Cambridgeshire and Peterborough ICS application - Sustainability & Transformation Partnership - NHS ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Cambridgeshire and Peterborough
Cambridgeshire &and
Sustainability Peterborough
Transformation Partnership
Sustainability & Transformation Partnership
Cambridgeshire and Peterborough ICS application
1
CONFIDENTIAL DRAFT FOR DISCUSSION
Cambridgeshire and Peterborough
Sustainability and Transformation Partnership
Contents
Cambridgeshire & Peterborough Integrated Care System
Who we are
Why become an ICS
What we have achieved
Where we are going
How will we get there
Appendices
1. System development journey
2. ICS Minimum Operating Requirements Summary
3. ICS Maturity Matrix Summary
4. System development plan
CONFIDENTIAL DRAFT FOR DISCUSSION
Cambridgeshire and Peterborough
Cambridgeshire &and
Sustainability Peterborough
Transformation Partnership
Sustainability & Transformation Partnership
Cambridgeshire and Peterborough ICS
3
CONFIDENTIAL DRAFT FOR DISCUSSION
Cambridgeshire and Peterborough
Sustainability and Transformation Partnership
Who we are: Our partnership is composed of NHS providers, our CCG, County and District
Councils, our Health and Wellbeing Board, Healthwatch, voluntary care, and other partners
The following partners work together to provide health and care services for our population:
Cambridgeshire and Peterborough
• Two upper tier local authorities: Cambridgeshire County Council, Peterborough City Council
Queen
• Five District Councils: Cambridge City, East Cambridgeshire, South Cambridgeshire, Fenland, North population: Elizabeth A&E ED
574,807 E
Huntingdonshire. D
• One Health and Wellbeing Board: Cambridgeshire and Peterborough Health and Wellbeing Board North Cambridge
MIU Minor Injuries Unit
• Three hospital providers: North West Anglia (NWAFT), Cambridge University Hospitals (CUH), and
Peterborough
Royal Papworth (RPH) City Hospital A&E ED Peterborough
MIU Minor Injuries Unit
• Two community providers: Cambridgeshire and Peterborough Foundation Trust (CPFT) and
Cambridgeshire Community Services (CCS) Doddington Minor
MIU Injuries Unit
• One mental health provider: Cambridgeshire and Peterborough Foundation Trust (CPFT)
Princess of Wales
MIU
• One ambulance trust: East of England Ambulance Service NHS Trust (EEAST) Minor Injuries Unit
• 87 GP practices, including 2 practices in North Hertfordshire and 2 in Northamptonshire
Hinchingbrooke
• One C&P wide Local Medical Committee, that represents, supports and advises GPs ED A&E
• One Clinical Commissioning Group (CCG): Cambridgeshire and Peterborough CCG
• Healthwatch Cambridgeshire and Peterborough providing an independent patient and service user St Neots Walk
Walk In In Centre
voice for health and social care
ED Addenbrookes A&E
• Other partners including parish councils as well as local voluntary, community and faith organisations
To facilitate integration of care and provision of services closer to home, we have established:
• 21 Primary Care Networks (PCNs), which will require additional support to progress neighbourhood Urgent Care – Type of unit
A&E
working. We expect all of our 21 neighbourhoods to develop into Integrated Neighbourhoods. Minor Injuries Unit
Walk In
North South population:
• 2 Alliances based on the footprints of our two acute providers in the north and south, co-chaired by South 422,900
Local Authorities
primary and secondary care. We will build upon their success to establish our two place-based ICPs.
4
CONFIDENTIAL DRAFT FOR DISCUSSION
Cambridgeshire and Peterborough
Sustainability and Transformation Partnership
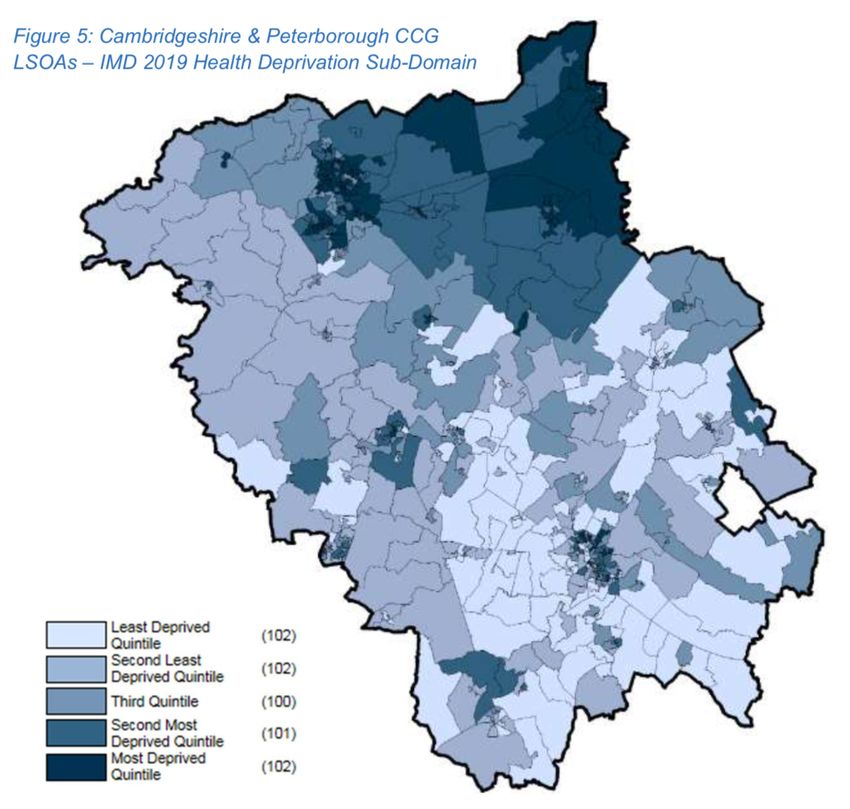
Who we are: Our system serves a diverse population that experiences significant health
inequalities
2019 IMD Health deprivation across Cambridgeshire
• The Cambridgeshire and Peterborough system is large, diverse and predominantly rural with two large cities
and Peterborough
(Cambridge and Peterborough) to the south and north-west. We serve a population of almost 1 million
• Overall, approximately 39,000 (9.8%) of our population have two or more long term conditions, and 15.5% of
the population have a long-term activity limiting illness. We also have over 2,000 people in touch with services for
severe mental illness, such as psychosis or bipolar disorder, and almost 4,000 people with learning disabilities
• Significant socio-economic and health inequalities exist between the North and the South within our system.
