Benefits 2023 Guide - Full-time & Permanent Part-time ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Employee
Benefits
2023 Guide
Full‑Time &
Permanent Part-Time Employees
Employee
Benefits Guide 2023
FULL‑TIME & PERMANENT PART-TIME EMPLOYEES
General Information
1. Employee Benefits Package Overview 12. Introduction
2. Contact Information 13. Eligibility
5. 2023 Payroll Processing and Holiday Calendar 14. Enrollment
6. 2023 Holiday Schedule 15. Changes in Coverage
7. Rates: Full‑Time Employees 16. 2023 Summary of Benefits and Coverage Notice
10. Rates: Permanent Part-Time Employees
Core Benefits
17. Medical – CalPERS 26. DeltaCare USA
18. 2023 CalPERS – EPO & HMO Basic Plans 26. Dental PPO
21. 2023 CalPERS – PPO Basic Plans 28. Vision
25. Dental
Other Benefits
29. Group Life and AD&D/Supplemental Life 33. Deferred Compensation
29. Disability 33. Retirement
32. Navia Benefits Card 33. Unemployment Insurance
32. Transit/Parking Commuter Benefits Program 34. Guaranteed Ride Home (GRH)
32. Dependent Care Assistance Program
Miscellaneous
35. Important Notices 46. Glossary
NEW! Click this icon in your benefits guide to watch a video explaining the associated topic.
NEW! See page 46 for a glossary of terms.
If you (and/or your dependents) have Medicare or you will become eligible for Medicare
in the next 12 months, a Federal law gives you more choices about your prescription drug coverage.
Please see page 39 for more details.
The information in this brochure is a general outline of the benefits offered under the City of Oakland’s benefits program. Specific details and plan
limitations are provided in the Summary Plan Descriptions (SPD), which is based on the official Plan Documents that may include policies, contracts and
plan procedures. The SPD and Plan Documents contain all the specific provisions of the plans. In the event that the information in this brochure differs
from the Plan Documents, the Plan Documents will prevail.
City of Oakland | Full-Time and Permanent Part-Time Employees i
Employee Benefits Package Overview
• CalPERS Medical • Group & Supplemental Life
Insurance
• Dental
• Employee Assistance
• Vision Program (EAP)
• Medical Waiver Plan – Cash-In-Lieu • Guaranteed Ride Home (GRH)
• Flexible Spending Accounts • Pension Benefits
• Commuter Benefits • Deferred Compensation
City of Oakland | Full-Time and Permanent Part-Time Employees 1
Contact Information
Benefits Contacts
You may contact the below benefit carriers or visit the following websites to confirm eligibility and verify coverage:
Employee
Benefits Staff Contact Information
Benefits Program
510.238.6891
Benefits Supervisor Tami Honda
thonda@oaklandca.gov
Benefits Enrollment Questions
New Hire Benefit Enrollment Benefits Unit BenefitsAdmin@oaklandca.gov
General Benefit Questions
510.238.7446
Denise Carter
dcarter@oaklandca.gov
COBRA
Administrator: Navia 877.920.9675
Benefits Solutions cobra@naviabenefits.com
Michael McGhee:
510.238.6485
Mission Square/ICMA-RC
mmcghee@missionsq.org
(Investment Option Inquiry Only)
Deferred Compensation
510.238.7445
Jeanette Delgado
jdelgado@oaklandca.gov
Benefits Unit Benefitsadmin@oaklandca.gov
• Medical Lisa Lavatai
510.238.6769
• Dental All city departments
llavatai@oaklandca.gov
• Vision EXCEPT Police & Fire
• Flexible Spending Accounts (Health Care Adrienne Cooper
FSA and Dependent Care FSA) 510.238.6474
Police & Fire staff (Sworn
• Commuter Benefits acooper2@oaklandca.gov
and Non Sworn)
Other Benefits
510.238.7446
• Life Insurance (Non-Sworn) The Hartford Denise Carter
dcarter@oaklandca.gov
510.238.6891
Guaranteed Ride Home Tami Honda
thonda@oaklandca.gov
2 City of Oakland | Full-Time and Permanent Part-Time Employees
Contact Information (continued)
Risk Contacts
Employee Benefits Program Risk Management Staff Contact Information
510.238.7165
Risk Administration Andrew Lathrop – Manager
alathrop@oaklandca.gov
• Administrative Support
• Safety Shoe Program, Health and Wellness
510.238.7660
• Paid Family Leave (non-sworn) Erika Turner
eturner@oaklandca.gov
• State Disability (Local 1021)
• Unemployment (EDD)
• Employee Assistance Program
510.238.4993
• Threat Assessment Greg Elliott
gelliott@oaklandca.gov
• CAL/OSHA Programs
• Ergonomics
510.238.7971
• Safety, Health & Wellness Lana Chan
LChan2@oaklandca.gov
• VDT Glasses
510.986.2898
• Risk – Contracts & Insurance Michael Bailey
mbailey@oaklandca.gov
• Workers’ Compensation
510.238.2270
• Fair Employment Housing Act (FEHA) Mary Baptiste
mbaptiste@oaklandca.gov
• Americans with Disabilities Act (ADA)
• Family Medical Leave Act (FMLA) 510-238-6488
Donella Williams
• Pregnancy Disability and Bonding dwilliams3@oaklandca.gov
City of Oakland | Full-Time and Permanent Part-Time Employees 3
Contact Information (continued)
You may also contact the below benefit carriers or visit the following websites to confirm eligibility and verify coverage:
Employee Benefits Program Phone Number Web Site
Medical
• CalPERS 888.225.7377 https://my.calpers.ca.gov
Dental
• Delta Dental – Group No. 00558 800.765.6003 www.deltadentalins.com
• DeltaCare – Group No. 76003 800.422.4234 www.deltadentalins.com
Vision
• Vision Service Plan – Group No. 00 826401 800.877.7195 www.vsp.com
Health Care and Day Care FSA
https://www.naviabenefits.com
• Navia Health Care FSA & Day Care FSA 800.669.3539 or
customerservice@naviabenefits.com
COBRA Administration
• Navia COBRA 877.920.9675 cobra@naviabenfits.com
Commuter Benefits
• GoNavia Commuter Benefits 800.669.3539 https://www.naviabenefits.com
• Guaranteed Ride Home Program 510.433.0320 ridehome@alamedactc.org
Life and Disability Insurance
• The Hartford - Life Insurance & Disability
800.523.2233 www.thehartford.com
Insurance Long & Short Term
Employee Assistance Program (EAP)
• Claremont EAP 800.834.3773 www.claremonteap.com
Deferred Comp
https://www.icmarc.org/city-of-
• Mission Square 800.669.7400
oakland-457-plan.html
4 City of Oakland | Full-Time and Permanent Part-Time Employees
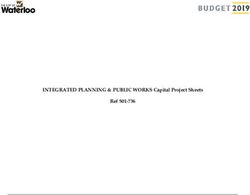
2023 Payroll Processing and Holiday Calendar
January JANUARY FEBRUARY MARCH
S M T W T F S S M T W T F S S M T W T F S
1 New Year’s Day
1 2 3 4 5 6 7 1 2 3 4 1 2 3 4
2 New Year’s Day (Observed)
8 9 10 11 12 13 14 5 6 7 8 9 10 11 5 6 7 8 9 10 11
16 Martin Luther King Jr. Day 15 16 17 18 19 20 21 12 13 14 15 16 17 18 12 13 14 15 16 17 18
22 23 24 25 26 27 28 19 20 21 22 23 24 25 19 20 21 22 23 24 25
February 29 30 31 26 27 28 26 27 28 29 30 31
20 President’s Day
APRIL MAY JUNE
March S M T W T F S S M T W T F S S M T W T F S
1 1 2 3 4 5 6 1 2 3
31 Cesar Chavez Day
2 3 4 5 6 7 8 7 8 9 10 11 12 13 4 5 6 7 8 9 10
9 10 11 12 13 14 15 14 15 16 17 18 19 20 11 12 13 14 15 16 17
May 16 17 18 19 20 21 22 21 22 23 24 25 26 27 18 19 20 21 22 23 24
