Balanced appetite regulation of Shu-mu acupoint catgut embedding in abdominal obesity: secondary analysis of a randomized clinical trial
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Balanced appetite regulation of Shu-mu acupoint
catgut embedding in abdominal obesity: secondary
analysis of a randomized clinical trial
Xinghe Zhang
Yunnan University of Chinese Medicine
Qifu Li
Yunnan University of Chinese Medicine
Gaoyangzi Huang
Yunnan University of Chinese Medicine
Xianmei Pei
Yunnan University of Chinese Medicine
Xin Tang
Yunnan University of Chinese Medicine
Renrui Zhang
Yunnan University of Chinese Medicine
Rong Yi
Kunming Hospital of Traditional Chinese Medicine
Li Li
Kunming Hospital of Traditional Chinese Medicine
Chonghui Xing
The Sports Trauma Specialist Hospital of Yunnan Province
Siwen Zhao
Yunnan University of Chinese Medicine
Taipin Guo ( gtphncs@126.com )
Yunnan University of Chinese Medicine
Fanrong Liang
Chengdu University of Traditional Chinese Medicine
Research Article
Keywords: Acupoint catgut embedding, Abdominal obesity, Randomized controlled trial, Appetite
Posted Date: January 16th, 2023
DOI: https://doi.org/10.21203/rs.3.rs-2472273/v1
Page 1/14License: This work is licensed under a Creative Commons Attribution 4.0 International License.
Read Full License
Page 2/14Abstract
Objective
To explore the effect of Shu-mu acupoint catgut embedding (ACE) on appetite in abdominal obesity (AO)
patients.
Methods
This is a secondary analysis of a multicenter, double-blind, randomized controlled trial. Which was
conducted in China between July 2018 and June 2022. Eighty AO participants who received Shu-mu ACE
intervention were divided into moderate appetite (MA) and strong appetite (SA) subgroups, according to
the appetite at baseline. While 79 AO participants who received NACE intervention were also divided into
MA and SA subgroups. All participants were given a 12-week actual intervention period and a 4-week
follow-up. Appetite was assessed at baseline and after 6, 12 and 16 weeks.
Results
71 participants who received Shu-mu ACE and 74 participants who received NACE were included in the
final analysis. After the Shu-mu ACE, at 16 weeks, the appetite of the SA subgroup decreased to the same
level as the MA subgroup (p > 0.05). All 36 AO participants’ appetite had decreased in the SA subgroup.
While in the MA subgroup, 22 AO participants had a decrease in appetite, 7 increased, 4 had no change,
and 2 had appetite data missing. During the NACE intervention and follow-up, the appetite of the SA
subgroup was always higher than the MA subgroup (p < 0.01). In the SA subgroup, 32 decreased, 4
increased, 5 had no change, and 2 appetite data missing. While in the MA subgroup, 14 decreased, 7
increased, and 10 had no change.
Conclusions
Catgut embedding at Shu-mu acupoint could regulate the appetite of AO to the normal level, rather than
dramatically inhibit the appetite.
Trial registration This study was registered in the Chinese Clinical Trial Registry (registration number:
ChiCTR1800016947). 4 July 2018; https://www.chictr.org.cn/showproj.aspx?proj=28782
Introduction
Abdominal obesity (AO) is a major type of obesity characterized by abdominal fat accumulation. The AO
rate in China is about 29.1% and the prevalence increased rapidly [1–3]. The regulation of appetite is
Page 3/14considered an important way the control fat accumulation [4]. Keeping appetite at a normal level is a
reasonable and healthy way to treat AO.
Acupoint catgut embedding (ACE) is a special acupuncture therapy based on the meridian and acupoint
theory of Traditional Chinese Medicine (TCM). Stimulation of the acupoints could maintain the stability
of visceral function [5]. Shu-mu acupoint is the specific point where the Qi of viscera gathers in the chest
and back. Our team’s previous research has shown that Shu-mu ACE could reduce waist circumference,
body weight, and appetite in AO patients [6]. In this secondary analysis of the multicenter, randomized,
double-blind, controlled study, we examined the efficacy of Shu-mu ACE for AO patients with different
appetite from another angle. Exploring whether Shu-mu ACE has a dramatic inhibition effect on different
appetite.
