Better Health Programme South Africa (BHPSA) - SBCC Strategy for NCD Prevention in South Africa October 2020 - NCDs
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Better Health Programme South Africa (BHPSA) SBCC Strategy for NCD Prevention in South Africa October 2020
Dr. Sara Jewett Nieuwoudt, School of Public Health, University of the
Witwatersrand (corresponding author: sara.nieuwoudt@wits.ac.za)
Dr. Nobulembu Mwanda-Motjuwadi, COPESSA
Ms. Matata Diomande, Independent SBCC Expert
This report was commissioned by BHPSA.
The UK’s Better Health Programme (BHP), is a global health system
strengthening programme led by the UK Foreign, Commonwealth and
Development Office (FCDO) and delivered in South Africa by Mott
MacDonald.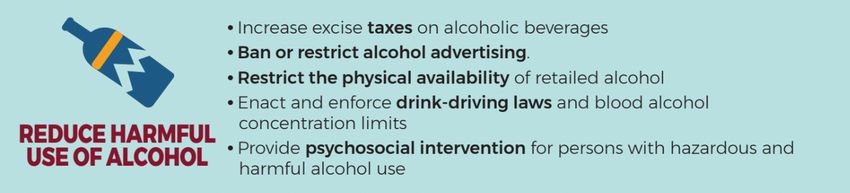
Mott MacDonald
10 Fleet Place
London EC4M 7RB
United Kingdom
T +44 (0)20 7651 0300
mottmac.com
Better Health Programme
Foreign and Commonwealth
Development Office
King Charles Street
London SW1A 2AH
United Kingdom South Africa (BHPSA)
SBCC Strategy for NCD Prevention in South
Africa
October 2020
Directors: J H K Harris (British), G W I
Leonard (British), M D Haigh (British), N
Pather, U M Thys
Mott MacDonald Development South
Africa (Pty) Limited is a member of the
Mott MacDonald Group. Registered in
South Africa no. 2002/007074/07.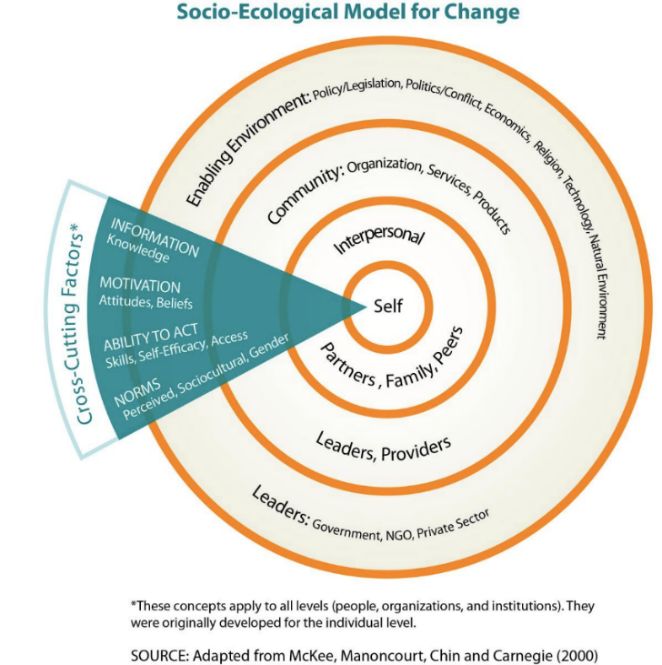
Mott MacDonald | Better Health Programme South Africa (BHPSA) 1
SBCC Strategy for NCD Prevention in South Africa
Issue and Revision Record
Revision Date Originator Checker Approver Description
Sara
1 30Oct20 Nieuwoudt Myles Ritchie Lucy Palmer First draft
Vimla Moodley
Document reference: 397868 1.1.2.1
Information class: Standard
This document is issued for the party which commissioned it and for specific purposes connected with the above-captioned
project only. It should not be relied upon by any other party or used for any other purpose.
We accept no responsibility for the consequences of this document being relied upon by any other party, or being used for
any other purpose, or containing any error or omission which is due to an error or omission in data supplied to us by other
parties.
This document contains confidential information and proprietary intellectual property. It should not be shown to other parties
without consent from us and from the party which commissioned it.
October 2020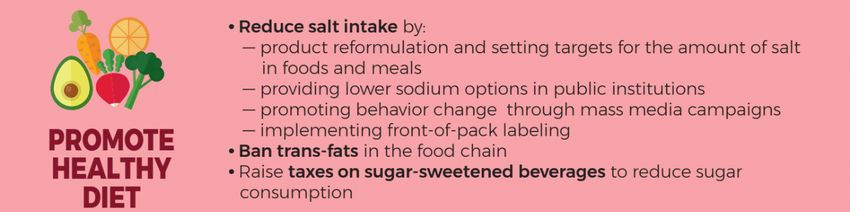
Mott MacDonald | Better Health Programme South Africa (BHPSA) 2
SBCC Strategy for NCD Prevention in South Africa
Contents
Acronyms 5
Executive summary 6
1 Background 10
1.1. Purpose 11
1.2. The importance of an SBCC strategy in NCD prevention 11
1.3. Process undertaken in the development of this document 11
1.4. Intended use of this document 12
2. KEY COMPONENTS OF AN EFFECTIVE SBCC STRATEGY 13
2.1. Summary of SBCC quality standards 13
2.2. Planned process 13
2.3. Grounded in evidence and context 14
2.4. Grounded in theory 15
2.5. Audience specific 16
2.6. Clear SBCC objectives 17
2.7. Strategic approaches 18
2.8. Participatory and multisectoral 19
2.9. Gender equity 19
2.10. Social inclusion and stigma prevention 19
2.11. Life course approach 20
3. CONTEXT FOR SBCC FOR NCD PREVENTION 21
3.1. Global NCD situation 21
3.2. NCD context in South Africa 21
3.3. NCD prevention: global “best buys” and recommended practices 23
3.3.1. Tobacco reduction intervention evidence 24
3.3.2. Physical activity intervention evidence 26
3.3.3. Promoting healthy diet intervention evidence 27
3.3.4. Reducing harmful use of alcohol intervention evidence 28
3.4. Successful SBCC campaigns: global and local 29
3.4.1. Global campaigns 29
3.4.2. NCD SBCC campaigns in South Africa 31
3.5. Common NCD prevention barriers and solutions 35
4. STRATEGIC ALIGNMENT WITH DRAFT NSP FOR NCDs 2021-2026 40
October 2020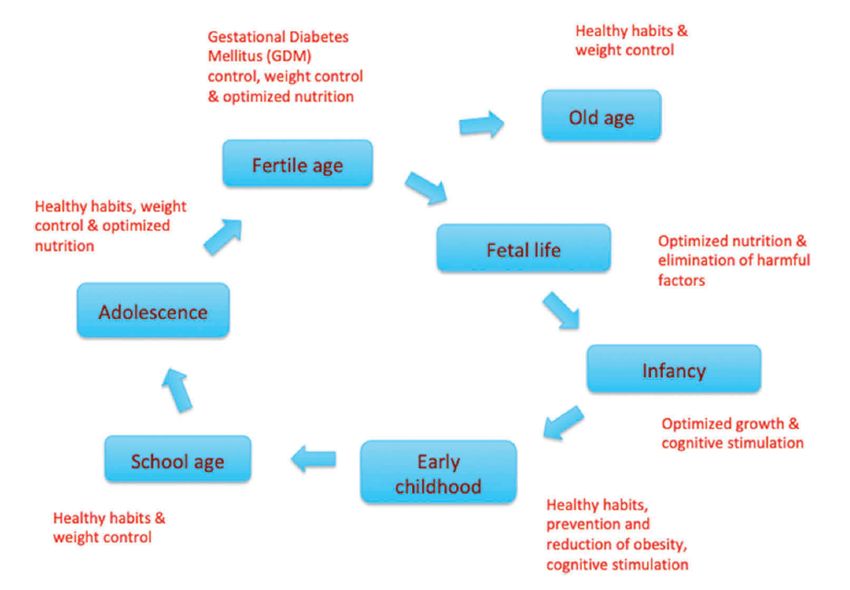
Mott MacDonald | Better Health Programme South Africa (BHPSA) 3
SBCC Strategy for NCD Prevention in South Africa
5. AUDIENCE ANALYSIS, EXAMPLES OF COMMUNICATION OBJECTIVES
AND APPROACHES FOR NCD PREVENTION 43
5.1. Audience analysis and insights 43
5.1.1. Tobacco use prevention or cessation - audience analysis 43
5.1.2. Physical inactivity prevention - audience analysis 44
5.1.3. Healthy diet promotion - audience analysis 46
5.1.4. Prevention of harmful alcohol use 47
5.2. Examples of NSP-aligned communication objectives 48
5.2.1. Tobacco sample communication objectives 49
5.2.2. Physical activity sample communication objectives 50
5.2.3. Healthy diet sample communication objectives 51
5.2.4. Alcohol sample communication objectives 52