29 Memorial Day 23 24 25 26 27 28 29 28 29 30 31 25 26 27 28 29 30
30
June JULY AUGUST SEPTEMBER
19 Juneteenth National S M T W T F S S M T W T F S S M T W T F S
Independence Day 1 1 2 3 4 5 1 2
2 3 4 5 6 7 8 6 7 8 9 10 11 12 3 4 5 6 7 8 9
July 9 10 11 12 13 14 15 13 14 15 16 17 18 19 10 11 12 13 14 15 16
16 17 18 19 20 21 22 20 21 22 23 24 25 26 17 18 19 20 21 22 23
4 Independence Day
23 24 25 26 27 28 29 27 28 29 30 31 24 25 26 27 28 29 30
30 31
September
OCTOBER NOVEMBER DECEMBER
4 Labor Day S M T W T F S S M T W T F S S M T W T F S
9 Admissions Day (HVA)* 1 2 3 4 5 6 7 1 2 3 4 1 2
8 9 10 11 12 13 14 5 6 7 8 9 10 11 3 4 5 6 7 8 9
November 15 16 17 18 19 20 21 12 13 14 15 16 17 18 10 11 12 13 14 15 16
11 Veteran’s Day (HVA)* 22 23 24 25 26 27 28 19 20 21 22 23 24 25 17 18 19 20 21 22 23
29 30 31 26 27 28 29 30 24 25 26 27 28 29 30
23 Thanksgiving Day
31
24 Day after Thanksgiving Day
Pay Period Ends
December Pay Dates
25 Christmas Day
*If applicable Holidays
City of Oakland | Full-Time and Permanent Part-Time Employees 5
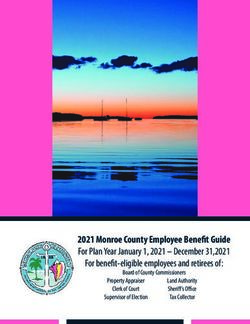
2023 Holiday Schedule
Date
2023 Holiday Day of the Week
Month Day
New Year’s Day January 01 Sunday
Dr. Martin Luther King, Jr. Day January 16 Monday
President’s Day February 20 Monday
Cesar Chavez Day March 31 Friday
Memorial Day May 29 Monday
Juneteenth National
June 19 Monday
Independence Day
Independence Day July 04 Tuesday
Labor Day September 04 Monday
Admissions Day September 09 Saturday
Veterans Day November 11 Saturday
Thanksgiving Day November 23 Thursday
Day After Thanksgiving November 24 Friday
Christmas Day December 25 Monday
Holidays that fall on Saturday, Sunday or Regular Day Off
If a designated holiday falls upon a normal day off which is either a Saturday; as to an employee who works a Monday
through Friday workweek, or the first day off a normal scheduled two day off, as to an employee whose workweek is one
other than Monday through Friday, shall thereafter receive one (1) additional day of vacation.
If a designated holiday falls upon a normal day off which is either a Sunday; as to an employee who works a Monday through
Friday workweek, or the second day off a normal scheduled two day off, as to an employee whose workweek is one other
than Monday through Friday, shall receive the next following day off.
Christmas Eve and New Year’s Eve
An employee whose regular workweek is Monday through Friday, and December 24th and December 31st occur on a
Saturday or Sunday, or employees that are required to work on both December 24th and December 31st shall be entitled to
one of the following:
• One half of the work-shift as paid time off on both • One full work-shift as paid time off on either the
the Friday preceding Christmas Eve and the Friday Friday preceding Christmas Eve or the Friday
preceding New Year’s Eve (when December 24th preceding New Year’s Eve (when December 24th
and December 31st falls on a Saturday or Sunday) and December 31st falls on a Saturday or Sunday)
or One half of the work-shift on both the or One full work-shift as paid time off on either of
above days; or the above days.
Local 1021
• One half of the work shift as paid time off on two • One full work shift as paid time off on
of the following: December 24th, December 26th, December 24th, December 26th, December 31st,
December 31st, or January 2nd; or or January 2nd.
6 City of Oakland | Full-Time and Permanent Part-Time Employees
Rates: Full‑Time Employees
Monthly Medical Plan Rates for Eligible Permanent Full-Time Employees
Effective January 1, 2023
REGION 1
Counties: Alameda, Alpine, Amador, Butte, Calavares, Colusa, Contra Costa, Del Norte, El Dorado, Glenn,
Humboldt, Lake, Lassen, Marin, Mariposa, Mendocino, Merced, Modoc, Mono, Monterey, Napa, Nevada,
Placer, Plumas, Sacramento, San Benito, San Francisco, San Joaquin, San Mateo, Santa Clara, Santa Cruz,
Medical Plans Shasta, Sierra, Siskiyou, Solano, Sonoma, Stanislaus, Sutter, Tehama, Trinity, Tuolumne, Yolo, and Yuba
Monthly Premium Cost Monthly Employee Contribution*
Employee + 2 Employee + 2
Employee Only Employee + 1 Employee Only Employee + 1
or more or more
Anthem EPO Del Norte $1,200.12 $2,400.24 $3,120.31 $286.38 $572.76 $744.59
Anthem Select HMO $1,128.83 $2,257.66 $2,934.96 $215.09 $430.18 $559.24
Anthem Traditional HMO $1,210.71 $2,421.42 $3,147.85 $296.97 $593.94 $772.13
Blue Shield Access+ HMO $1,035.21 $2,070.42 $2,691.55 $121.47 $242.94 $315.83
Blue Shield Access+ EPO $1,035.21 $2,070.42 $2,691.55 $121.47 $242.94 $315.83
Blue Shield Trio $888.94 $1,777.88 $2,311.24 $0.00 $0.00 $0.00
Health Net SmartCare HMO $1,174.50 $2,349.00 $3,053.70 $260.76 $521.52 $677.98
Kaiser (CA) HMO $913.74 $1,827.48 $2,375.72 $0.00 $0.00 $0.00
PERS Gold $825.61 $1,651.22 $2,146.59 $0.00 $0.00 $0.00
PERS Platinum $1,200.12 $2,400.24 $3,120.31 $286.38 $572.76 $744.59
PORAC (POLICE ONLY) $825.00 $1,875.00 $2,300.00 $0.00 $47.52 $0.00
United HealthCare HMO $1,044.07 $2,088.14 $2,714.58 $130.33 $260.66 $338.86
Western Health Advantage $760.17 $1,520.34 $1,976.44 $0.00 $0.00 $0.00
REGION 2
Fresno, Imperial, Inyo, Kern, Kings, Madera, Orange, San Diego, San Luis Obispo, Santa Barbara, Tulare,
and Ventura
Medical Plans Monthly Premium Cost Monthly Employee Contribution*
Employee + 2 Employee + 2
Employee Only Employee + 1 Employee Only Employee + 1
or more or more
Anthem Select HMO $765.37 $1,530.74 $1,989.96 $0.00 $0.00 $0.00
Anthem Traditional HMO $935.12 $1,870.24 $2,431.31 $21.38 $42.76 $55.59
Blue Shield Access+ HMO $842.61 $1,685.22 $2,190.79 $0.00 $0.00 $0.00
Blue Shield Access+ EPO $842.61 $1,685.22 $2,190.79 $0.00 $0.00 $0.00
Blue Shield Trio $760.71 $1,521.42 $1,977.85 $0.00 $0.00 $0.00
Health Net Salud y Mas $698.91 $1,397.82 $1,817.17 $0.00 $0.00 $0.00
Health Net SmartCare HMO $834.65 $1,669.30 $2,170.09 $0.00 $0.00 $0.00
Kaiser (CA) HMO $756.21 $1,512.42 $1,966.15 $0.00 $0.00 $0.00
PERS Gold $695.93 $1,391.86 $1,809.42 $0.00 $0.00 $0.00
PERS Platinum $1,014.80 $2,029.60 $2,638.48 $101.06 $202.12 $262.76
PORAC (POLICE ONLY) $820.00 $1,650.00 $2,100.00 $0.00 $0.00 $0.00
Sharp $764.96 $1,529.92 $1,988.90 $0.00 $0.00 $0.00
United HealthCare HMO $793.63 $1,587.26 $2,063.44 $0.00 $0.00 $0.00
United HealthCare
$871.58 $1,563.16 $2,032.11 $0.00 $0.00 $0.00
Harmony HMO
____________________
***IMPORTANT NOTE - You must verify the plan is available in your home or work zip code area.***
The information described on this page is only intended to be a summary of benefits. It does not describe or include all benefit provisions, limitations, exclusions, or
qualifications for coverage. Please review plan documents for full details. If there are any conflicts with information provided on this page, the plan documents will prevail.
