Investor Update 06 APRIL 2021
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
06
Investor Update
APRIL 2021
IN THIS ISSUE:
MESSAGE FROM THE CEO VALIDATION OF LAG-3 PARTNERSHIP PROGRESS CONTINUES
FINANCING INDUSTRY CONFERENCES & POSTER PRESENTATIONS
OPERATIONAL SNAPSHOT OUTLOOK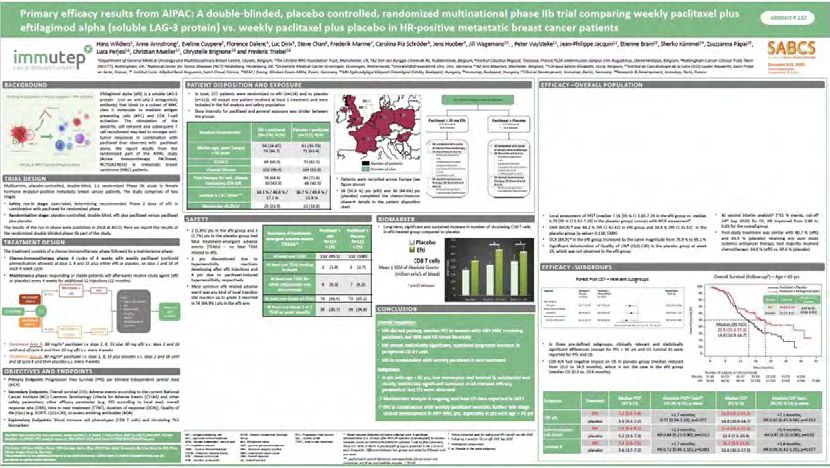
MARC VOIGT
Message from the CEO
The last few months have certainly been a very busy period, not only for Immutep but for our whole
sector. I would like to take the opportunity in our newsletter to add a bit more colour to the significance
of Bristol Myers Squibb’s (BMS) first validation of a LAG-3 product, and to elaborate on our second col-
laboration with MSD and our partnership with LabCorp to help develop immuno-oncology diagnostics.
From an industry perspective, March 2021 delivered the news we had all been anticipating for years:
the validation of LAG-3 as the next emerging immunotherapy target.
This validation came in the form of BMS’s announcement that its Phase II/III trial evaluating the
combination of relatlimab, an anti-LAG-3 antibody, and Opdivo, an approved anti-PD-1 blockbuster
drug, in melano-ma patients had met its primary endpoint of progression-free survival (PFS). In other
words, they report-ed the combination immunotherapy was helping patients.
BMS intends to release the details of the results at an industry conference soon. However, the top line
results are enough to confirm the interaction between LAG-3 and MHC II (the ligand that LAG-3 naturally
binds to) can be manipulated to help the body’s immune system fight cancer (See Diagram 1).
This is a significant milestone for cancer immunotherapy. We can now expect LAG-3-related products
to be featured prominently with more interest from partners and investors. LAG-3 is advancing quickly
to be-come the next emerging target for immunotherapy behind PD-1 and CTLA-4.
Diagram 1. Current immunotherapy targets including PD-1 and CTLA-4, which have approved therapeu-
tic products available for patients, plus LAG-3 which uniquely binds to the MHCII complex of an antigen
presenting cell.1
[Continued on p. 3]
1
https://www.frontiersin.org/files/Articles/402607/fimmu-09-01909-HTML/image_m/fimmu-09-01909-g001.jpg 2
MARC VOIGT
Message from the CEO
[Continued from p. 2]
BMS’s news is especially significant for the LAG-3 industry. It represents further validation of LAG-3, an
immune checkpoint that has been attracting increasing interest over the years, as can be seen by the
exponentially increasing rate of publications shown at Diagram 2.
Immutep’s CSO and CMO, Prof Frédéric Triebel, discovered LAG-3 in 1990 and has spent the last 30
years working in the field. In the interview below entitled “Validation of LAG-3”, Prof Triebel reflects on
his journey with LAG-3.
Immutep remains the only LAG-3 pure-play with more programs around LAG-3 than anyone else in the
field, including big pharma.
Within the exciting and growing LAG-3 space, Immutep continues to be the worldwide leader in devel-
oping LAG-3 therapeutics. We are contributing four product candidates which are being evaluated in
multiple clinical trials. No other company has such depth of pipeline or knowledge. This is one of the key
reasons LabCorp partnered with us to develop LAG-3 diagnostic tests.
In addition, we have the only MHC II agonist product candidate in development, known as efti. Efti is
an immune booster that has the versatility to be paired with PD-1 (or PD-L1) antagonists in combination
therapies. Notably, efti has a very different and unique mode of action from anti-LAG-3 products such
as relatlimab or leramilimab (LAG525) and this has several advantages that broaden our opportunity
(See Two Modes of Action for LAG-3 article). It also puts us in a category with no current competition
(see Overview of the LAG-3 Landscape at Diagram 3), while being part of practically every field of
LAG-3 related therapies i.e. with an agonist soluble LAG-3 protein and an antagonist antibody for
oncology and an agonist and a depleting antibody for autoimmune diseases.
We were also happy to inform you in mid-March 2021 that Immutep had deepened our relationship with
MSD through a second collaboration with them. MSD (known as Merck & Co. in the USA) is an American
multinational pharmaceutical company and one of the largest pharmaceutical companies in the world.
As you can imagine, this new collaboration involved much work from our team and I would like to thank
them for their steadfast commitment. We have certainly become a very effective team, having success-
fully secured multiple partnerships already (see our pipeline as summarised in the Operational Snapshot
section). Of course, there is always more to do on that front, and I can assure you that we always look to
the future for further opportunities to build the value of Immutep!
