Avacopan, a selective C5a receptor antagonist, for anti-neutrophil cytoplasmic antibody-associated vasculitis - Oxford Academic
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Modern Rheumatology, 00, 2022, 1–9
DOI: https://doi.org/10.1093/mr/roab104
Advance Access Publication Date: 4 January 2022
Invited Review Article Submission
Avacopan, a selective C5a receptor antagonist, for
anti-neutrophil cytoplasmic antibody-associated vasculitis
Masayoshi Harigai* and Hideto Takada
Downloaded from https://academic.oup.com/mr/advance-article/doi/10.1093/mr/roab104/6497529 by guest on 14 January 2022
Division of Rheumatology, Department of Internal Medicine, Tokyo Women’s Medical University School of Medicin, Tokyo, Japan
*Correspondence: Masayoshi Harigai; harigai.masayoshi@twmu.ac.jp; Division of Rheumatology, Department of Internal Medicine, Tokyo Women’s Medical
University School of Medicine, 8-1 Kawada-cho, Shinjuku-ku, Tokyo 162-8666, Japan.
ABSTRACT
Avacopan, an orally administered C5a receptor antagonist, has been approved for the treatment of microscopic polyangiitis (MPA) and granu-
lomatosis with polyangiitis (GPA) in Japan and the USA. In ADVOCATE Phase III clinical trial, patients with active MPA or GPA received either
30 mg avacopan twice daily or prednisone on a tapering schedule in combination with rituximab or cyclophosphamide (followed by azathioprine).
The trial met its two primary endpoints: avacopan showed non-inferiority to prednisone for achieving remission at Week 26 (avacopan, 72.3%;
prednisone, 70.1%; p < .001 for non-inferiority and p = .24 for superiority) and superiority for maintaining remission at Week 52 (65.7% for ava-
copan, 54.9% prednisone, p < .001 for non-inferiority and p = .007 for superiority). Of several key secondary endpoints tested, the glucocorticoid
toxicity index (GTI)-cumulative worsening score and GTI-aggregate improvement score were significantly lower in the avacopan group than in
the prednisone group at both Weeks 26 and 52. Serious adverse events related and unrelated to the worsening vasculitis were reported at
10.2% and 37.3% in the avacopan group and at 14.0% and 39.0% in the prednisone group, respectively. Avacopan has set the stage for the
semi-glucocorticoid-free or glucocorticoid-free treatment of MPA and GPA.
KEYWORDS: Avacopan; anti-neutrophil cytoplasmic antibody-associated vasculitis; clinical trial; targeted therapy
Introduction are presented, and the clinical implications of the drug are
Anti-neutrophil cytoplasmic antibody (ANCA) associated discussed.
vasculitis (AAV) is characterized by the presence of ANCA
in the sera of patients and various organ involvements due
Targeted therapies of MPA and GPA
to damage to small vessels (i.e. capillaries, venules, and arte-
rioles) [1]. AAV comprises microscopic polyangiitis (MPA), The first targeted therapy approved for MPA and GPA was
granulomatosis with polyangiitis (GPA), and eosinophilic RTX. The efficacy and safety of RTX have been demon-
granulomatosis with polyangiitis. Since MPA and GPA share strated in clinical trials on MPA and GPA [6, 7], lead-
several relevant clinical characteristics, clinical trials for devel- ing to approval of the drug for the diseases in Japan, the
oping a new drug have been implemented for these two USA, and Europe. Avacopan is the second targeted ther-
diseases. Current Japanese clinical practice guidelines for apy approved for MPA and GPA in Japan and the USA and
MPA and GPA [2] and those overseas [3, 4] recommend the European Medical Agency has recommended granting a
cyclophosphamide (CY) or rituximab (RTX) with concomi- marketing authorization in the European Union. Avacopan
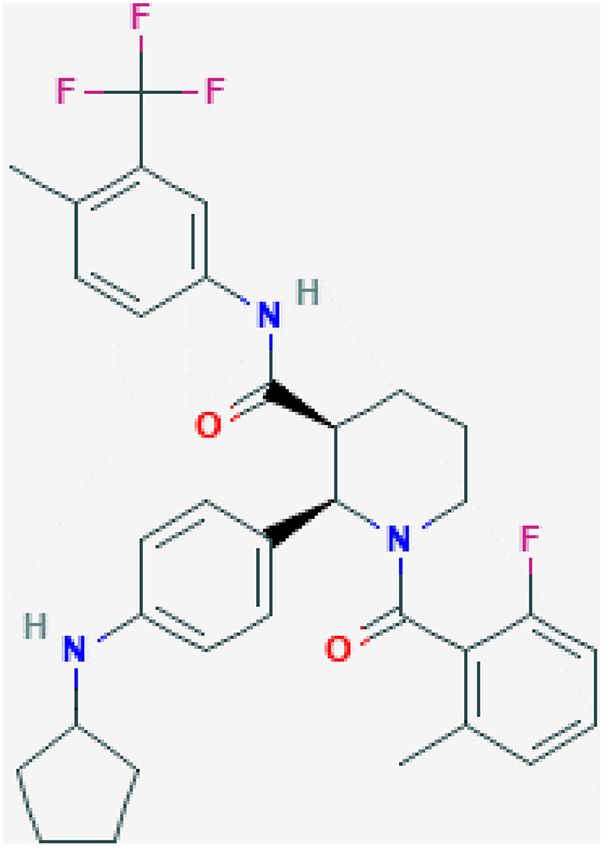
tant glucocorticoids (GCs) for remission induction therapy (C33 H35 F4 N3 O2 ) has a molecular weight of 581.6; its struc-
and azathioprine (AZA) or RTX for remission maintenance ture is shown in Figure 1. As of 14 November 2021, five
therapy. However, some patients with MPA and GPA do targeted therapies for MPA and GPA are under clinical devel-
not achieve remission with these treatments or have relapse opment: tocilizumab, vilobelimab, abatacept, belimumab,