City of Oakland | Full-Time and Permanent Part-Time Employees 7
Rates: Full‑Time Employees (continued)
Monthly Medical Plan Rates for Eligible Permanent Full-Time Employees
Effective January 1, 2023
REGION 3
Los Angeles, Riverside, San Bernardino
Medical Plans Monthly Premium Cost Monthly Employee Contribution*
Employee Employee Employee + Employee Employee Employee +
Only +1 2 or more Only +1 2 or more
Anthem Select HMO $737.91 $1,475.82 $1,918.57 $0.00 $0.00 $0.00
Anthem Traditional HMO $942.73 $1,885.46 $2,451.10 $28.99 $57.98 $75.38
Blue Shield Access+ HMO $738.29 $1,476.58 $1,919.55 $0.00 $0.00 $0.00
Blue Shield Trio $661.49 $1,322.98 $1,719.87 $0.00 $0.00 $0.00
Health Net Salud y Mas $606.34 $1,212.68 $1,576.48 $0.00 $0.00 $0.00
Health Net SmartCare HMO $755.29 $1,510.58 $1,963.75 $0.00 $0.00 $0.00
Kaiser (CA) HMO $754.64 $1,509.28 $1,962.06 $0.00 $0.00 $0.00
PERS Gold $680.37 $1,360.74 $1,768.96 $0.00 $0.00 $0.00
PERS Platinum $992.59 $1,985.18 $2,580.73 $78.85 $157.70 $205.01
PORAC (POLICE ONLY) $820.00 $1,600.00 $2,100.00 $0.00 $0.00 $0.00
United HealthCare HMO $790.46 $1,580.92 $2,055.20 $0.00 $0.00 $0.00
United HealthCare
$713.55 $1,427.10 $1,855.23 $0.00 $0.00 $0.00
Harmony HMO
REGION - OUT OF STATE
Monthly Premium Cost Monthly Employee Contribution*
Medical Plans
Employee Employee Employee + Employee Employee Employee +
Only +1 2 or more Only +1 2 or more
Kaiser Out of State $1,155.43 $2,310.86 $3,004.12 $241.69 $483.38 $628.40
PERS Platinum $1,003.90 $2,007.80 $2,610.14 $90.16 $180.32 $234.42
PORAC (POLICE ONLY) $935.00 $1,899.00 $2,250.00 $21.26 $71.52 $0.00
____________________
***IMPORTANT NOTE - You must verify the plan is available in your home or work zip code area.***
The information described on this page is only intended to be a summary of benefits. It does not describe or include all benefit provisions, limitations, exclusions, or
qualifications for coverage. Please review plan documents for full details. If there are any conflicts with information provided on this page, the plan documents will prevail.
8 City of Oakland | Full-Time and Permanent Part-Time EmployeesRates: Full‑Time Employees (continued)
Dental & Vision Rates
Benefit Plan Employee Only Employee + 1 Employee + Family
Delta Dental PPO
• City’s Contribution: $102.57
$0 $0 $0
• Total Premium Cost: $102.57
DeltaCare HMO
• City’s Contribution: $33.56
$0 $0 $0
• Total Premium Cost: $33.56
Vision Service Plan
• Employee Only
– City’s Contribution: $8.66 $0 - -
– Total Premium Cost: $8.66
• Employee + 1
– City’s Contribution: $17.32 - $0 -
– Total Premium Cost: $17.32
• Employee + Family
– City’s Contribution: $20.33 - - $0
– Total Premium Cost: $20.33
City of Oakland | Full-Time and Permanent Part-Time Employees 9Rates: Permanent Part-Time Employees
Monthly Medical Plan Rates for Eligible Permanent Part-Time Employees
Effective January 1, 2023
REGION 1
Counties: Alameda, Alpine, Amador, Butte, Calavares, Colusa, Contra Costa, Del Norte, El Dorado, Glenn,
Humboldt, Lake, Lassen, Marin, Mariposa, Mendocino, Merced, Modoc, Mono, Monterey, Napa, Nevada,
Placer, Plumas, Sacramento, San Benito, San Francisco, San Joaquin, San Mateo, Santa Clara, Santa Cruz,
Shasta, Sierra, Siskiyou, Solano, Sonoma, Stanislaus, Sutter, Tehama, Trinity, Tuolumne, Yolo, and Yuba
Medical Plans
Monthly Premium Cost Monthly Employee Contribution
Employee Employee Employee + Employee Employee Employee +
Only +1 2 or more Only +1 2 or more
Anthem EPO Del Norte $1,200.12 $2,400.24 $3,120.31 $514.82 $1,029.63 $1,338.52
Anthem Select HMO $1,128.83 $2,257.66 $2,934.96 $443.53 $887.05 $1,153.17
Anthem Traditional HMO $1,210.71 $2,421.42 $3,147.85 $525.41 $1,050.81 $1,366.06
Blue Shield Access+ HMO $1,035.21 $2,070.42 $2,691.55 $349.91 $699.81 $909.76
Blue Shield Access+ EPO $1,035.21 $2,070.42 $2,691.55 $349.91 $699.81 $909.76
Blue Shield Trio $888.94 $1,777.88 $2,311.24 $203.64 $407.27 $529.45
Health Net SmartCare HMO $1,174.50 $2,349.00 $3,053.70 $489.20 $978.39 $1,271.91
Kaiser (CA) HMO $913.74 $1,827.48 $2,375.72 $228.44 $456.87 $593.93
PERS Gold $825.61 $1,651.22 $2,146.59 $140.31 $280.61 $364.80
PERS Platinum $1,200.12 $2,400.24 $3,120.31 $514.82 $1,029.63 $1,338.52
United HealthCare HMO $1,044.07 $2,088.14 $2,714.58 $358.77 $717.53 $932.79
Western Health Advantage $760.17 $1,520.34 $1,976.44 $74.86 $149.73 $194.65
REGION 2
Fresno, Imperial, Inyo, Kern, Kings, Madera, Orange, San Diego, San Luis Obispo, Santa Barbara, Tulare,
and Ventura
Medical Plans Monthly Premium Cost Monthly Employee Contribution
Employee Employee Employee + Employee Employee Employee +
Only +1 2 or more Only +1 2 or more
Anthem Select HMO $765.37 $1,530.74 $1,989.96 $80.06 $160.13 $208.17
Anthem Traditional HMO $935.12 $1,870.24 $2,431.31 $249.82 $499.63 $649.52
Blue Shield Access+ HMO $842.61 $1,685.22 $2,190.79 $157.31 $314.61 $409.00
Blue Shield Access+ EPO $842.61 $1,685.22 $2,190.79 $157.31 $314.61 $409.00
Blue Shield Trio $760.71 $1,521.42 $1,977.85 $75.41 $150.81 $196.06
Health Net Salud y Mas $698.91 $1,397.82 $1,817.17 $13.60 $27.21 $35.38
Health Net SmartCare HMO $834.65 $1,669.30 $2,170.09 $149.35 $298.69 $388.30
Kaiser (CA) HMO $756.21 $1,512.42 $1,966.15 $70.91 $141.81 $184.36
PERS Gold $695.93 $1,391.86 $1,809.42 $10.62 $21.25 $27.63
PERS Platinum $1,014.80 $2,029.60 $2,638.48 $329.50 $658.99 $856.69
Sharp $764.96 $1,529.92 $1,988.90 $79.66 $159.31 $207.11
United HealthCare HMO $793.63 $1,587.26 $2,063.44 $108.33 $216.65 $281.65
United HealthCare
$871.58 $1,563.16 $2,032.11 $186.28 $192.55 $250.32
Harmony HMO
____________________
***IMPORTANT NOTE - You must verify the plan is available in your home or work zip code area.***
10 City of Oakland | Full-Time and Permanent Part-Time EmployeesRates: Permanent Part-Time Employees (continued)
Monthly Medical Plan Rates for Eligible Permanent Part-Time Employees
Effective January 1, 2023
REGION 3
Los Angeles, Riverside, San Bernardino
Medical Plans Monthly Premium Cost Monthly Employee Contribution
Employee Employee Employee + Employee Employee Employee +
Only +1 2 or more Only +1 2 or more
Anthem Select HMO $737.91 $1,475.82 $1,918.57 $52.60 $105.21 $136.78
