Caribbean Cooperation in Health Phase III (CCH III) - "Investing in Health for Sustainable Development" Phase III
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Caribbean Cooperation in Health Phase III (CCH III) a
Caribbean Cooperation
in Health Phase III (CCH III)
Regional Health Framework 2010 - 2015
“Investing in Health for
Sustainable Development”
Phase III
b Caribbean Cooperation in Health Phase III (CCH III)

Caribbean Cooperation in Health Phase III (CCH III) i
Caribbean Cooperation in Health Phase III
(CCH III)
Regional Health Framework 2010 - 2015
“Investing in Health for
Sustainable Development”
ii Caribbean Cooperation in Health Phase III (CCH III) Contents Foreword...............................................................................................2 Guiding Principles and Strategic Approaches...........................................3 Executive Summary...............................................................................4 I - Introductioin.....................................................................................8 II- Overview of the Health Situation........................................................11 III - Challenges We Face....................................................................... 14 IV - Priority Areas And Strategic Objectives............................................17 V - Management And Coordinating Mechanisms..................................... 23 Annex 1...............................................................................................26

Caribbean Cooperation in Health Phase III (CCH III) 1 Foreword

2 Caribbean Cooperation in Health Phase III (CCH III)
GUIDING PRINCIPLES AND STRATEGIC APPROACHES
The CARICOM member states are called upon to Solidarity
endorse and apply principles and strategic approaches
The people and institutions in the Caribbean working
as the commitment to achieving health goals. In
together to define and achieve the common good.
this regard CCHIII aims to facilitate the necessary
regional response to support country efforts towards People Centred
regional public goods and services and national Common health needs will be addressed as public
strategic directions. goods that all member states identify with and support
The Primary Health Care Approach will be the broad by virtue of their relevance to the national situation
over-arching health development framework which and the desire to promote health of the community as
will guide the health development in this region. The a whole. The ultimate aim is to get people healthy and
guiding principles reflect the foundation upon which to keep them healthy. This means that our regional
all interventions will be planned, implemented and initiatives must have as their main aim meeting the
evaluated. needs of the people, families and communities of the
region.
The right to the highest attainable level of
health Leadership
Health is a fundamental human right. Every citizen Public health leadership is a major priority. The at-
of the Caribbean has a right to the highest attain- tainment of Health for All will be dependent on
able level of health and therefore services must be leadership that shares regional vision and creates
responsive to people’s health needs. In addition, an enabling environment for mobilising resources,
there should be accountability in the health system, improving performance,
increased efficiency and ef- ensuring greater trans-
fectiveness whilst effecting parency and account-
no harm. ability of regional health
systems.
Equity
Working towards eliminating
unfair differences in health
status, access to health care
and health enhancing environ-
ments, and treatment within
the health and social services
system.
Caribbean Cooperation in Health Phase III (CCH III) 3
VISION AND GOAL
Caribbean Cooperation in Health (CCH III):
“Investing in Health for Sustainable Development”
4 Caribbean Cooperation in Health Phase III (CCH III)
Executive
Summary
Caribbean Cooperation in Health Phase III (CCH III) 5
Executive Summary
The countries of the Caribbean are proud of the Nassau Declaration and the 2007
gains in health which they have made. The suc- Declaration of Port of Spain re-
cess of these achievements, namely combating inforce the Millennium Declara-
serious public health problems such as poliomy- tion aimed at reducing poverty by
elitis, measles, and cholera, provide significant 2015. The CCH also recognizes
evidence of what can be achieved through a col- and aims to address the priority is-
lective regional response which supports develop- sues identified in the Report of the
ment at the national level. The Caribbean Coop- Caribbean Commission on Health
eration in Health (CCH) represents a mechanism and Development. The CCH III is
to unite Caribbean Territories in a common goal charged with the responsibility to
to improve health and wellbeing, develop the pro- invest in the people of the region
ductive potential of the people, and, by definition, to ensure the highest attainable
the competitive advantage of the region. Greater standard of health, reduce ineq-
efforts will be made to support Haiti, the newest uity, and mobilise traditional and
member of CARICOM to achieve these goals. non-traditional actors in tackling
Major regional and international policy and stra- health challenges and building
tegic guidelines serve as the backdrop against sustainable health systems.
The mandate of CCH III 2009-
2015 will address a new orientation
towards
• People-centred development,
• Genuine stakeholder and
community participation and
involvement,
• Effective regional coordina-
tion and public health leader-
ship,
• Outcome-oriented planning
and implementation and per-
formance-based monitoring,
and
• Resource mobilisation for
health, health coverage, and
social protection for the peo-
which the new Regional Strategic Framework ple of the region.
has been developed. This framework is a di- This framework represents a com-
rect response to the commitments made by the prehensive health and develop-
Caribbean Community (CARICOM) Heads of ment strategy for the Caribbean
Government in both regional and international region. The framework seeks to
declarations and policy guidelines. The 2001 break free from the overemphasis
6 Caribbean Cooperation in Health Phase III (CCH III)
on the disease model. While it acknowledges the im- The details of the program areas and indicators of
portance of sustaining health gains, and completing achievement are outlined in the matrices of the CCH
the unfinished health agenda, it proposes an empha- III. These matrices are available on www.caricom.org
sis on strengthening the building blocks of joint ac- and www.carpha.org.