Method
Study design
The foregone study was undertaken between July 2018 and March 2020, without the gender requirement
(n = 137). With the supplemented female samples (n = 22) between April 2020 and June 2022. Eighty AO
patients received Shu-mu ACE intervention and 79 AO participants received non-acupoints catgut
embedding (NACE) intervention. Finally, 71 participants (MA subgroup 35, SA subgroup 36) who received
Shu-mu ACE and 74 participants (MA subgroup 31, SA subgroup 43) who received NACE were included in
this secondary analysis. Every participant received a 12-week intervention period and a 4-week follow-up.
Appetite was measured at baseline, 6, 12, and 16 weeks after the intervention. Possible adverse events
were carefully monitored from 1 to 16 weeks. The flow chart was shown in Fig. 1.
This study was registered in Chinese Clinical Trial Registry (ChiCTR1800016947). Ethics was approved by
the Hospital Ethics Committee of Sports Trauma Specialist Hospital of Yunnan Province (2018CK-001).
All participants were fully informed and signed written informed consent forms.
Participant
All participants were recruited from the outpatient department in 4 Chinese clinical centers: Second
Affiliated Hospital of Yunnan University of Chinese Medicine, Kunming Hospital of Traditional Chinese
Medicine, Sports Trauma Specialist Hospital of Yunnan Province and ShengAi Hospital of Traditional
Chinese Medicine.
According to the diagnostic criteria of AO by Chinese Medical Association, waist circumference (WC) is
used to diagnose AO. In this study, the main inclusion criteria was: WC ≥ 90 cm in males and ≥ 85 cm in
females. The measurement method of WC: standing position, the circumference of the waist was
measured at the horizontal position of the lower costal edge of the midaxillary line and the midpoint of
the iliac crest line [7]. The second inclusion criteria included body mass index (BMI) ≥ 24 kg/m2, aged
between 18 and 60, and simply overweight or obese [8].
Page 4/14The exclusion criteria were: WC < 90 cm in males and < 85 cm in females, BMI < 24 kg/m2; secondary
obesity caused by medication or endocrine disease; pregnancy, lactation and childbirth within the past 6
months; chronic obstructive pulmonary disease, coronary heart disease, liver cirrhosis, nephritis and other
serious organ diseases; participants with severe mental and neurological diseases; hypertension without
effectively controlled; allergic to alcohol or catgut; received weight loss treatment within past 3 months.
Randomization and blinding
The randomization was computer generated by the Clinical Research Center of Yunnan University of
Chinese Medicine. Stratified randomization was performed in the 4 clinical centers. Opaque envelopes
with a random number were managed by an independent coordinator. Participants, inspector and analyst
were all blinded to the allocation. The acupuncturist performed the catgut embedding after the assistant
lays the drapes. Therefore, the acupuncturists were also blinded to the allocation.
Interventions
Participants received catgut embedding intervention every 2 weeks for 6 sessions. Catgut embedding
manipulations were performed by an acupuncturist with national medical qualifications. The acupoints
of the Shu-mu ACE group were Zhongwan (CV12), Tianshu (ST25), Zhangmen (LR13), Pishu (BL20),
Weishu (BL21) and Dachangshu (BL25). The non-acupoints were beside the acupoints, which were
labeled NA1 (1.5 cun to the left of the Zhongwan), NA2 (1 cun outward from the Tianshu), NA3 (2 cun
forward from the Zhangmen), NA4 (2 cun outward from the Pishu), NA5 (2 cun outward from the Weishu)
and NA6 (2 cun outward from the Dachangshu).
The assistant marked the position of acupoints and non-acupoints, conventionally disinfected the skin of
the operation area, and then layed the sterile drapes. Took the sterile medical catgut with a length of 1-
2cm (the length depends on the location of the acupoint), placed it on the front end of the trocar, then
connected the needle core, lifted the partial skin with the thumb and forefinger of one hand, pierced the
needle with another hand. When the piercing reached the desired depth, implanted the catgut in the
subcutaneous tissue or muscle layer. After the needle was removed, pressed the needle hole with a dry
cotton ball for half a minute to stop bleeding, and then pasted a bandage to protect the needle hole.
Participants were requested not to bathe for 24 hours and keep the embedding area dry.
The thread-embedded needle was 8# disposable needle (Jiangxi Glance Medical Equipment Co. Ltd.
Production, Nanchang, China). The medical catgut was an absorbable collagen line with the specification
of 2 − 0, 2 cm*20 length (Jiangxi Longteng Biotechnology co., LTD, Nanchang, China).
Participants’ diet and physical activity were not restricted during the whole course, they could continue
their lifestyle.