of the disease during treatment, and the long-term use of and tofacitinib (Table 1). Tocilizumab is a monoclonal anti-
concomitant GCs may result in adverse drug reactions lead- IL-6 receptor antibody developed by Chugai Pharmaceuti-
ing to a considerable decline in quality of life. Hence, a cal Co., Ltd. and F. Hoffmann-La Roche Ltd. That has
novel targeted therapy that has the potential to achieve GC- been approved for the treatment of rheumatoid arthritis,
free or semi-GC-free treatment of AAV has been eagerly other autoimmune diseases, and cytokine release syndrome of
awaited. chimeric antigen receptor T-cell therapy. A clinical trial com-
A series of complement-based therapies have been under paring tocilizumab and CY in combination with GCs is being
investigation for various renal diseases [5]. Consequently, performed in Japan [8]. Vilobelimab is an anti-C5a mono-
avacopan, an orally administered antagonist to the C5a recep- clonal antibody; its efficacy and safety versus placebo for MPA
tor (C5aR or CD88), has been approved in Japan and the and GPA are under investigation by InflaRx GmbH (https://
USA for the treatment of MPA and GPA. In this review, clinicaltrials.gov/ct2/show/NCT03712345?cond=Microsco-
basic and clinical evidence of avacopan in MPA and GPA pic+Polyangiitis&draw=2&rank=2). Abatacept, a selective
Received 27 October 2021; Accepted 19 November 2021
© Japan College of Rheumatology 2022. Published by Oxford University Press. All rights reserved. For permissions, please e-mail:
journals.permissions@oup.com2 Harigai and Takada
of tofacitinib, a Janus kinase inhibitor, and an RCT ver-
sus MTX are being performed in China (https://clinical
trials.gov/ct2/show/NCT04973033?term=ANCA-associated
+vasculitis&draw=4&rank=24, https://clinicaltrials.gov/ct
2/show/NCT04944524?term=ANCA-associated+vasculitis
&draw=2&rank=84).
Roles of complements in MPA and GPA
Historically, the contribution of the complement system
to AAV development has been considered trivial. This is
Downloaded from https://academic.oup.com/mr/advance-article/doi/10.1093/mr/roab104/6497529 by guest on 14 January 2022
because the histopathology of ANCA-associated glomeru-
lonephritis is characterized by a paucity of immunoglobu-
lin and complement depositions, and hypocomplementemia
is rarely observed in patients with AAV. However, in the
past two decades, advances in research have elucidated that
the complement system plays a crucial role in the patho-
genesis of AAV. The establishment of a murine model for
anti-myeloperoxidase (MPO) antibody-induced necrotizing
crescentic glomerulonephritis (NCGN) has paved the way
for subsequent studies [9]. In this disease model, the injec-
tion of anti-MPO IgG derived from MPO knockout mice
immunized with murine MPO into wild-type mice induced a
pauci-immune NCGN.
Studies using this experimental model showed that the
genetic deletion of C5 or a C5-inhibiting monoclonal antibody
prevented anti-MPO antibody-induced NCGN, revealing a
pivotal role of complement C5 in the development of AAV
[10, 11]. Moreover, the alternative complement pathway acti-
vation, but not the classic or lectin pathways, is essential in
Figure 1. Structure of avacopan. the development of NCGN [10]. In this study, the role of the
Source: National Center for Biotechnology Information (2021). PubChem three different complement activation pathways was explored
Compound Summary for CID 49841217, Avacopan Retrieved 12 July 2021
using mice deficient in the classic and lectin pathway compo-
(https://pubchem.ncbi.nlm.nih.gov/compound/Avacopan).
nent C4 and the alternative pathway component factor B. As a
result, factor B knockout abrogated NCGN, while C4 knock-
out mice developed diseases comparable to those in wild-type
costimulation modulator, is being compared with placebo mice. The pathogenic role of alternative complement pathway
to achieve sustained GC-free remission in patients with activation was supported by a subsequent human study show-
relapsing non-severe GPA (https://clinicaltrials.gov/ct2/show/ ing that patients with active AAV had higher levels of plasma
NCT02108860?term=abatacept&cond=ANCA-associated Bb than those in remission [12].