tion in health. The CCH III therefore maintains the The Regional Health Institutions (RHIs) have played
eight priority areas as defined in CCH II. a significant role in supporting the implementation
The eight priorities are: of the Caribbean Cooperation in Health at both re-
1. Communicable Disease gional and national
2. Non-Communicable levels. The establish-
Disease ment of the Carib-
bean Public Health
3. Health Systems
Agency (CARPHA)
Strengthening
as mandated by the
4. Environmental Health Heads of Government
5. Food and Nutrition in March 2010 will in-
6. Mental Health tegrate the functions
7. Family and Child Health and administration
8. Human Resource of the existing five
Development Caribbean Regional
Health Institutions
In looking at the determinants of (RHIs); the Carib-
these priority areas, it was recog- bean Epidemiology
nized that the strategies/actions Centre (CAREC), the
which need to be adopted in or- Caribbean Food and
der to have any significant impact Nutrition Institute
on these priority areas needed to (CFNI), the Carib-
be: bean Environmen-
• Cross cutting tal Health Institute
• Inter-programmatic (CEHI), the Caribbean Regional Drug Testing Labo-
• Trans-sectoral ratory (CRDTL) and the Caribbean Health Research
• Focused on the determinants of health Council (CHRC)). The proposed agency will ratio-
The CCH III therefore identifies five project goals nalize the functions of the current RHIs and have a
which have expected results that are inter-sectoral more comprehensive mandate in addressing the pub-
and inter-programmatic, addressing the eight pri- lic health needs of the wider Caribbean Region and
ority areas while aiming to achieve the stated goal will be a critical success factor in the implementation
“Investing in Health for Sustainable Development”. of the CCH III.Caribbean Cooperation in Health Phase III (CCH III) 7
Major Regional and International Guidelines:
• The Nassau Declaration
http://www.caricom.org/jsp/communications/meetings_statements/nassau_
declaration_on_health.jsp?menu=communications
• The 2001 Declaration of Commitment to the Pan Caribbean Partnership
Against HIV/AIDS – “Provide supportive environment for the collaborative
response to fighting HIV/AIDS
http://www.caricom.org/jsp/secretariat/legal_instruments/caribbean_
partnership_commitment.jsp
• Report of the Caribbean Commission on Health and Development
http://www.who.int/macrohealth/action/PAHO_Report.pdf
http://www.vision2020.info.tt/pdf/Policies%20and%20Procedures/Policy%20
Documents/Overview%20CCHD%20HOG.pdf
• Needham’s Point Declaration
http://www.caricom.org/jsp/pressreleases/pres167_07.jsp
• Declaration of Port of Spain – “Comprehensive and Integrated Approach to
the Control of CNCD”
http://www.caricom.org/jsp/pressreleases/pres212_07.jsp
http://www.caricom.org/jsp/community/chronic_non_communicable_diseases/
summit_chronic_non_communicable_diseases_index.jsp
• The Millennium Declaration and Development Goals – “ Reducing poverty
related inequalities by 2015”
http://idbdocs.iadb.org/wsdocs/getdocument.aspx?docnum=591088
http://www.unmillenniumproject.org/goals/index.htm
http://www.undp.org/publications/MDG_Report_2008_en.pdf
• Declaration of Montevideo on the New Orientations for Primary Health Care
– “Designing people-centered care through a Primary Health – care based
system)
http://www.paho.org/English/GOV/CD/cd46-decl-e.pdf
• International Health Regulations (2005)
http://whqlibdoc.who.int/publications/2008/9789241580410_eng.pdf - ISBN
978-92-4-158041-08 Caribbean Cooperation in Health Phase III (CCH III)
Introduction
A Regional LandmarkCaribbean Cooperation in Health Phase III (CCH III) 9
I - Introduction
A Regional Landmark The main thrust of the CCH initiative is to identify
The Caribbean Cooperation priority health areas and use
in Health (CCH) represents them as vehicles to1
a mechanism to unite Carib- • Foster technical coop-
bean territories in a com- eration among the coun-
mon goal to improve health tries;
and wellbeing, develop the • Optimise the use of re-
productive potential of the sources;
people, and, by definition, the
• Develop projects in the
competitive advantage of the
priority areas as a way to
region at the global level.
foster cooperation and
The concept of the Caribbean collectively focus on ar-
Cooperation in Health was eas of highest priority;
introduced in 1984 at a meet- and
ing of the CARICOM Con- • Mobilize all national and external resourc-
ference of Ministers responsible for Health (CMH). es to address the most important health problems in
The initiative called for collaborative action in health the Region.
among the Countries and Institutions of the Caribbe-
“Investing in Health for Sustainable
an Region. CCH II (1993) was a landmark in Carib-
bean cooperation and CCH has focused on collective Development “
action with optimisation in the use of resources over a This new strategic framework is a direct response to
given period, addressing commonly agreed upon ob- the commitments made by the Caribbean Community
jectives in priority health areas of common concern. (CARICOM) Heads of Government in both regional
The Bahamas
Atlantic O cean
Jamaica Antigua and Barbuda
St. Kitts and Nevis
Belize
Dominica
Ca r i b b e a n S e a Saint Lucia
St. Vincent & the Grenadines Barbados
Grenada
Trinidad & Tobago
Guyana
Suriname10 Caribbean Cooperation in Health Phase III (CCH III)
and international declarations and policy guidelines. The Reports of the Caribbean Commission on Health
The 2001 Nassau Declaration and the 2007 Decla- and Development and the Commission on the Social
ration of Port of Spain reinforced the Millennium Determinants of Health revealed the persistent and
Declaration aimed at reducing poverty by 2015. The growing inequalities in health and weak health sys-
CCH Phase III is charged with the responsibility to tems. Evidence of these shortcomings includes:
invest in the health of the people of the region to en- • The continued lack of resources for health,
sure the highest attainable socioeconomic achieve- • Limited attempts at universal population cover-
ment, reduce inequities in health, and mobilise tra- age to address new and emerging health prob-
ditional and non-traditional actors in tackling health lems e.g. non-communicable diseases, mental
challenges and building sustainable health systems. health,
• The mandate of CCHIII 2010-2015 will address • Inadequate access to quality health care services,
a new orientation towards: • Weak leadership and governance of the health
• People- centred development,
sector, and
• Genuine stakeholder and community participa-
• Inadequate evaluation and monitoring mecha-
tion and involvement,
nisms to chart progress and inform health action.