Anthem Traditional HMO $942.73 $1,885.46 $2,451.10 $257.43 $514.85 $669.31
Blue Shield Access+ HMO $738.29 $1,476.58 $1,919.55 $52.98 $105.97 $137.76
Blue Shield Trio $661.49 $1,322.98 $1,719.87 $0.00 $0.00 $0.00
Health Net Salud y Mas $606.34 $1,212.68 $1,576.48 $0.00 $0.00 $0.00
Health Net SmartCare HMO $755.29 $1,510.58 $1,963.75 $69.98 $139.97 $181.96
Kaiser (CA) HMO $754.64 $1,509.28 $1,962.06 $69.33 $138.67 $180.27
PERS Gold $680.37 $1,360.74 $1,768.96 $0.00 $0.00 $0.00
PERS Platinum $992.59 $1,985.18 $2,580.73 $307.29 $614.57 $798.94
United HealthCare HMO $790.46 $1,580.92 $2,055.20 $105.16 $210.31 $273.41
United HealthCare
$713.55 $1,427.10 $1,855.23 $28.24 $56.49 $73.44
Harmony HMO
____________________
***IMPORTANT NOTE - You must verify the plan is available in your home or work zip code area.***
Monthly Dental and Vision Plan Rates for Eligible
Permanent Part-Time Employees
Monthly Premium Cost Monthly Employee Contribution
Plan Employee Employee Employee + Employee Employee Employee +
Only +1 2 or more Only +1 2 or more
Delta Dental PPO $116.00 $116.00 $116.00 $29.00 $29.00 $29.00
DentalCare HMO $34.99 $34.99 $34.99 $8.75 $8.75 $8.75
VSP Vision $8.41 $16.82 $19.75 $2.10 $4.21 $4.94
The information described on this page is only intended to be a summary of benefits. It does not describe or include all benefit provisions, limitations, exclusions, or
qualifications for coverage. Please review plan documents for full details. If there are any conflicts with information provided on this page, the plan documents will prevail.
City of Oakland | Full-Time and Permanent Part-Time Employees 11Introduction
As City of Oakland employees, you and your family are entitled to a number of benefits. This benefits guide contains
information on all of the benefits you are entitled to as an employee of the City of Oakland.
In order to activate your benefits, complete and submit Benefit Choices
the following:
The City recognizes that your benefits are an important
• CalPERS Beneficiary Designation Form part of the reason you choose to work here. The City
• City of Oakland Employee Benefits Record (EBR) provides high quality benefits at a reasonable cost to you.
You can choose between different medical plans to meet
Optional Benefit Forms your individual and family needs. Since you have some
• Flexible Spending Plan Enrollment form choices to make, it is important to understand the various
programs. That is why this Handbook is being provided
• Cafeteria Plan Election form (Medical Waiver)
for you. There are also individual brochures for each
• Optional Life & Voluntary AD&D Insurance form of the benefit plans available in the Human Resources
• Spouse and child coverage available to employees department. Benefits provided by the City for eligible
who are enrolled employees include a choice of CalPERS medical plans, a
dental plan, a vision plan, group life insurance coverage,
• Evidence of Insurability form (Required only if
group disability and optional voluntary benefits.
enrolling in Life Insurance coverage that exceeds
$100,000)
• Pre-designation of Personal Physician
You have 60 days from the date of your initial
appointment to enroll or decline coverage for yourself
and eligible family members. Benefits will begin on
the 1st of the month after you submit your paperwork
and appropriate documentation to the Human Resources
Management and Risk Benefits Division. If you do not
enroll during the initial 60 days and have not experienced
a qualifying life event, your enrollment will be subject to
a 90-day waiting period or the following Open Enrollment
period, whichever comes first.
Any questions you may have regarding the enclosed
information can be referred to the corresponding
representative listed in your “Benefits Telephone
Directory” found at the beginning of this guide or
emailed to BenefitsAdmin@oaklandca.gov.
12 City of Oakland | Full-Time and Permanent Part-Time EmployeesEligibility
Employees Dependents
The City of Oakland offers Medical, Dental, Vision, Group When enrolling dependents, appropriate documentation
Life/AD&D, and Supplemental Coverage to full‑time and/or proof of dependent status is required by the City
and permanent part‑time employees and their eligible and will be requested by Human Resources.
dependents.
Accepted forms of proof include Marriage and Birth
Employees may opt out of coverage with proof of other Certificates, Tax Returns, Local City Government or State
group coverage. Issued Declaration of Domestic Partnership, Adoption
Certificate or Proof of Legal Guardianship.
To elect the medical waiver plan you must:
For purposes of medical plan coverage, the following
• Complete the Medical Wavier Form
dependents are eligible:
• Complete the Employee Benefits Record Form
• A spouse who is not currently enrolled as an
• Provide proof of other coverage in the form of a employee in a Public Employees Retirement
letter. Insurance cards are not accepted. Medical System (PERS)-administered medical plan
Waiver Premium
• A registered domestic partner
The Medical Waiver Premium amounts are based off
• Certified disabled child age 26 or older
your represented unit. Please refer to your MOU for
premium amounts. • Child (up to age 26) for whom you have a
parent-child relationship (restrictions apply)
• Adopted Child
For purposes of non‑sworn dental and vision plan
coverage, eligible dependents are as follows:
• A spouse
• Child (up to age 19, or age 25 with student status)
for whom you have a parent-child relationship
(restrictions apply)
• Adopted Child
• Certified disabled child, age 25 or older
• A registered domestic partner of an employee
Active Employment
Employees who are eligible to participate in the medical
and dental group insurance plans are full‑time employees,
permanent part‑time employees, and limited-duration
employees with an appointment of six (6) months
or longer.
Employees who are eligible to participate in the vision
plan are all non‑sworn unrepresented employees and
represented employees as provided for in the individual
Memoranda of Understanding.