5.3. SBCC: Recommended approaches, channels and message considerations 53
5.3.1. Important SBCC approaches for NCD prevention 53
5.3.2. Moving from approaches to channel selection and messages 54
5.3.3. Examples: key approaches, channels, and message considerations for
specific audiences 56
6. MONITORING AND EVALUATION CONSIDERATIONS 59
6.1. Why M&E is important 59
6.2. Key M&E milestones 59
6.2.1. Formative/Baseline evaluation 60
6.2.2. Ongoing monitoring 60
6.2.3. Process and implementation fidelity evaluations 60
6.2.4. Midterm evaluations 61
6.2.5. Outcome evaluations 61
6.2.6. Midterm and outcome evaluation research designs 61
6.2.7. National surveys and surveillance data 61
6.2.8. Cost-effectiveness evaluations 62
6.3. Theory based M&E: overview of change models 62
6.4. Proposed TOC for NCD prevention SBCC programming 62
6.5. M&E plan users 64
6.6. “SMART” SBCC communication objectives: implications for M&E planning 64
6.7. The importance of appropriate and informed indicators 64
6.7.1. SBCC communication objectives: impact and outcome indicators 65
6.7.2. Data collection sources: are data attainable? 65
6.8. Data analysis 66
6.8.1. Ensuring quality of data 66
6.8.2. Analysis 66
6.8.3. Interpretation of findings 67
6.8.4. Data use 67
7. RECOMMENDATIONS, LIMITATIONS AND CONCLUSION 68
October 2020
Mott MacDonald | Better Health Programme South Africa (BHPSA) 4
SBCC Strategy for NCD Prevention in South Africa
7.1. Clarify planning process 68
7.1.1. Identify key deliverables 68
7.1.2. Promote gender equity and social inclusion 68
7.1.3. Apply a life course perspective to audience selection 68
7.2. Clarify roles of different stakeholders in the design phase 68
7.2.1. Coordination and planning 68
7.2.2. Resource mobilisation and budget setting 70
7.2.3. Implementation and monitoring 70
7.2.4. Research and evaluation 71
7.3. Prioritise communication objectives (and audiences) based on evidence 71
7.4. Align SBCC approaches with communication objectives 71
7.5. Plan for disruption to mitigate its impact 72
7.6. Use this document 72
7.7. Document limitations 72
7.8. Conclusion 73
Appendices 74
APPENDIX A: Key Stakeholders consulted in the development process 74
APPENDIX B: SBCC Quality Assurance and Improvement Tool Overview 75
APPENDIX C: APEASE Criteria to assess proposed or existing aspects of SBCC
interventions 79
APPENDIX D: 20 steps to chart a healthier way forward for alcohol in SA, now and into the
future 80
REFERENCES 84
October 2020
Mott MacDonald | Better Health Programme South Africa (BHPSA) 5
SBCC Strategy for NCD Prevention in South Africa
Acronyms
APEASE Acceptability, practicability, effectiveness, affordability, side-effects
BAC Blood alcohol content
CEA Cost-effectiveness analysis
COVID-19 Coronavirus
CHW Community health worker
DHS Demographic Health Survey
DSD Department of Social Development
DTI Department of Trade and Industry
EBF Exclusive breastfeeding
IPC Interpersonal communication
HIV Human Immunodeficiency Virus
IYCF Infant and young child feeding
GBV Gender based violence
GDP Gross domestic product
LMICs Low-and middle-income countries
M&E Monitoring and evaluation
NCDs Noncommunicable diseases
NDoH National Department of Health
NIPHSA National Institute of Public Health South Africa
NGOs Non-governmental organisations
NSP National Strategic Plan
PLHIV People living with HIV
PW Phuza Wize
SANAC South African National AIDS Council
SBCC Social and behaviour change communication
SEM Socio-ecological model
SMART Smart, measurable, achievable, relevant, time-bound
STIs Sexually transmitted infections
ToC Theory of change
WHO World Health Organization
October 2020Mott MacDonald | Better Health Programme South Africa (BHPSA) 6
SBCC Strategy for NCD Prevention in South Africa
Executive summary
Noncommunicable diseases (NCDs) contribute to a significant burden of disease in South Africa. The
four most common NCDs are cardiovascular diseases, diabetes, cancers and chronic respiratory
diseases1, while mental health conditions are rapidly emerging as a major area of concern. Major risk
factors for the development of NCDs, such as obesity and hypertension, are also rising in South
Africa. This is concerning, as people living with one or a combination of NCDs are at higher risk of
disability and premature death. People living with NCDs, particularly diabetes, are also at higher risk of
severe consequences of COVID-19. At a population level, the social and economic costs of NCDs are
enormous, particularly when combined with the additional burden of communicable diseases, maternal
and child mortality and violence and injuries.