[Continued on p. 4]
3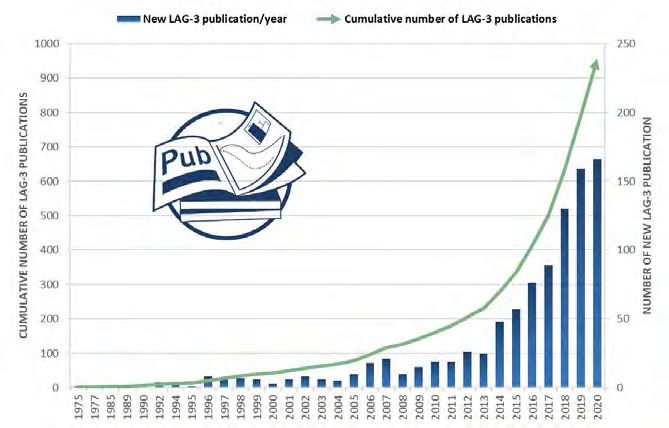
MARC VOIGT
Message from the CEO
[Continued from p. 3]
Two Modes of Action for LAG-3
The first mechanism of action relates to antagonist LAG-3 drugs, such as relatlimab (BMS) or leramilimab
(LAG525 from our licensee Novartis). These drugs are antibodies that bind to the naturally occurring LAG-3
proteins on T cells, blocking anything else from binding. When these antagonist drugs, also known as an-ti-
LAG-3 drugs, are bound, the LAG-3 receptor on activated T cells can’t bind MHC II molecules expressed by
antigen presenting cells (APC) such as dendritic cells. LAG-3 is an inhibitory receptor on T cells; when
LAG-3 is engaged by MHC II, it down-regulates T cell activation. Therefore, blocking the MHC II-LAG-3
interaction is analogous to releasing the brakes on the activated T cells.
Antagonists need to be given to patients at higher doses to ensure the drug can bind to all LAG-3 molecules
all the time to completely block the MHC II-LAG-3 interaction. From a medical perspective, the recent BMS
announcement validates the physiological importance of this MHC II-LAG-3 interaction as the simple block-
ade of this interaction at the tumor site or in the draining lymph node leads to clinical benefit.
Efti, which is a soluble recombinant LAG-3 protein, is not an anti-LAG-3 therapy. It’s mode of action
is as an MHC II agonist. It is an APC activator.
Agonists such as efti can be given at lower doses than antagonists, because they need to only bind to a few
percent of MHC II receptors to trigger APC activation which, is the first step of pushing the accelerator on
the immune system. Indeed, activated APCs like dendritic cells physiologically instruct the T cells what to do
in terms of antigen specificity (they present antigenic peptides to T cells), direction of the immune response
(anergy versus proliferation) or functionality (they give the CD8 T cells the “license to kill” signal, so that the
latter cells become more cytotoxic).
See our Mode of Action video for further explanation of LAG-3 immunotherapy.
https://www.youtube.com/watch?v=6EISCGYAGQw
4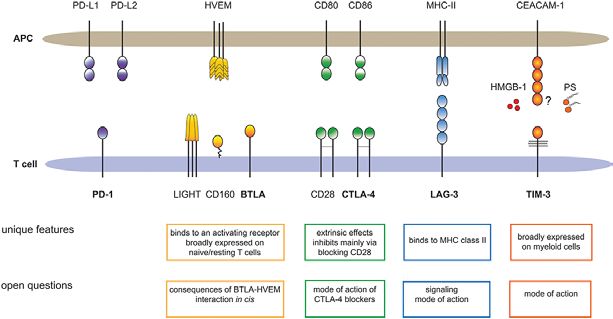
VALIDATION OF LAG-3
Quick Glossary
Agonists are molecules that bind to a receptor
and activate the receptor to produce a biological
response.
Alleles are one of two, or more, forms of a giv-
en gene variant.
Antagonists are a type of molecule that blocks a
receptor-ligand interaction and the associated bio-
logical response.
Antigen presenting cells (APCs) process and
present antigens for recognition by T cells. They
give instructions and a license to kill to CD8 T cells.
Prof Frederic Triebel is Immutep’s CMO/CSO
Antigens are molecules on the outside of a patho-
and the discoverer of the LAG-3 gene. Talking
gen cell. Cancer cells have tumour antigens.
to him from his home in Normandy, France,
where he is in lock down, he reflects on the MHC class II are a class of Quickmajor histocom-
discovery of LAG-3 and the significance of its patibility complex (MHC) molecules.
recent validation after a lifetime in the pursuit
of LAG-3 knowledge for the benefit of patients. T cells destroy foreign cells (including tumour cells)
in the body when given instructions from an APC.
When did you first know that LAG-3 was an important protein in the body’s immune system?
Back in 1988, I was working at Institut Gustave Roussy, south of Paris and cloned mRNA specifically
expressed in human T cells after their activation, therefore named Lymphocyte Activation Gene-1, -2, -3.
LAG-3 was first published in May 1990 and interestingly was found to be related phylogenetically to CD4,
a known ligand for MHC class II (MHC II) molecules.
This was exciting because we already knew MHC II was intricately involved in many aspects of the body’s
immune response. MHC II genes and molecules are related to a multitude of different diseases. For in-
stance, certain MHC II alleles are strongly associated with the risk of inheriting Type I diabetes.
What was the core question that drove your research for more than 30 years?
Because we understood the power of CD8 T cells to destroy tumours in animal models and the role of the
[Continued on p. 6]
5
VALIDATION OF LAG-3
[Continued from p. 5]
question: how could we get T cells to destroy cancer cells in patients with advanced disease?
I knew the answer lay in part in the interaction between MHC II and LAG-3, that is, bridging professional
APCs (dendritic cells) to activated T cells.
What is special about BMS’s news?
It shows us we are all “barking up the right tree” looking into the interaction between MHC II and LAG-3.
It demonstrates the interaction is important in the immune system and it can be used to destroy cancer
cells.
In oncology, this interaction can be leveraged in two ways, via two modes of action.
What are the two different modes of action?
In this MHC II/LAG-3 interaction, one can use a soluble LAG-3 protein to “push the accelerator” (an
agonist action) on the MHC II molecules in order to activate APCs (and subsequently CD8 killer T cells)
or one can use a blocking anti-LAG-3 antibody to stop MHC II engaging LAG-3 receptors on T cells (an
antagonist action), thereby leading directly to more activated T cells.
Both modes of action can be leveraged to restore the immune system’s ability to find and fight cancer
cells but probably in different patient populations. Patients with so-called “cold or tepid” tumors (the ma-
jority of patients, with few activated T cells at the tumor site) need APC activation via efti to induce more
T cells to recognise effectively the tumour cells while “hot” tumor patients, unfortunately the minority,
with a strong natural tumour bed infiltration by activated T cells could benefit from the antagonist effect,
releasing the brakes on the T cells using an anti-LAG-3 antibody. (For more detail see Two Modes of
Action for LAG-3).
Were there any moments along the LAG-3 journey where you had doubts?
