Brexanolone for Treatment of Postpartum Depression (PPD) - November 2, 2018 Sage Therapeutics, Inc. Joint Meeting of the Psychopharmacologic Drugs ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
CO-1 Brexanolone for Treatment of Postpartum Depression (PPD) November 2, 2018 Sage Therapeutics, Inc. Joint Meeting of the Psychopharmacologic Drugs Advisory Committee (PDAC) and Drug Safety and Risk Management Advisory Committee (DSaRM)
CO-2 Brexanolone for Treatment of Postpartum Depression (PPD) Stephen Kanes, MD, PhD Chief Medical Officer Sage Therapeutics, Inc.
CO-3
Postpartum Depression (PPD) is Serious and
Common
Most common medical complication of childbirth
Affects 1 in 9 women who have given birth in US1
400,000 women annually2
Many women blindsided by onset of depression
No approved treatment options indicated for PPD
1. Ko, 2017; 2. CDC birthrate statistics, 2017
CO-4
Proposed Mechanism of Disease of PPD
Fluctuations in
Reduced GABA Dysregulated Neural Postpartum
Neuroactive Steroids
Function2 Network3,4 Depressive Episode
in Peripartum Period1
1. Deligiannidis, 2013; 2. Licheri V, 2015; 3. Duan C, 2017; 4. Fiorelli M, 2015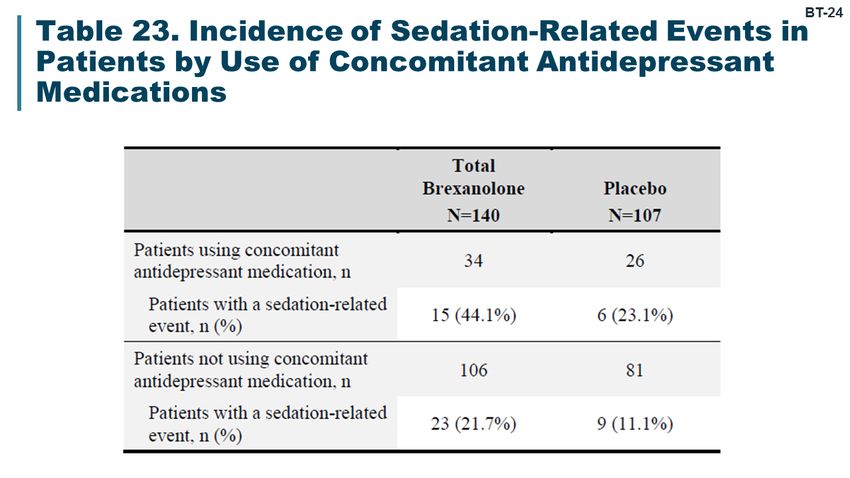
CO-5
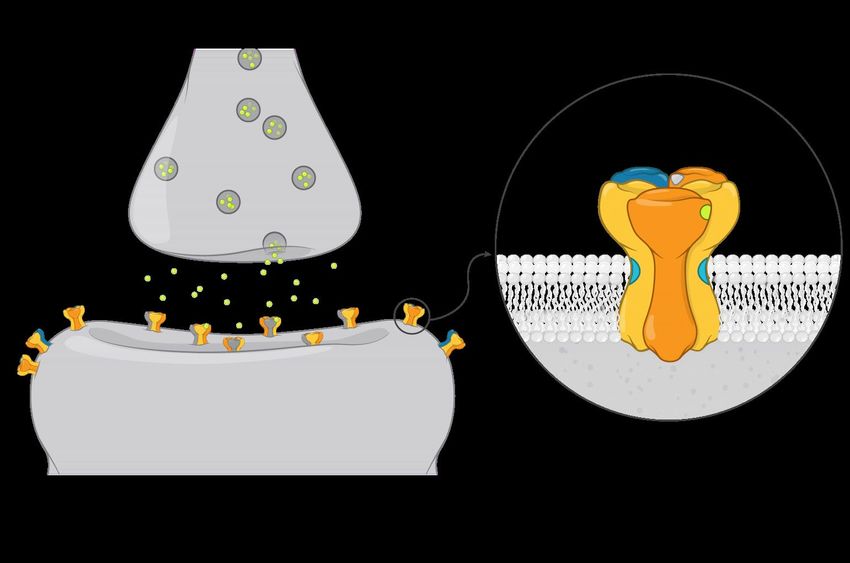
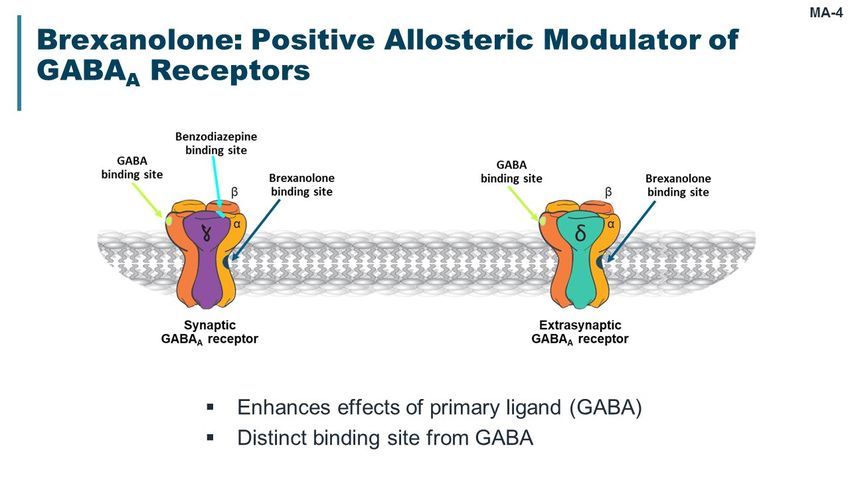
Brexanolone Modulates GABAA Receptors and
May Enhance Network Inhibition
Presynaptic
Chemically identical to terminal
endogenous
allopregnanolone
Positive allosteric modulator α β
GABA
site
of synaptic and GABA
Neuroactive
steroid site
extrasynaptic GABAA
receptors Extrasynaptic
Synaptic GABAA GABAA
Produces rapid and receptors receptors
sustained effects on Postsynaptic
GABAA receptor activity terminal
CO-6
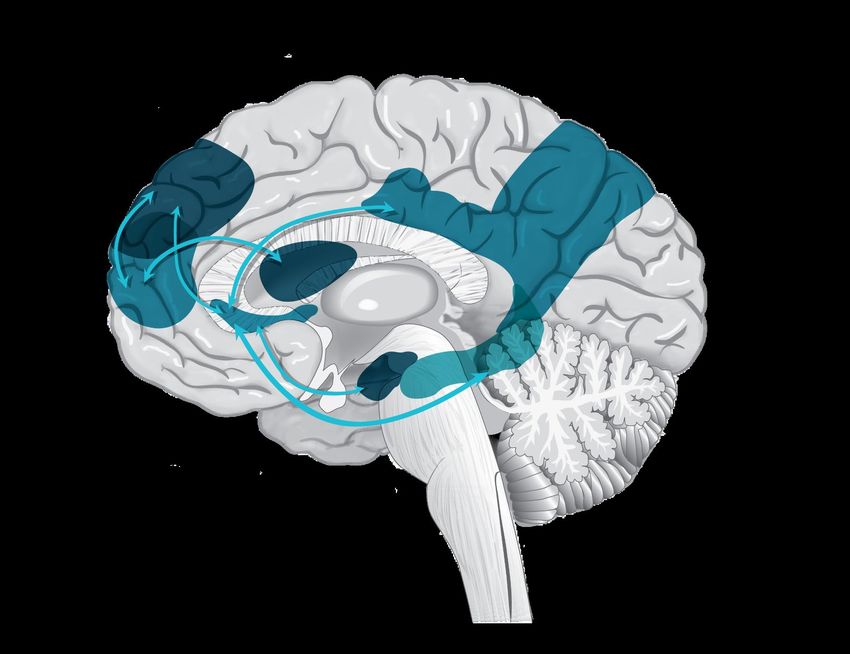
Network Dysregulation Associated with
Depression
GABAA receptors regulate
inhibition of brain networks
Brexanolone hypothesized
to alter symptoms of PPD
by resetting dysregulated
brain networks
CO-7
Brexanolone Designated as Breakthrough Therapy
for PPD
Breakthrough Therapy expedited development program
Serious condition
Preliminary clinical data indicate substantial improvement
over currently available therapy
Development program designed in consultation with FDA
First registration program specifically for PPD
Largest placebo-controlled PPD dataset collected
CO-8 Proposed Brexanolone Indication Brexanolone injection is indicated for the treatment of postpartum depression. Onset during pregnancy or after delivery Treated postpartum

CO-9 Brexanolone: Single Administration Over 60 Hours as Continuous Infusion Patient weight-based dosing Recommended maximum dosing regimen is 90 µg/kg/h Includes titration and taper