The causes of NCDs are multi-modal and complex, but there are known ways to prevent NCDs. While
biology and genetics influence NCD risk, many of the causes of NCDs are modifiable. These include
the four main behavioural risk factors (tobacco use, harmful alcohol use, physical inactivity and
unhealthy diets) as well as their social and commercial determinants. These determinants range from
the built and food environments to the aggressive marketing tactics of the tobacco, alcohol and food
and beverage industries. The way that all these factors interact is highly contextual and requires the
insights of a broad range of experts and stakeholders.
The government of South Africa, led by the NCD Cluster of the National Department of Health (NDoH),
is finalising a National Strategic Plan (NSP) for NCDs 2020-2025, which focuses on both the
prevention and control aspects of NCDs. A key lesson from the previous NSP for NCDs is that such a
plan needs to be complemented by additional strategies and operational plans that focus on specific
components, in our case NCD prevention. Global lessons from NCD prevention have also emphasised
the importance of strategies being context-specific as well as evidence-based.
This document is not a strategy but rather a formative piece of work that presents the ideal
components and research required for a social and behaviour change communication (SBCC)
strategy to complement those areas of the NSP focused on the primary prevention of NCDs.
The document also considers NCD prevention efforts in South Africa that fall outside of the usual
ambit of government but that fall firmly within the realm of SBCC, such as advocacy to shift structural
and systems barriers to change. We explain and model on how SBCC can focus strategic planning
processes to bring about desired behaviour and social change at scale.
This document provides a basis for the development of a SBCC strategy by addressing four
objectives:
1. To introduce the key components required for any SBCC strategy;
2. To present SBCC-relevant evidence for the primary prevention of NCDs in South Africa
(aligned with the draft NSP and drawing on international and context-specific evidence);
3. To model the process of planning a SBCC strategy specific to the primary prevention of
NCDs in South Africa; and
4. To recommend how to prevent NCDs in South Africa, using key SBCC insights.
1
https://www.gov.za/faq/health-non-communicable-diseases/what-non-communicable-disease
October 2020Mott MacDonald | Better Health Programme South Africa (BHPSA) 7 SBCC Strategy for NCD Prevention in South Africa Methodology The format, scope and content of this document was conceptualised in an inception report and then finalised in consultation with an Advisory Group and additional individual consultations. This document is the result of a desk review of international and South African literature on NCD prevention, complemented by a consultative process with experts from government, research institutions and civil society that spanned four months (July - October 2020), including a review by Public Health England experts. Results The length of this document reflects its dual purpose of 1) introducing key components and tools to support the design, implementation, monitoring and evaluation of any SBCC strategy and 2) presenting evidence that could be specifically used for the design of an SBCC Strategy for NCD prevention in South Africa, with specific examples modelled throughout. For those only interested in one of the above, we suggest reading the document as follows: For those interested in SBCC principles and tools Section 2 synthesises what is known about SBCC best practice. This includes a list of 11 quality standards for SBCC, supplemented by a quality assurance tool that can be used to support planning as well as evaluation of SBCC implementation (Appendix B). The focus of this section is on definition of key concepts and practices that are foundational to SBCC that may not be familiar to people who work outside of the field, e.g., the importance of the socio-ecological model and communication objectives. This section also includes references to practical “How To” guides, tools and checklists (see Appendix C) that can be used by individuals tasked with strategic planning and/or implementation of SBCC. Those wanting additional examples and explanations of SBCC best practice should refer to Section 5, which models SBCC best practices using NCD prevention evidence. The section focuses particularly on the linkages between audience insights, communication objectives, and design considerations, such as approach, channel and messaging, building on the evidence base presented in Section 3. Section 6 provides an overview of monitoring and evaluation (M&E) specific to SBCC. While some aspects of M&E may seem familiar to any programme planners, such as the M&E planning cycle, other elements are more distinctive. This includes how theories of change (ToCs) are applied to SBCC as well as the inclusion of communication objectives and associated indicators, which are often omitted in programme planning. This section provides examples both in the text as well as through modelling an example ToC (Appendix E) and Performance Framework (Appendix F). For those interested in applying NCD prevention evidence to SBCC Section 3 presents the global and local evidence for the importance of investing in NCD prevention in addition to NCD control and management, with an emphasis on the four key behavioural risk factors and their multi-level determinants, which range from an individual’s motivation to industry interference in the policy making process. The section highlights global NCD prevention “best buys”, successful international campaigns and local campaigns from which we can learn lessons for each risk factor. The section ends with common challenges to NCD prevention and possible solutions for the South African context. Section 5 then applies the evidence from Section 3 to model key steps in SBCC planning for the four behavioural risk factors, specific to South Africa. We intentionally select target audiences and communication objectives at different levels of the socio-ecological model, to emphasise how important it is to think beyond individual and interpersonal communication with the people who we October 2020
Mott MacDonald | Better Health Programme South Africa (BHPSA) 8
SBCC Strategy for NCD Prevention in South Africa
want to change, based on evidence. This section illustrates how embracing the complexity of contexts
can result in more robust and evidence-based strategies.
Section 6, while covering general M&E principles, also provides concrete suggestions of data sources
for NCD-relevant indicators and models the ToC and Performance Framework in Appendices E and F.
Limitations
The NSP for NCDs 2021-26 was not finalised during the period of consultation, and therefore
alignment considerations are based on a May draft of the NSP. As such, rather than present a final
SBCC strategy for NCD prevention, this document was redesigned to focus on the process of
designing a SBCC strategy, which should happen after the NSP has been finalised. While efforts were
made to make the consultation process inclusive of multiple stakeholders, given time limitations and
limited availability of key actors, key perspectives may have been missed. On a related note, most
consultations were conducted on an individual basis, via email or remote calls, as face-to-face
meetings were not possible during the drafting of this report due to COVID-19 considerations. In other
circumstances, a consultative workshop where a larger number of people were brought together to
discuss the document may have expedited the process and enabled more robust dialogue.
Summary of Recommendations
In addition to providing an overview of key SBCC components and characterising the evidence-base
for NCD prevention globally and in South Africa in Section s 2-6, this document highlights several key
recommendations for the design, implementation, and monitoring and evaluation of a SBCC strategy.
KEY RECOMMENDATIONS
1. Develop an SBCC strategy that supports the NSP and commit to an established SBCC planning
process with the appointment of dedicated person/s to oversee the process.
The following should be considered in the planning of the SBCC strategy:
2. Clarify the SBCC strategy planning process up front.
ü Identify key deliverables and ensure all key deliverables are pre-defined across the process.
ü Promote gender equity and social inclusion from the onset of the planning.
ü Apply a life course perspective to audience selection to reach people ideally prior to the
formation of harmful habits.