I have always believed in LAG-3. However, there were times in the industry where it was difficult to con-
vince others of LAG-3’s potential. For a long time, chemotherapy was the number one treatment for many
cancers, including breast cancer. The higher the dose, the more effective the chemo. The trouble was, it
is very toxic and not very effective in many other indications.
Still, it was difficult to shift the paradigm. Then cancer vaccines came along. They were very hard to de-
velop and there were many failures. They were safe, but they didn’t work. This made the oncology world
less open to new ideas. And then from 2010 onwards, the change came gradually when oncologists used
anti-CTLA-4 and anti-PD-1 antibodies in randomised clinical trials. These antibodies are not anti-cancer
agents per se. CTLA-4 or PD-1 are not expressed by tumour cells. They just unleash the power of the
natural pre-existing T cell responses specific for tumor antigens. The anti-cancer agents are the patient
CD8 T cells themselves that could get rid of massive metastatic tumour lesions in a few weeks. In short,
we moved from a small field of cancer immunotherapy experimentations with early phase clinical trials to
a new full-fledged medical science, named immuno-oncology.
Have there been sacrifices, personally or professionally along the way?
Absolutely! I wanted to focus completely on LAG-3, so I started Immutep with John Hawken in Septem-
ber 2001. It was just after the attack on the Twin Towers in New York. It was a hard time to start a new
biotech, very difficult to raise cash in Europe due to the war in Iraq.
[Continued on p. 7]
6
VALIDATION OF LAG-3
[Continued from p. 6]
I left my secure clinical job at the Institut Gustave Roussy, south of Paris, in 2002 and then quit my teach-
ing job as a Professor at the Paris-Sud university in 2004 and have also been the first investor, risking the
financial wellbeing of my family at that time. I burned my vessels on the beach like Agamemnon!
Now that LAG-3 has been validated, what will happen next in the LAG-3 space?
We have been waiting for BMS’s results for the last three years, ever since they completed their phase II
trial. We have never known the results of the earlier phase II trial, but obviously they were strong enough
for BMS to decide to proceed with the phase III.
I expect there will be more news coming from BMS which has 38 trials running in different indications.
We will also have a flurry of results from others in the space. It will go from being a secret with unknown
materiality, to an open race to the finish line! Of course, Immutep and its many collaborators will signifi-
cantly contribute to the LAG-3 related developments as well!
Where do you see LAG-3 10 years from now?
There is lots of work to be done to fully appreciate the significance of the MHC II/LAG-3 interaction not
only in immuno-oncology but also in autoimmunity and infection. We have a good chance of success in
autoimmune diseases with IMP761 (a LAG-3 agonist antibody), and in oncology and infectious diseases
with efti.
More broadly, I believe immunotherapies will be expanded beyond cancer and clearly defined autoim-
mune diseases, into new fields. We can use the new tools we have in immuno-oncology in other thera-
peutic fields where we don’t quite understand the implication of T cell aggressiveness, like arterioscle-
rosis or Parkinson disease (LAG-3 clearly plays a role there) or Alzheimer’s disease. It is truly exciting!!
LAG-3 LANDSCAPE
Diagram 2.
Acceleration in
the LAG-3 space.
Source: PubMed
[Continued on p. 8]
7
VALIDATION OF LAG-3
[Continued from p. 7]
Interest and investment in LAG-3 therapeutics has continued to accelerate over the last year. There are
now more than 91 clinical trials evaluating 15 LAG-3 product candidates for more than 17,000 patients
(See diagram 3).
Immutep and our collaboration partners have contributed to 22 trials for more than 2,000 patients. Apart
from Immutep’s candidates, all other LAG-3 candidates shown at Diagram 3 are all anti-LAG-3 antago-
nist antibodies with similar mechanisms of action being evaluated in cancer trials. Immutep’s IMP761 and
IMP731 (licensed to GSK) are being developed for autoimmune diseases.
Many pharmaceutical companies have entered the space and are rapidly advancing promising product
candidates, including BMS, Roche, Boehringer Ingelheim, plus our existing partners Novartis, MSD and
GSK and more than 30 others. Still, Immutep has an excellent and leading position in the field! However,
Immutep continues to have the only MHC II agonist in late-stage clinical development, as shown below
(Diagram 3).
Diagram 3. The LAG-3 therapeutic landscape.
Sources: GlobalData, Company websites, clinicaltrials.gov, and sec.gov, as of April 2021. The green bars above
represent programs conducted by Immutep &/or its partners. Total Trials includes all active, completed &/or inac-
tive trials. Patient totals are based on estimated total enrolled &/or to be enrolled. The above is not a complete list
of currently existing LAG-3 products.
1 As of January 7, 2019 Regeneron is in full control of program and continuing development
(https://www.sec.gov/Archives/edgar/data/872589/000110465919000977/a19-1325_18k.htm)
2 On April 3, 2020 Les Laboratoires Servier acquired Symphogen
3 Tesaro was acquired by and is now part of GSK (www.gsk.com/en-gb/media/press-releases/gsk-completes-acqui-
sition-of-tesaro-an-oncology-focused-biopharmaceutical-company/)
4 Includes two completed Phase I studies and one discontinued Phase 2 study
5 Including IITs, two planned trials (MBC trial by EOC and HNSCC trial)
6 RELATIVITY-047 (https://investors.bms.com/iframes/press-releases/press-release-details/2021/Bristol-My
ers-Squibb-Announces-RELATIVITY-047-a-Trial-Evaluating-Anti-LAG-3-Antibody-Relatlimab-and-Opdi
vo-nivolumab-in-Patients-with-Previously-Untreated-Metastatic-or-Unresectable-Melanoma-Meets-Primary-End
point-of-Progression-Free-Survival/default.aspx)
8
PARTNERSHIP
PROGRESS CONTINUES
Second Collaboration with MSD
In mid-March 2021, we were delighted to deepen our relationship with MSD (Merck & Co) through a
second clinical trial collaboration and supply agreement.