+vasculitis&draw=1&rank=2). A Phase 2 study inves- The complement C5 is cleaved by the C5 convertase into
tigating the efficacy of co-administration of RTX and C5a, a smaller fragment with chemotactic and anaphyla-
belimumab, a monoclonal antibody against B-cell activat- toxin properties, and C5b, a larger fragment that forms the
ing factor/B lymphocyte stimulator, compared to RTX and C5b-9 membrane attack complex. Studies using knockout
placebo in Proteinase3 (PR3) ANCA-positive patients with mice demonstrated that the interaction of C5a and C5aR on
AAV is currently recruiting participants (https://clinicaltrials. myeloid cells, but not the C5b-9 membrane attack complex,
gov/ct2/show/NCT03967925?term=ANCA-associated+vasc was crucial for anti-MPO antibody-induced NCGN [13, 14].
ulitis&draw=4&rank=27). An open-label, single-arm study C5a serves as a chemoattractant for neutrophils and primes
Table 1. Targeted therapies for MPA and GPA.
Drug Mechanism of action Development phase
Rituximab Anti-CD20 chimera antibody Approved
Avacopan C5a receptor antagonist Approved
Tocilizumab Anti-interleukin-6 receptor monoclonal antibody Phase 2
Vilobelimab Anti-C5a monoclonal antibody Phase 2
Abatacept Cytotoxic T-lymphocyte-associated antigen 4-Fc portion of immunoglobulin G1 Phase 3
fusion protein, a selective costimulation modulator
Belimumab Anti B-cell activating factor/B lymphocyte stimulator monoclonal antibody Phase 2
Tofacitinib Janus kinase inhibitor Pilot study, Phase 4
Clinical trials registered in ClinicalsTraial.gov were tabulated as of September 2021.Avacopan for anti-neutrophil cytoplasmic antibody-associated vasculitis 3
them for subsequent ANCA-induced activation by upregulat- avacopan. Mild to moderate liver dysfunction (i.e. Child-
ing the surface expression of ANCA antigens (i.e. MPO and Pugh A or B) modestly increased Cmax and AUC0–∞ (both
PR3) [13]. The binding of ANCA to these antigens induces the parameters 30 red blood
pan is mediated through the blockade of C5a—C5aR inter- cells per high power field or >2+ by urine dipstick) plus
actions, inhibiting neutrophil recruitment and activation at albuminuria (at least 0.5 g/g creatinine) for Steps 1 and 2,
inflammatory sites. or at least one major or three non-major items, or at least
two renal items on the Birmingham Vasculitis Activity Score
Metabolism (BVAS) version 3 for Step 3. Patients with severe disease
In Phase 1 avacopan clinical trial involving 48 healthy vol- (i.e. rapidly progressive glomerulonephritis, alveolar haemor-
unteers (24 men and 24 women), 35 received avacopan and rhage leading to Grade 3 hypoxia, rapid-onset mononeuritis
13 received placebo [17]. Avacopan at 1–100 mg per dose multiplex, or central nervous involvement) were excluded.
was well tolerated. The mean maximal plasma levels (Cmax) The original primary objective was to assess the safety of
after the 7-day administration of avacopan at 30 mg twice avacopan, and the efficacy endpoint was added to the pro-
daily was 191 ng/mL (328 nM), followed by a long termi- tocol after the completion of Steps 1 and 2 with satisfactory
nal phase with a half-life of 129 h and an area under the results. The primary endpoint of CLEAR was the proportion
curve (AUC) of 5710 ng∙h/mL. The steady-state mean trough of patients with a treatment response at Week 12, defined
concentration at 12 h after dosing was 36 ng/mL (61 nM) as a BVAS decrease from baseline of at least 50% plus the
on Day 7 with avacopan dosed at 30 mg twice daily. Phar- absence of worsening in any body system of BVAS in the
macokinetics in eight Japanese patients were as follows and intention-to-treat population. Avacopan was considered non-
similar to those of the Phase 1 study in Switzerland; the mean inferior to the control if the lower bound of the one-sided
maximal plasma levels reached 246.6 ng/mL after the admin- 95% confidence interval (CI) for the difference in the primary
istration of avacopan at 30 mg twice daily for 7 days [18]. The endpoint (avacopan minus control) was >−0.20 and consid-
effects of low-fat and high-fat diets on Cmax were modest but ered superior to the control if the lower bound was >0.0.
AUC0–∞ moderately increased (2.11-fold after low-fat diet The results from all three steps were combined to conduct
and 1.72-fold after high-fat diet). Avacopan possessed pro- the primary analysis according to the prespecified statistical
tein binding rates of ≥99.9% to human serum albumin and plan.
α1-acid glycoprotein, and its M1 active metabolite showed In Steps 1 and 2, all patients received five intravenous
similar high protein binding rates in vitro. Avacopan mainly infusions of CY (IVCY) on Day 1 and at Weeks 2, 4, 8,
metabolized via CYP3A4 together with CYP2D6, 2C19, 2C8, and 12, followed by AZA at a target dose of 2 mg/kg/day
and 2B6. M1 showed a pharmacological activity similar to from Weeks 14 to 24. In Step 3, all patients received either
that of avacopan. Approximately 10% of [14 C]-avacopan IVCY followed by AZA, as in Steps 1 and 2, or rituximab
was excreted in the urine and 77% in the faeces. The pro- 375 mg/m2 per week for four consecutive weeks. Patients were
portions of unmetabolized avacopan in the urine and faeces allocated to the treatment arms in each step as follows: Step 1,
were 0.1% and 7%, respectively. In 368 patients, includ- placebo plus 60 mg prednisone (control) or avacopan 30 mg
ing 51 Japanese patients, mild to moderate renal dysfunction twice daily plus 20 mg prednisone at a 1:2 ratio; Step 2, con-
did not show a significant effect on the pharmacokinetics of trol or avacopan 30 mg twice daily plus placebo prednisone4 Harigai and Takada
Table 2. Main demographic and clinical characteristics at baseline in CLEAR.