3. Clarify roles of the various stakeholders in the design phase. The four key roles to be identified in
the planning, implementation and evaluation of the strategy are:
ü Coordination and Planning: Multisectoral work requires a coordination body. (Details are
outlined in the final section, including strengths and weaknesses).
ü Mobilise resources and provide a dedicated budget for the SBCC strategy. Joint budgeting
and delegated budgets for NCD prevention are needed.
ü Cost the implementation of the SBCC strategy: A costed workplan is needed to support the
implementation and a monitoring and evaluation framework aligned to the communication
objectives is a prerequisite for effective implementation of the strategy.
ü Facilitate research and evaluation: Provisions for formative research, pre-testing of SBCC
materials and the evaluation of the interventions need to be included in the budget.
4. Prioritise communication objectives (and audiences) based on evidence.
The decision about which audiences are most important to target with SBCC requires a transparent
prioritisation process based on analysis of context-relevant information.
October 2020Mott MacDonald | Better Health Programme South Africa (BHPSA) 9
SBCC Strategy for NCD Prevention in South Africa
5. Align SBCC approaches with communication objectives.
A mix of multi-level approaches is the benchmark for optimal outcomes, although some changes may
be achieved with less complex approaches.
6. Plan for disruption to mitigate its impact.
Disruptions can push programmes or campaigns to change dramatically. Risk communication
strategies and systems are needed to mitigate the impact of unforeseen events.
7. Use this document for guidance and direction in the development of the SBCC strategy for NCD
prevention.
Draw on some or all of the tools, evidence or specific recommendations to forward the agenda of NCD
prevention in South Africa. Given the variety of people who may draw on this document, we highlight
areas where critical information can be quickly accessed by various actors:
• Campaign implementers (government or civil society) can use Section 2 and the quality
assurance checklist (Appendix B) to determine how well their current or past campaigns align to
key SBCC components. Section 2 also provides several additional references and tools (see
Appendix C) to guide the actual planning and design process. Implementers may also find
Section 6 and its appendices useful in the design of M&E plans.
• Government, particularly NDoH, may draw on all or parts of this document as the basis for a
National SBCC strategy for NCD prevention and a costed operational plan to support the NSP.
Section 4 is dedicated entirely to NSP alignment considerations.
• Non-governmental organisations (NGOs) and civil society actors involved in NCD
prevention communication can draw on the analysis and recommendations in Section s 2, 3, and
5-7, at whatever level is within their means and scope for implementation, e.g., related to alcohol,
tobacco, diet or physical activity. The social mobilisation and advocacy approaches may be of
particular interest.
• Research institutions and universities may be interested in the M&E framework and proposed
indicators for current or future studies that would contribute to NCD prevention, found in Section
6 and Appendices E and F. The evidence presented in Section s 3 and 5 may also be of interest
to subject experts.
Concluding Remarks
The evidence is clear: NCD prevention cannot only focus on individuals at risk. This document
highlights the social determinants of NCDs, including gross income inequality, gender inequities and
racial disparities, which need to be addressed. In addition, this document underlines how commercial
determinants of (ill) health are costing society. The alcohol, tobacco, food and beverage industries
have far greater resources at their disposal to interfere in NCD prevention than government and NGOs
have to promote well-being. If we do not use SBCC strategies to proactively address industry influence
at the policymaking table or through their marketing, NCD prevention efforts will falter.
On a more positive note, the COVID-19 pandemic has refocused attention on the importance of NCDs
at an opportune time, when the new NSP for NCDs is being finalised. Through the process of
compiling this document, a wealth of experience and expertise was identified, both in the literature as
well as among those we consulted. South Africa is fortunate to have a large community of SBCC and
NCD experts who are eager not only to share ideas, but also to act. We are also fortunate to have a
government that recognises the importance of multi-sectoral action and public health approaches. It is
our hope that such individuals and institutions can draw on this collective work to support better health
and well-being for all South Africans.
October 2020Mott MacDonald | Better Health Programme South Africa (BHPSA) 10
SBCC Strategy for NCD Prevention in South Africa
1 Background
Noncommunicable diseases (NCDs) contribute to a significant burden of disease in South Africa. The
four most common NCDs are cardiovascular diseases, diabetes, cancers and chronic respiratory
diseases2, while mental health conditions are rapidly emerging as a major area of concern. Major risk
factors for the development of NCDs, such as obesity and hypertension, are also rising in South
Africa. This is concerning, as people living with one or a combination of NCDs are at higher risk of
disability and premature death. People living with NCDs, particularly diabetes, are also at higher risk of
severe consequences of COVID-19. At a population level, the social and economic costs of NCDs are
enormous, particularly when combined with the additional burden of communicable diseases, maternal
and child mortality, and violence and injuries.
In addressing the chronic diseases of lifestyles and the growing burden of NCDs, the National
Department of Health (NDoH) is in the process of finalising the National Strategic Plan (herein, NSP)
for Noncommunicable Diseases (NCDs) for 2021-2026. One of the recommendations from the 2018
review of the previous Strategic Plan for the Prevention and Control of NCDs 2013-17 was that a
broad-reaching NSP should be complemented by specific policies and plans focusing on different
areas proposed in the National Strategic Plan, in this case prevention.
COVID-19 has further focused the country’s attention on the importance of NCDs. People living with
one or more of the four main NCDs experience a higher risk of contracting and developing more
severe forms of the virus (Young et al, 2020). People living with NCDs, including those with mental
health conditions, also experienced significant disruptions to routine services (WHO, 2020a and
2020b). This focused attention on the urgent need for the new NSP to both prevent NCDs as well as
support those living with NCDs, with the control and management of their conditions.
From a NCD prevention perspective, the national state of disaster in response to COVID-19 led to
temporary restrictions in alcohol and tobacco sales that have previously been untested in South Africa,
creating a natural experiment for how restrictions impact on consumption patterns. Similarly, reduced
economic activity, road and air traffic in countries with strict lockdowns led to improved air quality.
While the longer-term impacts of these restrictions remain to be seen, these experiences have led to
calls for a “new normal” that prevents a return to harmful norms. Such calls have not focussed
exclusively on the restructuring of health systems, such as proposed by the National Health Insurance
(NHI) bill. Ideally the “new normal” should redirect attention and resources to health promotion and
disease prevention, following a whole of government approach to supporting the nation’s well-being.
This document is not a strategy but a formative piece of work that presents the ideal components and
research required for a social and behaviour change communication (SBCC) strategy to complement
those areas of the NSP focused on the primary prevention of NCDs as well as other NCD prevention
efforts in South Africa. We explain and model on how SBCC can focus strategic planning processes to
bring about desired behaviour and social change.
Our focus is on primary or primordial prevention, preventing NCDs before they occur in the first place.