CO-10
Brexanolone PPD Clinical Studies
Key Studies
Proof of
Concept Study 202A Study 202B Study 202C
Study PPD 201CO-11
Brexanolone Clinical Pharmacology Program
Study Population Objective
101 Healthy male volunteers Metabolism/excretion
Non-dependent healthy subjects experienced with
102 Human abuse potential
recreational CNS depressant drugs
Patients with hepatic impairment
103 Safety/PK
Healthy volunteers
Patients with renal impairment
104 Safety/PK
Healthy volunteers
105 Healthy volunteers Drug/Drug interaction
106 Healthy volunteers QT study
107 Healthy volunteers Bioavailability/food effect
108 Healthy lactating female volunteers Breast milk concentrationsCO-12 Brexanolone Provides Rapid, Stable Reduction in Depressive Symptoms with Principles for Safe Administration Rapid reduction in depressive symptoms within 2.5 days Well-characterized safety profile consistent with GABA mechanism of action Principles for safe administration
CO-13
Agenda
Samantha Meltzer-Brody, MD University of North Carolina
Unmet Need for Ray M. Hayworth Distinguished Professor at Chapel Hill
Postpartum Depression of Mood Disorders
Treatment Associate Professor, Department of Psychiatry UNC Center for Women’s Mood
Director, Perinatal Psychiatry Program Disorders
Brexanolone Clinical
Christopher Silber, MD
Study Design and Sage Therapeutics, Inc.
Senior Vice President, Clinical Development
Efficacy
Helen Colquhoun, MD
Brexanolone Safety Sage Therapeutics, Inc.
Vice President, Medical Science
University of North Carolina
Clinical Perspective Samantha Meltzer-Brody, MD at Chapel Hill
Amy Schacterle, PhD
Q&A Moderator Senior Vice President, Regulatory Affairs Sage Therapeutics, Inc.
and Quality AssuranceCO-14
Additional External Experts
Associate Professor of Psychiatry, Ob/Gyn, and
Quantitative Health Sciences
University of Massachusetts Medical School
Nancy Byatt, DO, MS, MBA
Director, Women’s Mental Health Division
Medical Director, Massachusetts Child Psychiatry Access Program
(MCPAP) for Moms
Vice President, Product Development
Kendra Howard, PharmD Option Care
Home and Alternate Treatment Site Infusion ServicesCO-15 Unmet Need for Postpartum Depression Treatment Samantha Meltzer-Brody, MD, MPH Ray M. Hayworth Distinguished Professor of Mood Disorders Associate Professor, Department of Psychiatry The University of North Carolina at Chapel Hill Director, Perinatal Psychiatry Program UNC Center for Women’s Mood Disorders President Marcé of North America (Perinatal Depression Research Society)
CO-16
PPD Distinct from Baby Blues
Baby Blues Postpartum Depression
