Categorisation of medicines and prescribing and dispensing tools - BASt
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Categorisation of medicines
and
prescribing and dispensing tools
Katerina Touliou (CERTH-HIT)
Susana Monteiro, Silvia Ravera, Han de Gier (RUGPha, the Netherlands)
Sofie Boets, Uta Meesmann, Mark Tant (IBSR-BIVV, Belgium)
Sara-Ann Legrand, Trudy Van der Linden, Alain Verstraete (Ugent, Ghent University, Belgium)
Inmaculada Fierro, Trinidad Gómez-Talegón, Lourdes Martín Lara, Javier Alvarez (UVa, University of Valladolid, Spain)
November 2006
DRUID Final Conference, 28.09.2011 1
Rationale
• Professional guidelines provide the foundation for better and cost-
effective practice
• The rising of comparability in medical practice ensures the
development of collaboration between research findings and
evidence-based medicine
• The realisation of the need for alterations in existing guidelines
on the way physicians and pharmacists prescribe and dispense
medicines was a general goal of WP7
• Experts have formulated new guidelines and protocols within the
framework of the European DRUID project
November 2006
DRUID Final Conference, 28.09.2011 2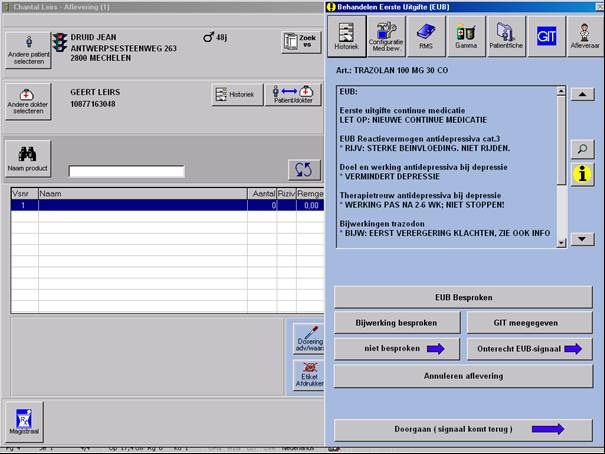
The study objectives
• Prescribing and dispensing guidelines developed within the DRUID project
were evaluated in clinical practice settings as one of the tasks in Work
Package 7
• The primary goal of this task was to evaluate the effectiveness of the
implementation of developed protocols and guidelines to healthcare
professionals’ (physicians, pharmacists, nurses):
– Attitudes/Awareness
– Knowledge
– Reported Behaviour
• via two different approaches:
– by using an integrated (ICT) tool
• additional software integrated into the ICT software used by the professional in his/her
daily practice; country specific development
– by using a non-integrated tool for presenting the protocols and
guidelines
• ICT tool developed within the framework of the project
November 2006
DRUID Final Conference, 28.09.2011 3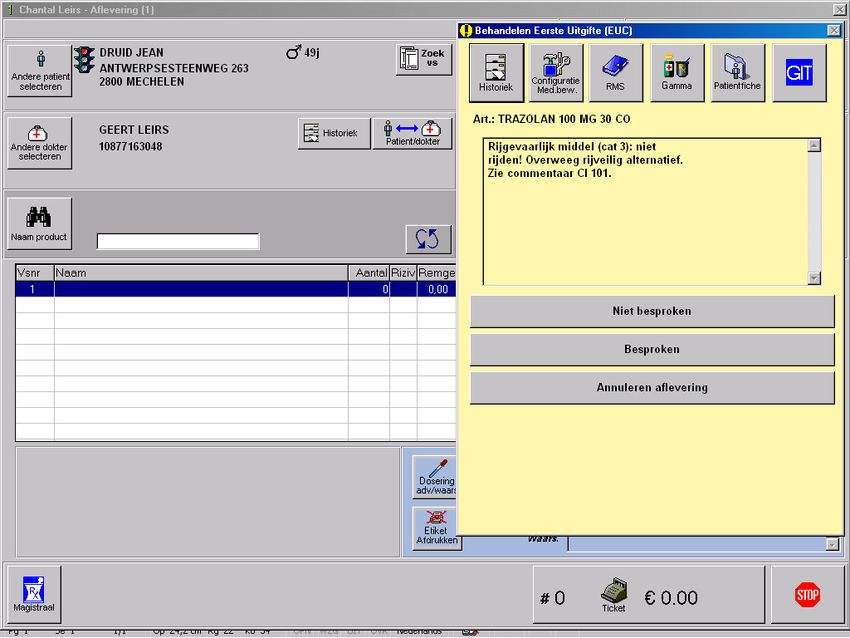
Design (1/2)
• The target populations were health care professionals in the primary care
setting:
– Physicians (Belgium, Spain)
– Pharmacists (Belgium, the Netherlands, Spain)
– Nurses (Spain)