Outcome measures
Outcome measurements were performed at baseline, 6 and 12 weeks in the intervention period, and 16
weeks in follow-up. No eating or drinking for 2 hours before the test. The outcome of this secondary
Page 5/14analysis was the visual analogue scale (VAS) of appetite. Assessed appetite by VAS as reported in the
article [9]. As shown in Fig. 2, no appetite and minimal intake (0 score). Slight appetite and small amount
of intake (1–3 score). Moderate appetite and moderate intake (4–6 score). Strong appetite and large
intake (7–10 score).
Statistical analysis
All data were analyzed by SPSS (vers 28.0, SPSS Institute, Chicago, IL, USA) and GraphPad Prism (vers
7.0, GraphPad Software, San Diego, CA, USA). The outcomes described and baseline characteristics were
based on the intention-to-treat (ITT) population, which included participants who have received the whole
intervention. Continuous data were presented as the mean and standard deviation (SD). Categorical
variables were described as numbers and percentages. As the missing data were all in follow-up, the last
observation was carried forward and the expectation maximization method was not suitable. Therefore,
the missing data was disposed by listwise deletion. The significance level for the statistical analysis was
5% with 2-tailed testing.
Normality of continuous variables was determined by Shapiro-Wilk test, Kolmogorov-Smirnov test.
Homogeneity of continuous variables was determined by F test. Independent-Sample t-test was used
when compared between every two groups. One-way ANOVA test was used to compare the repeated
measurements (≥ 3) within the group. The χ2 test was performed to evaluate the significance of the
difference For the categorical data.
Results
Participants and baseline characteristics
Approximately 600 potential people were invited. After the initial screening, 159 participants (80 received
Shu-mu ACE and 79 received NACE) were submitted to the randomized process. However, a total of 71
participants (MA subgroup 35, SA subgroup 36) who received Shu-mu ACE and 74 participants (MA
subgroup 31, SA subgroup 43) who received NACE were included in the ITT population (Fig. 1). During all
interventions phases, 159 participants (100%) completed 6 treatments and 3 tests. Noted that 3
participants were unwilling to undergo follow-up. During the follow-up test, 1 participant had an
emergency and failed to complete the measure. Meanwhile, the recruiters mistakenly included 13
participants who were abdominal pre-obesity. The baseline characteristics were shown in Table 1.
Page 6/14Table 1
Baseline characteristics of 145 participants included in the ITT analysis
Baseline Characteristics Shu-mu ACE (n = 71) NACE (n = 74)
MA (n = 35) SA (n = 36) MA (n = 31) SA (n = 43)
Women, No. (%) 31 (88.57%) 27 (75.00%) 27 (87.10%) 38 (88.37%)
58 (81.69%) 65 (87.84%)
Age, mean (SD), y 36.77 (11.04) 34.17 (9.44) 36.48 (8.52) 34.77 (8.92)
35.45 (10.27) 35.49 (8.74)
Appetite, mean (SD) 5.57 (0.78) 7.86 (0.68) 5.42 (0.81) 8.07 (0.94)
6.73 (1.36) 6.96 (1.58)
Appetite outcomes
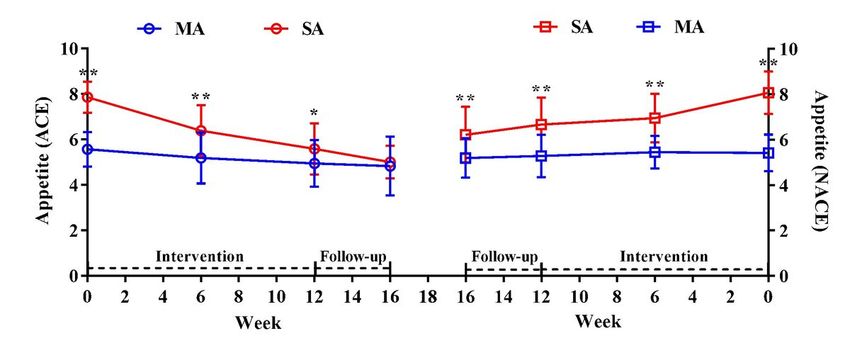
For the participant who received Shu-mu ACE intervention. At baseline and 6 weeks, the appetite of the SA
subgroup was significantly higher than the MA subgroup (p < 0.01). At 12 weeks, the appetite of the SA
subgroup was still higher than the MA subgroup (p < 0.05). At 16 weeks, the appetite of the SA subgroup
showed no significant difference from the MA subgroup (p > 0.05). During intervention and follow-up, the
appetite (7.86 ± 0.68) of the SA subgroup significantly decreased to the normal level (5.00 ± 0.72). All
participants’ appetite(100%) in the SA subgroup had decreased. Though the appetite (5.57 ± 0.78) of the
MA subgroup has also decreased (4.82 ± 1.24). The appetite was still at a normal level. What’s more, in a
total of 35 participants, 22 participants (62.86%) had a slight decrease, 7 participants’ appetite increased
(20.00%), 4 had no change (11.43%), and 2 had appetite data missing. The results were shown in Fig. 3
and Table 2.