This is guided by the large number of conditions that fall under NCDs and the complex prevention
pathways that exist. This is not to diminish the value or importance of conducting similar SBCC
planning exercises that focus on other aspects of the NSP, particularly in relation to people already
living with NCDs and the control and management of conditions. However, in terms of scope,
prevention was sufficient in and of itself.
2
https://www.gov.za/faq/health-non-communicable-diseases/what-non-communicable-disease
October 2020Mott MacDonald | Better Health Programme South Africa (BHPSA) 11
SBCC Strategy for NCD Prevention in South Africa
1.1. Purpose
The purpose of this document is to provide a basis for the development of a SBCC strategy. This is
done by addressing the following four objectives:
• To introduce the key components required for any SBCC strategy;
• To present SBCC-relevant evidence for the primary prevention of NCDs in South Africa
(aligned with the draft NSP and drawing on international and context-specific evidence);
• To model the process of planning a SBCC strategy specific to the primary prevention of NCDs
in South Africa; and
• To recommend how to prevent NCDs in South Africa, using key SBCC insights.
Further analysis would be required to complete the NCD prevention SBCC strategy and to include
other secondary prevention and NCD control measures highlighted in the NSP for NCDs. Suggestions
on how this could be addressed are included in the recommendations.
1.2. The importance of an SBCC strategy in NCD prevention
An SBCC strategy acts as a bridge between a national or programmatic strategy and specific SBCC
campaigns. SBCC strategies present the underlying logic of campaigns and guide their planning
processes. They support the design, implementation and evaluation of practical and strategic
communication activities. Most often SBCC strategies focus on a single condition, e.g., HIV or
obesity, as opposed to an entire cluster of conditions like NCDs. This is rightfully so because the
specificity of evidence required for effective SBCC campaigns is high.
An SBCC strategy always includes a situational analysis, audience identification and segmentation,
communication objectives and recommendations for evidence-based approaches and channels that
focus on meeting strategic or programme goals and objectives. SBCC strategies often supplement
and align with national plans and include their own work plans and M&E plans to support action.
The South African government has adopted the language of SBCC in several national strategies,
most notably the National Strategic Plan for HIV, TB and STIs: 2017-2022 (SANAC, 2017). The
South African National AIDS Council (SANAC) and the Department of Social Development (DSD)
have developed several campaigns aligned to this strategy, which are framed as SBCC campaigns.
However, evaluations of some of these campaigns suggest that they may not have an SBCC-specific
strategy and M&E framework (Khosa, Dube & Nkomo, 2017). While it is possible to have
communication campaigns without an SBCC strategy, planners are likely to miss core components in
the planning process, which may mitigate effectiveness. The core components of SBCC are
described in Section 2.
1.3. Process undertaken in the development of this document
The development of this document involved a phased consultative process with key stakeholders led
by a team of three independent consultants with SBCC expertise. This happened in phases.
An inception report was developed, and the format, scope and content of the strategy was then
finalised in consultation with an Advisory Group and additional individual consultations. This was used
to compile a first full draft. This draft was shared with a broader range of stakeholders for feedback
and finalisation.
The resulting document is a synthesis of a desk review of international and South African literature
and best practice, consultation with the Advisory Group comprised of representatives from government
and civil society as well as consultations with multiple expert stakeholders (see Appendix A).
October 2020Mott MacDonald | Better Health Programme South Africa (BHPSA) 12 SBCC Strategy for NCD Prevention in South Africa 1.4. Intended use of this document This document is intended for programme designers, implementers, technical working groups and others who are using health communication to prevent NCDs in South Africa. This includes a wide range of stakeholders such as, but not limited to, those working for NDoH, NGOs, civil society, researchers and the private sector. The types of people who may find this useful are those involved in strategy, health communication, health promotion and/or monitoring and evaluation. Practical suggestions for coordination, implementation and research are discussed at the end of the document. This formative document was designed to align with and feed into the primary prevention components of the latest NSP on NCDs. As such, government actors in the NCD cluster and related sectors will find practical ideas to achieve targets set out in the NSP. This strategy could be the basis for a national SBCC strategy for NCD prevention that could be refined into a costed operational plan. The analysis and recommendations are also relevant to NGOs and civil society actors who are involved in NCD prevention communication; evidence and recommendations within this strategy can be taken forward at whatever level is within their means and scope. Similarly, research institutions and universities may take an interest in the M&E framework and proposed indicators for current or future studies that would contribute to NCD prevention. October 2020
Mott MacDonald | Better Health Programme South Africa (BHPSA) 13
SBCC Strategy for NCD Prevention in South Africa
2. KEY COMPONENTS OF AN EFFECTIVE
SBCC STRATEGY
2.1. Summary of SBCC quality standards
Upon evaluation, a high quality SBCC programme or campaign should be able to demonstrate that it
adhered to the following standards:
1. Followed a planned process.
2. Drew on context-relevant evidence.
3. Was grounded in theory, from inquiry until evaluation.
4. Applied audience insight and segmentation.
5. Had clearly defined communication objectives, aligned to programme objectives.
6. Used a mix of strategic approaches aligned to communication objectives.
7. Modelled participatory approaches.
8. Supported multisectoral action.
9. Promoted gender equity and social inclusion.
10. Avoided stigmatising people or conditions.
11. Reflected a life-course perspective.
These standards are described in greater detail in this section. They also have been developed into a
quality assurance tool that can be used to support planning of new campaigns as well as to measure
the institutional systems context and implementation fidelity of specific campaigns that have already
been conducted (see Appendix B).
2.2. Planned process
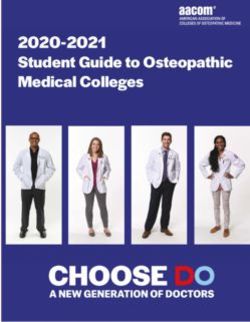
SBCC is a process that draws on planning frameworks. The P-PROCESS is most closely associated
with SBCC (see Figure 1), although other planning frameworks can be used. What is common across
planning frameworks are the following phases, which are sequential:
1. Inquiry to understand the situation and the people you will
be working with, often referred to as audiences. This
culminates with a clear problem statement.
2. Design, where audiences and targets of change are
prioritised based on evidence to develop a SBCC strategy.
Key criteria, e.g., APEASE (acceptability, practicability,
effectiveness, affordability, side-effects) can be used to
assess intervention ideas at this stage (see Appendix C).
3. Create and test any communication products or processes
proposed in the strategy to ensure they are appropriate.
4. Implementation and monitoring of the final strategy.
5. Evaluation, which often leads to adaptations or re-planning
for the next programme cycle based on results.
Cross-cutting components of SBCC planning frameworks are
the integration of theory, community/stakeholder/audience
participation and capacity strengthening, which are addressed
separately.
Figure 1. P-PROCESSTM
October 2020Mott MacDonald | Better Health Programme South Africa (BHPSA) 14
SBCC Strategy for NCD Prevention in South Africa
2.3. Grounded in evidence and context
The planning process requires us to draw on different types of evidence to focus an SBCC strategy on
the context in which it will be implemented during the inquiry step. An SBCC strategy that works in one
place or community may not work in another, which is why context matters.