City of Oakland | Full-Time and Permanent Part-Time Employees 13Enrollment
Open Enrollment
Once a year, usually during the fall, the City of Oakland The following forms must be provided in order to
holds an Open Enrollment period. During this time, you commence your benefits (please attach required copies of
may change to a different medical plan, enroll in the documents for dependents):
dental plan, the vision plan or choose the cash in lieu
• Employee Benefits Record (EBR) form
option (waiver). You may also add or delete dependents
to your medical, dental or vision plan. • CalPERS Beneficiary Designation form
Supporting documentation will be required by Online enrollment is required for Parking and Transit
Human Resources to add or delete new dependents. Programs, and the Guaranteed Ride Home.
Please submit your forms and required documents to the
Enrollment Instructions Benefits Unit, 150 Frank Ogawa Plaza, 2nd Floor front
counter or you can fax your forms to 510.238.6560.
When you are hired, you will receive this Employee
Benefits Guide describing your different benefits. All benefits information and forms can be found on the
Additional brochures are available at the City of Oakland. City of Oakland website at www.oaklandca.gov/benefits
Your coverage will start on the first of the month following or at 150 Frank H. Ogawa Plaza, 2nd Floor
the date your enrollment paperwork is received (provided (Human Resources Front Counter) Oakland, CA 94612.
you submit your enrollment forms within 60 days of
the enrollment period).
Change in Beneficiaries
Here are some basic guidelines you need to keep in mind
Certain events in your life such as marriage, divorce, or
when going over these choices:
a death in the family can affect who you name as your
1. Review the section of this Guide on medical plans designated beneficiary for certain benefits. You may
to determine which medical plan suits your health change your beneficiary(ies) at any time. If you wish
and financial needs. to do so, you can obtain most beneficiary forms from
Human Resources.
2. Determine your life insurance needs and decide if
you wish to buy additional coverage above what is You can designate a beneficiary for:
provided by the City.
• Deferred Compensation
3. Review additional voluntary benefits offered by the
City to determine whether they meet your needs. • Life Insurance
4. If you have medical coverage through another • Retirement - CalPERS
source, such as a spouse, you may want to consider
the benefit waiver option. Proof of other group
coverage will be required in order to qualify for
this option.
14 City of Oakland | Full-Time and Permanent Part-Time EmployeesChanges in Coverage
Qualifying Events
You may experience certain events during the plan year that would allow you to change you or your dependent’s medical
coverage. If any of the following events occur, you must change your benefit coverage within 60 days of the event:
• Change in your legal marital or domestic • Your dependent satisfies or no longer meets the
partner status, including marriage, death of your eligibility requirements for dependents.
spouse/domestic partner, divorce, legal separation
• A change in the place of residence or worksite of
or annulment.
you or your spouse/domestic partner (this move
• Change in the number of your dependents, must affect your coverage options).
including birth, adoption, placement for adoption
• You, your spouse/domestic partner or your
or death of your dependent.
dependents lose COBRA coverage.
• Change in your employment status, including
• You, your spouse/domestic partner or your
termination or commencement of employment of
dependents enroll for Medicare or Medicaid or lose
you, your spouse, your domestic partner or your
coverage under Medicare or Medicaid.
dependent.
• A significant change in benefit or cost of coverage
• Change in work schedule for you or your
for you or your spouse/domestic partner.
spouse/domestic partner, including an increase or
decrease in the number of hours of employment, • Your spouse/domestic partner employer provides
a switch between full‑time and part‑time status, a the opportunity to enroll or change benefits during
strike, lockout or commencement or return from an an open enrollment period.
unpaid leave of absence.
Special Enrollment Rights as Provided by HIPAA
• You initially declined coverage under the plan because you had coverage under another plan and subsequently
incurred a loss of coverage under the other plan.
• Occurrence of certain events such as birth, adoption, placement for adoption or marriage.
Click here to watch a video on Qualifying Life Events.
City of Oakland | Full-Time and Permanent Part-Time Employees 152023 Summary of Benefits and Coverage Notice
Choosing your health plan is an important decision. To assist you with this process, each health plan available through the
California Public Employees’ Retirement System has produced a Summary of Benefits and Coverage (SBC). In addition,
the federal government has compiled a glossary of common health insurance terms. Together, these documents provide
important information to help you better understand your health benefit coverage and more easily compare health
plan options.
To access the SBCs and glossary online, visit www.calpers.ca.gov and select View Health Plan Rates to access the Plans &
Rates page, or visit any of the health plan websites below. To request a free paper copy of the SBC and glossary, contact
each health plan directly.
Anthem Blue Cross HMO & EPO Kaiser Permanente
855.839.4524 800.464.4000
www.anthem.com/ca/calpers www.kp.org/calpers
Blue Shield of California Peace Officers Research Association of California1
800.334.5847 800.288.6928
www.blueshieldca.com/calpers http://ibt.porac.org
California Association of Highway Patrolmen1 PERS Gold and PERS Platinum
800.734.2247 877.737.7776
www.thecahp.org www.anthem.com/ca/calpers
California Correctional Peace Officers Association1 Sharp Health Plan
800.257.6213 855.995.5004
www.ccpoabtf.org www.sharphealthplan.com/calpers
Health Net of California UnitedHealthcare
888.926.4921 877.359.3714
www.healthnet.com/calpers www.uhc.com/calpers
Western Health Advantage
888.942.7377
www.westernhealth.com/calpers
_______________
1 To enroll in these health plans, you must belong to the specific employee association and pay applicable dues.
16 City of Oakland | Full-Time and Permanent Part-Time EmployeesMedical – CalPERS
The City of Oakland offers several different medical plan options; Health Maintenance Organizations (HMO) or Preferred
Provider Organizations (PPO) for all full‑time and permanent part‑time employees and their eligible dependents.
Health Maintenance Organizations (HMOs)
HMOs allow you to receive comprehensive coverage at set prices, called copays.
• Doctors/Other Medical Care Providers. You • Copays. When you receive medical care, you pay a
can only use doctors, hospitals, and pharmacies set dollar amount called a copay.
that participate in the HMO network. Doctors
• Annual Out-of-Pocket Maximum. The HMO plans
who participate in the HMO network are called
include an annual out-of-pocket maximum. This
in- network providers. There is no coverage if
is the maximum amount you must pay out of your
you go to out-of-network providers, except for
own pocket for copays during the plan year. Once
emergency services.
you reach the out-of-pocket maximum, the plan
• Annual Deductible. You don’t need to pay an pays 100% of covered charges for the remainder of
annual deductible before the plan begins to pay the plan year.
for a portion of covered medical services.
Preferred Provider Organization (PPO)
The PPO plan allows you to use any provider you choose.
• Doctors/Health Care Providers. You can choose • Paying for Care. When you receive medical care,
any doctor you want, and you can go to any there are two ways you pay for services:
hospital or pharmacy. However, you’ll pay less
– Copays. When you go to an in-network
when you use a provider or facility that participates
doctor for an office visit, go to the emergency
in-network.
room, or pick up a prescription, you pay
• Preventive Care. Preventive care is 100% a set dollar amount called a copay. (You
covered when you use in-network providers. Visit may need to pay the annual deductible
healthcare.gov/preventive-care-benefits/ for a first before the copay applies.)
complete list of preventive care benefits required
– Coinsurance. When you receive any other
to be covered at 100% per the Affordable
medical services, you pay a percentage of
Care Act.
the cost of the service and the plan pays
• Annual Deductible. You generally pay an annual the remaining percentage. This is called
deductible before the plan begins to pay for a coinsurance. (You will need to pay the annual
portion of covered medical services. deductible first before coinsurance applies.)
• Annual Out-of-Pocket Maximum. The PPO
Click here to watch a includes an out-of-pocket maximum. This is the
video on Health Maintenance maximum amount you must pay out of your
Organizations (HMO). own pocket (under the applicable coinsurance
percentage) after meeting the deductible. Once
you reach the out-of-pocket maximum, the
Click here to watch a plan pays 100% of in- network charges for the
video onPreferred Provider remainder of the plan year. Please note that your
out-of-pocket maximum will be lower when you use
Organizations (PPO).
in-network providers.