Normal emotional adjustment to Meets DSM-5 criteria for major
having a baby depressive episode
Occurs in most women (≤ 80%)1 Persistent symptoms
Transient symptoms Impairs function for at least
Mild mood lability 2 weeks
No more than mild dysfunction Warrants treatment
Resolves within 10 to 14 days
1. NIMH, 2018.CO-17
PPD Homogenous Form of Major Depression
Occurs in reproductive-aged women at discrete time point in
3rd trimester of pregnancy or after childbirth
Specific pathophysiology including hormonal fluctuations and
genetic contributions
More heritable than non-perinatal depression1
44 to 54% in perinatal vs 32% in non-perinatal depression
1. Viktorin, 2016CO-18
PPD is Debilitating with Broad Range of Clinical
Symptoms
Low mood, decreased interest, unable to enjoy baby
Anxiety, ruminating thoughts, vigilance
Being unable to sleep even when baby is sleeping
Interference with mother-baby relationship
Untreated PPD may result in significant adverse consequences
for child and family1
1. Netsi, 2018CO-19
Women with PPD May Experience Suicidal Ideation
and Increased Risk for Suicide1
Recent studies suggest postpartum suicidal ideation occurs in
19% to 30% of women with PPD2-3
Leading cause of maternal death following childbirth4
Severe cases can have intrusive thoughts and fear of harming
baby
41% of women with PPD vs 7% in control mothers5
Stigma around PPD symptoms
1. Savitz, 2011; 2. Mauri, 2012; 3.Wisner, 2013; 4. Oates, 2003; 5. Jennings, 1999CO-20
Women Suffering with PPD Often Not Diagnosed
Screening for PPD is inconsistent
National movement to improve standardized screening
American College of Obstetricians and Gynecologists
(ACOG) 4th trimester guidelines1
California Maternal Mental Health legislation signed
September 26, 20182
1. ACOG, 2018; 2. http://leginfo.legislature.ca.govCO-21
Currently No Pharmacologic Therapies Approved
to Treat PPD
Standard of Care Limitations
Approved for major depressive disorder
SSRI antidepressant May take weeks to months for initial effect
medications Many women do not achieve adequate
response or symptom remission1
Patients and physicians need novel pharmacologic options
1. Molyneaux, 2014CO-22 Great Need for New, Effective, Rapidly-Acting Therapies for PPD Lasting negative effects associated with untreated or poorly treated PPD Clear unmet need for improved treatment options Effective and rapidly-acting medication would Reduce potential for significant morbidity and mortality Allow more positive interactions with mother and baby
CO-23 Brexanolone Clinical Study Design and Efficacy Christopher Silber, MD Senior Vice President, Clinical Development Sage Therapeutics, Inc.