Table 1. Types of SBCC evidence and potential data sources
Evidence type Definition in the context of NCDs Potential sources
Social This evidence tells us about the hopes and Quality of life surveys, qualitative
aspirations of at-risk communities, such as desired research, journal articles
body size, what is considered attractive, dietary
patterns, etc.
Epidemiological Burden of disease data, including how NCDs are Demographic Health Survey
distributed geographically and among different (DHS), WHO reports
population groups to help us identify those at
highest risk.
Environmental Structural and policy factors that may either Policy reviews, journal articles,
facilitate or inhibit NCD prevention. This includes media use surveys
looking at the communication landscape.
Behavioural Data on behaviours linked to NCD risk, e.g., National surveys (DHS, National
tobacco use, or NCD prevention, e.g., physical Health and Nutrition Examination
activity. This type of information is richest when it Survey, etc.); journal articles
explains factors associated with behaviours, e.g.,
gender, age, economic factors, beliefs, etc.
Interventions Process, outcome, or impact evaluations of WHO Best Buys, systematic
interventions. A subset of intervention research reviews, journal articles
measures cost efficiency, which is important for
decision makers.
In the design step, these different sources of information are synthesised and interpreted to make
strategic decisions based on a) what would be most impactful and b) what is modifiable (changeable)
in the timeframe and context. Particularly for social evidence, it is important to engage meaningfully
with the communities or “audiences” we hope will respond to and benefit from our interventions.
The process of setting priorities in SBCC planning occurs at several phases. Firstly, evidence should
be used to determine which behavioural changes, e.g., healthier diets vs. tobacco reduction, would
have the greatest impact on the desired outcome, in this case reducing NCDs. At this point,
implementers may also want to weigh the benefits of approaches that consider the whole individual,
allowing them to decide on NCD prevention priorities (see for example https://oneyou-
hay.service.nhs.uk/oneyou/how-are-you/) vs. selecting a single issue on which to focus. Once
determined, evidence should be used to identify what facilitators or barriers to the behaviour(s) would
likely bring about the most significant change if extended (for facilitators) or reduced (for barriers). This
evidence is often derived by looking at evaluations of prior interventions but may also draw on theory
(described in 2.4). The selection of audiences is closely related, depending on an analysis of who has
the greatest power or agency to extend the facilitator or remove the barrier (described in 2.5). The
actual prioritisation of communication objectives puts this information together with far more attention
to the actual quantum of change that can be expected (described in 2.6). Again, this relies on baseline
evidence as well as evidence of past interventions. Finally, the identification and selection of
approaches combines insights into theory as well as past intervention evidence. As described in 2.7,
this can be done following a process called Intervention Mapping (Bartholomew et al, 2011), which
embraces all levels of the socio-ecological model (see 2.4). There are also practical tools, such as the
Behaviour Change Wheel, that have been developed to simplify this complex process, albeit with more
October 2020Mott MacDonald | Better Health Programme South Africa (BHPSA) 15
SBCC Strategy for NCD Prevention in South Africa
of a focus on the individual and interpersonal levels (Michie et al, 2011). The selection and
prioritisation of channels and message design draws on specific audience insights as well as practical
considerations in terms of budget and human resources.
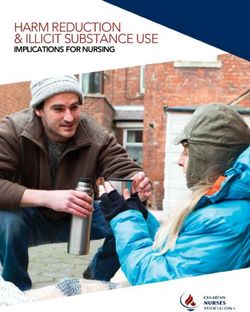
2.4. Grounded in theory
SBCC uses a socio-ecological model (SEM,
see Figure 2) to analyse the situation and
community members to identify barriers and
facilitators to change at the inquiry phase,
through formative research that may include
both desk reviews and primary research, as
described in Section 2.3. The SEM
illustrates how social and structural
environments influence individuals and the
decisions they make. The political and
economic environments of a society
influence community dynamics and vice
versa.
The findings of this multi-level analysis are
also used to support decision -making on
priorities and which approaches to use
during the design phase, which will be
described further under Strategic Approaches (2.7).
Figure 2. Adapted SEM for Change for SBCC
The SEM is flexible in that it supports the use of constructs from other social and behavioural theories
to explain or predict how change is expected to happen. These can be used as entire theories, such
as the Theory of Planned Behaviour, or constructs from different theories can be combined to support
an SBCC strategy in what is called a theory of change. The reason that SBCC campaigns often use a
combination of theories and constructs, as opposed to the use of a single theory, is that many
behavioural theories and those based on behavioural economics concentrate on change dynamics at
the individual level only. They oversimplify complex change processes, missing key conceptual
barriers to, or facilitators of, change that may exist at interpersonal, community or societal levels. This
is supported by evidence of “what works” that point to the strength of multi-level interventions that
draw on more complex theories of change aligned to the SEM (see also Alive & Thrive example in
3.3.3.).
The SEM, as the theoretical framework for SBCC, shows how barriers to real and sustained change
are often beyond the individual. The commercial determinants of health, defined as ‘factors that
influence health which stem from the profit motive’ of industries such as tobacco, alcohol, sugar-
sweetened beverages and highly processed foods, operate at both community and societal levels
(Kickbusch, Allen & Franz, 2016). At community level, they manifest in the marketing of products
whereas at the societal level commercial determinants influence trade agreements and regulation
debates. The SEM illustrates that if we only focus on changing individual behaviour, without
accounting for their home, community, social and commercial environments, we can expend huge
financial and human resources, without achieving change.
In Box 1, we illustrate how the SEM can be applied to physical activity for adolescent girls in South
Africa. The reason for doing this is to explain why most, if not all, SBCC campaigns address a variety
of stakeholders from different levels of the model. SEM is very useful as a framework during the
inquiry stage.