Placebo plus 60 mg prednisone Avacopan plus 20 mg prednisone Avacopan without prednisone
Characteristics (n = 23) (n = 22) (n = 22)
Number of patients per step
Step 1 4 8 0
Step 2 6 0 8
Step 3 13 14 14
Age, years 59.1 ± 14.0 57.0 ± 14.2 57.4 ± 14.0
Men/women, no. 17/6 14/8 16/6
Duration of vasculitis, months 0 (0–162) 0 (0–61) 1 (0–108)
Disease history, no. (%)
Downloaded from https://academic.oup.com/mr/advance-article/doi/10.1093/mr/roab104/6497529 by guest on 14 January 2022
Newly diagnosed 18 (78) 15 (68) 16 (73)
Relapsed disease 5 (22) 7 (32) 6 (27)
ANCA type, no. (%)
MPO-ANCA 10 (43) 12 (55) 13 (59)
PR3-ANCA 11 (48) 10 (45) 8 (36)
Double positive 1 (4) 0 0
ANCA equivocal or negative 1(4) 0 1(5)
Disease type, no. (%)
GPA 10 (44) 11 (50) 12 (55)
MPA 12 (52) 11 (50) 10 (45)
Unknown 1 (4) 0 0
Disease assessment scores
BVAS 13.2 ± 5.8 14.3 ± 6.0 13.8 ± 6.4
VDI 1.2 ± 1.4 0.9 ± 1.5 0.5 ± 1.2
Plus–minus values are mean ± standard deviation.
BVAS version 3 (range 0–63) was used for assessing vasculitis disease activity.
Reproduced with permission from the J Am Soc Nephrol 2017;28:2756–67 [22].
at a 1:2 ratio; Step 3, control, avacopan 30 mg twice daily group, one in the avacopan plus 20 mg prednisone group, and
plus 20 mg prednisone and avacopan 30 mg twice daily plus three in the avacopan without prednisone group.
placebo prednisone at a 1:1:1 ratio. The main demographic
and clinical characteristics and the number of patients at Phase III clinical trial: ADVOCATE
each step of the treatment arm are summarized in Table 2. ADVOCATE Phase III, randomized, double-dummy,
The mean age was 57–59 years; 70.1% of the patients were active-controlled, multicentre, international clinical trial
male; 73% of the patients were newly diagnosed with MPA demonstrated the efficacy and safety of avacopan in combi-
or GPA, 54% and 45% were positive for MPO-ANCA and nation with CY followed by AZA or in combination with
PR3-ANCA, respectively (one patient was double positive), RTX, the standard remission induction treatment of MPA and
GPA and MPA were noted in 49% each, 97% had renal GPA [19]. The major inclusion criteria of ADVOCATE were
involvement, and BVAS at baseline was 13.2–14.3. as follows: (1) clinical diagnosis of GPA or MPA, consistent
The proportions of patients who achieved the primary end- with the Chapel-Hill Consensus Conference definitions; (2)
point were 70% in the control group, 86.4% in the avacopan age of at least 18 years, with newly diagnosed or relapsed
plus 20 mg prednisone group, and 81% in the avacopan with- AAV where treatment with CY or RTX is needed; (3) a pos-
out prednisone group (Table 3). Both avacopan groups met itive test for PR3- or MPO-ANCA; (4) at least one major
the prespecified non-inferiority criteria (p = .002 for avaco- item, at least three minor items, or at least two renal items
pan plus 20 mg prednisone group and p = .01 for avacopan of proteinuria and haematuria in the BVAS version 3.0; (5)
without prednisone group). In the subgroup analysis, similar eGFR ≥ 15 mL/min/1.73 m2 (using Modification of Diet in
responses to avacopan were observed. The mean percent- Renal Disease method) at screening; and (6) willingness and
age decrease in BVAS at Week 12 was −56% in the control ability to provide written informed consent for the require-
group, −79% in the avacopan plus 20 mg prednisone group, ments of the study protocol. The major exclusion criteria were
and −73% in the avacopan without prednisone group. Uri- as follows: (1) pregnancy or breastfeeding; (2) alveolar haem-
nary albumin-to-creatinine ratio (UACR) at Weeks 4 and 8 orrhage requiring invasive pulmonary ventilation support; (3)
in both avacopan groups and Week 12 in the avacopan plus diagnosis of any other known multi-system autoimmune dis-
20 mg prednisone group improved significantly compared to ease; (4) dialysis or plasma exchange within 12 weeks before
the control group. In the 12-week treatment period, two screening; (5) kidney transplantation; (6) treatment of CY
patients (9%) in each treatment arm had Grade 3 or higher within 12 weeks before the screening, or RTX or other anti-
adverse events (AEs). Four (17%), three (14%), and eight B-cell antibodies with 52 weeks of screening or 24 weeks
(36%) patients had serious AEs and two (9%), one (5%), and provided CD19+ cell counts were ≥0.5 × 109 /L.
three (14%) patients had worsening of vasculitis as AE or seri- The two primary endpoints were as follows: (1) pro-
ous AE (SAE) in the control, avacopan plus 20 mg prednisone, portion of subjects achieving disease remission at Week 26
and avacopan without prednisone groups, respectively. Seri- and (2) proportion of subjects achieving sustained disease
ous infection was reported in one patient in each treatment remission at Week 52. Disease remission at Week 26 was
arm. No Grade 3 lymphopenia was observed in the control defined as achieving a BVAS version 3.0 of 0 at Week 26Avacopan for anti-neutrophil cytoplasmic antibody-associated vasculitis 5
Table 3. Efficacy results at Week 12 in CLEARa .