Fenland is in the worst 20% of all local authorities for most health deprivation and Peterborough is in the worst
30%, while South Cambridgeshire is in the top 10% for low health deprivation. This is evident in the chart of
health deprivation on the right.
• There are significant gaps in life expectancy across the patch. Life expectancy of a man living in the poorest part
of Peterborough is 75.8 years compared to 85.2 years for a man living in the richest part of Cambridge
• Risk factors such as obesity and adverse childhood experiences are more prevalent in Peterborough and
Fenland. For example, more children and adults are obese in the most deprived areas of Cambridgeshire and
Peterborough, with 14% more children in Year 6 overweight or obese in Peterborough, compared to South
Cambridgeshire. Peterborough ranks 13th out of 14 similar local authorities for ‘best start in life’ outcomes.
• Peterborough and Fenland are more ethnically diverse than Cambridge, with longstanding residents from
many different countries of origin including a Pakistani community of over 12,000 in Peterborough. In rural areas
there are longstanding Gypsy and Traveller populations as well as an migrant workers from Eastern Europe,
most markedly in Fenland (113% increase in 10 years)
• Thriving industry means that our population is expected to increase by 80,000 in the next 15 years, putting
pressure on housing availability, transport links and a range of public services. Our increasing population is one
factor that has led to housing and homelessness issues, with a lower level of access to health services for
vulnerable populations such as rough sleepers in Peterborough and Wisbech compared with Cambridge
5
CONFIDENTIAL DRAFT FOR DISCUSSIONCambridgeshire and Peterborough
Sustainability and Transformation Partnership
Why become an ICS: The challenges facing the health and wellbeing of our population
requires an integrated care system approach to improve and sustain best outcomes
We have communities which experience unacceptably poorer access, outcomes and life expectancy than the rest of our population. To solve wider issues
impacting people’s mental and physical health, we need a holistic snapshot of a person’s needs, behaviours and environment. All of our public sector needs to be involved
to address challenges in quality of services and equity of outcomes: the public, schools and early year settings, fire services, councils, voluntary, community and faith
sectors, housing associations, social services and the police. Collaboration between health, local government, and communities enables us to align our collective
resources to make significant impacts on preventing ill health and reducing inequalities, joining up delivery, and improving people’s independence,
experience and quality of life. We will work as a system to solve common challenges while applying local approaches. We are already working in partnership and have
developed a draft Clinical Strategy for the future ICS and a joint Health and Wellbeing Strategy across Cambridgeshire and Peterborough for 2020-24, focused on the
wider determinants of physical and mental health.
Which factors impact our health?
Social and
Our Our
Healthcare economic Genetics
environment behaviours
circumstances
Peterborough has a 25% greater adult
Particulate matter Avoidable admissions 10yr life expectancy higher number of BAME obesity rate in Fenland
index in central are almost twice as difference between women who may vs Cambridge.
Wisbech (Fenland) high in the most men in the poorest struggle to use breast Smoking is also 9%
exceeds EU limits for deprived areas, with areas of Peterborough cancer services, such as more prevalent in
15-30 days a year, an additional 1700 and the richest areas genetic screening, due Fenland than
placing children at risk admissions per capita of Cambridge to language barriers. Cambridge.
6
CONFIDENTIAL DRAFT FOR DISCUSSIONCambridgeshire and Peterborough
Sustainability and Transformation Partnership
Why become an ICS: Becoming an ICS will benefit our population, our staff, and our
financial position
For the population:
• Integration across the system will create a seamless patient journey and improve patient experience
• Greater working between the NHS, local authorities, and voluntary sector leaders will enable more opportunities to make shared decisions about how to best use
resources collectively to improve the wider determinants of health in C&P and improve outcomes for disadvantaged groups
• Our partners will better be able to work together to redesign care around the needs of communities to improve mental health, building on our previous
collaborations as an early implementor of community mental health services in Peterborough for example
• We will be better able to work together from beginning to end of patient pathways and standardise approaches to safeguarding, complaints, and infection
prevention to ensure patients receive high quality services regardless of where they are treated
• Our work towards a shared patient record means our patients will no longer need to repeat their story to different teams and will improve the quality of their care,
because their full needs will be better understood
• As ill health has significant impacts on economic productivity, improvements in health outcomes will translate to greater contributions to the local economy
For the staff: For the public purse:
• ICS designation would facilitate the sharing of staff • Closer collaboration across the health and care
and best practice across wider networks, reducing system can improve the use of resources through
strain in high-demand places across Cambridgeshire reductions in length of stay and unnecessary
and Peterborough and encouraging innovation attendances
• Cambridge & Peterborough’s system-wide people plan • Opportunities to work together on enablers, such as
emphasises our desire to create a safe environment development of digital infrastructure, at a system-level
for all NHS staff. Our ability to work at various levels, can reduce duplication and enable more efficient use
including across the system, will enable us to ensure a of resources
great work environment • The ICS strategic commissioner will enable collective
• PCN feedback will provide a mechanism for direct management of system finances and performance,
staff representation and allow leaders to which will allow organisations to better work together
continuously assess the efficacy of the People Plan. to address historical financial challenges
7
CONFIDENTIAL DRAFT FOR DISCUSSIONCambridgeshire and Peterborough
Sustainability and Transformation Partnership
Why become an ICS: ICS designation is the next step on our development journey to improve
outcomes and deliver integrated care for the Cambridgeshire and Peterborough population
Being designated as an ICS will be the start of a new chapter in our system’s journey. We have already made progress and in the areas where, a year ago, we
were still ‘developing’, we are now beginning to ‘mature’. We have worked together to develop robust plans to meet all of the operating requirements. Our goal,
for 2021/22 and beyond, is to ‘thrive’ as a health and care system.