CO-24
3 Key Brexanolone Studies: 202A, 202B, and 202C
Used Nearly Identical Study Designs
90 µg/kg/h
Randomization
Follow-up Follow-up
60 µg/kg/h (202B)
Day 7* Day 30
Placebo
Start Dose End Dose Discharge
Hour 0 Hour 60 Hour 72
Screening Clinical Research Site Home
Primary Endpoint
* 62% of patients in key studies also had visits at Days 14 and 21CO-25
Dose Titration and Taper to Optimize Tolerability
100
90
80
70
60
Dose
50
(µg/kg/h)
40
30
20
Brexanolone 90 dose regimen
10 Brexanolone 60 dose regimen
0
0 4 8 12 16 20 24 28 32 36 40 44 48 52 56 60
Time (hours)
Day 1 Day 2 Day 2.5CO-26 Key Study Entry Criteria Ages 18 to 45 years ≤ 6 months postpartum Major depressive episode verified by Structured Clinical Interview for DSM Onset 3rd trimester through 4 weeks postpartum Willing to temporarily cease breastfeeding Hamilton Rating Scale for Depression (HAM-D) total score prior to dosing of ≥ 26 (Studies 202A and 202B) 20 to 25 (Study 202C)
CO-27 Primary Endpoint: 17-Item HAM-D Change from baseline in HAM-D total score at end of infusion (Hour 60) Valid and reliable scale used in clinical research One of several standard measures to quantify drug effect for approval Adapted for rapid onset of action for PPD Assessment standardized to minimize variability
CO-28 Key Secondary Endpoint and Additional Analyses Key secondary endpoint (202B and 202C) Change from baseline in HAM-D total score at Day 30 Additional HAM-D analyses Change in total score over time Individual item scores Subgroup by baseline characteristic Response (50% reduction from baseline) Remission (total score ≤ 7 points) Clinical Global Impression Improvement (CGI-I) response
CO-29 Statistical Considerations Consistent Across Key Studies Full Analysis Set (FAS): All randomized and dosed patients Primary statistical analysis for primary and key endpoints Mixed effects model for repeated measures (MMRM)
CO-30
Few Patients Discontinued in Key Studies
Study 202A Study 202B Study 202C
N=21 N=122 N=104
Pooled Overall
N=247
Brexanolone 60 Brexanolone 90 Placebo
n=38 n=102 n=107
Adverse event (n=1)
Reason for Lost to follow-up (n=1)
Lost to follow-up (n=3) Lost to follow-up (n=2)
Discontinuation Withdrawal by patient (n=2)
Withdrawal by patient (n=4)
Completed Brexanolone 60 Brexanolone 90 Placebo
Study n=35 n=94 n=105CO-31
Key Studies: Demographics Balanced Across
Treatment Groups
202A 202B 202C
BRX 90 PBO BRX60 BRX90 PBO BRX90 PBO
N=10 N=11 N=38 N=41 N=43 N=51 N=53
Age, years Mean (SD) 27 (5) 29 (5) 28 (6) 28 (6) 27 (6) 28 (6) 27 (6)
18 to 24 years 30 18 37 39 37 33 32
Age in categories, %
25 to 45 years 70 82 63 61 63 67 68
White 30 45 66 71 63 57 62
Race, % Black or African-American 70 55 32 20 35 43 36
Asian/Other - - 3 10 2 - 2
Hispanic or Latino - - 8 17 16 20 26
Ethnicity, %
Not Hispanic or Latino 100 100 92 83 84 80 74