Placebo plus 60 mg prednisone Avacopan plus 20 mg prednisone Avacopan without prednisone
Characteristics (n = 23) (n = 22) (n = 22)
Treatment responseb at Week 12, no 14 (70.0) 19 (86.4) 17 (81.0)
(%)
Difference in percentage compared to Reference 16.4 (−4.3 to 37.1) 11.0 (−11.0 to 32.9)
control (two-sided 90% CI)
BVAS
Actual 5.0 ± 1.6 2.6 ± 0.7 3.6 ± 1.1
% change −56 ± 14 −79 ± 5 −73 ± 7
VDI
Downloaded from https://academic.oup.com/mr/advance-article/doi/10.1093/mr/roab104/6497529 by guest on 14 January 2022
Actual 1.8 ± 0.4 1.2 ± 0.3 0.8 ± 0.3
% change 0.7 ± 0.2 0.3 ± 0.1 0.2 ± 0.1
BVAS = 0, no. (%) 8 (40) 10 (45) 7 (33)
Renal responsec , number of patients 20 18 18
Renal response, no. (%) 8 (40) 10 (56) 6 (33)
UACR (milligrams per gram creati- 20 22 20
nine) in patients with albuminuria
at baseline, number of patients
At baseline 318 279 280
At Week 12 252 127 158
% change −21 −56d −43
eGFR, mL/min/1.73 m2
At baseline 47.2 ± 3.5 52.5 ± 5.7 54.8 ± 4.4
At Week 12 52.8 ± 3.6 56.2 ± 4.3 56.1 ± 5.2
% change 5.6 ± 2.3 6.0 ± 2.3 0.8 ± 2.2
Urinary red blood cell count (cells 20 20 19
per HPF) in patients with haema-
turia at baseline, number of
patients
At baseline 22 26 17
At Week 12 2 5 3
% change −92 −83 −85
BVAS version 3 (range, 0–63) was used for assessing vasculitis disease activity.
Reproduced with permission from the J Am Soc Nephrol 2017;28:2756–67 [22].
a
Plus-minus values are mean ± SEM; UACR actual values are geometric means; and percentage change from baseline are ratios of geometric means of visit
over baseline. Number of patients per group for each end point is as indicated in the first row unless otherwise indicated.
b
Primary end point: treatment response on the basis of BVAS decrease of at least 50% from baseline and no worsening in any body system. Avacopan plus
20 mg prednisone group was statistically non-inferior to control (p = 0.002) and avacopan without prednisone was also non-inferior to control (p = 0.01).
c
Renal response was assessed in patients with hematuria and albuminuria at baseline, and was defined as an improvement in renal parameters, i.e., an increase
in eGFR, a decrease in urinary red blood cell count, and a decrease in UACR.
d
p < 0.01 for comparison of avacopan versus control.
and not taking GCs for treatment of AAV within 4 weeks at Day 1 and Weeks 2, 4, 7, 10, and 13), or oral CY
before Week 26. Sustained remission at Week 52 was defined (2 mg/kg/day as a target dose) at the discretion of the site
as remission at Week 26 without relapse to Week 52 and investigators. Patients who received IVCY or oral CY started
achieving a BVAS of 0 without taking GCs for treatment AZA at a target dose of 2 mg/kg/day from Week 15 onwards.
of AAV within 4 weeks before Week 52. Secondary efficacy Patients who received RTX did not receive AZA or other
measures included the GTI, early remission, Short Form-36 immunosuppressants. The avacopan group received 30 mg
version 2 (SF-36), EuroQOL-5D-5L (EQ-5D-5L), relapse, of avacopan twice daily orally plus prednisone-matching
eGFR, UACR, urinary monocyte chemoattractant protein-1 placebo, while the prednisone group received a tapering oral
(MCP-1)-to-creatinine ratio, and the Vasculitis Damage Index regimen of prednisone plus avacopan-matching placebo in a
(VDI). The sample size was calculated to provide at least 90% double-dummy design. GC treatment was allowed in the 14-
power to show the non-inferiority of avacopan to prednisone day screening period and had to be tapered to 20 mg/day
regarding the primary endpoint of remission at Week 26, with or less of prednisone equivalent before entering the trial,
an assumption of a non-inferiority margin of −20 percentage and this open-label GC treatment was further tapered to
points and an incidence of remission in the prednisone group discontinuation by the end of Week 4 of the trial. The
of 60%. To avoid Type I error, non-inferiority at Week 26 prednisone-tapering schedule in the prednisone group in this
was analysed first in the modified intention-to-treat popula- study is shown in Table 4.