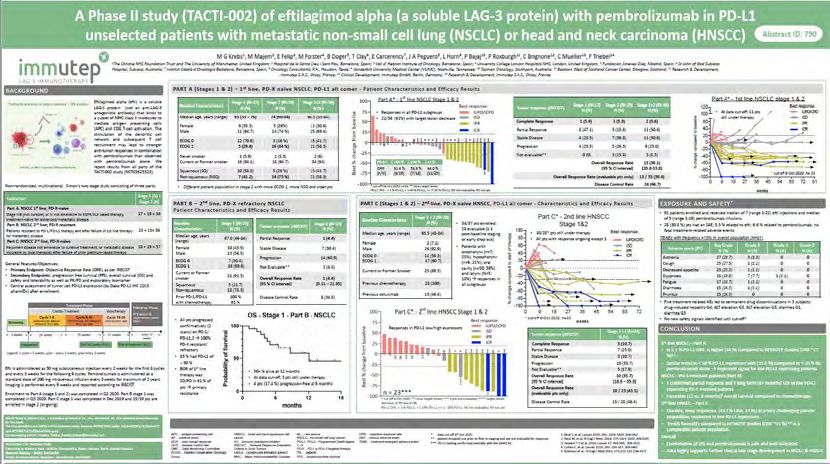
Called TACTI-003, the new trial evaluates efti in combination with MSD’s KEYTRUDA® (pembrolizumab)
as a first line therapy in unresectable recurrent or metastatic Head and Neck Squamous Cell Carcinoma
(HNSCC) patients.
This is the same combination therapy already being tested in Immutep’s ongoing Phase II TACTI-002
study (also designated KEYNOTE-798) and is delivering very promising results in second line HNSCC.
Planning for the new trial is progressing well and we expect to enroll the first patient in the study in mid-2021.
New Agreement with LabCorp
In late October, we started a new collaboration with the Laboratory Corporation of America Holdings,
known as LabCorp. Working with LabCorp, we will support the development of immuno-oncology prod-
ucts or services. This work enables Immutep to enter the immuno-oncology diagnostics field.
Interestingly LabCorp and Bristol Myers Squibb have an abstract at AACR 2021, discussing the expres-
sion of LAG-3 in different cancer types. It shows how closely the industry works together.
Our deep LAG-3 pipeline and highly experienced team reflects a significant amount of know-how in
immuno-oncology, specifically related to LAG-3.
9
FINANCING
Demonstrating strong interest and confidence in Immutep’s clinical program from existing and new
high-quality investors, we completed a A$29.6 million placement in November 2020. Australian Ethical,
Perennial Value Management, Regal Funds Management, Firetrail Investments and US-based, Ridge-
back Capital were all leading participants in the capital raise.
In addition, in December 2020, the Company received $10.66 million from the exercise of warrants over
American Depository Shares.
The proceeds will drive the ongoing development of our promising immuno-oncology and autoimmune
programs. Immutep now has a strong cash runway, into calendar year 2023 and beyond several signifi-
cant data read-outs.
10INDUSTRY CONFERENCES
Immutep was pleased to announce new data from our TACTI-002 phase II clinical trial (also designated
KEYNOTE-798) at the Society for Immunotherapy of Cancer (SITC) 35th Anniversary 2020 Annual
Meeting in November. More mature data from the trial was accepted as a late breaker poster presenta-
tion and poster walk for highly scored abstracts.
The data showed Overall Response Rates (ORR) in 1st line Non-Small Cell Lung Cancer (NSCLC) and
2nd line HNSCC had continued to be very favourable. Five patients demonstrated a Complete Response
(a complete disappearance of all tumour lesions): two patients were in the 1st line NSCLC group and
three patients were in the 2nd line HNSCC group. The results also demonstrated encouraging efficacy in
low PD-L1 expressing patients who do not typically respond to anti-PD-1 therapy.
SITC is the world’s leading member society of medical professionals dedicated to advancing cancer
immunotherapy and biological therapy.
A month later, in December 2020, Immutep presented data from our phase IIb APIAC trial in metastatic
breast cancer at the San Antonio Breast Cancer Symposium (SABC). The data was selected for a
spotlight presentation and showed a statistically significant survival benefit for key patient groups.
[Continued on p. 12]
11INDUSTRY CONFERENCES
AND POSTER PRESENTATIONS
[Continued from p. 11]
Specifically, a s tatistically significant Overall Survival (OS) benefit was seen in the efti group in pre-
defined patient groups. Patients under the age of 65 years showed a + 7.1 months survival benefit
(median of 21.9 vs. 14.8 months, nearly 50% longer) from efti with chemotherapy, compared to chemo-
therapy plus placebo (p=0.012). A +9.4 months survival benefit (median of 22.4 vs. 12.9 months, 74%
longer) was seen from efti with chemotherapy for patients with a low starting monocyte count (p=0.02).
A statistically significant increase in CD8 T cells (key immune cells) was observed in patients treated with
efti plus chemotherapy and this increase correlated with prolonged OS, indicating pharmacodynamic
activity and proof of concept of efti’s mode of action.
In addition, a promising and improving overall trend in OS in the total population was observed, based on
approximately 60% of events. A median survival benefit of +2.7 months from the efti plus chemotherapy
group was reported.
The results were the first time an antigen presenting cell (APC) activator has shown an OS benefit in a
randomised setting in metastatic breast cancer patients known to be insensitive to immune checkpoint
inhibitor therapy. The collection of OS is data ongoing and final data is expected to be reported
mid-2021.
SABC is a leading international conference focused on clinical, translational and basic research in
breast cancer. It is attended by a broad international audience of academic and private researchers and
physicians from over 90 countries.
Following the encouraging results presented at SITC and SABC, we have prioritised the recommence-
ment of scaling up the manufacturing efti.
12
OPERATIONAL SNAPSHOT
OPERATIONAL SNAPSHOT
EftilagimodSNAPSHOT Global Rights
OncologyOncology
OPERATIONAL
Alpha SNAPSHOT AIPAC Phase IIb
OPERATIONAL
(efti or IMP321) Metastatic Breast Cancer (Chemo – IO) §
Eftilagimod Global Rights
Alpha AIPAC Phase IIb
Eftilagimod Global Rights
Oncology
Overall Survival
(efti or
Overall IMP321)
Survival
Alpha
(OS) data from
Metastatic
AIPAC
(OS) data
the AIPAC
Breast
from
clinical
Cancer trial
(Chemo
thedata
AIPAC
were
– presented
IO)
clinical
at SABCS
trial were
2020 (see Industry
presentedPhase
Conferences
at SABCS
IIb
for a § (seetheIndustry
summary
2020
of results).
The collection of
(efti or IMP321)
OPERATIONAL
OS data is ongoing
Metastatic
SNAPSHOT
and
Breast final
Cancer is
(Chemo expected
– IO) to be reported mid-2021.