• In addition, a “pure” control group was added to evaluate the effectiveness of
current practices with no DRUID-relevant information
• Participants were introduced to the tools/software(s) used through a training
scheme
• Used the software during their daily practice for either prescribing or
dispensing medicines depending on the professional groups they belonged
• Filled in a post-questionnaire investigating the same artefacts more or less
as the initial one in order to enhance and allow comparability and evaluate
the effectiveness of the tool and the applied guidelines
November 2006
DRUID Final Conference, 28.09.2011 4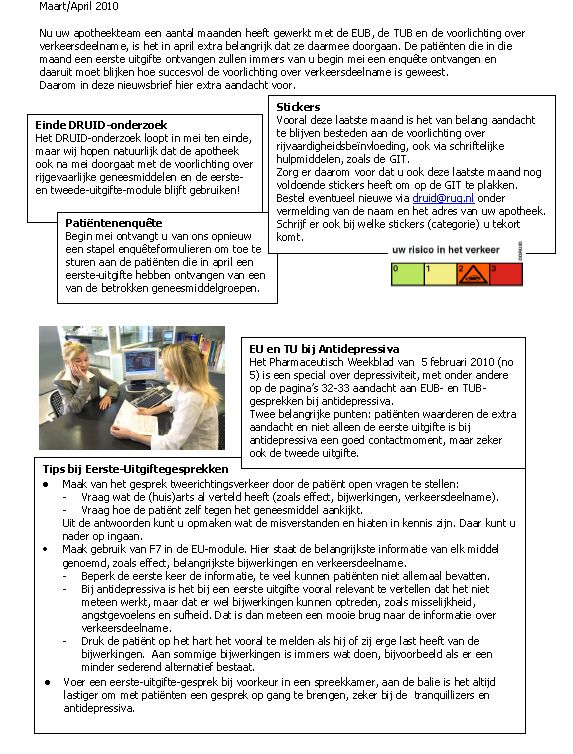
Design (2/2)
No information
66 months
months
No information
November 2006
DRUID Final Conference, 28.09.2011 5
DRUID information
• Information about the following medicinal categories:
– Anxiolytic (ATC:N05B)
– Hypnotic (ATC: N05C)
– Antidepressant (ATC: N05C)
• DRUID Medicines categorisation (0-III)
• Alternative medicines (less impairing effect on driving
behaviour)
• Guidelines about health care professionals
• Patient related information
November 2006
DRUID Final Conference, 28.09.2011 6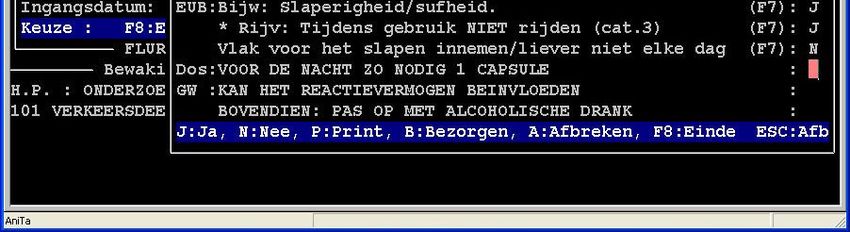
Categorisation and labelling
November 2006
DRUID Final Conference, 28.09.2011 7
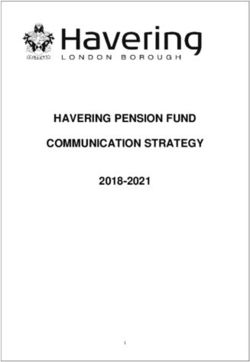
The DRUID tool
Selecting ibuprofen (continued)
Select the substance out of the list with
all names starting with the typed
characters.
November 2006
DRUID Final Conference, 28.09.2011 8
SoSoeMe for physicians (Belgian study)
November 2006
DRUID Final Conference, 28.09.2011 9
Pharmacom® for pharmacists (Dutch study)
November 2006
DRUID Final Conference, 28.09.2011 10ViaNova for Pharmacist (Belgian study)
November 2006
DRUID Final Conference, 28.09.2011 11Materials
• Pre and post 1 Background information (7 items)
Aiming at gathering information about basic demographic,
questionnaires were educational background and expertise of participating
professional.
administered to all 2 New Technologies Literacy (6 items)
As already discussed in the Glossary, this cluster
contained items that would target to investigate the
participants in all test sites familiarity of the participant with similar tools and,
therefore, their willingness to apply them in everyday
medical practice.