Over the past 5 years we have made significant changes to the way that we work together, as partner organisations, to integrate our health and care
services and improve the health outcomes of our population.
• We have spent time with the people in our communities learning more about what matters to them and through this approach broadened our understanding of our
population. We have started to bring together health and care to meet the needs of our citizens closer to home. E.g. “The Big Conversation”
• We have integrated many of our services to improve patient experience, reduce delays in handover, and to ensure patients do not fall through cracks. We have
created new partnerships and progressed plans for wider public service reform. E.g Children’s Board, MH and LD system wide governance
• We have spent time and effort understanding our financial position and developing plans to reduce our historic deficit. E.g. The Drivers of Deficit, McKinsey
• Our Public Service Board has begun to reform our public services, bringing together general practice, community, third sector and wider public services through a
Think Communities approach which empowers local citizens to shape services.
• Our acute services in the North and South have worked closely together to reduce health inequalities across the patch, including staff working across
organisations (e.g. joint CUH-NWAFT posts for radiology and neurophysiology, RPH respiratory consultants embedded in NWAFT), mutual aid (e.g. pathology), and
new ways of delivering care (e.g. Hub for vascular services, Rapid NSTEMI pathway)
• For mental health, we are a national pilot site for transformation of community mental health services, which brings together primary care, mental health
specialist provision, voluntary sector and social care, linking with the Think Communities programme.
Our first Sustainability and Transformation Plan (STP) (2016) set out changes we wanted to make to health services in Cambridgeshire and Peterborough. It
described our core clinical framework: health and care services provided closer to people’s homes and excellence in hospital and specialist services. The plan also set
out how we would change the way we worked together as partner organisations across the system to implement this strategy.
Our Long Term Plan (LTP) (2019) built on the progress made and described our ambition to do more to bring together health care across our system, in our places and
through our neighbourhoods as we develop to become an Integrated Care System (ICS).
8
CONFIDENTIAL DRAFT FOR DISCUSSIONCambridgeshire and Peterborough
Sustainability and Transformation Partnership
Why become an ICS: Our system agreed a vision of joined-up, proactive care closer to home
Our vision for our system is to provide joined-up, proactive care in the most appropriate setting, so that we improve health outcomes and wellbeing equitably for
the people of Cambridgeshire & Peterborough. We will provide safe, personalised health and care services closer to people’s homes with more support for
people to stay healthy, to keep their independence and to make decisions about their own health and care. We will strive to ensure all residents receive the right
care at the right time, experiencing a seamless patient journey through the health and care system.
LTP Priorities Our System Partnership Board has agreed the vision and priorities for our system to deliver improvements in
care and deliver our financial package while ensuring patient safety. Our conversations with local people tell us we
1) Outpatient transformation
could do more to support them to remain independent by delivering evidenced-based, personalised care
2) Health inequalities/prevention informed by joint health needs analysis (JSNA) closer to home, which the evidence suggests is also better for
3) Integrated out of hospital care patient outcomes. Subsidiarity has become the heart of our consistent operating model.
4) Redesigning care pathways We want to focus on prevention at every opportunity: working with children, families and communities and
supporting healthy lifestyles; working with local government on improving housing, employment opportunities and
5) Urgent and emergency care
other determinants of health; and working with staff to understand how every contact can be used to promote good
6) Research and innovation health and wellbeing.
We are revising our 2019 LTP in Q4
20/21 to reflect emerging priorities We will actively address health inequalities by concentrating our resources and initiatives in those areas that have
around Children and Young People, the poorest outcomes, focusing on both physical and mental health. We have set out a comprehensive programme
Mental Health and Learning Disabilities, of expansion and transformation for mental health, to ensure that we reduce the inequality in life expectancy for
and Covid-19 recovery people with serious mental illness across our system, focussing first on areas with the greatest needs.
As well as trying to avoid the need for some emergency hospital care, we think more planned care can take place
out of hospital. Specialist advice and support need to be available much more readily within local communities so
that outpatient appointments are not always required. When people do need to access hospital services, we want
them to receive consistently outstanding clinical care. Our ICS will continue to build on our work today to support
integration in patient pathways across health and care and leverage collective assets.
9
CONFIDENTIAL DRAFT FOR DISCUSSIONCambridgeshire and Peterborough
Sustainability and Transformation Partnership
What have we achieved: We have made significant progress Achieved ICS consistent operating arrangement G
Plan delivering significant milestones GA
towards achieving the consistent operating arrangements
KEY
Plan agreed and on track A
Plan to be developed in next quarter AR
Discussion ongoing R
Our record of delivering successful transformation at system, place, and neighbourhood levels makes us confident in our capabilities for the
System
future. Our C&P CCG has performance and transformation capabilities at the system-level, and our individual providers have capabilities at
capabilities
place and neighbourhood, which will strengthen. Assurance will continue to be managed at the system-level.
We have agreed our CCG will become an ICS strategic commissioner. We will establish 2 ICPs as well as MH & LD and CYP system-level
Streamlined
collaboratives responsible for commissioning services. We are developing transition plans, which we will finalise and begin to implement in
commissioning
Q1 21/22. We will continue to joint commission with LAs where beneficial. We are working closely with region and using available support.
We have developed a 4-phased plan to develop and implement a shared health and care record that protects patient data. We are on track
Shared care to deliver phase 1 of our plan, to develop and roll out technical capacity, in September 2021. We are still in the process of identifying
record
funding for phases 2-4 on pathway redesign, PHM, and patient portal.
We have established a Systems Partnership Board, chaired by Mike More, and a Systems Leaders Group, co-chaired by Jan Thomas and
Leadership Roland Sinker. We have agreed a distributed leadership model to best utilise clinical leaders and non-executive directors. We are in the
process of appointing 2 VSMs to lead our ICPs at place, and we have clinical directors to lead our all of our PCNs and INs.
We have established a transitional governance structure, and we are preparing end-state governance structures considerate of both
Governance potential legislative options. We are finalising the roles and responsibilities of individual partners and groups. As part of our work to
establish ICPs, we will need to agree a governance structure, which we will do by Q1 21/22.