§
Conferences for a summary of the results). The collection of OS data is ongoing and final data is
Overall Survival (OS) data from the AIPAC clinical trial were presented at SABCS 2020 (see Industry Conferences for a summary of the results).
expected
Overall to be
TheEftilagimod
collection of
Survival
OPERATIONAL
reported
OS
(OS) data
data isfrom
SNAPSHOT
mid-2021.
ongoing and final
the AIPAC datatrial
clinical is expected to be reported
were presented mid-2021.
at SABCS 2020 (see Industry Conferences for a summary ofGlobal
the results).
Rights
Eftilagimod TACTI-002 (KEYNOTE-798) Global Rights
Oncology
The collection
Alpha of OS dataAIPACis ongoing and final data is expected to be reported mid-2021. Phase II
Oncology
Alpha Non-Small-Cell Lung Carcinoma (IO – IO) Phase IIb
(efti or IMP321)
(efti or IMP321) Metastatic Breast Cancer (Chemo – IO)
Head and Neck Squamous Cell Carcinoma (IO – IO) §
Eftilagimod Global
Global Rights
Oncology
Eftilagimod TACTI-002 (KEYNOTE-798) Rights
Alpha AIPAC Phase IIb
Alpha
Eftilagimod – IO) trial were reportedPhase IIin November Global Rights
Oncology
Non-Small-Cell Lung Carcinoma (IO
More
(efti mature
(efti or
Overall or and
IMP321)
Survival
IMP321)
Alpha
TACTI-002
Metastatic
encouraging
(OS) data
Head from
andthe
(KEYNOTE-798)
Breast
results
AIPAC
Neck
Cancer
from (Chemo
Immutep’s
clinical trial
Squamous Cell were
– IO)
TACTI-002
presented
Carcinoma (IO –atIO)
at SITC 2020. Since
SABCS 2020 (see Industry Conferences for a summary
Phase II
§
SITC, Immutep has
of the results).
Oncology
Non-Small-Cell Lung Carcinoma (IO –and
IO)started
completed theof
recruitment of patients
andwith
final2 data
lineisHNSCC the recruitment
mid-2021.of an additional cohort of 1 line §NSCLC patients in
nd st
The collection
(efti or IMP321)
OPERATIONAL OS data
SNAPSHOT is ongoing expected
Head and Neck Squamous Cell Carcinoma (IO – IO)
to be reported
January 2021. Further interim data from TACTI-002 is expected in H1 of 2021.
Overall Survival
More mature (OS)
and data from results
encouraging the AIPACfromclinical trial were
Immutep’s presented
TACTI-002 trialat SABCS
were 2020 (see
reported Industry
at SITC Conferences
in November 2020.for a summary
Since of the results).
SITC, Immutep has
The
Morecollection
completed
mature of
theandOS data is ongoing
recruitment
encouraging and
of patients
results finalImmutep’s
with
from data
2nd lineisHNSCC
expected andtostarted
TACTI-002 be reported
trial were mid-2021.
the recruitment
reported atof an in
SITC additional
Novembercohort
2020.ofSince
1st line NSCLC
SITC, patients
Immutep hasin
Eftilagimod Global Rights
Oncology
TACTI-002 (KEYNOTE-798)
January
completed 2021.
theFurther AIPAC
interim
recruitment data from
of patients TACTI-002
with 2nd line is expected
HNSCC and in H1 ofthe
started 2021.
recruitment of anII trial
additional cohort of 1st line NSCLC patients inNo-
More mature
Eftilagimod
Alpha and encouraging results from Immutep’s TACTI-002Phase were
Phase IIbreported at SITC
GlobalinRights
Oncology
Non-Small-Cell Lung Carcinoma (IO – IO)
January 2021.
Alpha
(efti or IMP321) TACTI-003
FurtherMetastatic
interim Breast
data from Cancer (Chemo
TACTI-002 – IO) in H1 of 2021.
is expected Phase II §
Oncology
vember 2020. Since Head and
SITC, Neck Squamous
Immutep Cell
has Carcinoma
completed (IO –– IO)
the recruitment of patients with 2nd line HNSCC
Eftilagimod
(efti or IMP321)
Alpha
Head and Neck Squamous
TACTI-002 (KEYNOTE-798) Cell Carcinoma (IO IO) § Global Rights
Phase II patients in January 2021.
Oncology
and More
started
Eftilagimodthe Non-Small-Cell
recruitment of Lung Carcinoma (IOcohort
anclinical
additional – IO) ofat 1st line NSCLC GlobalFurther
Rights
(efti mature
Overall or IMP321)
Survival
Alpha
Eftilagimod
and encouraging
(OS) data from
TACTI-003 results
the AIPACfrom Immutep’s
trial TACTI-002
were
Head and Neck Squamous Cell Carcinoma (IO – IO) trial
presented were reported
SABCS 2020 at
(seeSITC in
Industry
Phase II
November 2020.
Conferences Since
for a §
SITC,
summary Immutep has
of the results).
Global Rights
Oncology
interim data
Immutep
completed
The is from
theof
collection
(efti or IMP321)
Alpha
TACTI-002
progressing well
Head
recruitment
OS data with
and
of patients
is ongoing
TACTI-003 is
plans
Neck expected
to start
Squamous
andwith nd the
final2 data Cell in
study H1
in
Carcinoma
lineisHNSCC
expected of 2021.
mid-2021.
(IO
andtostarted – IO) mid-2021.of an additional cohort of 1 line§NSCLC patients in
the recruitment
be reported st
Phase II
Oncology
January or2021.
(efti mature
More Further
IMP321)
and Head
encouragingand
interim Neck
data
results Squamous
from TACTI-002
from Cell
Immutep’s Carcinoma
is expected
TACTI-002 (IO of
in H1
trial – IO)
2021.reported at SITC in November 2020. Since SITC,
were § Immutep has
completed
Immutep isthe
Eftilagimod recruitment
progressing wellofwith
patients
planswith 2nd line
to start HNSCCinand
the study started the recruitment of an additional cohort of 1st line NSCLC patients
mid-2021. Global in
Global Rights
Oncology
Eftilagimod TACTI-002 (KEYNOTE-798) Rights
January
Immutep 2021.
is
Alpha FurtherINSIGHT-004
progressinginterim
well data
with fromtoTACTI-002
plans start the is expected
study in in H1
I of 2021.
mid-2021.