• Each site slightly adapted 3 Attitudes/Awareness (6 items)
Professional judgments on medicines and driving were
the questionnaire to their 4
investigated.
Reported Behaviour (8 items)
These questions reflected what the professionals actually
country study needs do in their daily practice.
5 Sources (4 items)
In order to get an idea of the various sources professionals
• Pre and post use in order to gather information and knowledge, this
section was added.
questionnaires provided 6 Actual knowledge (5 items)
Investigate acquired knowledge on medicines’ effect in
driving behaviour.
the basis for the 7 User acceptance (pre-2 items)
How willing are to use such a tool prior testing phase
investigation of the begins.
8 User acceptance (post tool-8 items)
Acceptance of the content and the functionalities of the
effectiveness of the tools tool after the testing phase ends.
9 Future use of the tool (3 items)
and the implemented For what searches they would more likely use the tool for
and which tool they preferred.
guidelines
November 2006
DRUID Final Conference, 28.09.2011 12Newsletters
The importance of a good follow up
November 2006
DRUID Final Conference, 28.09.2011 13Previous education/training
Physicians Pharmacists
• 74% of participants had • 67% of participants had
not received any type of not received driving
training/education related education on the
regarding medicinal effect of medicines on
effects on driving driving
behaviour
• With the exception of the
Spanish study that 51%
of participants had
received related
education
November 2006
DRUID Final Conference, 28.09.2011 14Previous education about the effects
of medicines on driving
November 2006
DRUID Final Conference, 28.09.2011 15Pharmacists
November 2006
DRUID Final Conference, 28.09.2011 16The Belgian study (1/2)
• Significant positive
changes in reported
behaviour and
medicinal risk specific
knowledge
• These changes were
found for the integrated
tool after training and
the six-months
intervention period
• Limited change in
attitudinal and
awareness questions
• DRUID dispensing
guidelines were well-
accepted and liked
November 2006
DRUID Final Conference, 28.09.2011 17The Belgian study (2/2)
High importance of having a support system integrated in
their daily practice as long as it is:
– Integrated into their daily software
– Updates automatically
– Easy to use
– Focus on first deliveries
– Cost-and time-efficient
– Contains concrete and detailed information
– Contains safer alternatives
November 2006
DRUID Final Conference, 28.09.2011 18The Dutch study (1/2) • Pharmacists awareness increased both before and after the training every time the patient was: – a professional driver (above 90%) – drove frequently (above 85%) – drove long distances (above 80%) • Increased awareness, knowledge, and reported behaviour but still positive change was attained after training • Significant increase in awareness (p
The Dutch study (2/2)
Number of participants
per study group
Knowledge about causes of road
accidents increased after training
November 2006
DRUID Final Conference, 28.09.2011 20The Spanish study • Increased reported behaviour (p
Physicians
Results
November 2006
DRUID Final Conference, 28.09.2011 22The Belgian study
• Only for the integrated group a significant pre-post change was
found with regard to the reported behaviour questions
• The SoSoeMe participants provided the patient significantly more
with written information materials after the trial period
• Willingness to use a prescribing support tool when this tool is:
– integrated in their daily used software
– asks no extra efforts or time to update
– is easy to use and
– contains practical information
• The physicians underlined the need for more information on the topic
‘medicines and driving’
• This information should not only be made available to physicians but
also be integrated in the patient leaflet or on the medicine box
November 2006
DRUID Final Conference, 28.09.2011 23The Spanish study
• Pharmacists did not
significantly change their
dispensing habits or their
attitudes towards
medicines and
Pre-Post knowledge composite score. Samples' percentages on
driving(p>.05) 45
each puntuation
• Their knowledge about the 40
potentially detrimental 35
Total sample %
30
effects of medicines on 25
driving behaviour 20
increased (pNurses
Results
November 2006
DRUID Final Conference, 28.09.2011 25Nurses
• No significant differences after the training
• Nursing staff (58%) does not use integrated tools as often
as pharmacists (99%) but almost as often as physicians
(65%)in order to access information about medicines
– This finding may result from the close collaboration of
physicians and pharmacists
November 2006
DRUID Final Conference, 28.09.2011 26Patients
November 2006
DRUID Final Conference, 28.09.2011 27The Dutch study
• Patients’ knowledge about causes of road accidents did not significantly change
after the training.