tion, followed by non-inferiority at Week 52, superiority at The selected characteristics of the enrolled patients were
Week 52, and superiority at Week 26. No interim analysis well balanced (Table 5). Of the 330 enrolled patients, 21 were
was performed. Japanese. The mean age was 61 years, 54–59% of the patients
Patients were randomized at 1:1 ratio to either the ava- were male, 69–70% of the patients had newly diagnosed AAV,
copan or prednisone group, and all patients received RTX 57% were positive for MPO-ANCA, 45% had MPA, and
(375 mg/m2 at Day 1 and Weeks 1, 2, and 3), IVCY (15 mg/kg 81–82% had renal involvement. The mean BVAS score was6 Harigai and Takada
Table 4. Tapering schedule of prednisone in the prednisone group of Table 5. Selected demographic and clinical characteristics at baseline of
ADVOCATE. the patients in ADVOCATE.
Prednisone (adult) Avacopan Prednisone
Characteristic (n = 166) (n = 164)
Body weight ≥55 kgAvacopan for anti-neutrophil cytoplasmic antibody-associated vasculitis 7
Table 6. Primary and selected key secondary endpointsa of ADVOCATE.
End point Avacopan (n = 166) Prednisone (n = 164) Difference (95% CI)
Primary endpoints
Remission at Week 26, %b 72.3 70.1 3.4 (−6.0 to 12.8)c,d
Sustained remission at Week 52, %e 65.7 54.9 12.5 (2.6 to 22.3)c,f
Secondary endpoints
GTI-CWS at Week 26g
Patients evaluated 154 153
Least-squares mean 39.7 ± 3.4 56.6 ± 3.4 −16.8 (−25.6 to −8.0)
GTI-AIS at Week 26h
Downloaded from https://academic.oup.com/mr/advance-article/doi/10.1093/mr/roab104/6497529 by guest on 14 January 2022
Patients evaluated 154 153
Least-squares mean 11.2 ± 3.5 23.4 ± 3.5 −12.1 (−21.1 to −3.2)
Change in eGFR from baseline to Week 26i
Patients evaluated 121 127
Least-squares mean, mL/min/1.73 m2 5.8 ± 1.0 2.9 ± 1.0 2.9 (0.1 to 5.8)
Change in eGFR from baseline to Week 52i
Patients evaluated 119 125
Least-squares mean, mL/min/1.73 m2 7.3 ± 1.0 4.1 ± 1.0 3.2 (0.3 to 6.1)
Change in SF-36 physical component score from baseline
to Week 26
Patients evaluated 153 147
Least-squares mean 4.45 ± 0.73 1.34 ± 0.74 3.10 (1.17 to 5.03)
Change in SF-36 physical component score from baseline
to Week 52j
Patients evaluated 147 144
Least-squares mean 4.98 ± 0.74 2.63 ± 0.75 2.35 (0.40 to 4.31)
Change in EQ-5D-5L VAS from baseline to Week 52k
Patients evaluated 149 146
Least-squares mean 13.0 ± 1.4 7.1 ± 1.4 5.9 (2.3 to 9.6)
Change in UACR from baseline to Week 4l
Patients evaluated 121 124
Least-squares mean −40 ± 10 0±9 −40 (−53 to −22)
a
Plus–minus values are means or least-squares means ± SE.
b
Remission was defined as a BVAS of 0 and no receipt of glucocorticoids for vasculitis within 4 weeks before the Week 26 visit.
c
Shown are estimated common differences in percentage points and two-sided 95% confidence intervals.
d
One-sided p-value for non-inferiority,8 Harigai and Takada
Table 7. Safety results of ADVOCATE.
Eventa Avacopan Prednisone
Any adverse event 98.8 98.2
Any serious adverse eventb 42.2 45.1
Life-threatening adverse event 4.8 8.5
Death 1.2 2.4
Any serious event related to vasculitis worseningc 10.2 14.0
Any serious event not related to vasculitis worsening 37.3 39.0
Discontinuation of trial medication due to adverse event, % 15.7 17.7
Any infection 68.1 75.6
Any serious infection 13.3 15.2
Downloaded from https://academic.oup.com/mr/advance-article/doi/10.1093/mr/roab104/6497529 by guest on 14 January 2022
Any serious opportunistic infection 3.6 6.7
Death due to infection 0.6 1.2
Serious adverse event of abnormality on liver-function testing 5.4 3.7
Any adverse event potentially related to glucocorticoidsd 66.3 80.5
Any adverse event potentially related to glucocorticoids as assessed by the investigators 64.5 79.9
Any serious adverse event potentially related to prednisone as assessed by the investigators 6.6 14.6
a
Incidence is expressed as the percentage of patients having at least one event.
b
Serious adverse events were defined as any adverse event that resulted in death, was immediately life-threatening, required or prolonged hospitalization,
resulted in persistent or clinically significant disability or incapacity, was a birth defect, or was an important event that might jeopardize the patient or might
have required intervention to prevent any of the above.
c
Data are for patients who had a serious adverse event of ANCA-positive vasculitis (worsening), granulomatosis with polyangiitis (worsening), or microscopic
polyangiitis (worsening).
d
Predefined Medical Definition for Regulatory Activities preferred terms based on the European League against Rheumatism search criteria were included for
each cluster.