Phase
Alpha
Eftilagimod Global Rights
Phase II
§
Oncology
Non-Small-Cell Lung
Solid Tumors (IO – IO) Carcinoma (IO – IO)
(efti
(efti or
or IMP321)
IMP321) TACTI-003
Alpha Head and Neck Squamous Cell Carcinoma (IO – IO) Phase II
Oncology
Eftilagimod Head and Neck Squamous Cell Carcinoma (IO – IO) § Global Rights
Oncology
(efti or IMP321) INSIGHT-004
Eftilagimod
Alpha
Eftilagimod Phase I Global
Global Rights
Rights
Oncology
In (efti
MoreSeptember
mature
Alpha
or IMP321)
Alpha
2020,
and Immutep
TACTI-003
Solid
encouraging
INSIGHT-004 reported
Tumorsresults improving
(IOfrom data from
– IO)Immutep’s the INSIGHT-004
TACTI-002 trial. 41.7%
trial were reported of patients
at SITC
Phase II in November 2020. Since SITC, §
showed a Partial Response to thehas
Immutep
Oncology
Phase I
combination
(efti
Immutep
completedor is therapy
IMP321) Head
of
progressing
the
(efti or IMP321)
efti
Solid
well
recruitment and
and
Tumors
with
of Neck
plans
patients Squamous
avelumab,
(IO –
to building
IO)
start
with 2 nd
theCell
line onCarcinoma
the
study
HNSCC in (IO –reported
previously
mid-2021.
and started IO) recruitment
the result of 33%
of an showing a
additional Partial
cohort Response.
of 1st
§
line NSCLC patients in
January 2021. Further interim data from TACTI-002 is expected in H1 of 2021.
Immutep is progressing
In September 2020, Immutepwell with
reported plansdata
improving to start
from the the study
INSIGHT-004
12
in mid-2021.
trial. 41.7% of patients showed a Partial Response to the
Immutep
combination
In September is progressing
therapy of well
2020, Immutep with
efti and plans to
avelumab,
reported start
improving thedata
building study
on theinpreviously
from mid-2021. reportedtrial.
the INSIGHT-004 result of 33%
41.7% showingshowed
of patients a Partiala Response.
Partial Response Global
to the Rights
Eftilagimod
Oncology
combination
Alpha therapyINSIGHT-004
of efti and avelumab, building on the Phase previously
I reported result of 33% showing a Partial Response. Global Rights
Eftilagimod
(efti or IMP321)
Alpha
Solid Tumors (IO – IO)
TACTI-003 12 Phase II §
Oncology
Eftilagimod Global Rights
§
Oncology
(efti or IMP321) Head and Neck Squamous Cell Carcinoma (IO – 12
INSIGHT-004 IO)
Alpha Phase I
In (efti or IMP321)
September Solid Tumors (IO – IO)
2020, Immutep §
reported improving data from the INSIGHT-004 trial. 41.7% of patients showed a Partial Response to the
combination therapy of well
Immutep is progressing efti and
withavelumab, building
plans to start on theinpreviously
the study mid-2021.reported result of 33% showing a Partial Response.
In September 2020, Immutep reported improving data from the INSIGHT-004 trial. 41.7% of patients showed a Partial Response to the
12
combination therapy of efti and avelumab, building on the previously reported result of 33% showing a Partial Response.
In September
Eftilagimod2020, Immutep reported improving data from the INSIGHT-004 trial. 41.7% Global of patients
Rights
Oncology
Alpha INSIGHT-004
Phase I
showed a Partial
(efti or IMP321) Response
Solid Tumorsto
(IO the
– IO) combination therapy
12 of efti and avelumab, building on
§ the previously
reported result of 33% showing a Partial Response.
In September 2020, Immutep reported improving data from the INSIGHT-004 trial. 41.7% of patients showed a Partial Response to the
combination therapy of efti and avelumab, building on the previously reported result of 33% showing a Partial Response.
Encouraging early anti-tumour activity signals were observed in a variety of cancer indications not typ-
ically responsive to immunotherapy. Importantly, the 12combination of efti and avelumab continues to be
safe and well tolerated. Final data is expected in 2021.
[Continued on p. 14]
13OPERATIONAL SNAPSHOT
Encouraging early anti-tumour activity signals were observed in a variety of cancer indications not typically responsive to immunotherapy.
Importantly, the combination of efti and avelumab continues to be safe and well tolerated. Final data is expected in 2021.
[Continued from p. 13]
Encouraging early anti-tumour activity signals were observed in a variety of cancer indications not typically responsive to immunotherapy.
Importantly, the combination of efti and avelumab continues to be safe and well tolerated. Final data is expected in 2021.
Eftilagimod Global Rights
Oncology
TACTI-mel PhaseII
Alpha Phase
(efti or IMP321)
Encouraging
Melanoma (IO – IO)
early anti-tumour activity signals were observed in a variety of cancer indications not typically responsive § to immunotherapy.
Importantly, the combination of efti and avelumab continues to be safe and well tolerated. Final data is expected in 2021.
The results of Immutep’s TACTI-mel trial were featured prominently in Issue 38 of the Melanoma Research Review which is a summary of the
Encouraging early
Eftilagimod anti-tumour activity signals were observed in featured
a variety of cancer indications not
in typically responsive to immunotherapy.
Global Rights
Oncology
Thelatest
results of
research inImmutep’s for TACTI-mel
TACTI-mel
melanoma trial
health professionals. were
Healthcare
Phase prominently
professionals can access the ReviewIssue 38online
for free of the
at: Melanoma Re-
Alphathe combination of efti and avelumab continues
Importantly, to beIIsafe and well tolerated. Final data is expected in 2021.