• Effective regional coordination and public health
leadership, Implementation of the new orientation is supported
• Outcome-oriented planning, implementation by the Needham’s Point Declaration (2007) which
and performance monitoring, proposes to use functional cooperation as the means
• Increased efforts at resource mobilisation for of delivering agreed Common Public Goods.
health, health coverage, and social protection for
The chapters which follow outline the new regional
the people of the region, and
strategic framework.
• “A Community for All”.Caribbean Cooperation in Health Phase III (CCH III) 11
Chapter two summarises the health challenges facing areas and Strategic objectives for CCH111. This chap-
this region and reinforces the need for collaborative ter details the areas for joint collaborative action in
responses to these common issues. the Region to achieve the five strategic project goals.
Chapter three presents the lessons learnt and justifies Chapter five discusses the Management and Coordi-
the approach for the nating mechanisms. The critical success factors are
new CCHIII man- discussed including
date “Investing in the regional coordinat-
Health for Sustain- ing mechanism for suc-
able Development”. cessful implementation
at the national and re-
Chapter four de- gional level.
scribes the Priority12 Caribbean Cooperation in Health Phase III (CCH III)
An OverviewCaribbean Cooperation in Health Phase III (CCH III) 13
II - An Overview of the Health Development Challenges
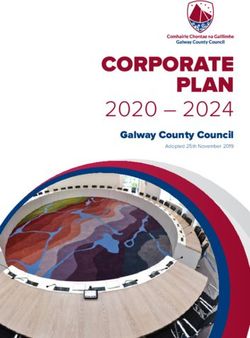
Overview of the Health Situation of the The overall population has doubled in the last 50
Region years, but the proportion of the population aged less
than 15 years has been declining, while the population
The regional and international policy discourse has
aged over 60 years has been increasing. Population
elevated the importance of the social determinants of
dynamics for 2010 reveal that the child population
health in health development planning. Recognition
is stable or decreasing, population aged 25-64 years
of the importance of changing social norms (related to
will increase by 13% and the labour force population
violence, injuries, sexual behaviour,
and environmental management)
will become more important as Population Pyramid for the Caribbean - 2010
Caribbean societies advance in the
Age - Group
new millennium. While disease
65+
prevention and treatment have
played a significant role in securing 75-79
our health status gains and will
remain critical, equally important 65-69
will be the increased recognition of 55-59
health as a tool for development and
45-49
well being.
Sustainable health systems will 35-39
be needed to support the goal of 25-29
“Health for All”. Use of integrated
comprehensive multi-sector 15-19
measures including information 5-9
and communication networks, legal
and fiscal reform and healthy public 400 300 200 100 0 100 200 300 400
policies, will necessitate new ways Thousands Male Female Thousands
of working with traditional and non-
traditional partners, in the public
and private sectors of national,
regional and international entities.
will comprise 65% of the total population. The
Demographic and Social Indicators greatest population increase will be in the 45-64 year
The countries of the Caribbean are undergoing a old group, with a rate of increase of >10,000 per year.
demographic transition. Demographic indicators of Persons 65+ will constitute 10% of total population.
most Caribbean countries are consistent with health Birth and fertility rates are significantly higher in
conditions expected for middle income countries Haiti compared with the rest of the Caribbean.
with the exception of Haiti. Today, both men and
The current demographic transition has implications
women live longer, with women living on average four
for increasing rates of chronic non-communicable
to six years longer than men.
diseases, and an increasing need for care of the14 Caribbean Cooperation in Health Phase III (CCH III) elderly. Increased urbanisation is also making its Emerging and Re-emerging Infectious contribution to increased rates of life style diseases. Diseases The Caribbean has benefited from universal access to Among the diseases subject to the International good primary and secondary education. Its high rates Health Regulations (2005) and global surveillance, of literacy have been fundamental determinants of only yellow fever and cholera are of real concern to good health and essential in sustaining health gains the Caribbean Region. The possibility of importation and achieving social and economic development. into the islands exists. Maintenance of phytosanitary Mortality standards are also important to our trade in food The disease epidemiology of the region is products. characterised by the coexistence of consequences Whilst malaria is more dangerous where it exists, of communicable diseases with those of chronic, dengue fever has become the more significant vector- degenerative illnesses4, including heart disease, borne illness for the CARICOM States. The threat of strokes, diabetes, and cancer, as well as with other re-introduction of malaria is real, as evidenced in the health priorities such as injuries, violence, trauma, recent outbreaks in Jamaica and Bahamas. This now occupational disease and mental illness. Chronic demands risk reduction strategies and maintenance diseases have replaced communicable diseases as of outbreak detection and response capacity where leading causes of death and ill-health. risks are high. Mortality from communicable diseases has been The Caribbean boasts of high rates of childhood rising since the late 1980s, after years of decline. This vaccination. Smallpox and polio have been eliminated. is linked in particular to the epidemic of HIV/AIDS, The elimination of measles is now only to be certified. but more recently to vector-borne illnesses such as On the heels of the measles elimination will follow dengue and malaria. In childhood, while infections mumps, rubella and Congenial Rubella Syndrome. have decreased as a cause of illness and death, nutrition-related illness or risk factors for illness Economic Challenges such as obesity have increased. In early adulthood, Most countries of the region are deemed to be diabetes, suicide and homicide have increased as of middle income status. However, considerable causes of death over the past 10-15 years. challenges persist in maintaining economic stability While national and regional statistics show that and viability. The current global economic challenges chronic non-communicable diseases are the leading have created increased pressures on Caribbean causes of death for the population, HIV/AIDS, economies and will eventually challenge their injuries, and violence are the leading causes of death competitive advantage in key sectors such as tourism, among the youth and population of productive and as recovery begins. reproductive age. Climate change Risk Factors Climate change can affect, and has affected, the Current studies in Behavior Risk Factor Surveillance agricultural economies of the Caribbean. The effects will greatly assist in identifying the risk factors most of climate change threatens beaches and low-lying dominant in influencing the increasing incidence of coastal zones and will have an enormous potential non-communicable diseases (NCDs) in all the states. to impact livelihoods. Catastrophic hurricanes and The known risk factors of tobacco use, physical frequent floods have inflicted damage to health and inactivity, unhealthy nutrition, and alcohol misuse, other infrastructure, and impacted food security. will no doubt feature prominently. Similar studies In addition, the health impacts of the increased will have to be undertaken in relation to accidental vector borne diseases like dengue is already being and intentional violence. witnessed.