We are working on refreshing our LTP in light of the pandemic and develop operational plans and a financial framework, which we will
submit to the region by Q1 21/22. We have agreed to share financial risk as a system and agreed how we want to work as a through
System plans
several system-wide strategies such as our people plan and digital strategy. We have developed a timetable to finalise our revised financial
plan and an 18-month roadmap for system development. We will continue to work closely with region and access available support.
We have agreed enablers will be managed at the system level, including capital and estates. We have already established an estates
System capital workstream, and we will finalise our estate strategy and capital plans by March 2021. We are working to consider the value of our assets to
and estates plans
the system and how to use them more efficiently.
10
CONFIDENTIAL DRAFT FOR DISCUSSIONCambridgeshire and Peterborough
Sustainability and Transformation Partnership
What have we achieved: Our partnership has successfully delivered programmes to progress
our priorities (1/2)
• We rapidly shifted from F2F to virtual outpatients appointments during the pandemic, while ensuring our patients with the most need were not left behind
– 45.1% of all consultant-led outpatient appointments were delivered virtually in Oct 2020. This ensured we were able to reduce the risk of Covid-19
infections for our staff and patients while still delivering high quality care during the pandemic, both virtually and F2F where needed.
• We are transforming our models of care to deliver more services in primary and community care
– Diagnostic services such as ultrasound and MRI have already moved into the community. We have implemented a community-based CT service in
Outpatient collaboration with PCNs, which sees 40-50 patients per day, reducing pressure on acutes and allowing patients to receive care closer to home
transformation – Across C&P, we have established drive-through phlebotomy, which sees 200+ patients per day, and out-of-hours phlebotomy as well as drive-
through spirometry. This has enabled patients to receive diagnostic tests safely while releasing in-person capacity for people with reduced means
– NWAFT is working with primary care to enable GPs to deliver cardiology services as part of local community cardiology clinics. This will allow residents
to access care closer to home, better integrate primary and secondary care, and improve CVD outcomes, which are associated with health inequalities
• We are working through the national NHSEI OP Adopt & Adapt framework to both support local and accelerate recovery within C&P. Examples of this
include scaling-up and ensuring initiatives such as virtual consultation and Patient Initiated Follow Up (PIFU) become business as usual
• We have established a system-wide Health Inequalities Board, to oversee delivery of our Health Inequalities Strategy. Our Strategy details priority action
areas that include increasing the use of the Health Inequality Impact Assessment, addressing inequalities in workforce distribution, needs-based commissioning,
and targeted action on hypertension and diabetes
• We have identified “Early Adopter PCNs” with clinical leaders and introduced Eclipse data to identify the key health care inequalities, with the ambition to reduce
Health inequalities the hypertension control inequality gaps by 50% to reduce the number of heart attacks and strokes in deprived areas.
/ prevention • We have allocated primary care diabetes spend based on diabetes prevalence and deprivation, to ensure populations with the most need receive sufficient
funding and we can reduce health inequalities in diabetes care
• We are working on increasing cancer screening in hard-to-reach populations to reduce inequalities. For example, our PCNs, Peterborough City Council, and
CPSL Mind have developed an integrated sexual, mental and general health service for sex workers in Peterborough, who experience barriers to accessing
healthcare, through the ‘Wildflowers’ project which has led to a 30% increase in cervical cancer screening.
• We have established 21 PCNs and 7 Integrated Neighbourhoods to facilitate integrated care and better address local needs
• We are developing two complementary integrated community health and care hubs, the South Alliance at the Princess of Wales site and the North
Integrating out of Alliance at Doddington. These hubs will deliver local health services that help care for people at home and keep them out of acute hospitals.
hospital care • Peterborough and Cambridgeshire LA have invested in developing “Think Communities” approach, which aims to unite key public sector organisations
behind a common set of goals and priorities which support the development of communities, deliver better outcomes through earlier intervention at community
level, and reduce demand on statutory services.
11
CONFIDENTIAL DRAFT FOR DISCUSSIONCambridgeshire and Peterborough
Sustainability and Transformation Partnership
What have we achieved: Our partnership has successfully delivered programmes to progress
our priorities (2/2)
• We have implemented new ways of working and new care models including:
– Rapid high-risk NSTEMI pathway to transfer patients directly to RPH within 24 hours to improve services for heart attack patients in the region
– Mental health joint response car pilot as a collaboration between EEAST and CPFT to ensure people receive the right assessments at home
– Roll-out of digital health, such as digital appointments in primary, community, and mental health care as well as 5 pilot sites for digital diabetes,
improving residents’ access to care while making pathways more efficient
Redesign care – 10 Clinical Assessment Services, with another 8 being mobilised, to enable greater clinical expertise in patient assessment
pathways – Increasing the use and quality of Advice & Guidance to better support GP’s to provide high quality care close to home and reduce the need for hospital
referrals. C&P are nationally the highest users of the A&G service and used as an exemplar by NHSEI on how we collate and share our data.
• The ‘Getting It Right First Time’ (GIRFT) programme has produced recommendations on areas where quality of care can be improved through reduction in
variation in service delivery. Examples of this include developing more joint posts between RPH and NWAFT based on the Cardiology GIRFT review and
supporting NWAFT to develop imagining functions, which will ensure patients in the North receive as high quality care as patients in the South.
• In the North, we are piloting Admission Avoidance by increasing primary care monitored telemetry and diverting patients from A&E to respiratory
community teams has increased COPD patients access to specialist community teams, providing care in the most appropriate setting
• We have made significant progress towards integrated UEC. This includes:
– EEAST ambulance handover improvement work with NWAFT including introduction of Rapid Assessment & Treatment
– Completed public consultation for Peterborough UTC move to PCH site, work in progress on integrated front door service to go live Apr 2021
– Implementation of D2A including introduction of whole system Single Point of Access for discharge management
Urgent and
emergency care • Our UEC collaborative, composed of the CCG, EEAST, NWAFT, CUHFT and others, have implemented several programmes to reduce A&E attendances
and emergency admissions which has set a national precedent
– ED front door pilots that diverted patients to 111, primary care pathways or self-care advice
– “111 First” went live in Dec 2020 to manage increased calls to 111, reduce unheralded ED attends, and facilitate direct booking from 111
– Strengthened MDT support to care homes to reduce avoidable unplanned admissions with support of PCN clinical leadership
• We have ensured our population has access to Covid-19 vaccine trials and anti-body testing. We rapidly established a Covid-19 Testing Centre in April
2020. The facility has processed 2 million tests, ensuring residents in the region are able to receive accurate and timely testing.