Reproduced with permission from the New Engl J Med 2021;384:599–609 [19].
(i.e. avacopan) and acquired immune systems (i.e. RTX) may endpoints, both avacopan groups showed better responses
work better than other drug combinations. than the control group, with statistical differences at some
Subgroup analyses also suggested a better response to visits compared to the control group [22]. Despite the dif-
avacopan at Week 52 in patients with MPO-ANCA vs PR3- ference in the primary endpoints between ADVOCATE and
ANCA and with MPA vs GPA. An observational study from CLEAR and the small number of participants in the CLEAR
the Japan Research Committee of the Ministry of Health, trial, these data indicate that avacopan plus RTX or CY
Labour and Welfare for Intractable Vasculitis demonstrated could be used completely without GCs to achieve remission.
that positivity for MPA-ANCA and MPA was dominant in However, in a clinical setting, low-dose and short-term (i.e.
Japanese patients with AAV in contrast to the data from 3–4 weeks) concomitant GCs with or without methylpred-
Europe and the USA [20]. In that cohort, 95 patients (85.6%) nisolone pulse therapy may be necessary depending on the
with MPA and GPA achieved remission by 6 months, and 23 extent and severity of organs affected by AAV. Post hoc anal-
relapsed during the observation period of 24 months with- ysis of ADVOCATE data and accumulation of post-marketing
out significant differences in relapse rates between the two registry data are required to draw a more robust conclusion.
diseases (MPA 29% and GPA 15% at month 18) [21]. Several other important questions remain to be answered:
Considering these data, avacopan appears to have a good pos- (1) Is avacopan plus reduced-dose GC without RTX/CY
sibility to improve the clinical outcomes of Japanese patients efficacious in remission induction therapy? (2) Are RTX/CY
with MPA and GPA, and evidence supporting this hypothesis plus reduced-dose GC and RTX/CY plus avacopan without
should be generated in Japan. GC equally efficacious in remission induction therapy? (3)
In ADVOCATE, the use of GCs was allowed during the Does avacopan have a GC tapering effect in remission mainte-
screening period (i.e. Week −2 to Week −1), and 75.3% in the nance therapy? (4) Are RTX and avacopan equally efficacious
avacopan group and 82.3% in the prednisone group used IV in remission maintenance therapy? (5) Is drug-free remis-
or oral GCs. In the avacopan group, 59.6% used oral GC at sion after discontinuing avacopan possible? A well-designed
a mean prednisone-equivalent dose of 13.4 mg/day, and 38% observational study and randomized controlled trial will be
used intravenous GC with a mean total dose of 466.9 mg. GCs necessary to provide answers to these questions in the next
used in the screening period were tapered and discontinued by decade.
Week 4. It has not been reported whether intravenous GC was
administered as pulse therapy. Although prednisone as a test
drug was not administered in the avacopan group after Day 1, Acknowledgement
these data raise the question of whether treatment with avaco-
We thank Editage for the English editing service.
pan plus RTX or CY shows an expected efficacy irrespective
of oral or intravenous GC use at the start of treatment. No
subgroup analysis data were provided for patients who did or
did not use GCs during the screening period. The primary end-
Conflict of interest
point of the CLEAR trial was achieved in 86.4% and 81.0% M.H. has received research grants from AbbVie Japan GK,
of the avacopan plus 20 mg prednisone group and avacopan Asahi Kasei Corp., Astellas Pharma Inc., Ayumi Pharmaceu-
without prednisone group, respectively. In most secondary tical Co., Boehringer Ingelheim Japan, Inc., Bristol MyersAvacopan for anti-neutrophil cytoplasmic antibody-associated vasculitis 9
Squibb Co., Ltd., Chugai Pharmaceutical Co., Daiichi- [8] Harigai M, Tsutsumino M, Takada H et al. Molecular targeted
Sankyo, Inc., Eisai Co., Ltd., Kaken Pharmaceutical Co., Ltd., therapies for microscopic polyangiitis and granulomatosis with
Kissei Pharmaceutical Co., Ltd., Mitsubishi Tanabe Pharma polyangiitis. Korean J Intern Med 2019;34:492–503.
Co., Nippon Kayaku Co., Ltd., Sekisui Medical, Taisho [9] Xiao H, Heeringa P, Hu P et al. Antineutrophil cytoplas-
mic autoantibodies specific for myeloperoxidase cause glomeru-
Pharmaceutical Co., Ltd., and Teijin Pharma Ltd. M.H. has
lonephritis and vasculitis in mice. J Clin Invest 2002;110:
received speaker fees from AbbVie Japan GK, Astra Zeneca K.
955–63.
K., Ayumi Pharmaceutical Co., Boehringer Ingelheim Japan, [10] Xiao H, Schreiber A, Heeringa P et al. Alternative complement
Inc., Bristol Myers Squibb Co., Ltd., Chugai Pharmaceutical pathway in the pathogenesis of disease mediated by anti-neutrophil
Co., Ltd., Eisai Co., Ltd., Eli Lilly Japan K.K., GlaxoSmithK- cytoplasmic autoantibodies. Am J Pathol 2007;170:52–64.
line K.K., Gilead Sciences Inc., Janssen Pharmaceutical K.K., [11] Huugen D, van Esch A, Xiao H et al. Inhibition of complement fac-
Kissei Pharmaceutical Co., Ltd., Nippon Kayaku Co., Ltd., tor C5 protects against anti-myeloperoxidase antibody-mediated
Downloaded from https://academic.oup.com/mr/advance-article/doi/10.1093/mr/roab104/6497529 by guest on 14 January 2022
Nippon Shinyaku Co., Ltd., Novartis Japan, Pfizer Japan glomerulonephritis in mice. Kidney Int 2007;71:646–54.