October 2020Mott MacDonald | Better Health Programme South Africa (BHPSA) 16 SBCC Strategy for NCD Prevention in South Africa However, as mentioned above, more detailed theories of change (ToC) are often developed as part of the design stage. The ToC draws on meaningful constructs (ideas) to explain how change is supposed to happen to achieve a specific objective. This is described further and modelled in Section 6. Box 1. Socio-ecological model of physical activity for adolescent girls in South Africa In this example, adolescent girls are at the centre of the SEM (Self). Individual factors, such as their knowledge about physical activity, motivation to be active and perceptions about what others think about physical activity would all be important influences. Other internal factors, like self-esteem, may also impact on an adolescent girl’s motivation to be physically active. The interpersonal environment would most likely be comprised of family members and peers, who would either reinforce or challenge girls’ ideas about physical activity. For instance, an adolescent girl may want to participate in sports, but her peers may tease her. Her parents may discourage her to exercise if they live in an area where they fear for her safety, or they may expect her to participate in household chores (whereas her adolescent brother may be allowed to participate in sports). At the community level, leaders determine access to acceptable and safe spaces for physical activity, which influences both adolescents and their interpersonal environment. While the adolescents may never interact directly with these community leaders, such leaders indirectly influence their physical activity behaviours. Similarly, the institutional level decisions of whether schools promote and provide sports for females influences access. In SBCC we recognise that these leaders are influenced by their own sets of beliefs, norms and motivations, which is why these factors are shown as being cross-cutting in Figure 2. Factors like policies and legislation, religious or social norms, and the natural environment are located at the outermost level. Things like climate, may need to be accounted for without being able to change the factor itself. For example, people living in a hot climate may need to schedule outdoor activities in the morning or early evening. Other factors are more modifiable and linked to individuals. For example, the Department of Basic Education can require all government schools to offer the same number of sports for both boys and girls, to address gender equity. The levels (Self, Interpersonal, Community and Societal) interact dynamically with one another. If a policy changes at the outermost level, it is likely to have a ripple effect. Likewise, if parent or peer attitudes shift to become more supportive, this may lead to a shift both for individual adolescents as well as among the leaders of their community institutions, e.g., schools. 2.5. Audience specific In SBCC, the term audience is used to describe the person or people for whom (and ideally with whom - see 2.8) an intervention is designed. While the term audience often connotes a passive group of people receiving a message, as you will read later, a much more dynamic and horizontal form of communication is preferred in SBCC, which recognises people’s agency. That said, there are several important types of audiences when it comes to terminology. Primary audience: These are the people we ultimately want to benefit from our efforts. At the programme level, we will measure whether their behaviours have changed and/or the health outcome has been achieved. If adolescent girls are our primary audience, we would want to know if their physical activity levels increased in the medium term and, ultimately, if fewer developed NCDs linked to physical inactivity as a longer-term impact (often measured over several years). Influencing audiences: These are the people who directly (a.k.a secondary) or indirectly (a.k.a. tertiary) influence the primary audience. A secondary audience for adolescent girls may be their peers or caregivers, while the Minister of Basic Education may be a tertiary audience. Many SBCC strategies only refer to these groups collectively as influencing audiences. October 2020
Mott MacDonald | Better Health Programme South Africa (BHPSA) 17
SBCC Strategy for NCD Prevention in South Africa
Target audiences: These are the person or people to whom specific communication strategies are
directed. They could be the primary audience, e.g., adolescent girls, or influencing audiences, e.g., the
Minister of Basic Education or adolescent caregivers.
Audience segmentation is another practice followed in SBCC. Once a target audience is identified,
e.g., adolescent girls, a more detailed breakdown is required to ensure that the right people are
addressed. Each segment needs to be mutually exclusive and meaningful for the change being
sought. While some campaigns may seek to address all segments of an audience with communication
tailored to their needs or interests, resource constraints often require planners to prioritise only a few
audience segments for a concentrated campaign.
The diagram below provides an example of how segmenting adolescent girls for a physical activity
SBCC strategy could help planners identify who should be prioritised. In this case, we would break
down adolescent girls by their physical environment (rural/urban), current physical activity levels and
motivation to change for those who are inactive. Physically inactive, but motivated adolescent girls
would be the primary target audience, with those who are inactive and unmotivated as a second target
(resources allowing).
Rural Adolescents Girls Urban Adolescent Girls
Physically Active Physically Inactive Physically Physically Inactive
Active
Motivated Motivated
Unmotivated Unmotivated
This above breakdown is fairly simplistic. Ideally, segmentation should also consider factors linked to
the psychographic parameters of the audiences, such as their beliefs, aspirations and needs. There
are step-by-step guides on how to make audience segmentation decisions, such as the one found in
the link: https://www.thecompassforsbc.org/how-to-guides/how-do-audience-segmentation. (NB: This
particular guide includes a checklist for ensuring that your segments are meaningful.)
When thinking about audiences, it is important to consider questions of equity. If particular socio-
economic groups, race groups, genders, or people living in particular regions (for example) experience
an unfair burden of disease, these are potential starting points for segmentation. This would ensure
that systematically disadvantaged populations are given priority in terms of attention and resources to
reduce health inequities.
2.6. Clear SBCC objectives
Communication objectives are vital components to inform the development of effective campaigns and
interventions. SBCC uses communication objectives to support programme objectives and focus on
SBCC-specific strategies. While programme objectives focus on changing behaviours or policies,
communication objectives focus underlying factors that explain why the change has not already
occurred. Decreasing barriers or increasing facilitators are the focus of communication objectives.
For example, if the programme objective is ‘to increase physical activity by 50% among adolescent
girls by 2025’, the communication objective would focus on either a barrier or facilitator to physical
activity within that target audience: ‘To increase self-efficacy to participate in school sport to 75% of
adolescent girls by 2025’.
October 2020Mott MacDonald | Better Health Programme South Africa (BHPSA) 18
SBCC Strategy for NCD Prevention in South Africa
Communications objectives are based on research on key sub-populations affected by NCDs and the
NCD-related risky health behaviours, as discussed under audiences. Information on their unique
barriers and facilitators to change, such as: knowledge and motivation levels, and ability to act along
with normative and structural factors, is vital to effective messaging and programming to promote
healthy behaviours. While there is existing literature and data on some factors that influence
behaviour, a gap assessment in the early stages of planning identifies what information is accessible
and what formative data needs to be collected.
Making your Objectives Count
Both programme and communication objectives should meet SMART criteria to enable targeted
communication and measurement. The SMART acronym stands for:
Specific Measurable Achievable Relevant Timebound
A generic formula for a SMART objective that can be adapted to different needs is as follows:
For objectives targeting individuals: behaviours (including policy enforcement); attitudes;
knowledge; etc.
To [increase/decrease] by [amount: # or %] the [target] of [population/audience] by [time change will
be assessed] (e.g., to increase to 40% the level of participation in school sports of adolescent girls
(aged 16-19) in South African rural settings by 2025).
For objectives targeting structural or policy change: laws, funding, new institutions, etc.
For [audience/person] to [constitute/fund/approve/pass] [target: institution/policy/legislation name]
within [specific setting/government structure] by [target date to complete] (e.g. for the Department of
Basic Education to legislate that all public secondary schools provide equal sports opportunities for
male and female learners by 2021)
Both examples above are programme-level objectives, as they focus on changing behaviour and
policy. Examples of communication objectives are presented in Section 5.