• The Cambridge Clinical Research Centre has carried out over 1,000 clinical studies supporting more than 100,000 patients, ensuring early access for our
Research &
population to ground-breaking clinical trials and the forefront of medical innovation. For example, the University of Cambridge is collaborating with the system-
Innovation wide diabetes programme to start a large trial for digital weight loss apps for use with diabetes.
• We have rapidly implemented innovative treatments in primary care. The Cytosponge test, developed by Cambridge researchers, has enabled GPs to detect
Barret’s oesophagus in their surgeries, saving patients from unnecessary endoscopies in the hospital while still enabling early detection during the pandemic.
12
CONFIDENTIAL DRAFT FOR DISCUSSIONCambridgeshire and Peterborough
Sustainability and Transformation Partnership
What we have achieved: We have responded collectively to emerging priorities
• Our partners have worked closely throughout the Covid-19 pandemic to share staff, reduce pressure on acutes, rapidly implement transformation, and
continue delivery of high quality care
• EEAST has worked with NWAFT to maintain elective services by bringing suspected Covid patients to PCH and non-Covid patients to HH. EEAST
has also worked with CUH to set up a separate ED for suspected Covid patients, enabling normal A&E services to continue safely
Covid-19 • Our CCG has acted as system coordinator and facilitated information sharing across the health and care system as well as with other public sector
partners to collectively problem solve and manage capacity and demand, so our residents can receive the care they need
• Our System Partnership Board agreed a Phase 3 Recovery Plan in September 2020, using input from our managerial and clinical leadership. We are making
significant progress to recover elective admissions as we delivered 81% of the activity from Dec 2019.
• Our partners’ Chief Nurses and Medical Directors have established a Harm Reduction Cell to manage the clinical risks of backlogs and ensure patient safety
• We have updated our local People Plan to focus on upskilling staff and our staff health and wellbeing through the Covid-19 pandemic. The Covid-19
pandemic has highlighted the importance of staff support and our strategy reflects this. We offer a comprehensive suite of sickness support ranging from
internal line management support to independent employee assistance programs.
Workforce
• System-wide networks such as the Staff Mental Health Service allow for partner Trusts to access medical assistance
• We are working to address staff shortages, reduce workforce inequalities, and improve workforce sustainability. We are reviewing our system to identify entry
routes for unskilled workers as well as maintaining existing routes, like the Nursing Apprenticeship Degree scheme
• Our integrated mental health and community trust utilises best practice and innovation. CPFT is the third largest MH research organisation in the UK, with
significant international impact.
• As a system, we pilot MH crisis services models, ensuring our patients receive cutting edge care in mental health, including a “111” MH Crisis Service and
Mental health & Suicide Prevention Support Groups. We lead the way in MH and have shaped the national service models.
Learning
• CPFT hosts one of 12 national early implementer pilots for community mental health and for eating disorders.
Disabilities
• Children’s mental health and learning disabilities are a key focus of our children’s recovery plan
• We offer high quality Early Intervention in Psychosis services and exceed national referral to treatment targets, evidenced by results of 2019-20 national audit
by Royal College of Psychiatrists. In 18/19, 92% of people experiencing their first episode of psychosis were treated within two weeks.
• We developed a Best Start in Life Strategy which aims to improve life chances of children (pre-birth to 5 years) in C&P by addressing inequalities, narrowing
the gap in attainment and improving outcomes for all children, including disadvantaged children and families
Children’s and
• The development of the Cambridge Children's Hospital, which integrates children’s physical and mental health care, is an opportunity to provide leadership
Young People’s
and focus on specialised pathways to support the whole of the East of England region
Services
• Our specialist services, such as the only PICU unit in East of England and one of three regional Level 3 neonatal intensive care units at The Rosie
Hospital, are also working to reduce health inequalities across the region, given the correlation between babies requiring intensive care and deprivation
13
CONFIDENTIAL DRAFT FOR DISCUSSIONCambridgeshire and Peterborough
Sustainability and Transformation Partnership
What have we achieved: To improve our population’s health outcomes, our partnership is
working together to enhance our existing population health management approach
What is in place for population health management? What have we achieved?
• Analytics Community is in place across STP and was meeting regularly • Successfully applied to be part of the PHM Wave 3 Development program
prior to the Covid-19 pandemic, with plans to restart meetings in 2021 with
• Identified 5 conditions that contribute the most to excess deaths due to
ICP representation
socio-economic inequalities in our Health Inequalities Strategy, so we can
• PHM Strategy developed prior to pandemic, awaiting final sign-off due to focus our efforts on where we can make the most difference on inequalities
operational pressures. Discussed and shared with ICPs and PCN Clinical
• Started pilot of pro-active population health management for Long Term
Directors. Restarted Analytics Community will review.
Conditions using Eclipse Vista in our PCNs in the North
• Eclipse Vista and Eclipse Diabetes modules rolled out across the
• Roll-out of Eclipse and Diabetes Local Enhanced Service to improve diabetes
system. This enables the CCG to identify in real-time where practices need
additional support to care for patients care and screening. We have c.46,000 people living with diabetes on Eclipse.
GPs are using Eclipse to quickly identify patients that are out of range for the
• Integrated Performance Report now includes Sentinel Indicators to ensure 3TTs or not received all 8CPs, improving outcomes and reducing care variation
Health Inequalities is discussed at the highest levels
• In Jan 2020, the CCG was rated as the second worst CCG in the country for
• CCG team generate intelligence reports through performing bespoke delivery of the 3 treatment targets. In Oct 2020, the CCG is rated as 35/67 using
analyses on areas of interest Eclipse system data and above the national average performance.