Caribbean Cooperation in Health Phase III (CCH III) 15 Challenges We Face
16 Caribbean Cooperation in Health Phase III (CCH III)
III - Challenges We Face
The lessons learnt from the design and implementation and partners, including the private sector, in the
of the CCH I and CCH II have been carefully new global health environment
considered in this new planning and implementation Resource Mobilisation and Efficiency
stage.
Resource constraints were identified as one of the
Governance main barriers to the successful implementation
The importance of governance and stewardship in of health initiatives. There is need for greater
the region cannot be understated. There is need emphasis on a more strategic approach to resource
to prioritise efforts at ensuring sound leadership mobilisation for health and an understanding of
to bring about change in our complex regional the real cost of achieving health outcomes. It is
generally agreed that recent economic growth
environments. Equally important is the need to clarify
brought additional resources to health, though the
the monitoring roles and functions of all stakeholders
more recent global and economic and financial crisis
and responsible agencies.
now puts their sustainability at risk. However, this is
Weak structural and institutional operations were accompanied by the growing demand for health and
identified as major weaknesses in the execution of better performance. The Caribbean Region will have
CCH I and CCH II. to show better results in programme planning and
• Limited effectiveness and efficiency in the deliv- implementation and the link to health development
ery and financing of functional cooperation ini- if it is to secure much-needed funding for health.
tiatives Pooled financing of country needs and priorities
• Lack of adequate resources for the implementa- can help increase the relevance of interventions and
tion of developmental health initiatives address the lack of capacity in country. The lack of a
• Absence of sustainable approaches to health de- clear financial strategy to support the implementation
velopment of the regional strategic direction must be addressed
in this new orientation. The new framework must
• Inadequate emphasis on performance manage-
demonstrate greater integration among the strategic
ment
objectives to reduce duplication and better utilise
• Inadequate focus on knowledge creation and
scarce resources. This will require the following:
management • Refinement of overlaps, consolidation and priori-
• Insufficient staff and technical resources to coor- tisation of some interventions,
dinate and inform implementation processes • Feasibility studies, and
• Weak strategy for monitoring performance and • Greater focus on cross sectional opportunities.
competence of the regional human resources
• Inadequate harmonisation and alignment of re- Capacity
gional programmes and policy declarations in The issue of limited human resource capacity in
health the region calls for a new strategy to reversing
• General lack of strong leadership and governance the negative impacts of professional migration.
in the field of health at all levels of the system Equally important is the need to enhance skills and
• Lack of a truly regional approach to address the competencies of our human resources and also the
unimplemented health agenda institutions responsible for nurturing and training
• Inadequate emphasis on and support for explor- minds. Standards of quality in all educational
ing the potential of non-traditional stakeholders institutions need to be enhanced.Caribbean Cooperation in Health Phase III (CCH III) 17
Participatory Strategies and Stakeholders in Areas where common public goods have been derived
Health include cross-regional frameworks for the control of
NCDs and HIV/AIDS, development of HIS, reporting
Given the intersectoral nature of health and the on health status, and strengthening the regional
importance of all sectors in the achievement of health mental health response. While resource constraints
outcomes, the multi-sector approach in health is may prohibit a closer examination of health tourism,
gaining prominence. Private sector and other non- the role played by this sector cannot be ignored.
traditional sectors can play a meaningful role in the
implementation of CCH III. Monitoring and Evaluation
How we engage our stakeholders will determine the Performance–based funding is presently being
degree and quality of different forms of participation. used by many funding agencies to chart progress
The regional focus will make this issue all the more and performance in use of funds for stated health
challenging. Enhancing stakeholder buy-in, and interventions. The establishment of monitoring
engendering a truly multi-sector and intersectoral and evaluation mechanisms and effective health
approach will require continued use of top down and information systems to chart progress is critical
to securing funding for health and ensuring the
bottom-up approaches involving policy guidance and
following:
genuine input from countries and institutions.
• Effective and efficient programme implementa-
Priority Health Areas tion,
The priority areas reflect the main issues affecting • Improving health and sustainable funding,
the health and well-being of the region to date. The • Obtaining accurate information for evidence-
challenge to arrive at common public goods is further based decisions, and
exacerbated by inadequate health information and • Supporting accountability mechanisms.
health research, weak health information systems Regional Challenges and Priorities
(HIS) and lack of focal points to continually monitor
The establishment of the Caribbean Public Health
progress.