• In patients’ opinion, pharmacists are the preferable source of information about
medicines and its use
– This information is often spontaneously provided to patients, especially after the training
• During a pharmacy consultation, patients were mainly informed about the influence of
medicines on driving fitness and on operating machinery and about the severity
of the impairment
• The majority of the patients decided not to change their driving frequency, despite the
information that was provided to them by their healthcare provider
– This did not change depending on neither the pharmacy group nor time of measurement
• Patients’ attitudes towards the use of driving impairing medicines while driving and
concerning the consequences on the use of driving impairing medicines while driving
were not influenced by the pharmacy group or the time of measurement
November 2006
DRUID Final Conference, 28.09.2011 28The Spanish study
• 1385 patients responded and filled in the questionnaire when the
patient visited a health service or a pharmacy
• The majority of patients knew that some medicines can influence
fitness to drive
• Most patients (83.4%) interviewed would reduce their driving
frequency if they were prescribed a “medicine which has the
pictogram concerning driving on the packaging”
November 2006
DRUID Final Conference, 28.09.2011 29Overall conclusions & recommendations
November 2006
DRUID Final Conference, 28.09.2011 30Overall conclusions
• Decision support tools are welcome and usable
• DRUID materials fulfilled a need and most participants anticipated
the ultimate integration of these materials to their own software
packages
• The implementation of computerised guidelines and DRUID
categorisation was well accepted as practical information by both
physicians and pharmacists and participants were willing to
continue using the DRUID information if integrated in their
prescribing and dispensing computer systems for easier
incorporation in their daily practices
• Participants offered ideas for future developments :
– inclusion of other medicines in the categorisation scheme
– the information should be adjusted to the native language
– inclusion of specialised and elderly directed advices incorporated in the system
– adaptation to other target groups and not only drivers (e.g. heavy machinery usage)
November 2006
DRUID Final Conference, 28.09.2011 31Future directions
• A long term goal would be to evaluate the impact to the health care
system and to various stakeholder groups associated with the
implementation of health care professionals’ guidelines and compare
it with other related studies’ findings
• Further research could facilitate its adaptation and customisation
for different groups of health care professionals and national settings
• A set of DRUID recommendations has been derived from the main
conclusions of both composite cross comparisons and country
studies
• The key message is clear about the necessity of diffusion of
DRUID information to physicians, pharmacists, and nurses in all
clinical settings
November 2006
DRUID Final Conference, 28.09.2011 32Recommendations-Integrated tools
• DRUID guidelines should be incorporated into
integrated tools to maximise potential for successful
implementation and consequently be more effective and
efficient in daily practice
• DRUID guidelines should be available in native
languages to avoid any difficulties time spend because
of misinterpretations
• The DRUID categorisation system could serve as a tool
to improve prescribing and dispensing practices both at
national and European level
November 2006
DRUID Final Conference, 28.09.2011 33Recommendations-Health care professionals
• The effective implementation of DRUID guidelines would be
enhanced and maximised by the productive collaboration of
different groups of health care professionals involved in
prescribing/dispensing medicines with regard to patient decision
making
• The DRUID warning label could be applied in order to facilitate
health practitioners’ and patients’ communication
• Pharmacists should be informed about safer alternative medicines
with regard to driving
• DRUID guidelines should be personalised and adapted to:
– local services idiosyncrasies
– local strategies
– cultural perspectives
– legal/political frameworks
November 2006
DRUID Final Conference, 28.09.2011 34Recommendations-Patients
• Patients should be trained about the impairing effects of
medicines and the potential consequences
– training should be adjusted to general population and probably
through edutainment
• A straightforward grading system and description of
actions to follow could be included in the patient leaflet
(the warning label could be printed on the medicine box)
similar to the one described for health care professionals
November 2006
DRUID Final Conference, 28.09.2011 35Recommendations-Methodology
• The conduction of evidence based studies seriously
benefits from:
– face-to-face communication
– close follow up (e.g. reminders, newsletters)
– concrete set of instructions (i.e. productive assistance)
• Training is essential for the success of DRUID
guidelines and support throughout the testing phase
• The latter can be translated into continuous education
for natural health settings
November 2006
DRUID Final Conference, 28.09.2011 36November 2006 DRUID Final Conference, 28.09.2011 37
You can also read