Click here to watch a video
on PPO vs HMO.
City of Oakland | Full-Time and Permanent Part-Time Employees 172023 CalPERS – EPO & HMO Basic Plans
For more details about the benefits provided by a specific plan, refer to that plan’s Evidence of Coverage (EOC) booklet.
Anthem UnitedHealthcare
Blue Shield Health Net Western
Blue Cross Sharp SignatureValue
Kaiser Health
Benefits EPO Access+ HMO & Performance
Salud y Más & Permanente Alliance HMO Advantage
Select HMO Access+ EPO Plus
SmartCare Harmony HMO HMO
Traditional HMO Trio HMO
Calendar Year Deductible
• Individual N/A N/A N/A N/A N/A N/A N/A
• Family N/A N/A N/A N/A N/A N/A N/A
Maximum Calendar Year Copay or Coinsurance (excluding pharmacy)
• Individual $1,500 (copay) $1,500 (copay) $1,500 (copay) $1,500 (copay) $1,500 (copay) $1,500 (copay) $1,500 (copay)
• Family $3,000 (copay) $3,000 (copay) $3,000 (copay) $3,000 (copay) $3,000 (copay) $3,000 (copay) $3,000 (copay)
Hospital (including Mental Health and Substance Abuse)
• Deductible
N/A N/A N/A N/A N/A N/A N/A
(per admission)
• Inpatient No Charge No Charge No Charge No Charge No Charge No Charge No Charge
• Outpatient
No Charge No Charge No Charge $15 No Charge No Charge No Charge
Facility Charge
Emergency Services
• Emergency Room
N/A N/A N/A N/A N/A N/A N/A
Deductible
• Emergency (copay
waived if admitted
as an inpatient or $50 $50 $50 $50 $50 $50 $50
for observation as
an outpatient)
• Non-Emergency
(copay waived if
admitted as an
$50 $50 $50 $50 $50 $50 $50
inpatient or for
observation as
an outpatient)
The information described on this page is only intended to be a summary of benefits. It does not describe or include all benefit provisions, limitations, exclusions, or qualifications for coverage. Please review plan documents for full details. If there
are any conflicts with information provided on this page, the plan documents will prevail.
18 City of Oakland | Full-Time and Permanent Part-Time Employees2023 CalPERS – EPO & HMO Basic Plans (continued)
For more details about the benefits provided by a specific plan, refer to that plan’s Evidence of Coverage (EOC) booklet.
Anthem UnitedHealthcare
Blue Shield Health Net Western
Blue Cross Sharp SignatureValue
Kaiser Health
Benefits EPO Access+ HMO & Performance
Salud y Más & Permanente Alliance HMO Advantage
Select HMO Access+ EPO Plus
SmartCare Harmony HMO HMO
Traditional HMO Trio HMO
Physician Services (including Mental Health and Substance Abuse)
• Office Visits (copay $15 $15 $15 $15 $15 $15 $15
for each service provided)
• Inpatient Visits No Charge No Charge No Charge No Charge No Charge No Charge No Charge
• Outpatient Visits $15 $15 $15 $15 $15 $15 $15
• Urgent Care Visits $15 $15 $15 $15 $15 $15 $15
• Preventive Services No Charge No Charge No Charge No Charge No Charge No Charge No Charge
• Surgery/Anesthesia No Charge No Charge No Charge No Charge No Charge No Charge No Charge
Diagnostic X-Ray/Lab
No Charge No Charge No Charge No Charge No Charge No Charge No Charge
Prescription Drugs
• Deductible N/A N/A N/A N/A N/A N/A N/A
Tier 1: $5 Generic/Tier 11: $5 Tier 1: $5 Tier 1: $5 Tier 1: $5 Tier 1: $5
• Retail Pharmacy Brand Preferred/Tier 21: $20 Generic: $5
Tier 2: $20 Tier 2: $20 Tier 2: $20 Tier 2: $20 Tier 2: $20
(30-day supply) Non-Preferred/Tier 31: $50 Brand: $20
Tier 3: $50 Tier 41: $30 Tier 3: $50 Tier 3: $50 Tier 3: $50 Tier 3: $50
• Retail Preferred
Tier 1: $10 Generic/Tier 11: $10 Tier 1: $10 Tier 1: $10 Tier 1: $10 Tier 1: $10
Pharmacy Brand Preferred/Tier 21: $40
Maintenance Tier 2: $40 Non-Preferred/Tier 31: $100
Tier 2: $40 N/A Tier 2: $40 Tier 2: $40 Tier 2: $40
Medications Tier 3: $100 Tier 41: $60 Tier 3: $100 Tier 3: $100 Tier 3: $100 Tier 3: $100
(90-day supply)
• Mail Order Generic/Tier 11: $10
Pharmacy Program Tier 1: $10 Tier 1: $10 Generic: $10 Tier 1: $10 Tier 1: $10 Tier 1: $10
Brand Preferred/Tier 21: $40
(not to exceed Tier 2: $40 Non-Preferred/Tier 31: $100
Tier 2: $40 Brand: $40 Tier 2: $40 Tier 2: $40 Tier 2: $40
90-day supply for Tier 3: $100 Tier 41: $60 Tier 3: $100 (31-100 day supply Tier 3: $100 Tier 3: $100 Tier 3: $100
maintenance drugs)
• Mail order
maximum
copayment $1,000 $1,000 $1,000 N/A $1,000 $1,000 $1,000
per person per
calendar year
_______________
1 Tier formulary BSC Trio HMO only
Tier 1 refers to medications classified as ‘Generic’; Tier 2 refers to medications classified as “Preferred Brand”; and Tier 3 refers to medications classified as “Non-Preferred Brand”.
The information described on this page is only intended to be a summary of benefits. It does not describe or include all benefit provisions, limitations, exclusions, or qualifications for coverage. Please review plan documents for full details. If there
are any conflicts with information provided on this page, the plan documents will prevail.
19 City of Oakland | Full-Time and Permanent Part-Time Employees2023 CalPERS – EPO & HMO Basic Plans (continued)
For more details about the benefits provided by a specific plan, refer to that plan’s Evidence of Coverage (EOC) booklet.
Anthem UnitedHealthcare
Blue Shield Health Net Western
Blue Cross Sharp SignatureValue
Kaiser Health
Benefits EPO Access+ HMO & Performance
Salud y Más & Permanente Alliance HMO Advantage
Select HMO Access+ EPO Plus
SmartCare Harmony HMO HMO
Traditional HMO Trio HMO
Durable Medical Equipment
No Charge No Charge No Charge No Charge No Charge No Charge No Charge
Infertility Testing/Treatment
50% of Covered 50% of Covered 50% of Covered 50% of Covered 50% of Covered 50% of Covered 50% of Covered
Charges Charges Charges Charges Charges Charges Charges
Occupational /Physical /Speech Therapy
• Inpatient
(hospital or skilled No Charge No Charge No Charge No Charge No Charge No Charge No Charge
nursing facility)
• Outpatient
(office and $15 $15 $15 $15 $15 $15 $15
home visits)
Diabetes Services
Coverage
• Glucose monitors Coverage varies No Charge Coverage varies No Charge Coverage varies Coverage varies
varies
• Self-management
$15 $15 $15 $15 $15 $15 $15
training
Acupuncture
$15/visit $15/visit $15/visit $15/visit $15/visit $15/visit $15/visit
(acupuncture/chiropractic; (acupuncture/chiropractic; (acupuncture/chiropractic; (acupuncture/chiropractic; (acupuncture/chiropractic; (acupuncture/chiropractic; (acupuncture/chiropractic;
combined 20 visits per combined 20 visits per combined 20 visits per combined 20 visits per combined 20 visits per combined 20 visits per combined 20 visits per
calendar year) calendar year) calendar year) calendar year) calendar year) calendar year) calendar year)
Chiropractic
$15/visit $15/visit $15/visit $15/visit $15/visit $15/visit $15/visit
(acupuncture/chiropractic; (acupuncture/chiropractic; (acupuncture/chiropractic; (acupuncture/chiropractic; (acupuncture/chiropractic; (acupuncture/chiropractic; (acupuncture/chiropractic;
combined 20 visits per combined 20 visits per combined 20 visits per combined 20 visits per combined 20 visits per combined 20 visits per combined 20 visits per
calendar year) calendar year) calendar year) calendar year) calendar year) calendar year) calendar year)
The information described on this page is only intended to be a summary of benefits. It does not describe or include all benefit provisions, limitations, exclusions, or qualifications for coverage. Please review plan documents for full details. If there
are any conflicts with information provided on this page, the plan documents will prevail.