Agency (CARPHA) will provide an opportunity in
It was generally accepted that significant realizing the goals of the CCH111. This institution
improvements were realised during the execution will provide leadership in public health and support
of CCH I and II in the original priorities of CCH. evidence based decision making in the Caribbean
However, the real challenge remains two-fold: Region, guide the development of policy and monitor
1. The limited capacity of the region to finance and and evaluate interventions in priority areas. This
sustain sub-regional initiatives, and will involve rationalization of services provided by
2. The limited capacity of countries to translate the existing five Regional Health Institutions and
regional objectives into concrete policy formula- significant attention will need to be paid to ensuring
tion and sustainable programmes and infrastruc- a smooth transition in the establishment of this new
ture at the national level. Agency.18 Caribbean Cooperation in Health Phase III (CCH III)
Priority Areas
& strategic objectivesCaribbean Cooperation in Health Phase III (CCH III) 19
IV - Priority Areas And Strategic Objectives
Investing in Health for Sustainable matrices outlining the expected outcomes, lines of
Development in the Caribbean action and indicators of achievement can be found
The Caribbean Ministers of Health have recognized on various websites in the Region including www.
that the eight priority areas to be addressed in CCH caricom.org; www.carpha.org.
III are:
1. Communicable Disease Creation of a Healthy Caribbean
2. Non-Communicable Disease environment conducive to promoting the
3. Health Systems Strengthening health of its people and visitors
4. Environmental Health Expected Outcomes at National Level:
5. Food and Nutrition • Strengthened legal and
6. Mental Health regulatory framework for
7. Family and Child Health environmental health (EH)
8. Human Resource Develop- management
ment • Improved management
of water resources, in-
In order to achieve an impact cluding recreational wa-
on these priority areas, it ters, through a holistic
is necessary to address the and integrated approach
determinants of the diseases/ to ensure quality
conditions. The strategies/ • Implementation of the
actions which need to be integrated vector-borne
adopted must be: management strategy
• Cross cutting • Implementation of inte-
• Inter-programmatic grated waste manage-
• Trans-sectoral ment options
• People-focused • Full implementation of
• Holistic in their approach the International Health
• Increasingly focused on ad- Regulations (2005)
dressing the determinants of health • Availability of healthy
• Able to create an enabling environment for foods for consumption
change through trans-sectoral policy develop-
ment to make the healthy choices the easier Areas for Joint Collaborative Action:
choices • Development of Regional Environmental Health
framework that incorporates climate change ef-
In looking at the need to adopt a people-focused fects and projections using the risk management
approach in CCH III, a focus on the priorities as approach
defined, and sustainable strategies to be harmonized • Development and implementation of Regional
with the Nassau Declaration, “the Health of the Environmental Health Strategic Plan as ap-
Region is the Wealth of the Region”, the goals for propriate (EH professional network, climate
CCH III were defined along the theme: “Investing in change, tourism, guidelines for drinking and
Health for Sustainable Development”. The detailed recreational waters)20 Caribbean Cooperation in Health Phase III (CCH III)
• Development of model harmonized legislation • Improved capacity to monitor and manage condi-
for environmental health priorities, including tions which influence perinatal, fetal and neona-
port health tal mortality and diseases in the under-5 popula-
• Development of regional guidelines, strate- tion
gies and tools to promote environmental health • Improved capacity of the health and other sectors
awareness to respond to the specific health and develop-
• Development of guidelines and indicators in var- ment needs of adolescents and youth
ious settings which impact on the population’s • Strengthened and integrated programmes to
health, namely schools, workplaces, home and promote and protect the health and well-being of
recreation facilities the elderly
• Development of Core Indicators and Framework • Strengthened multi-sectoral approach and ca-
for Health Promoting Schools and support for pacity of countries to reduce the incidence of vio-
the development of Health Promoting Schools lence and unintentional injuries
in the Region through the strengthening of the
Caribbean Health Promoting School Network Areas for Joint Collaborative Action:
• Ensuring/establishing regional nutritional and • Development of models and pilot programs
quality criteria for imported and locally pro- which address Integration of Early Childhood
duced foods as part of trade policy which would Development programs into primary care
include standards for food labeling • Support for the implementation of the new WHO
• Development of intersectoral policies with agri- Child Growth Policy and Standards
culture, trade and marketing to develop a mecha- • Maintenance of high levels of immunization
nism to assure that healthy foods are available at rates for the vaccine preventable diseases and
affordable prices assessment of feasibility of introducing new vac-
• Support for capacity at the regional and nation- cines in the Region, with particular emphasis on
al level to implement the International Health HPV vaccine for the prevention of cervical can-
Regulations (2005) and to mount an effective cer
response to outbreak or disaster crisis at national • Development of Regional nutrition standards
and regional level. and guidelines for school meals and food sold in
• Support for enhanced capacity at national and school cafeterias; dietetic guidelines for institu-
regional level to establish an effective early warn- tions on NCDs
ing system for disasters and mount an effective • Development of a regional plan to adopt an inte-
and coordinated response. grated approach to the challenges of Adolescent
Health, which will include, amongst other issues,
Improved health and quality of life for mental health, unintentional injuries and vio-
Caribbean people throughout the life cycle lence, and sexual and reproductive health
• Development of a Regional plan on Injury and
Adding years to life and Life to Years
Violence Reduction
Expected Outcomes at National Level
• Development of models of care and sharing of
• Promotion of mental wellness of the population
best practices of integrative care for the elderly
and mechanisms to support appropriate care for
and the physically and mentally challenged
the mentally ill at the primary care level, with
• Implementation of the Caribbean Regional Stra-
early detection and appropriate care
tegic Framework for HIV/AIDS
• Programs for early childhood development inte-
grated into Primary Health CareCaribbean Cooperation in Health Phase III (CCH III) 21
• Support for implementation of the Port of Spain • Development of Regional Quality Management
Declaration on Stemming the Tide of Non-Com- and Accreditation Framework, including Patient
municable Diseases Charters
• Support for implementation of the Regional • Support for the implementation of the safe hospi-
Mental Health Policy tal assessments in all hospitals in the Region
• Support for the development of national centres
Health Services that respond effectively to of excellence in laboratory and public health
• Support for the implementation of the Caribbean
the needs of the Caribbean people
HIV/AIDS Plan for the Health Services
Expected Outcomes at the National Level:
• Universal access to health care services at pri-
mary care level Developing Human Resource capacity to
• Re-orientation of health care to Primary Health support health development in the Region
Care-based systems Our smaller member states are faced with problems of
• Access to safe, affordable and effective medicines retention of trained personnel, the quality, skills and
and their rational use improved competencies of the existing health workforce, as well
• Health sector organized and prepared to respond as limitations in capacity to train a health workforce
to disasters through safe hospitals and health to meet their needs. This includes the full extent of
care facilities the health workforce such as nurses, physician, public
• Health sector organized and prepared to respond health practitioners, researchers and health care
to mass casualty national/regional events/disas- managers. This is also mirrored at CARICOM level.