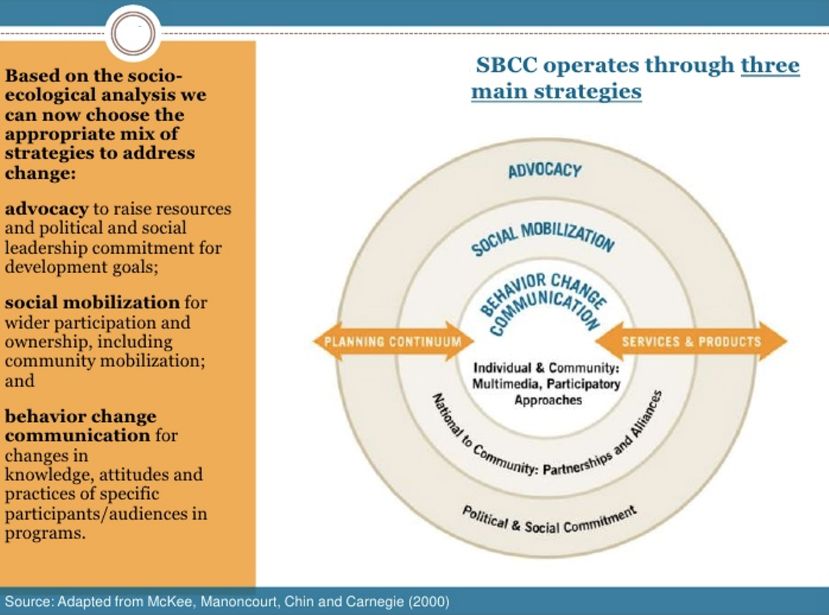
2.7. Strategic approaches
Based on the audiences and change sought
in the communication objectives, one or
more strategic approach shown in Figure 3
should be selected to promote change.
These need to be described in detail within
the SBCC Strategy. Strategic approaches
should specify activities and potential
channels appropriate for the audience and
context. A channel is the medium through
which communication takes place. It can be
unidirectional, e.g., TV, or enable dialogue,
such as a training or interpersonal
communication.
While strategic approaches should be
aligned with communication objectives,
sometimes one approach, e.g., mass media,
can address multiple communication
objectives.
Figure 3. SBCC strategic approaches
October 2020Mott MacDonald | Better Health Programme South Africa (BHPSA) 19 SBCC Strategy for NCD Prevention in South Africa The three strategic approaches shown in Figure 3 are derived from the work of McKee and colleagues (2000 and 2014) over the past several decades as one way to differentiate intervention types by SEM levels. However, as will be discussed in Section 5.3, the range of approach options within any of these concentric circles is broad and ever-expanding. Tools to support prioritisation are also presented in that section. 2.8. Participatory and multisectoral The meaningful participation of affected communities and other key stakeholders/audiences is critical throughout the SBCC planning process. A shared vision of where you want to go (compared with where you are now) facilitates success. A key SBCC insight is that ‘in developing your shared vision, the “shared” is more important than the vision itself.’ (C-CHANGE, 2012) Participation means engaging stakeholders from the outset and pre-testing any products or processes with the intended audiences before implementation. The concept of participation is closely aligned with the idea of multisectoral action. For example, the implementation of the NSP for NCDs requires the buy-in and support of multiple sectors, not only NDoH. In a study of the key barriers to multisectoral action to prevent NCDs in South Africa and four other African nations, lack of awareness by various sectors about their potential contribution, weak political will, coordination complexity and inadequate resources were identified (Juma et al, 2018). 2.9. Gender equity Gender equity underpins SBCC and the development of this document. Unlike biological sex, gender is a construct that varies by context and changes over time. Many gender related norms, expectations and beliefs prevent people from accessing services and achieving wellness. This may manifest as an adolescent girl who is told by her parents that she cannot participate in afterschool sports because she has chores (unlike her adolescent brother), an adolescent girl who avoids sports because they are not considered “feminine” or a transgendered girl who avoids sports for fear of stigma or discrimination. SBCC strategies require the critical examination of gender norms that negatively impact health outcomes as well as those that may positively influence change. At a minimum, SBCC strategies should be gender sensitive and never gender exploitative (where harmful gender norms are reinforced). Gender transformative approaches are preferable, whereby harmful norms are directly challenged. Gender needs to be included from the very first step of the planning process with an effort to disaggregate and analyse data by gender. However, mainstreaming gender also requires that the planning process itself is inclusive. For example, planning meetings should be scheduled at times that enable both men and women to participate equally and leadership bodies should encourage gender parity. 2.10. Social inclusion and stigma prevention An SBCC strategy also needs to prevent social exclusion. Collins (2004, p.727) defines social exclusion as a process that ‘can be described more comprehensively as a lack of access to four basic social systems: democracy, welfare, the labour market, and the family and community,’ with the idea that the exclusion is often outside of the individual’s control. Repper and Perkins (2003) argue that social inclusion requires equality of opportunity and participation in the rudimentary and fundamental functions of society. Examples of these functions include access to health care, employment, education, and good housing. Ways that social inclusion can be promoted, particularly through participatory processes, are integrated into the recommendations. This document models how to focus on populations that are often excluded, for economic or social reasons as well as disability. October 2020
Mott MacDonald | Better Health Programme South Africa (BHPSA) 20
SBCC Strategy for NCD Prevention in South Africa
Social inclusion should include special consideration of people living with disabilities, who may be
overlooked particularly around ableist framings of NCD prevention areas, such as physical activity.
Closely related to social inclusion is the prevention of stigma. The unintended consequences of many
public health communication campaigns have been the stigmatisation of people who look like or have
the condition that messaging is trying to prevent. For example, early fear-based campaigns about HIV,
depicting people living with HIV (PLHIV) as being sickly or having engaged in stigmatised behaviour,
led to discrimination and social exclusion of PLHIV. Similar risks are possible in NCD prevention, with
the stigmatisation of people who are overweight and obese, for instance. This “fat shaming” or “body
shaming” is counterproductive to long-term prevention efforts.
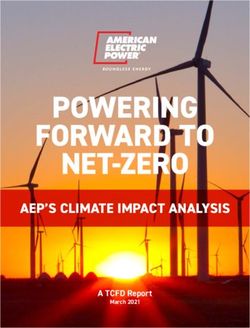
2.11. Life course approach
While not always included in SBCC strategies, there is a
growing recognition that what happens in early life has an
impact in later life. According to estimates by WHO, 70%
of premature deaths that occur in adulthood globally are
due to behaviours that began in adolescence (WHO,
2009).
For this reason, it is important to consider when we
engage with people to bring about change. For NCD
prevention, this requires us to decide when in the life
course we are likely to have the biggest impact. For
example, promoting activity from an early age may set
lifelong habits, exclusively breastfeeding an infant can
reduce NCD risks, and prevention of alcohol or tobacco
use during adolescence vs. after a person has started
experimenting, can have a greater impact.
Figure 4 uses evidence to demonstrate how a life course approach can be used to identify audiences
as well as behavioural targets that are likely to have a significant impact on NCDs.
Figure 4. A circular display of the life course and examples of key priorities at various stages
(Source: Aagaard-Hansen et al, 2019)
October 2020You can also read