Phase
search(eftiReview
Melanoma (IO – IO)
or IMP321)which is a summary of the latest research in melanoma for health professionals.
www.researchreview.com.au/au/Clinical-Area/Internal-Medicine/Medical-Oncology/Melanoma.aspx
§ Health-
care professionals can access the Review for free online at:
TheEftilagimod GlobalofRights
OncologyOncology
results of Immutep’s TACTI-mel trial were featured prominently
TACTI-mel PhaseII
in Issue 38 of the Melanoma Research Review which is a summary the
Alpha Phase
latest research in melanoma
Eftilagimod Melanoma (IO – IO)
for health professionals. Healthcare professionals can access the Review for free online at:
§ Global Rights
Oncology
(efti or IMP321)
www.researchreview.com.au/au/Clinical-Area/Internal-Medicine/Medical-Oncology/Melanoma.aspx
Alpha Solid Tumors (Cancer Vaccine) Phase
PhaseIII
Phase
Eftilagimod Global Rights
(efti or IMP321)
Alpha
TACTI-mel
YNP01 and YCP02
www.researchreview.com.au/au/Clinical-Area/Internal-Medicine/Medical-Oncology/Melanoma.aspx
PhaseII
Phase §
The results
(efti
Melanoma (IO – IO)
of Immutep’s TACTI-mel trial were featured prominently in Issue 38 of the Melanoma Research Review which
or IMP321) § is a summary of the
latest research
CYTLIMIC in melanoma
has been conductingfor twohealth professionals.
studies (YNP01 and YCP02) Healthcare
withprofessionals
CYT001 whichcan access thelead
is CYTLIMIC’s Review for free
cancer online
vaccine. at: comprises peptides
CYT001
Eftilagimod Global Rights
Oncology
designed
The results using artificial
of Immutep’s intelligence
Solid Tumors from
TACTI-mel theVaccine)
trial were
(Cancer HSP30 andprominently
featured GCP-3 proteins, plus38
in Issue two of adjuvants,
the Melanoma efti and Hiltonol
Research (Poly-ICLC).
Review which isUnder the terms
a summary of theof
Alpha Phase
PhaseIII
www.researchreview.com.au/au/Clinical-Area/Internal-Medicine/Medical-Oncology/Melanoma.aspx
Phase
clinical
latest collaboration,
(efti research
or IMP321) service
YNP01 and
in melanoma for supply
andhealth
YCP02 agreements with
professionals. Immutep,
Healthcare CYTLIMIC has
professionals canfull responsibility
access the Review forfor
thefree
continued
online at: §
development of the
cancer vaccine and Immutep is eligible to receive development-based milestone payments.
www.researchreview.com.au/au/Clinical-Area/Internal-Medicine/Medical-Oncology/Melanoma.aspx
Eftilagimod Globalpeptides
Rights
Oncology
CYTLIMIC has been conducting two studies (YNP01 and YCP02) with CYT001 which is CYTLIMIC’s lead cancer vaccine. CYT001 comprises
Alpha Solid Tumors (Cancer Vaccine) Phase
Phase
Phase III
designed using artificial intelligence from the HSP30 and GCP-3 proteins, plus two adjuvants, efti and Hiltonol (Poly-ICLC). Under the terms of
CYTLIMIC Eftilagimod has
(efti or IMP321)
clinical
been
collaboration,
Alpha
YNP01 conducting
and
service and
YCP02
supply
two
agreements
studies (YNP01
with Immutep,
and YCP02) with CYT001 which
Phase I CYTLIMIC has full responsibility for the continued development
§ Chinese
is CYTLIMIC’s
Global
Rights
ofRights
the
Eftilagimod Metastatic Breast Cancer (Chemo – IO)
Oncology
leadcancer
cancer vaccine. SolidCYT001
Tumors comprises
(Cancer Vaccine) peptides designed using artificial intelligence from the HSP30
(efti or vaccine
IMP321)
Alpha and Immutep is eligible to receive development-based
PhaseIII milestone payments.
Phase
Phase §
terms§CYT001
Oncology
YNP01 andtwo YCP02
and CYTLIMIC
GCP-3 proteins,
has
(efti or IMP321)been conductingplus two adjuvants,
studies (YNP01 and eftiYCP02)
and withHiltonol
CYT001(Poly-ICLC).
which is CYTLIMIC’s Under the vaccine.
lead cancer of clinical collab-
comprises peptides
designed using artificial intelligence from the HSP30 and GCP-3 proteins, plus two adjuvants, efti and Hiltonol (Poly-ICLC). Under the terms of
oration,
In Decemberservice
Eftilagimod
2020,andEOC supply agreements
Pharma announced its planswith Immutep,
to conduct a new phaseCYTLIMIC
II trial of eftihas full responsibility
in metastatic breast cancer. Thisfor the
follows continued
Immutep’s
clinical
CYTLIMIC
announcement collaboration,
has been service and
conducting
of encouraging twosupply
first studies
OS dataagreements
(YNP01
from itsand with Immutep,
YCP02) CYTLIMIC
with CYT001 which hasis full responsibility
CYTLIMIC’s for thevaccine.
lead cancer continued development
CYT001 Chinese
comprises of the
Rights
peptides
development
cancerAlpha
designed vaccine ofandthe cancer
Metastatic
Immutep
using artificial isBreast
intelligence
vaccine
Cancer (Chemo
eligible
fromtothe
receive andPhase
– IO)
IIb
Immutep study,
HSP30development-based
AIPAC
and GCP-3 proteins,milestone
(see above).
Phase Iis eligiblepayments. to receive development-based milestone
plus two adjuvants, efti and Hiltonol (Poly-ICLC). Under the terms of
(efti or IMP321)
payments. §
Oncology
clinical collaboration, service and supply agreements with Immutep, CYTLIMIC has full responsibility for the continued development of the
13
cancer vaccine and Immutep is eligible to receive development-based milestone payments.
Eftilagimod
In December 2020, EOC Pharma announced its plans to conduct a new phase II trial of efti in metastatic breast cancer. This followsChinese Immutep’s Rights
Alpha of encouraging
announcement Metastatic Breast
first OSCancer (Chemo
data from IO) IIb Phase
its –Phase study, IAIPAC (see above).
(efti or IMP321)
Eftilagimod § Chinese Rights
Oncology
Alpha Metastatic Breast Cancer (Chemo – IO) Phase I
13
In(efti or IMP321)
December 2020, EOC Pharma announced its plans to conduct a new phase II trial of efti in metastatic breast cancer. § This follows Immutep’s
Oncology
announcement of encouraging first OS data from its Phase IIb study, AIPAC (see above).
In December 2020, EOC Pharma announced its plans to conduct a new phase II trial of efti in metastatic breast cancer. This follows Immutep’s
announcement of encouraging first OS data from its Phase IIb study, AIPAC 13(see above).
In December 2020, EOC Pharma announced its plans to conduct a new phase II trial of efti in metastatic
breast cancer. This follows Immutep’s announcement of encouraging first OS data from its Phase IIb
13
study, AIPAC (see above).
EOC Pharma is the exclusive licensee of efti for the Chinese market.
EOC Pharma is the exclusive licensee of efti for the Chinese market.