Table 2
Changes in appetite of AO participants between 16 week and baseline
Intervention Subgroup Decreased Increased No Data Decreased
Change Missing Rate
Shu-mu ACE (n = MA (n = 22 7 4 2 62.86%
71) 35)
SA (n = 36 0 0 0 100.00%
36)
NACE (n = 74) MA (n = 14 7 10 0 45.16%
31)
SA (n = 32 4 5 2 74.42%
43)
For the participant who received NACE intervention. During the whole course, the appetite of the SA
subgroup was always higher than the MA subgroup (p < 0.01). In the SA subgroup, 32 AO participants
Page 7/14had a decrease in appetite (74.42%), 4 slightly increased (9.30%), 5 had no change (11.63), and 2 were
appetite data missing. The proportion of participants with decreased appetite was significantly lower
than that of Shu-mu ACE (p < 0.01). For the MA subgroup, 14 participants (45.16%) had a slight decrease
in appetite, 7 participants’ appetite increased (22.58%), and 10 had no change (32.26%). The proportion
of participants with decreased appetite was not significantly different from the Shu-mu ACE (p > 0.05).
Conclusion
Catgut embedding at Shu-mu acupoint could regulate the viscera function and balance appetite to the
normal level of AO. Rather than dramatically inhibiting the appetite. Catgut embedding at non-acupoint
could not stably regulate the appetite of AO.
Declarations
Acknowledgments The authors wish to thank the Human Resources & Social Security Department and
the Science & Technology Department of Yunnan Province for providing funding.
Author Contributions TPG and FRL designed this trial. CHX reviewed the ethics of the trial. QFL, GYZH,
XMP, XT and RRZ recruiting participants. XHZ managed the random numbers and kept them blind to
participants, inspectors, and analysts. QFL, SWZ and TPG performed the treatment. RY and LL detected
related indicators. QFL analyzed the data. XHZ and TPG conducted this manuscript. All authors reviewed
the article.
Funding This work was funded by the Yunnan Expert Workstation-Liang Fanrong Station (No.2018IC101),
Yunnan Province Ten-thousand Plan-Youth Special (No.YNWR-QNBJ-2019-257), Yunnan Provincial
Science Project (No.2017FF117-011, 2019FF002-021, 202101AZ070001-096) from the Human Resources
& Social Security Department and Science & Technology Department of Yunnan Province. The funding
bodies do not play any role in the design of the study, collection, analysis, or writing manuscripts.
Availability of data and materials Data will be available upon request from the corresponding author.
Conflict of Interest The authors declare that the research was conducted in the absence of any
commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Zhang LF, Wang ZW, Wang X, Chen Z, Shao L, Tian Y, Dong Y, Zheng C, Li S, Zhu M, Gao R, China
Hypertension Survey I (2019) Prevalence of abdominal obesity in china: Results from a cross-
sectional study of nearly half a million participants. Obesity (Silver Spring) 27(11):1898–1905.
https://doi.org/10.1002/oby.22620
2. Lyu Y, Jiang H, Zhang B, Wang H, Wang L, Jia X, Wang Z (2020) Trend of central obesity prevalence
among the farmers in nine provinces (autonomous region) of china and social-demographic
Page 8/14difference from 1993 to 2015. Wei Sheng Yan Jiu 49(3):357–373.
3. Hua J, Zhang L, Gao D, Huang Y, Ning P, Cheng P, Li Y, Hu G (2020) Prevalence of overweight and
obesity among people aged 18 years and over between 2013 and 2018 in hunan, china. Int J Environ
Res Public Health 17(11) https://doi.org/10.3390/ijerph17114048
4. Al-Khudairy L, Loveman E, Colquitt JL, Mead E, Johnson RE, Fraser H, Olajide J, Murphy M, Velho RM,
O'Malley C, Azevedo LB, Ells LJ, Metzendorf MI, Rees K (2017) Diet, physical activity and behavioural
interventions for the treatment of overweight or obese adolescents aged 12 to 17 years. Cochrane
Database Syst Rev 6:CD012691. https://doi.org/10.1002/14651858.CD012691
5. Wu Y, Yuan J, Feng XM (2011) [Effect of acupuncture-assisted anesthesia on stress response during
laparoscopic cholecystectomy in aged patients]. Zhongguo Zhen Jiu 31(2):155–157.
