequential positive impact on cost
efficiency and waiting times. enhance the quality of their lives’
However, more robust data would Experience of staff working in SHARC - Staff responses:
need to be collected to validate this
assumption.
Contact
Martin O'Driscoll
Head of Audiology,
martin.o'driscoll@cmft.nhs.uk
Shahad Saeed
Pre-registration Clinical Scientist,
Audiology
shahad.saeed@cmft.nhs.uk
www.improvement.nhs.uk/audiologyYou can also read