ters
• Strengthened capacity of Member States to per- Our vision aims to provide access to quality health
form essential public health functions services for all people of the CARICOM Region
through the strengthening of health human
Areas for Joint Collaborative Action resources. The strategic direction laid out in the
• Assessment of the feasibility of developing a CCH III aims to mobilise institutional actors at the
mechanism for Shared Services in tertiary care national, regional and global levels of the health and
in the Caribbean Region related sectors and other relevant civil society actors,
• Development/Review of protocols and standards to collectively strengthen the human resources in
of care for mental health, non-communicable dis- health through policies, interventions, and networks.
eases and other priority diseases identified in the
CCH III We have incorporated strategies to mitigate against
• Study to assess the feasibility of establishing a the effects of regional and international labour
Regional Health Insurance Scheme force challenges but to also embrace the potential
• Development of a comprehensive and integrated opportunities presented by the regional and global
chronic disease management models trends. Our response supports the Toronto Call to
• Support the design and implementation of a Action (2006) and is designed to specifically address
Caribbean Pharmaceutical Policy and mecha- the Millennium Development Goals in accordance
nisms to enhance access, quality and rational use with national health priorities.
of medicines in the Region;
• Support the strengthening and the harmoniza- Areas for Joint Collaborative Action:
tion of pharmaceutical regulation, including • Support for the development of a Regional Stra-
Pharmacovigilance; tegic plan for health human resources22 Caribbean Cooperation in Health Phase III (CCH III)
• Support for the development of infrastructure to including substance abuse prevention and care,
enable the free movement of skilled health per- into primary health care systems
sonnel in the CARICOM Region
• Development of a Regional Health Professional Evidence-based decision making as the
Registration Database mainstay of Policy Development in the
• Models and frameworks of trans-sectoral poli- Region
cies and protocols for health workforce planning Expected Outcomes at the National Level:
• Development of a mechanism for the coordina- • Improved surveillance systems in the priority ar-
tion of schools of public health in the Caribbean, eas of CCH III
to strengthen research and training in public • Evidence-informed policy formulation
health
• Enhanced coordination of schools of medicine, Areas for Joint Collaborative Action
nursing, and allied health professions in the Ca- • Support for the development of a minimum data
ribbean to strengthen the training of health pro- set for health information systems, to include in-
fessionals to meet the health and development dicators in the priority areas for CCH III namely,
needs of the CARICOM Region mental health, environmental health, communi-
• Development of mechanisms for coordination of cable and non-communicable diseases, food and
the health services and the Caribbean academic nutrition, human resource development, health
institutions to work cooperatively in human re- systems assessments and program evaluation
source planning and the development of human • Establishment/Review of guidelines for the sur-
resources management programs as part of the veillance of selected communicable diseases,
curricula vector-borne diseases, nutrition, and environ-
mental hazards including vector surveillance
• Identification of regionally accepted compe-
• Enhanced laboratory capacity at the Regional
tencies in the health workforce for primary and
level to support countries in surveillance of com-
secondary prevention, quality health and health
municable diseases, environmental health, wa-
care, with particular emphasis on the CCH III
ter- and food-borne diseases, and quality assess-
priority areas ments
• Development of initiatives and strategies to sup- • Establishment of baseline data for the CCH III
port the expansion of residency training pro- priorities and support for countries’ capacity to
grams that focus on primary care and chronic collate, analyze data and present in a meaningful
disease prevention and management way to various stakeholders
• Curriculum development at pre-service level, • Development and implementation of a Carib-
Continuing Professional Development (CPD) bean Health Information System supported by a
and integration of mental health management, regional health information networkCaribbean Cooperation in Health Phase III (CCH III) 23 management & coordinating mechanisms
24 Caribbean Cooperation in Health Phase III (CCH III)
V - Management And Coordinating Mechanisms
This new phase of the CCH III will require • Provide adequate data on monitoring indicators;
stronger leadership, more effective management • Ensure adequate participation of traditional
and coordination, and enhanced technical and and non-traditional sectors in the attainment of
administrative capacity at both regional and country health and development objectives; and
level, as well as effective resource mobilization. • Build capacity at national level to contribute to
Emphasis will be placed on achieving genuine national and regional progress.
involvement and participation by all actors in health
and related sectors as well as instituting greater Management Mechanism
accountability for the delivery of agreed upon The Council of Health and Social Development
common public goods and related interventions.