• Daily Covid Surveillance that brings together NHS and Local Authority • We have allocated primary care diabetes spend based on diabetes prevalence
data to understand how the pandemic is spreading and impacting services and deprivation as part of our efforts to reduce health inequalities
• Programmes centred on hard to reach, hard to treat populations, such as • Pilot launched in Jan 2021 for 8 Specialist Healthcare Assistant roles to
a pilot for dedicated staff to perform physical health checks for people with deliver annual health checks and medical monitoring of Eating Disorder patients,
severe mental illness and collaboration with third sector organisations to a hard to engage population that experiences poorer outcomes
provide information about the Covid-19 vaccine to migrant workers
• We are an early implementor of community mental health in Peterborough, in
• Public health programme theory approach to community mental health which PCNs, secondary care mental health, third sector and community partners
transformation with evaluation independently undertaken by the NIHR use a public health programme theory approach to redesign care with the needs
Applied Research Collaborative for national learning and adoption. of the people and their community at the centre of improving mental health
14
CONFIDENTIAL DRAFT FOR DISCUSSIONCambridgeshire and Peterborough
Sustainability and Transformation Partnership
Where are we going: Our system is well placed to leverage unique assets to benefit the
local population across the whole ICS and wider afield
As an ICS, we would seek to better utilise our unique assets, such as our innovative GPs and NHS trusts. For example, one of International
our PCNs was shortlisted for a HSJ award in 2020 for its Health, Wellbeing and Community Champions programme to support
National
minority ethnic groups. CPFT is a leader in mental health and is renowned for its innovation and application of research,
shaping national service models. CCS provides high quality sexual health, HIV services, and children’s services across the Regional
region. Our large DGH NWAFT, composed of Hinchingbrooke Hospital and the Peterborough City Hospital, serves a diverse
multi-ethic population that experiences significant health inequalities. We will use the opportunity of a potential rebuild of
Hinchingbrooke to maximise capacity and access to services for our growing population.
Cambridgeshire &
Peterborough population
Unlike the majority of systems, Cambridgeshire and Peterborough also has a major role in the development and delivery of
services to regional and national populations, representing 37% of the total East of England Specialist Commissioner spend.
Our Cambridge Biomedical Campus is home to two leading specialist hospital providers. Our specialised services are
LAs GPs
wide-ranging, from renal dialysis to highly specialised Pulmonary Thromboendarterectomy (PTE) surgery, from our major
trauma centre to neurosurgery. CUH is the regional centre for specialist services for 5 million people in the East of England
and a regional centre of excellence for organ transplantation, neurosciences, paediatrics, genetics, and maternity care. CUH NWAFT CUH RPH
also leads the regional specialist MDT meetings and supports the development of other specialist providers in the region, such
as supporting neurology at Norwich and Norfolk. Treating 100,000 patients each year, RPH is the UK’s leading heart and
CCS CPFT
lung hospital and the only national centre for a range of specialist cardiothoracic services. Our developing children’s hospital
will integrate physical and mental health, building on the CYP services offered by CUH, CPFT, and CCS, and will expand our
regional and national offering, along with our specialist cancer hospital.
Our ICS will create an integrated health and care system that optimises the benefits of having world-leading research centres through seamlessly integrated datasets, community
approach to specialty services, and delivering improvements in health outcomes. For example, we are utilising our unique relationship with AstraZeneca, to develop a partnership on
remote monitoring for heart and lung conditions across the system. We have ongoing partnerships to ensure the benefits of our research reach deprived areas and benefit the whole of
our local population, and we are in the process of applying for a £500k grant from the Health Foundation to support an Innovation Hub to enable the spread of innovation from the
South to the North. As an ICS, we will build on our previous work together and better facilitate the sharing of knowledge, best practice, and staff. Our unique assets contribute to the local
economy as well – NWAFT has a well-established relationship with the University of Peterborough to train nurses, as will our specialist cancer hospital. Attracting unique talent to
Cambridge provides opportunity to create roles that have benefit for populations across the ICS as a whole, through training, outreach and joint roles, for example.
At the same time, we will continue to collaborate with other providers in the region, supported by the development of specialist hospitals for children’s and cancer. Our providers are
significant regional and national providers and are lead providers for many clinical networks that reach out beyond the ICS. Evident during the Covid-19 pandemic, our 3 on-call
respiratory rotas, 134 critical care beds, and clinical leadership support the region and maintain critical care for our population and neighbouring systems.
15
CONFIDENTIAL DRAFT FOR DISCUSSIONCambridgeshire and Peterborough
Sustainability and Transformation Partnership
Where are we going: We have developed a consistent operating model to provide high
quality integrated services, delivered as closely to residents as possible
We recognise one of critical success factors to continue to provide safe, joined-up care and improve population outcomes is a consistent operating model. We
have already established architecture at system, place, and neighbourhood, built on the principle of subsidiarity.
Integrated Care Systems
• The ICS will take a bird’s eye view of challenges and health and social care needs across C&P. It will
determine distribution of financial and other resources to meet those needs. Only things that
can’t be done at IN
• The C&P CCG will transition to deliver an ICS strategic commissioning function, with devolution of or ICP level are
relevant functions to the ICPs and other provider collaboratives. The ICS SC will commission some done at ICS level
specialised services and agree outcomes for each ICP.
Integrated Care Partnerships Only things that
can’t be done at IN
• ICPs are partnerships at the place-level, serving populations of approximately 500,000 people, that
level are done at
works to address wider determinants of health to improve health outcomes. ICP level
• Two Integrated Care partnerships will be developed in C&P, building on the work of the North and
South Alliances. Additional provider collaboratives for CYP and MH will also be developed.
Anything that can be
Integrated Neighbourhoods devolved to IN level
should be
• With GPs at the core, INs serve populations of 30,000 – 50,000. They will be enabled by new
contracts, which support delivery of primary care at neighbourhood level.