6. Zhang X, Li Q, Yi R, Xing C, Jin Y, Meng J, Zhao S, Liang F, Guo T (2022) Effect of acupoint catgut
embedding for abdominally obese female with strong appetite: Mixed analysis of a randomized
clinical trial. Diabetes Metab Syndr Obes 15:3387–3395.https://doi.org/10.2147/DMSO.S388485
7. Association CM (2020) Guideline for primary care of obesity:Practice version (2019). Chin J Gen
Pract 19(02):102–107.
8. Group COW (2004) Guidelines for the prevention and control of overweight and obesity in Chinese
adults (excerpt). Acta Nutrimenta Sinica (1):1–4.
9. Doucet E, Imbeault P, St-Pierre S, Almeras N, Mauriege P, Richard D, Tremblay A (2000) Appetite after
weight loss by energy restriction and a low-fat diet-exercise follow-up. Int J Obes Relat Metab Disord
24(7):906–914. https://doi.org/10.1038/sj.ijo.0801251
10. Krentz AJ, Fujioka K, Hompesch M (2016) Evolution of pharmacological obesity treatments: Focus
on adverse side-effect profiles. Diabetes Obes Metab 18(6):558–570.
https://doi.org/10.1111/dom.12657
11. MacLean PS, Wing RR, Davidson T, Epstein L, Goodpaster B, Hall KD, Levin BE, Perri MG, Rolls BJ,
Rosenbaum M, Rothman AJ, Ryan D (2015) Nih working group report: Innovative research to improve
maintenance of weight loss. Obesity (Silver Spring) 23(1):7–15. https://doi.org/10.1002/oby.20967
12. Yu EW, Lee MP, Landon JE, Lindeman KG, Kim SC (2017) Fracture risk after bariatric surgery: Roux-
en-y gastric bypass versus adjustable gastric banding. J Bone Miner Res 32(6):1229–1236.
https://doi.org/10.1002/jbmr.3101
13. Chen IJ, Yeh YH, Hsu CH (2018) Therapeutic effect of acupoint catgut embedding in abdominally
obese women: A randomized, double-blind, placebo-controlled study. J Womens Health (Larchmt)
27(6):782–790. https://doi.org/10.1089/jwh.2017.6542
14. Sheng J, Jin X, Zhu J, Chen Y, Liu X (2019) The effectiveness of acupoint catgut embedding therapy
for abdominal obesity: A systematic review and meta-analysis. Evid Based Complement Alternat
Med 2019:9714313. https://doi.org/10.1155/2019/9714313
15. Ren XY (2004) Discussion on the origin and mechanism of acupoint embedding. Chi J Med
19(12):757–759.
Page 9/1416. Li Y, Zheng H, Zeng F, Zhou SY, Zhong F, Zheng HB, Chen M, Jing XH, Cai YY, Jia BH, Zhu B, Liu ZS
(2012) Use acupuncture to treat functional constipation: Study protocol for a randomized controlled
trial. Trials 13:104. https://doi.org/10.1186/1745-6215-13-104
17. Sun QH, Li TT, Huang MT, Wang MY, Xiao X, Bai XH (2020) Acupoint selection rules in treating
gastroesophageal reflux disease with acupuncture in china based on data mining. Zhongguo Zhen
Jiu 40(12):1374–1378. https://doi.org/10.13703/j.0255-2930.20191107-0003
18. Zheng H, Li Y, Zhang W, Zeng F, Zhou SY, Zheng HB, Zhu WZ, Jing XH, Rong PJ, Tang CZ, Wang FC,
Liu ZB, Wang SJ, Zhou MQ, Liu ZS, Zhu B (2016) Electroacupuncture for patients with diarrhea-
predominant irritable bowel syndrome or functional diarrhea: A randomized controlled trial. Medicine
(Baltimore) 95(24):e3884. https://doi.org/10.1097/MD.0000000000003884
19. Zheng H, Liu ZS, Zhang W, Chen M, Zhong F, Jing XH, Rong PJ, Zhu WZ, Wang FC, Liu ZB, Tang CZ,
Wang SJ, Zhou MQ, Li Y, Zhu B (2018) Acupuncture for patients with chronic functional constipation:
A randomized controlled trial. Neurogastroenterol Motil 30(7):e13307.
https://doi.org/10.1111/nmo.13307
20. Kalarchian MA, Levine MD, Arslanian SA, Ewing LJ, Houck PR, Cheng Y, Ringham RM, Sheets CA,
Marcus MD (2009) Family-based treatment of severe pediatric obesity: Randomized, controlled trial.