(COHSOD) responsible for Health
Coordination and monitoring of the implementation
The COHSOD is ultimately responsible for
of the CCH Phase III is structured along two levels:
guiding the implementation of the CCH III. The
- The Regional Level Functions
Annual Caucus of Ministers of Health will have the
- The National level Functions
responsibility to direct the CCH in between meetings
of the COHSOD. The CARICOM CAUCUS of
Regional Level Functions will
Health Ministers is a sub-committee of the Council
• Support individual countries in developing ca-
for Human and Social Development (COHSOD).
pacity to implement and monitor regional public
The Caribbean Cooperation in Health Secretariat
goods and fulfil global health and development
The Secretariat comprises the CARICOM Secretariat
commitments;
and the PAHO/WHO Office of the Caribbean
• Provide effective and efficient technical coopera-
Programme Coordination (OCPC). The Secretariat
tion through a greater streamlining of regional
will be strengthened to manage the administrative
agency responsibility;
and technical implementation of CCH.
• Establish multi-sector and multi-disciplinary
Priority Area and Program Goal monitoring
committees; The CCH Secretariat will hold formal meetings
• Provide timely reports on regional and national and will be responsible for the following:
progress towards accepted goals and indicators; • Definition of the technical and administrative
• Improve regional support machineries through support required for implementation and coordi-
effective technical support to countries; nation of project implementation;
• Reduce duplication and gaps in technical sup- • Development of an annual implementation plan;
port to countries; and • Formulation of annual reports;
• Facilitate a regional data base and knowledge ac- • Commissioning of the Monitoring and Evalua-
cess tools to ensure involvement by all participat- tion Framework;
ing agencies and countries. • Coordination of resource mobilisation; and
• Adopting and supporting a communications
National Level Functions: strategy.
The individual countries will, through national
mechanisms: The Steering Committee
• Ensure effective functioning of national mecha- The Steering Committee (SC) comprises the
nisms; Executive Committee of the Chief Medical OfficersCaribbean Cooperation in Health Phase III (CCH III) 25
(CMOs); Regional Focal Points for the Priority Areas in the Caribbean Region, guide the development of
drawn from the Regional Technical Programmes; policy and monitor and evaluate interventions in
Regional Tertiary Institutions; and the Caribbean priority areas.
Cooperation in Health Secretariat (which will be the
SC secretariat as well). Sustained commitment from all responsible
parties to ensure the following:
The Committee will meet twice per year and its • Ownership from the regional and national levels
functions are: and among non-traditional actors in health .
• Supporting and facilitating the implementation • Strong leadership at country level and at the level
at national level based on sound evidence; of the CARICOM Secretariat.
• Promoting and facilitating technical cooperation • More effective monitoring of regional and associ-
within and among countries, agencies, and insti- ated national programs.
tutions in both traditional and non-traditional • Adequate technical cooperation for implementa-
sectors; tion of health care programmes.
• Resource mobilisation; and • Capacity building at country level and among
• Monitoring and evaluation of progress of the technical staff for using the regional priorities
CCH III implementation. and objectives to guide national planning and to
produce reliable health data.
The Regional Focal Points • Support for the regional and national coordinat-
This technical structure will operate at two levels. ing mechanisms
Firstly, at the level of the individual agencies with 1. A proficient joint CCH Secretariat (PAHO/
specific responsibility, and secondly as an integrated WHO OCPC and CARICOM Secretariat) to
multi-disciplinary team. Overall responsibilities will coordinate, and work in close collaboration with
include: the Chief Medical Officers CMOs ( the CCH co-
• Monitoring the progress of priority health pro- ordinators).
grammes and reporting to the Steering Commit- 2. Greater attention to communication and access
tee, to knowledge sharing networks between and
• Promoting, facilitating and guiding countries within countries through the implementation of
in developing plans, policies, programmes, and a comprehensive communications strategy, up-
projects to achieve the regional goals set in the grading existing systems where necessary, to fa-
priority areas at the national level, and cilitate communication between the Secretariat
• Assisting in building capacity for the implemen- and countries.
tation of CCH III at the national level. • Establishment of regional data base for mon-
itoring of all indicators and ensuring that
Critical Success Factors reliable data are available for evidence-based
The Caribbean Public Health Agency (CARPHA) planning and decision making in health
planning and programme strengthening,
will rationalize the functions of the current
nationally and regionally.
Regional Health Institutions (RHIs) and have a more
comprehensive mandate in addressing the public Country level responsibilities:
health needs of the wider Caribbean Region and will • Formulation, needs identification, resource mo-
be a critical success factor in the implementation of the bilisation and information sharing
CCH III. CARPHA will provide leadership in public • Provision of guidance, direction and relevant in-
health and support evidence based decision making formation to the CCH Secretariat26 Caribbean Cooperation in Health Phase III (CCH III)
• Communication with key stakeholders, particu- accountability will be carefully defined. The
larly the public, about CCH benefits regional planning, monitoring and implementation
• Support for the CCH Coordinators( CMOs) in mechanism outlined above will serve as the main
implementing the Initiative programme accountability system.