20 City of Oakland | Full-Time and Permanent Part-Time Employees2023 CalPERS – PPO Basic Plans
For more details about the benefits provided by a specific plan, refer to that plan’s Evidence of Coverage (EOC) booklet.
PERS Gold PERS Platinum PORAC
(Association Plan)
Benefits
PPO Non-PPO PPO Non-PPO PPO Non-PPO
Calendar Year Deductible
• Individual $1,0001,3 $5003 $300 $600
• Family $2,000 1,3
$1,000 3
$900 $1,800
Maximum Calendar Year Copay or Coinsurance (excluding pharmacy)
• Individual $3,000 (coinsurance) Unlimited $2,000 (coinsurance) Unlimited $2,000 Unlimited
• Family $6,000 (coinsurance) Unlimited $4,000 (coinsurance) Unlimited $4,000 Unlimited
Hospital (including Mental Health and Substance Abuse)
• Deductible (per admission) N/A N/A $250 N/A
• Inpatient 20% 2
40% 4
10% 40% 4
20% 20%4
• Outpatient Facility/
20% 40%4 10% 40%4 20% 20%4
Surgery Services
Emergency Services
• Emergency Room Deductible $50 $50 N/A
(applies to hospital emergency room facility charge only) (applies to hospital emergency room facility charge only)
• Emergency 20% 10% 20%
(applies to other services such as physician, x-ray, lab, etc.) (applies to other services such as physician, x-ray, lab, etc.)
20% 40% 10% 40%
• Non-Emergency 50%
(payment for physician charges only; emergency (payment for physician charges only; emergency (for non-emergency services provided by hospital emergency room)
room facility charge is not covered) room facility charge is not covered)
_______________
1 Incentives available to reduce individual deductible (max. $500) or family deductible (max. $1,000) include: getting a biometric screening ($100 credit); receiving a flu shot ($100 credit); getting a non-smoking certification
($100 credit); getting a virtual second opinion ($100 credit); and getting a condition care certification ($100 credit).
2 Coinsurance waived for deliveries if enrolled in Future Moms Program.
3 Deductible is transferable between PERS Gold and PERS Platinum.
4 Of the allowable amount as defined in the EOC.
The information described on this page is only intended to be a summary of benefits. It does not describe or include all benefit provisions, limitations, exclusions, or qualifications for coverage. Please review plan documents for full details. If there
are any conflicts with information provided on this page, the plan documents will prevail.
21 City of Oakland | Full-Time and Permanent Part-Time Employees2023 CalPERS – PPO Basic Plans (continued)
For more details about the benefits provided by a specific plan, refer to that plan’s Evidence of Coverage (EOC) booklet.
PERS Gold PERS Platinum PORAC
(Association Plan)
Benefits
PPO Non-PPO PPO Non-PPO PPO Non-PPO
Physician Services (including Mental Health and Substance Abuse)
• Office Visits (copay for
$351 40%3 $202 40%3 $10/$351 20%3
each service provided)
• Inpatient Visits 20% 40%3 10% 40%3 20% 20%3
• Outpatient Visits $35 40%3 $20 40%3 20% 20%3
• Urgent Care Visits $35 40%3 $20 40%3 $35 20%3
• Preventive Services No Charge 40% 3
No Charge 40% 3
No Charge
• Surgery/Anesthesia 20% 40% 3
10% 40% 3
20% 20%3
Diagnostic X-Ray/Lab
20% 40%3 10% 40%3 20% 20%3
_______________
1 Reduced to $10 when seen by primary physician
2 $35 for specialist visit
3 Of the allowable amount as defined in the EOC
The information described on this page is only intended to be a summary of benefits. It does not describe or include all benefit provisions, limitations, exclusions, or qualifications for coverage. Please review plan documents for full details. If there
are any conflicts with information provided on this page, the plan documents will prevail.
22 City of Oakland | Full-Time and Permanent Part-Time Employees2023 CalPERS – PPO Basic Plans (continued)
For more details about the benefits provided by a specific plan, refer to that plan’s Evidence of Coverage (EOC) booklet.
PERS Gold PERS Platinum PORAC
(Association Plan)
Benefits
PPO Non-PPO PPO Non-PPO PPO Non-PPO
Prescription Drugs
• Deductible N/A N/A N/A
Generic: $10
Tier 1: $5 Tier 1: $5
• Retail Pharmacy Brand Formulary: $25
Tier 2: $20 Tier 2: $20
(30-day supply) Non-Formulary: $45
Tier 3: $50 Tier 3: $50
Compound: $45
Tier 1: $10 Tier 1: $10
• Retail Preferred Pharmacy
Tier 2: $40 Tier 2: $40 N/A
Maintenance Medications
Tier 3: $100 Tier 3: $100
• Mail Order Pharmacy Program Tier 1: $10 Tier 1: $10 Generic: $20
(not to exceed 90-day supply Tier 2: $40 Tier 2: $40 Brand Formulary: $40 N/A
for maintenance drugs) Tier 3: $100 Tier 3: $100 Non-Formulary: $75
• Mail order maximum copayment
$1,000 $1,000 N/A
per person per calendar year
Durable Medical Equipment
20% 40% 1 10% 40% 1 20% 20%1
(pre-certification required for the purchase of
(pre-certification required for equipment)
equipment priced at $1,000 or more)
_______________
1 Of the allowable amount as defined in the EOC
The information described on this page is only intended to be a summary of benefits. It does not describe or include all benefit provisions, limitations, exclusions, or qualifications for coverage. Please review plan documents for full details. If there
are any conflicts with information provided on this page, the plan documents will prevail.
23 City of Oakland | Full-Time and Permanent Part-Time Employees2023 CalPERS – PPO Basic Plans (continued)
For more details about the benefits provided by a specific plan, refer to that plan’s Evidence of Coverage (EOC) booklet.
PERS Gold PERS Platinum PORAC
(Association Plan)
Benefits
PPO Non-PPO PPO Non-PPO PPO Non-PPO
Infertility Testing/Treatment
50% 50% 50% 50%2
Occupational / Physical / Speech Therapy
• Inpatient (hospital or 20%
No Charge No Charge (no copay for inpatient 20%2
skilled nursing facility) PT/OT by a PAR provider)
20% 40% 10% 40% $15/visit 20%2
• Outpatient (Occupational therapy 20%) (Occupational therapy 20%) (all other services 20%)3
(office and home visits)
(Pre-certification required for more than 24 visits) (Pre-certification required for more than 24 visits)
Diabetes Services
• Glucose monitors Coverage Varies Coverage Varies Coverage Varies
• Self-management training $201 40%2 $201 40%2 $20 60%2
Acupuncture
$15/visit 40%2 $15/visit 40%2 $15 20%2
(acupuncture/chiropractic combined 20 visits per calendar year) (acupuncture/chiropractic; combined 20 visits per calendar year) (all other services 20%)3
Chiropractic
$15/visit 40%2 $15/visit 40%2 $15/visit 20%2
• Office Visit (combined 20 visits
(acupuncture/chiropractic combined 20 visits per calendar year) (acupuncture/chiropractic; combined 20 visits per calendar year)
per calendar year)
_______________
1 $35 for specialist visit
2 Of the allowable amount as defined in the EOC
3 Combined 20 visits per calendar year. Speech therapy is not included in the 20 visit per calendar year combination; see EOC for Speech Therapy benefit.