Pediatrics 124(4):1060–1068. https://doi.org/10.1542/peds.2008-3727
21. Apovian CM, Aronne LJ, Bessesen DH, McDonnell ME, Murad MH, Pagotto U, Ryan DH, Still CD
(2015) Pharmacological management of obesity: An endocrine society clinical practice guideline. J
Clin Endocrinol Metab 100(2):342–362. https://doi.org/10.1210/jc.2014-3415
22. Morton GJ, Meek TH, Schwartz MW (2014) Neurobiology of food intake in health and disease. Nat
Rev Neurosci 15(6):367–378. https://doi.org/10.1038/nrn3745
23. Raka F, Farr S, Kelly J, Stoianov A, Adeli K (2019) Metabolic control via nutrient-sensing mechanisms:
Role of taste receptors and the gut-brain neuroendocrine axis. Am J Physiol Endocrinol Metab
317(4):E559-e572. https://doi.org/10.1152/ajpendo.00036.2019
24. Han H, Yi B, Zhong R, Wang M, Zhang S, Ma J, Yin Y, Yin J, Chen L, Zhang H (2021) From gut
microbiota to host appetite: Gut microbiota-derived metabolites as key regulators. Microbiome
9(1):162. https://doi.org/10.1186/s40168-021-01093-y
25. Higgs S, Spetter MS, Thomas JM, Rotshtein P, Lee M, Hallschmid M, Dourish CT (2017) Interactions
between metabolic, reward and cognitive processes in appetite control: Implications for novel weight
management therapies. J Psychopharmacol 31(11):1460–1474.
https://doi.org/10.1177/0269881117736917
26. de Wouters d'Oplinter A, Rastelli M, Van Hul M, Delzenne NM, Cani PD, Everard A (2021) Gut microbes
participate in food preference alterations during obesity. Gut Microbes 13(1):1959242.
https://doi.org/10.1080/19490976.2021.1959242
27. Pan B, Castro-Lopes JM, Coimbra A (1996) Activation of anterior lobe corticotrophs by
electroacupuncture or noxious stimulation in the anaesthetized rat, as shown by colocalization of
Page 10/14fos protein with ACTH and beta-endorphin and increased hormone release. Brain Res Bull 40(3):175–
182. https://doi.org/10.1016/0361-9230(96)00011-1
28. Eshkevari L, Permaul E, Mulroney SE (2013) Acupuncture blocks cold stress-induced increases in the
hypothalamus-pituitary-adrenal axis in the rat. J Endocrinol 217(1):95–104.
https://doi.org/10.1530/JOE-12-0404
29. Eshkevari L, Mulroney SE, Egan R, Lao L (2015) Effects of acupuncture, ru-486 on the hypothalamic-
pituitary-adrenal axis in chronically stressed adult male rats. Endocrinology 156(10):3649–3660.
https://doi.org/10.1210/EN.2015-1018
30. Guojie Z, Heping H, Shuju W, Xuping W, Yanjun D, Lihong K (2008) Research on the mechanism of
action in regulation blood pressure of rats with different status by acupuncture. Chine J Rehab.
(01):5–7.
31. Tatewaki M, Harris M, Uemura K, Ueno T, Hoshino E, Shiotani A, Pappas TN, Takahashi T (2003) Dual
effects of acupuncture on gastric motility in conscious rats. Am J Physiol Regul Integr Comp Physiol
285(4):R862-872. https://doi.org/10.1152/ajpregu.00715.2002
Figures
Page 11/14Figure 1
Flowchart of the screening, enrollment, randomization, and follow-up.
Page 12/14Figure 2
Visual analogue scale (VAS) of appetite.
In the assessment of appetite, integer was taken.
Figure 3
Appetite during the treatment and follow-up.
Page 13/14Data were presented as mean (SD). Independent-Sample t-test was used when compared between every two groups. One-way ANOVA test was used to compare the repeated measurements within the group. **p
You can also read