Baseline weight, kg Mean (SD) 87 (29) 77 (22) 87 (21) 81 (20) 82 (23) 87 (25) 87 (24)CO-32
Baseline Characteristics in Key Studies
202A 202B 202C
BRX 90 PBO BRX60 BRX90 PBO BRX90 PBO
N=10 N=11 N=38 N=41 N=43 N=51 N=53
Antidepressant use at baseline, % 30 27 32 24 28 18 19
Duration between delivery and index treatment, months
Mean (SD) 4 (2) 3 (1) 4 (2) 4 (2) 3 (2) 4 (2) 3 (2)
Onset of current PPD, %
3rd trimester 30 36 26 20 33 22 23
Within 4 weeks after delivery 70 64 74 81 67 78 77
Baseline HAM-D total score mean (SD) 28 (1) 29 (2) 29 (3) 28 (2) 29 (3) 23 (2) 23 (2)
Edinburgh Postnatal Depression Scale,
21 (4) 19 (4) 22 (3) 20 (4) 22 (3) 19 (4) 19 (4)
mean (SD)CO-33
Each Key Study Independently Demonstrated
Brexanolone Efficacy: Study 202A
0 Brexanolone 90 (N=10)
Placebo (N=11)
-5
LS Mean -10
Change in
HAM-D ∆ = 12.2 ∆ = 11.9
Total Score -15 p=0.008 p=0.010
(SE)
-20 *
* * *
*
-25
0 4 8 12 16 20 24 28 32 36 40 44 48 52 56 60 Day 30
Time (hours)
*p < 0.05CO-34
Each Key Study Independently Demonstrated
Brexanolone Efficacy: Study 202B
Brexanolone 60 (N=38)
0 Brexanolone 90 (N=41)
Placebo (N=43)
-5
BRX 90 ∆ = 3.7 ∆ = 3.8
LS Mean -10 vs Placebo p=0.03 p=0.048
Change in
HAM-D
Total Score -15
(SE) * * * *
* *
-20
* *
BRX 60 ∆ = 5.5 ∆ = 5.6
vs Placebo p=0.001 p=0.004
-25
0 4 8 12 16 20 24 28 32 36 40 44 48 52 56 60 Day 30
Time (hours)
*p < 0.05
At Hour 60: Brexanolone 60 (n=37) Brexanolone 90 (n=39) Placebo (n=43)CO-35
Each Key Study Independently Demonstrated
Brexanolone Efficacy: Study 202C
0 Brexanolone 90 (N=51)
Placebo (N=53)
-5
∆ = 2.5 ∆ = 0.54
p=0.016 p=0.671
LS Mean -10
Change in
HAM-D
Total Score -15 *
(SE) *
-20
-25
0 4 8 12 16 20 24 28 32 36 40 44 48 52 56 60 Day 30
Time (hours)
*p < 0.05
At Hour 60: Brexanolone 90 (n=49) Placebo (n=52)CO-36
Key Studies: Individual HAM-D Item Scores
Consistently Favor Brexanolone at Hour 60
Study 202B Pooled
Item Description Brexanolone 60 vs Placebo Brexanolone 90 vs Placebo
Depressed mood
Feelings of guilt
Suicide
Work and activities
Insomnia – early
Insomnia – middle
Insomnia – late
Retardation
Agitation
Anxiety psychic
Anxiety somatic
Somatic symptoms GI
Somatic symptoms general
Genital symptoms
Hypochondriasis
Loss of weight
Insight
-1.2 -0.6 0.0 0.6 1.2 -1.2 -0.6 0.0 0.6 1.2
Brexanolone 60 (N=38)
Brexanolone 90 (N=102) Favors Brexanolone Favors Placebo Favors Brexanolone Favors PlaceboCO-37
Key Studies: Brexanolone Efficacy Consistent
Across Subgroups at Hour 60
Study 202B Pooled
Subgroup Brexanolone 60 vs Placebo Brexanolone 90 vs Placebo
Overall
18 to 24 years
Age
25 to 45 years
White
Race
African-American
Hispanic or Latino
Ethnicity
Not Hispanic or Latino
Antidepressant Yes
use No
≤ 25 kg/m2
BMI > 25 to < 30 kg/m2
≥ 30 kg/m2
Duration delivery < 3 months
to index tx ≥ 3 months
3rd trimester
Symptom onset
Within 4 weeks delivery