The information described on this page is only intended to be a summary of benefits. It does not describe or include all benefit provisions, limitations, exclusions, or qualifications for coverage. Please review plan documents for full details. If there
are any conflicts with information provided on this page, the plan documents will prevail.
24 City of Oakland | Full-Time and Permanent Part-Time EmployeesDental
When it comes to choosing a dental plan, you want benefits that fit the needs of you and your family. Delta Dental PPO
and DeltaCare USA both offer comprehensive dental coverage, quality care and excellent customer service. The City allows
non‑sworn full‑time and permanent part‑time employee and their eligible dependents to elect from one of the two plan
offerings.
DeltaCare USA Delta Dental PPO
Delta Care USA is our prepaid plan that features set Delta Dental PPO, our preferred provider organization
copayments, no annual deductibles and no maximums (PPO) plan, provides access to the largest PPO dentist
for covered benefits. In most states, enrollees must select network in the U.S. Delta Dental PPO dentists agree
a primary care dentist in the DeltaCare USA network to accept reduced fees for covered procedures when
from whom they receive treatment as in a traditional treating PPO patients. This means your out-of-pocket
dental HMO. costs are usually lower when you visit a PPO dentist than
when you visit a non-Delta Dental dentist, but you have
the freedom to visit any licensed dentist, anywhere in
the world.
The information described on this page is only intended to be a summary of benefits. It does not describe or include all benefit provisions, limitations, exclusions, or
qualifications for coverage. Please review plan documents for full details. If there are any conflicts with information provided on this page, the plan documents will prevail.
City of Oakland | Full-Time and Permanent Part-Time Employees 25Dental (continued)
DeltaCare USA Dental PPO
With the DeltaCare Plan, you receive care from your Although the percentages of Benefits are the same no
assigned dentist and are informed of copay amounts matter which dentist you choose, your out-of-pocket
ahead of time. expenses may be greater if you choose a non-Delta
Dental PPO Dentist.
Delta Dental PPO
Plan Benefits DeltaCare USA
In-Network Out-of-Network
General Plan Information
• Annual Deductible
– Individual $0 $25 $25
– Family $0 $75 $75
• Waived for Preventive N/A No No
• Annual Plan Maximum N/A $2,000 $2,000
• Lifetime Orthodontia Plan Maximum N/A $2,000 $2,000
Diagnostic and Preventive Services
• Diagnostic and Preventive $0 – $45 copay 100% 100%
• Oral Exams 100% covered 100% 100%
• Bitewing X-rays 100% covered 100% 100%
• Full Mouth X-rays 100% covered every 24 months 100% 100%
• Cleaning and Scaling 100% covered every six months 100% 100%
• Prophylaxis Treatments 100% covered every six months 100% 100%
• Fluoride Treatments 100% covered 100% 100%
• Space Maintainers $10 copay 100% 100%
$5 copay; limited to permanent
• Sealants 100% 100%
molars through age 15
Basic Services $0
• Basic $0 – $220 copay 100% 80%
• Oral Surgery (Extractions and
$0 – $90 copay 100% 80%
Other Surgical Procedures)
• Endodontic Treatment $0 – $220 copay 100% 80%
• Periodontic Treatment $0 – $195 copay 100% 80%
• Re-linings and Re-basings of
$0 – $35 copay 100% 80%
Existing Removable Dentures
• Repair or Re-cementing
of Crowns, Inlays, Onlays, $0 – $75 copay 100% 80%
Dentures or Bridgework
For more information on Delta Dental please visit deltadentalins.com.
To look up a dental provider please visit deltadental.com/DentistSearch/DentistSearchController.ccl.
The information described on this page is only intended to be a summary of benefits. It does not describe or include all benefit provisions, limitations, exclusions, or
qualifications for coverage. Please review plan documents for full details. If there are any conflicts with information provided on this page, the plan documents will prevail.
26 City of Oakland | Full-Time and Permanent Part-Time EmployeesDental (continued)
Delta Dental PPO
Plan Benefits DeltaCare USA
In-Network Out-of-Network
Major Services
• Major $0 – $195 copay 60% 60%
• Crowns, Jackets and
$0 – $195 copay 60% 60%
Cast Restorations
• TMJ Not covered Not covered Not covered
• Prosthodontic Benefits (Fixed
$0 – $195 copay 60% 60%
Bridges, Partial/Complete Dentures)
Not covered; see Not covered; see
• Implants Not covered
plan document plan document
Orthodontia Services
$0 – $2,000 copay; see plan
• Orthodontia 50% 50%
document for limitations
Covered; $0 – $2,000 copay
• Dependent Children Covered Covered
for children up to age 19
• Adults (and Covered Full‑time Covered; $0 – $2,000 copay for adults and
Covered Covered
Students, if eligible) dependent adult children over age 19
• Adult Lifetime Maximum N/A $2,000 $2,000
For more information on Delta Dental please visit deltadentalins.com.
To look up a dental provider please visit deltadental.com/DentistSearch/DentistSearchController.ccl.
The information described on this page is only intended to be a summary of benefits. It does not describe or include all benefit provisions, limitations, exclusions, or
qualifications for coverage. Please review plan documents for full details. If there are any conflicts with information provided on this page, the plan documents will prevail.
City of Oakland | Full-Time and Permanent Part-Time Employees 27Vision
The City offers a vision plan through VSP. The plan pays benefits and offers discounts for most vision care expenses you
incur while covered by the plan, subject to the maximum amounts shown below. Vision coverage is available for non‑sworn
full‑time and permanent part‑time employees and their eligible dependents. If you use VSP providers, your costs for most
services and materials are limited to the applicable copays. To find more information on VSP or to locate a provider, please
visit vsp.com.
Vision Service Plan
Plan Benefits
In-Network Out-of-Network
General Plan Information
• Exam $10 copay, combined with materials copay Up to $50 allowance
• Materials $10 copay, combined with materials copay Up to $70 allowance
Benefit Frequency
• Exam 12 months 12 months
• Lenses 12 months 12 months
• Frames 12 months 12 months
• Contacts 12 months 12 months
Covered Services
• Single Vision Lens Covered after copay Up to $50
• Bifocal Lens Covered after copay Up to $75
• Trifocal Lenses Covered after copay Up to $100
• Lenticular Covered after copay Up to $125
• Basic Progressive $50 copay Up to $75
Lens Options
• UV Coating $14 copay Not covered
• Tint (Solid and Gradient) 100% Up to $5
• Scratch Resistance $15 copay Not covered
$23 copay for single vision
• Basic Polycarbonate Not covered
$28 copay for multifocal
• Standard Anti-Reflective $37 copay Not covered
• Other Add-Ons and Services Discounts available Not covered
Contact Lenses
• Medically Necessary Covered after copay Up to $210 allowance
• Elective Up to $105 allowance Up to $105 allowance
• Frames Up to $105 allowance Up to $70 allowance
Other Services
• Corrective Vision Services (Laser Surgery) Discount available Not covered
• Second Pair of Glasses Discount available Not covered
The information described on this page is only intended to be a summary of benefits. It does not describe or include all benefit provisions, limitations, exclusions, or
qualifications for coverage. Please review plan documents for full details. If there are any conflicts with information provided on this page, the plan documents will prevail.
28 City of Oakland | Full-Time and Permanent Part-Time EmployeesYou can also read