Inc., CIMIC Holdings Co., Ltd., Mitsubishi Tanabe Pharma [12] Gou S-J, Yuan J, Chen M et al. Circulating complement activation
Co., Teijin Pharma Ltd, and UCB Japan. M.H. is a consultant in patients with anti-neutrophil cytoplasmic antibody–associated
vasculitis. Kidney Int 2013;83:129–37.
for AbbVie, Boehringer Ingelheim, Bristol Myers Squibb Co.,
[13] Schreiber A, Xiao H, Jennette JC et al. C5a receptor mediates neu-
Kissei Pharmaceutical Co., Ltd., and Teijin Pharma. T.H. has
trophil activation and ANCA-induced glomerulonephritis. J Am
no conflicts of interest to declare. Soc Nephrol 2009;20:289–98.
[14] Xiao H, Dairaghi DJ, Powers JP et al. C5a receptor (CD88)
blockade protects against MPO-ANCA GN. J Am Soc Nephrol
Funding 2014;25:225–31.
This work was supported by the Ministry of Health, Labour, [15] Schreiber A, Rousselle A, Becker JU et al. Necroptosis controls
and Welfare of Japan Grant Number H29-nanchitou(nan)- NET generation and mediates complement activation, endothelial
ippan-018, 20FC1044, and 20FC1033. damage, and autoimmune vasculitis. Proc Natl Acad Sci U S A
2017;114:E9618–25.
[16] Nakazawa D, Masuda S, Tomaru U et al. Pathogenesis and ther-
apeutic interventions for ANCA-associated vasculitis. Nat Rev
References Rheumatol 2019;15:91–101.
[1] Jennette JC, Falk RJ, Bacon PA et al. 2012 revised International [17] Bekker P, Dairaghi D, Seitz L et al. Characterization of pharmaco-
Chapel Hill Consensus Conference Nomenclature of Vasculitides. logic and pharmacokinetic properties of CCX168, a potent and
Arthritis Rheum 2013;65:1–11. selective orally administered complement 5a receptor inhibitor,
[2] Harigai M, Nagasaka K, Amano K et al. 2017 Clinical prac- based on preclinical evaluation and randomized phase 1 clinical
tice guidelines of the Japan Research Committee of the Ministry study. PLoS One 2016;11:e0164646.
of Health, Labour, and Welfare for Intractable Vasculitis for [18] Japan Ministry of Health, Labour, and Welfare. Japanese Pack-
the management of ANCA-associated vasculitis. Mod Rheumatol age Insert for Avaopan. https://www.info.pmda.go.jp/go/pack/
2019;29:20–30. 39990E0M1029_1_02/39990E0M1029_1_02?view=body&lang
[3] Ntatsaki E, Carruthers D, Chakravarty K et al. BSR and BHPR =ja(31 December 2021, date last accessed).
guideline for the management of adults with ANCA-associated [19] Jayne DRW, Merkel PA, Schall TJ et al. Avacopan for the treat-
vasculitis. Rheumatology 2014;53:2306–9. ment of ANCA-associated vasculitis. N Engl J Med 2021;384:
[4] Chung SA, Langford CA, Maz M et al. 2021 American College 599–609.
of Rheumatology/Vasculitis Foundation guideline for the manage- [20] Sada K-E, Yamamura M, Harigai M et al. Classification and
ment of antineutrophil cytoplasmic antibody–associated vasculitis. characteristics of Japanese patients with antineutrophil cytoplas-
Arthritis Care Res 2021;73:1088–105. mic antibody-associated vasculitis in a nationwide, prospective,
[5] Reddy YNV, Siedlecki AM, Francis JM. Breaking down the com- inception cohort study. Arthritis Res Ther 2014;16:R101.
plement system: a review and update on novel therapies. Curr [21] Sada K-E, Yamamura M, Harigai M et al. Different responses
Opin Nephrol Hypertens 2017;26:123–8. to treatment across classified diseases and severities in Japanese
[6] Stone JH, Merkel PA, Spiera R et al. Rituximab versus patients with microscopic polyangiitis and granulomatosis with
cyclophosphamide for ANCA-associated vasculitis. N Engl J Med polyangiitis: a nationwide prospective inception cohort study.
2010;363:221–32. Arthritis Res Ther 2015;17:305.
[7] Jones RB, Tervaert JW, Hauser T et al. Rituximab versus [22] Jayne DRW, Bruchfeld AN, Harper L et al. Randomized trial of
cyclophosphamide in ANCA-associated renal vasculitis. N Engl J C5a receptor inhibitor avacopan in ANCA-associated vasculitis. J
Med 2010;363:211–20. Am Soc Nephrol 2017;28:2756–67.You can also read

















