-15 -10 -5 0 5 10 15 -15 -10 -5 0 5 10 15
Favors Brexanolone Favors Placebo Favors Brexanolone Favors PlaceboCO-38
HAM-D Remission Achieved in Greater Proportion of
Patients with Brexanolone than Placebo at Hour 60
Study 202A Study 202B Study 202C
p=0.008 p=0.083 p=0.001 p=0.003
100%
80%
70%
Patients 61%
Achieving 60% 51%
HAM-D
Remission 39%
40% 31%
at Hour 60
20% 16%
9%
0%
N=10 N=11 N=39 N=37 N=43 N=49 N=52
Brexanolone 90 Brexanolone 60 Placebo
HAM-D remission is ≤ 7 HAM-D total scoreCO-39
HAM-D Remission Maintained in Brexanolone Group
at Day 30
Study 202A Study 202B Study 202C
p=0.030 p=0.351 p=0.105 p=0.309
100%
80%
70%
Patients 62%
Achieving 60%
49% 48%
HAM-D
Remission 39%
40% 31%
at Day 30
18%
20%
0%
N=10 N=11 N=39 N=37 N=43 N=49 N=52
Brexanolone 90 Brexanolone 60 Placebo
HAM-D remission is ≤ 7 HAM-D total scoreCO-40
HAM-D Response Achieved in Greater Proportion of
Patients with Brexanolone than Placebo at Hour 60
Study 202A Study 202B Study 202C
p=0.198 p=0.049 p=0.005 p=0.017
100%
87%
80% 74% 76%
70%
Patients 60%
Achieving 60% 56%
HAM-D
Response 40% 36%
at Hour 60
20%
0%
N=10 N=11 N=39 N=37 N=43 N=49 N=52
Brexanolone 90 Brexanolone 60 Placebo
HAM-D response is ≥ 50% reduction from baseline in HAM-D total scoreCO-41
HAM-D Response Maintained in Brexanolone Group
at Day 30
Study 202A Study 202B Study 202C
p=0.086 p=0.035 p=0.004 p=0.586
100%
83%
79%
80% 71%
70% 69%
Patients
Achieving 60%
50%
HAM-D
Response 40%
at Day 30 27%
20%
0%
N=10 N=11 N=39 N=37 N=43 N=49 N=52
Brexanolone 90 Brexanolone 60 Placebo
HAM-D response is ≥ 50% reduction from baseline in HAM-D total scoreCO-42
CGI-I Response Achieved in Greater Proportion of
Patients with Brexanolone than Placebo at Hour 60
Study 202A Study 202B Study 202C
p=0.080 p=0.010 p=0.013 p=0.001
100%
82% 84%
80% 80%
80%
Patients
Achieving 60% 56% 56%
CGI-I
Response 40% 36%
at Hour 60
20%
0%
N=10 N=11 N=39 N=37 N=43 N=49 N=52
Brexanolone 90 Brexanolone 60 Placebo
CGI-I Response is ‘very much improved’ or ‘much improved’CO-43
CGI-I Response Achieved in Greater Proportion of
Patients with Brexanolone than Placebo at Day 30
Study 202A Study 202B Study 202C
p=0.030 p=0.046 p=0.014 p=0.440
100%
80% 80% 81% 79%
80% 72%
Patients
Achieving 60% 52%
CGI-I
Response 40%
at Day 30 27%
20%
0%
N=10 N=11 N=43 N=38 N=41 N=51 N=53
Brexanolone 90 Brexanolone 60 Placebo
CGI-I Response is ‘very much improved’ or ‘much improved’CO-44 Brexanolone Demonstrated Rapid and Clinically Meaningful Symptom Improvement in 2.5 Days Primary endpoint met in all 3 independent studies Brexanolone consistently demonstrated improvement across Studies Severities of PPD Endpoints Stable effect sustained through 4 weeks after infusion Efficacy demonstrated for both 60 and 90 dose regimens
CO-45 Brexanolone Safety Helen Colquhoun, MD Vice President, Medical Science Sage Therapeutics, Inc.