• Full participation in all activities of CCH
• The CARICOM Secretariat
Programme and Financial Accountability • CCH Secretariat
Lines of reporting for technical and financial • Caribbean Public Health Agency (CARPHA)Caribbean Cooperation in Health Phase III (CCH III) 27 Annex 1 Background The Caribbean Community (CARICOM) was for the collective program. In this process the Pan established in 1973 by the signing of the Treaty of American Health Organization, the Regional Office of Chaguaramas in Trinidad and Tobago with the purpose the World Health Organization in the Americas (PAHO/ of enhancing economic and foreign policy coordination WHO), has been the major partner. PAHO/WHO has and promoting functional cooperation. CARICOM provided technical and financial resources through its Member States are Antigua & Barbuda, The Bahamas, country representations and to at least two of the five Barbados, Belize, Dominica, Grenada, Guyana, Haiti, Caribbean Regional Health Institutions (RHI), namely the Jamaica, Montserrat, Saint Kitts & Nevis, Saint Lucia, Saint Caribbean Epidemiological Centre (CAREC) and the Vincent & the Grenadines, Suriname, and Trinidad & Caribbean Food and Nutrition Institute (CFNI), which Tobago. Associated Membership is extended to Anguilla, are PAHO/WHO specialized centres. The other RHI Bermuda, British Virgin Islands, Cayman Islands, and Turks are the Caribbean Health Research Centre (CHRC), and Caicos Islands. the Caribbean Environmental Health Institute (CEHI), The Caribbean Cooperation in Health Initiative and the Caribbean Regional Drug Testing Laboratory (CCH) was developed in the framework of functional (CRDTL). cooperation. It was adopted by CARICOM Health CCH II, approved in 1999 for the period 1999- Ministers in 1984 to optimize the utilization of resources, 2003, sought to emphasize country ownership in the promote technical cooperation among countries, development of the processes and the implementation develop projects in priority health areas, and secure of programs. The CCH II established eight program funding for their implementation.The concept promoted priorities, namely Chronic Non-Communicable collective and collaborative action to solve critical health Diseases; Communicable Diseases including HIV/AIDS; problems best addressed through a regional approach Environmental Health; Family Health; Food and Nutrition; rather than by individual country action. Health Systems Development; Human Resource The initiative was approved by CARICOM Heads of Development; and Mental Health. The management and Government in 1986 and CCH Phase I was launched. monitoring of the program was the responsibility of the The CCH, although lauded by both Caribbean regional CCH Secretariat, comprising the Health Desk of the governments and international agencies as a positive CARICOM Secretariat and the PAHO/WHO Office of intervention, only partially realized the goal of securing Caribbean Program Coordination (OCPC), supported external funding to implement all the priority projects. by a Steering Committee with technical representatives However the concept of collective and collaborative from the Chief Medical Officers and the RHIs. action and the prioritization of health concerns During the period 1999-2005, the actual timeframe of was adopted by the countries as a framework for CCH II, only limited success was achieved in obtaining national interventions and the promotion of technical external funds for special regional projects. However, the cooperation. CARICOM Heads of Government recognised the CCH Over the years special efforts were made to promote mechanism as a contributor to enhancing development partnership with national, bilateral, multilateral, regional and formulated the Nassau Declaration 2001, which and international agencies to secure additional resources proclaimed that the “Health of the Region is the Wealth
28 Caribbean Cooperation in Health Phase III (CCH III)
of the Region”. This Declaration mandated that special Carr and Ward recommended that the successor to
attention be given to three of the eight priorities namely, CCH II, namely CCH III, should retain the same eight
Chronic Non-Communicable Diseases, Mental Health, priorities as in CCH II and add an additional goal to
and HIV/AIDS. Among these, HIV/AIDS obtained address the promotion of healthy lifestyles and behaviour
significant funding and an increase in programming change from at-risk behaviour.
and partnerships. As a result, CARICOM established a CARICOM Policy decisions and initiatives
separate Secretariat, the Pan Caribbean Partnership for
At the 2001 CARICOM Heads of Governments’
HIV/AIDS (PANCAP), for coordination and monitoring.
Conference, the Nassau Declaration recognised that
Resources for monitoring the CCH II process and the “Health of the Region is the Wealth of the Region”,
progress were also not readily available, as there was also recommended continued emphasis should be given
a reduction in “project resources” from the OCPC and to the implementation of the CCH Framework and
CARICOM for the management of the CCH Secretariat. mandated that increased attention should be given to
However the PAHO/WHO programming budget for the development and implementation of three priority
the Caribbean was used to support specific activities health areas namely HIV/AIDS, Mental Health and
relating to the priority areas as a component of its Chronic Non-Communicable Diseases. These items
ongoing work-plan. Some of these activities included the provide the stimulus to keep the strategic health agenda
hosting of several regional meetings to build consensus for functional cooperation in focus.
and accelerate program development, for example the Process of developing CCHIII
completion of a draft action plan for the management of
PAHO/WHO OCPC and the CARICOM Secretariat
Chronic Non-Communicable Diseases (CNCD) and the
convened a series of meetings with the relevant
preparation of a core curriculum for building capacity for
stakeholders and facilitators to review the CCH II
environmental health officers.
Evaluation Report and define the roles and functions of
Evaluation of CCH II and PAHO/WHO and the CARICOM RHI in the formulation
Recommendations and implementation of CCH III.
The CCH II evaluation report highlights that although Administrative structure for
some regional projects were developed by CARICOM, implementation of CCH III
PAHO/WHO OCPC, CAREC, CFNI, CEHI, and CHRC, The management structure for the CCH III should
insufficient additional resources were secured by the include a mechanism for working with CARPHA.
region to mobilize, promote, and coordinate technical However, the role of the CCH Secretariat as proposed
cooperation among countries. As a result, the CCH, in the Carr and Ward report will fulfil the responsibilities
although used conceptually in planning by most countries, for strategic direction and monitoring and evaluation of
took a lesser role in the context of national programming. the initiative.
Some of this posture was also due to limitations in the
national management and program structures.Caribbean Cooperation in Health Phase III (CCH III) 29
30 Caribbean Cooperation in Health Phase III (CCH III) Regional Health Framework 2010 - 2015 Caribbean Cooperation in Health Phase III (CCH III)
You can also read