• The 21 PCNs in C&P will mature to be INs, building partnerships to integrate all health and care Start closest to
services within their communities. individuals
16
CONFIDENTIAL DRAFT FOR DISCUSSIONCambridgeshire and Peterborough
Sustainability and Transformation Partnership
Where are we going: Our success is enabled through our work to establish our future
consistent operating model for system, place, and neighbourhood levels
ICS responsibilities
• Set overarching strategy and strategic priorities, as well as develop clinical strategy and care model core requirements, as needed
• Manage outcomes framework and provide population health management capability for all population levels
• Act as health commissioner with bilateral contracts with ICPs and providers, ensuring consistency of quality, clinical standards, core pathways and outcomes
• Establish consistent clinical standards, guidelines and thresholds (e.g. diabetes pathway) health and care
ICP responsibilities
• Plan, transform, and secure the delivery of care for populations of approximately 500,000. They will have responsibility for leading and developing INs
• Establish and utilise local delivery structures to implement transformation in line with ICS priorities
• Coordinate INs and provider support, acting as an operational liaison
IN responsibilities
• Provide integrated care in local teams for populations based on GP lists • Locally implement and deliver system and place strategies
• Build community capacity through relationships across public services • Proactively manage care, including providing diagnostics
Our consistent operating model is based around subsidiarity, with responsibilities and finances held as closely to the patient as is safely possible. It
supports delivery of high quality, integrated care closer to home, wrapping resources around people and neighbourhoods.
17
CONFIDENTIAL DRAFT FOR DISCUSSIONCambridgeshire and Peterborough
Sustainability and Transformation Partnership
Where are we going: Our consistent operating model includes the transition of our CCG
to ICS strategic commissioner, which will commission better outcomes for our population
• The CCG will be starting the transition in February 2021 to move from being a CCG to the ICS Strategic Commissioner and support the system’s integration. We will be
moving away from a traditional, transactional model of health commissioning to a more strategic, ‘thinner’ role at system level, focusing on how we can best support and enable the
short and long-term changes that we need to make as a system. Operational health commissioning will happen through ICPs and other provider collaboratives.
• We will describe the process for this transition in our emerging development plan, which we will submit to NHSEI in March 2021. Over the next 18 months, we will maintain a
partially integrated commissioner function through the CCG fully responsible for developing the health commissioning strategy for the system, but playing a hands-on role
orchestrating and supporting the ICS and ICP creation and delivery. During this transition period, the CCG Governing Body will continue its statutory duties for delivering the
commissioning strategy.
• The ICS strategic commissioner will be responsible for assessing health needs in collaboration with the C&P Health and Wellbeing Board and agreeing outcome-based contracts
with ICPs based on needs system strategies, agreed by the Partnership Board. The ICS SC will support patient choice and will ensure that, whenever possible, assurance is done
once and as a system to avoid duplication, and be responsible for managing system performance management.
• Following the principle of subsidiarity, future ICPs at place will become responsible for the full budget of all cohorts / priorities in their localities and delivering the outcome-based
contracts they agree with ICS SC, including procuring and designing services, planning capacity and managing demand, and managing service performance. ICPs will become
responsible for all urgent care, planned care, primary care, and CHC. System resources in terms of budgets and clinical and managerial staff will follow these functions into our
ICPs. We have identified a need for support from NHSEI for greater clarity around future contracting arrangements (noted on pg 31).
• The ICS through the strategic commissioner is working with the regional team to take responsibility for the current commissioning areas held by NHSEI, such as forensics,
specialised (e.g. eating disorder services, CYP inpatient services), and other areas of primary care (e.g. dentistry, optometry, and pharmacy). This assumes that locally we can
secure the appropriate funding level for the services required and supporting resources to manage the expanded portfolio. Each of these service areas will be evaluated and as
long as sufficient resources are allocated and delegation is clear, this could transition over time. Our system will continue to work with NHSEI to consider how our financial
framework can appropriately compensate our specialist providers for specialist activity.
• The CCG has a statutory duty for financial targets and the LTP, and the system has committed to a financial profile agreed by the CCG Governing Body. Until future legislation
clarifies the future roles of the ICS and CCG, strategic finance decisions will be made through FPPG and the final plans will need approval of the CCG GB and partners’ boards
• The strategic commissioner will retain the accountability for agreed areas where due to scale, statutory accountability, or reasons such as regional provision, it makes sense to be
done at the system-level. We will ensure the development of two ICPs at place from a single CCG will avoid duplication while enabling greater decision-making closer to individuals,
in line with our consistent operating model.
• Work between the CCG and local authorities will continue. All current joint funding with local authorities will continue for areas including for people with learning disabilities. Our
aspiration is to build on current joint commissioning arrangements with LAs and others where it adds values and to continue Intelligence hub that is a joint provider, CCG and LA
function will become permanent and all reporting for the ICS will be generated through the hub.
18
CONFIDENTIAL DRAFT FOR DISCUSSIONCambridgeshire and Peterborough
Sustainability and Transformation Partnership
Where are we going: We will develop and implement plans to streamline commissioning and
establish our provider collaboratives and ICPs
Based on our understanding of the NHSEI paper ‘Integrating care: Next steps to building strong and effective integrated care systems across England’, our system is
developing our system architecture to include vertical provider collaboratives that work to improve health and care at place through ICPs and horizontal provider
collaboratives that work across C&P, and potentially across systems, in clinical areas that are necessary to work across a larger footprint to ensure equitable access to
high quality services. Our provider collaboratives will involve all relevant partners, including commissioners and voluntary care, and deliver improvements for our population.
Our provider collaboratives will be built on 6 key principles:
Evidence-based, Integration of Flexible Sustainability through
Embed co-production Collaboration and joint
responding to local pathways to improve commissioning realignment of existing
with patients & families accountability
need and inequalities care and outcomes arrangements resources
Our 2 ICPs at place will progress work to integrate health and care services, so We want to build on our existing infrastructure to develop several system-wide
our patients have better experiences and outcomes. Our ICPs will work together, collaboratives which will improve how we deliver our services for our patients:
such as leveraging the research in the South to reduce inequalities in the North,
but will tailor solutions to their unique populations. • System-wide Mental Health and Learning Disabilities collaborative with
CPFT, CCG, and other relevant partners including VCS and patient
We have outlined a high-level plan for development: representatives. We aim to have this in shadow form by late Spring 2021.