CO-46
Brexanolone PPD Program Safety Exposures
Number Exposed
to Brexanolone
Total unique exposures 367
Clinical pharmacology 198
Essential tremor 25
Postpartum depression 144
Study 201 (Open-label) 4
Key studies 140
Study 202A 10
Study 202B 79
Study 202C 51CO-47 Safety and Tolerability of 90 and 60 Dose Regimens Similar Well-characterized safety and tolerability profile Most events related to primary pharmacology of brexanolone Onset in first 24 hours – all receiving same dose After 24 hours – similar frequency and type of AEs Generally similar safety profiles in brexanolone 90 and 60 doses Combining doses provides larger dataset to detect and summarize less frequent events Presentation includes doses separately and combined
CO-48 Agenda for Brexanolone Safety Presentation Suicidality Lactation study Overall adverse events Adverse events related to primary pharmacology
CO-49 No Evidence of Increased Suicidality Columbia Suicide Severity Rating Scale (C-SSRS) did not show clinical worsening in patients on brexanolone compared to placebo 2 patients reported suicidal behavior after discharge; both had history of suicidal behavior prior to study entry 1 reported SAE of overdose of other medications 1 reported non-suicidal self-injurious behavior
CO-50
No Need to Interrupt Breastfeeding While
Receiving Brexanolone
Breastfeeding during infusion should be discussed by mother and
physician
Lactation study using 90 dose regimen demonstrated low Relative
Infant Dose (RID) (1.3% at maximum)
Drugs with RID < 10% considered low risk to breast fed infant1
Low oral bioavailability (< 5%) in adults
1. Bennett, 1996CO-51
Brexanolone Adverse Event Incidence
Similar to Placebo
Brexanolone Placebo
N=140 N=107
n (%) n (%)
AE 70 (50.0) 54 (50.5)
SAE 2 (1.4) 0
AE leading to study withdrawal 1 (0.7) 0
AE leading to study drug discontinuation 3 (2.1) 1 (0.9)
AE leading to dose interruption or reduction 10 (7.1) 3 (2.8)
Severe AE 3 (2.1) 2 (1.9)
Death 0 0CO-52
Brexanolone Has a Well-Characterized Adverse
Event Profile
Adverse Events in ≥ 3% Patients in Either Total Brexanolone or Placebo Group
Brexanolone
60 Dose 90 Dose Total Placebo
N=38 N=102 N=140 N=107
Adverse Event % % % %
Headache 18.4 14.7 15.7 14.0
Dizziness 15.8 12.7 13.6 7.5
Somnolence 18.4 7.8 10.7 4.7
Infusion site pain 2.6 8.8 7.1 4.7
Nausea 2.6 5.9 5.0 7.5
Dry mouth 10.5 2.9 5.0 0.9
Sedation 2.6 4.9 4.3 0.9
Fatigue 2.6 3.9 3.6 1.9
Rash 2.6 1.0 1.4 3.7
Abnormal dreams 0 1.0 0.7 3.7CO-53
Sedation-Related Events Reflect Primary
Pharmacology of Brexanolone
Sedation-Related Events
AEs reported Dizziness 14%
Somnolence 11%
Sedation 4%
Fatigue 4%
AEs coded in MedDRA to closest Loss of consciousness 2%
preferred term Vertigo 1%
Syncope 1%
Feeling drunk < 1%
AEs related to GABAA pharmacology Altered state of consciousness < 1%
grouped further Presyncope < 1%CO-54
Sedation-Related Events: Incidence and Risk
Factors
Incidence of sedation-related events
Brexanolone: 27% (38/140) patients
34% patients on 60 dose regimen
26% patients on 90 dose regimen
Placebo: 14% (15/107) patients
Increased incidence of sedation-related events reported in
patients taking concomitant
Antidepressants
BenzodiazepinesCO-55
No Incremental Sedation Risk Associated with
Increasing 90 Dose Level at Hour 24
Total brexanolone
All brexanolone patients Placebo
receiving same dose
Brexanolone 90
30%
Brexanolone 60
23.6%
20%
Percent
of
Patients 10.3%
10% 7.8% 7.9%
3.7%
2.0% 1.9%
0%
0%
0 to 24 Hours > 24 to 60 Hours > 60 Hours (Post Infusion)CO-56
Loss or Near Loss of Consciousness Events
Dose at Time to Excessive
Onset of AE Onset Sedation-Related Time to Regain
(µg/kg/h) (hours) AE Dose Action Taken Consciousness Comments
Loss of Interrupted/Restart
Patient A EST* +38.5 10 minutes
consciousness at 90 µg/kg/h Overdose-
infusion pump
Loss of Interrupted/Restart malfunction
Patient B EST** +1.5 14 minutes
consciousness at 60 µg/kg/h
Syncope and Dizziness, sweating,
Patient C 60 +8.6 altered state of Discontinued 10 minutes nausea 10 minutes
consciousness before LOC
Loss of Interrupted/Restart Somnolence shortly
Patient D 60 +34.8 15 minutes
consciousness at 30 then 60 µg/kg/h before LOC
Self-limiting
Vertigo and presyncope earlier
Patient E 90 +36.5 Discontinued Not applicable
Presyncope that day; did not
lose consciousness
* A: estimated to be > 700 µg/kg as a bolus ** B: estimated to be > 1,200 µg/kg/h over 90 minutesCO-57
Clearance of Brexanolone is Rapid and Biphasic
Initial phase has half-life of 40 minutes
Results in rapid clearance of brexanolone from plasma if
Infusion interrupted
At end of infusion
Brexanolone dose reduced
Rapid resolution of any sedative symptoms underpins recommendation
To pause infusion if excessive sedation quickly progresses
To reduce dose if excessive sedation progresses more slowly
If patient is well, monitoring may cease at end of infusionCO-58
Excessive Sedation is Monitorable and
Manageable
Monitorable by healthcare professional oversight
Patient report of feeling overly sedated
Pulse oximetry
Manageable
Immediately pause infusion if loss of consciousness
Pause infusion if excessive sedation progresses quickly
Reduce dose if excessive sedation evolving more slowly
No sequelae such as airway, respiratory or hemodynamic
compromise and no falls or injuries to patient or babyCO-59 Excessive Sedation is Reversible Excessive sedation reversed within 15 minutes of pausing infusion Patients observed until awake and alert No other interventions necessary Once recovered, infusion restarted in 3 of 5 cases of excessive sedation at protocol or lower dose
CO-60 Supporting Safe Administration of Brexanolone Healthcare professional oversight Monitoring with pulse oximetry Communication of risks of and mitigations for excessive sedation and loss of consciousness Patient will not be primary caregiver of baby and should sit or lie down if feeling dizzy or somnolent
CO-61
Risk Evaluation and Mitigation Strategy
Goal of REMS: to mitigate risk of loss of consciousness
Key components of REMS with Elements to Assure Safe Use
Enrollment of prescriber in REMS
Enrollment of all patients in registry
Data collected and further characterization of loss of
consciousness, if it occurs
Restricted distribution to certified healthcare settingsCO-62
Brexanolone Has Positive Benefit-Risk
Assessment
Rapid and stable efficacy in 3 adequate, controlled studies
Well-characterized safety profile and well-tolerated
Risk of loss of consciousness mitigated by healthcare
professional oversight, labeling, medication guide, and REMS
Both dose regimens support efficacy and tolerability
Efficacy of 90 dose regimen replicated
Down-titration easier to operationalize than active
up-titrationCO-63 Clinical Perspective Samantha Meltzer-Brody, MD, MPH
CO-64 Goal of PPD Treatment: Reduce Symptoms as Quickly as Possible Postpartum period vulnerable time for women and their families Critical to rapidly treat women who suffer with PPD to improve depressive symptoms and impairment in functioning Brexanolone magnitude of improvement in HAM-D unlike any currently available treatments
CO-65 Brexanolone Provides an Opportunity to Urgently Alleviate Suffering from PPD Current treatment with SSRIs Weeks to months for potential treatment effect Many women do not achieve full response Often troublesome side effects Brexanolone Know response within 60 hours
CO-66 Potential Risks are Manageable Safely managed sedation related side effects Dose reduction successful strategy to mitigate risk of loss of consciousness Measures to ensure oversight and monitoring of potential side effects matches supervision during clinical trials
CO-67 Brexanolone is Primary Treatment for PPD 71% of brexanolone patients did not receive antidepressants at any time during study Efficacy demonstrated regardless of antidepressant use ~75% of patients achieved HAM-D Response at Hour 60 ~50% of patients achieved HAM-D Remission at Hour 60
CO-68 Remission Data are Clinically Meaningful 50% remission rate by 60 hours of treatment can impact Ability to function Depressive symptoms Interactions with baby and family Brexanolone completely new and most welcome tool for helping women with PPD
CO-69 Brexanolone for Treatment of Postpartum Depression (PPD) November 2, 2018 Sage Therapeutics, Inc. Joint Meeting of the Psychopharmacologic Drugs Advisory Committee (PDAC) and Drug Safety and Risk Management Advisory Committee (DSaRM)
CO-70 Backup Slides
CO-71
CO-72
CO-73
CO-74
CO-75
CO-76
CO-77
CO-78
CO-79
CO-80
CO-81
CO-82
CO-83
CO-84
CO-85
CO-86
CO-87
CO-88
You can also read