• Phase 1 (Q1-Q4 21/22): We will agree outcome-based contracts for initial • System-wide Children and Young People collaborative that will include all
cohorts, for which ICPs will take responsibility of planning and delivering relevant partners such as LAs, CCS, and CPFT and will build on our existing
services using a ring-fenced budget based on current spend and population Children’s Board. We aim to operate in shadow form by late Summer 2021.
needs (such as health inequalities)
• Across-ICS development of our specialist clinical networks, with strategic
• Phase 2 (Q1-Q2 22/23) will see ICPs take responsibility for additional cohorts and operational responsibilities
• Phase 3 (Q3 22/23 onward) will see ICPs take responsibility for all • Acute care collaborative development for NHS acute providers
cohorts/priorities in their locality and full budget responsibility
We are still at the start of this journey. We will need to agree their responsibilities,
This will be a transitional process as we strengthen the ICP mandate and they take governance structure, and relationships with ICPs. Horizontal provider
on increasing responsibility for delivering against agreed outcomes and budgets. collaboratives will have to be sensitive to places and neighbourhoods.
CONFIDENTIAL DRAFT FOR DISCUSSION 19Cambridgeshire and Peterborough
Sustainability and Transformation Partnership
Where are we going: Our operating model is underpinned by our approach to leadership
We have an established leadership team with two joint executives, Roland Sinker from CUH and Jan Thomas from the CCG, to
ensure we benefit from both commissioning and provider insights. Our leadership team also includes our Chair, Mike More. System
Distributed leadership model
leaders meet weekly and engage through various forums to share learning and jointly problem solve, e.g. agreeing the distribution of
funding and resources across the system.
We have agreed at the ICS Partnership Board future ICS-wide roles, based on examples from thriving systems. We recognise the
importance of clinical and managerial leadership, and therefore we intend for all our ICS priorities, workstreams and enabling functions
to each have an Executive Lead, a NED Lead, and a Clinical Lead, as well as involvement of LAs where appropriate. Workstreams
have been established for our 6 LTP priorities and enabler groups, which are funded by all health organisations in the system to reflect
system commitment and responsibility. More information about our leadership model and current appointees can be found in the
appendix.
Over the next 18 months, we will establish 2 ICPs in the North and the South, building on the success of our Alliances. 2 Senior
Locality Directors, with experience in commissioning, place-based care and service provision, will be appointed to lead each of the
ICPs. These posts will be advertised and appointed to by end of Q4 20/21. Their role will be to lead the ICPs, as they take on
increasing responsibility for delivery at place, and ensure the infrastructure is in place to allow the ICPs to manage budgets locally. The
Alliances already have some dedicated capacity and infrastructure to drive change at place and neighbourhood level, but this will need
to be significantly increased to support larger scale delivery in future ICPs.
Leading within systems requires different attitudes, behaviours and skills to leading in organisations. Delivered with Co-create and Frimley Leadership Academy, we
offer a 6-month OD programme for the entire STP Board and a 12-month 20/20 Leading Beyond Boundaries for 35 Fellows from across the system. We will
continue to build on the a culture of learning, sharing, and collective problem solving we have relied on during the Covid-19 pandemic.
We believe that system change requires clinicians and managers who respect the skills each bring and can innovate, implement and evaluate transformation together.
We therefore offer development opportunities to clinical and non-clinical staff across the system, which we actively promote to equality, diversity and inclusion
networks. Our further development programmes include:
• Apprenticeship funded MBA for over 60 colleagues delivered by Henley Business School
• System-commissioned Stepping Up programme for Band 5-7 BAME staff that leads to access to additional opportunities such as stretch assignments in other
organisations and 21 BAME mentors in our mentoring network
• Additional information about our leadership development model can be found in the appendix.
20
CONFIDENTIAL DRAFT FOR DISCUSSIONCambridgeshire and Peterborough
Sustainability and Transformation Partnership
Where are we going: Our partnership is working on the development of our end state
governance structure as part of our consistent operating model
We recognise the importance of a clear governance structure as part of an operating model that enables us to achieve our vision and priorities. The recent consultation
paper published by NHSEI describes two potential legislative options, which will require different governance structures. Under option one, our System Partnership
Board would become a statutory committee and the CCG would retain its statutory accountabilities. Under option two, the ICS would be responsible for delivery of CCG
statutory functions. Our governance structure will flexibly respond to legislation and update to reflect the option pursued and meet the needs of the population.
In either case, for our end-state governance structure, we envision the ICS as accountable for developing and delivering a system-wide strategy. Our System
Partnership Board has agreed the vision and priorities for our system to deliver improvements in care and deliver our financial package. We will continue to manage
delivery of system priorities through our System Transformation and Delivery Group that will report over time into the statutory committee or ICS corporate body
Task and finish groups will be established to deliver on national priorities as needed.
Finances will continue to be managed at the system-level. Under option one, the ICS would continue to make strategic financial decisions through the already
established Finance, Planning and Performance group, and the CCG Governing Body and partners’ Boards would approve final plans. Both the ICS and the CCG GB
would be involved in agreeing and committing to a system-wide control total. If the ICS becomes a statutory body under option two, the ICS would become accountable
for all financial matters as well as strategic commissioning.
We will continue the development of our emerging Integrated Care Providers (ICPs), who from April 2022 will become accountable for capitated budgets and ensuring
delivery of high quality integrated care for their populations. Our emerging ICPs will also provide support to place-based development over the next year, including the
identification of place leaders.
We will embed primary care and specialist clinical leadership in our governance structure through our ICS Clinical Group and through designated clinical leadership for
our LTP priorities. Our end state governance model will incorporate the clinical and corporate governance that has been build up by GP leaders and will ensure a clear
voice from GPs at the top level of system governance. We will continue to ensure quality and patient safety at all levels, including appropriate quality oversight at
system and place.
The system has a System Partnership Board that meets monthly, in public every other month, and has an agreed ToR and attendance from councillors, VCS and the
Police as needed. When we agreed our ToR, Board members expressed concerns about the size of the Board, so we plan to revisit our ToR in June 2021 to ensure the
Board is the right size to facilitate engaging discussions and make decisions informed by all relevant partners.
21
CONFIDENTIAL DRAFT FOR DISCUSSIONYou can also read