Infectious
Eftilagimod Global Rights
Disease
Alpha COVID-19 Phase II
(efti or IMP321) §
The University Hospital Pilsen in the Czech Republic has commenced an investigator-initiated randomised phase II clinical trial evaluating efti in
up to 110 hospitalised patients with COVID-19. Recruitment of patients commenced in October 2020.
The University Hospital Pilsen in the Czech Republic has commenced an investigator-initiated ran-
The trialphase
domised aims to boost a patient’s
II clinical immune
trial response toefti
evaluating prevent the to
in up patient
110from developing severe
hospitalised COVID-19with
patients symptoms that requireRecruit-
COVID-19. intensive
care and can lead to respiratory failure and death. As an antigen presenting cell (APC) activator, efti could help to control the viral load in
menthospitalised
of patients commenced in
patients by boosting T cells. October 2020.
Initial results from the safety run in of the trial were reported in January 2020 and showed all six patients received the three planned 10 mg efti
The injections
trial aims to discharged
and were boost afrom patient’s immune
hospital. No response
adverse events to prevent
were reported. the patient
An independent from
review of this safetydeveloping severe
run-in data prompted the
COVID-19 symptoms
recommendation that
to proceed withrequire
enrolmentintensive care portion
for the randomised and canof the lead to respiratory
EAT COVID study. failure and death. As an
antigen
Initialpresenting
interim efficacycell (APC)
results activator,
are expected efti could
to be reported before help
the endto
of control
the year. the viral load in hospitalised patients by
boosting T cells.
Autoimmune
Global Rights
IMP761 Preclinical
(Agonist AB)
§
[Continued on p. 15]
14OPERATIONAL SNAPSHOT
EOC Pharma is the exclusive licensee of efti for the Chinese market.
Infectious
Eftilagimod Global Rights
Disease
Alpha COVID-19 Phase II
(efti or IMP321) §
[Continued from p. 14]
The University Hospital Pilsen in the Czech Republic has commenced an investigator-initiated randomised phase II clinical trial evaluating efti in
up to 110 hospitalised patients with COVID-19. Recruitment of patients commenced in October 2020.
The trial aims to boost a patient’s immune response to prevent the patient from developing severe COVID-19 symptoms that require intensive
Initial results from the safety run in of the trial were reported in January 2020 and showed all six patients
care and can lead to respiratory failure and death. As an antigen presenting cell (APC) activator, efti could help to control the viral load in
received the patients
hospitalised three byplanned
boosting T10 mg efti injections and were discharged from hospital. No adverse events
cells.
wereInitial
reported.
results from the safety run in of thereview
An independent trial wereof this safety
reported in Januaryrun-in
2020 anddata
showedprompted the
all six patients recommendation
received the three planned 10tomgpro-
efti
ceedinjections
with enrolment for the
and were discharged fromrandomised portion
hospital. No adverse eventsof thereported.
were EAT COVID study.
An independent review of this safety run-in data prompted the
recommendation to proceed with enrolment for the randomised portion of the EAT COVID study.
Initial interim
Initial interim efficacy results
efficacy results are expected
are expected tobefore
to be reported be reported before
the end of the year. the end of the year.
Autoimmune
Global Rights
IMP761 Preclinical
(Agonist AB)
§
Immutep is continuing cell line and other preclinical development activities for IMP761 in preparation for clinical trials.
Immutep is continuing cell line and other preclinical development activities for IMP761 in preparation for
Immutep
clinical is continuing cell line and other preclinical development activities for IMP761 in preparation for clinical trials.
trials.
Solid Tumors + Blood Cancer (IO-IO Combo) Phase II
Solid Tumors + Blood Cancer (IO-IO Combo) Phase II
Triple Negative Breast Cancer (Chemo-IO Combo) Phase II
14
LAG525
Triple Negative Breast Cancer (Chemo-IO Combo) Phase II §
(Antagonist Phase II
AB)
Melanoma (IO-IO-Small Molecule Combo)
§ Global Rights
Oncology
LAG525
(Antagonist Melanoma (IO-IO-Small Molecule Combo) Phase II
AB) Global Rights
Oncology
Solid Tumors (IO-IO Combo) Phase II
Solid Tumors (IO-IO Combo) Phase II
Triple Negative Breast Cancer
(Chemo-IO-Small Molecule Combo) Phase I
Triple Negative Breast Cancer
(Chemo-IO-Small Molecule Combo) Phase I
LAG525, now called leramilimab, a humanised form of IMP701 is being evaluated by Novartis in several Phase I and/or Phase II clinical trials in
combination with Novartis’ PD-1 inhibitor spartalizumab for the treatment of certain cancers.
LAG525, now called leramilimab, a humanised form of IMP701 is being evaluated by Novartis in several Phase I and/or Phase II clinical trials in
LAG525,
Novartisnow
combination called
has full
with leramilimab,
responsibility
Novartis’ forinhibitor
PD-1 a humanised
the continued development
spartalizumab form of IMP701
oftreatment
for the the LAG-3 certainis
antibody
of beingandevaluated
program
cancers. by Novartis
Immutep is eligible in several
to receive development-
based milestone payments and sales-based royalties.
Phase I and/or Phase II clinical trials in combination with Novartis’ PD-1 inhibitor spartalizumab for the
Novartis has full responsibility for the continued development of the LAG-3 antibody program and Immutep is eligible to receive development-
treatment of certain cancers.
based milestone payments and sales-based royalties.
Novartis has full responsibility for the continued development of the LAG-3 antibody program and
Immutep is eligible to receive development-based milestone payments and sales-based royalties.
15
15
[Continued on p. 16]
15OPERATIONAL SNAPSHOT
[Continued from p. 15]
Ulcerative Colitis Phase II
Global Rights
Autoimmune
GSK‘781
Healthy Japanese and Caucasian Subjects Phase I
(Depleting AB) §
Psoriasis Phase I
In January 2021, GSK stopped its phase II clinical trial evaluating GSK2831781 (derived from Immutep’s IMP731 antibody) in ulcerative colitis
In January 2021,
based on the GSKofstopped
assessment clinical dataits phase
as part II clinical
of a planned interimtrial evaluating
analysis conducted inGSK2831781 (derived
consultation with the trial’s Datafrom
ReviewImmutep’s
Committee.
GSK is conducting further reporting, assessment and analyses of the efficacy and safety data and evaluating the biology to determine next steps
IMP731 antibody) in ulcerative
for the GSK2831781 development program.
colitis based on the assessment of clinical data as part of a planned
interim analysis conducted in consultation with the trial’s Data Review Committee. GSK is conducting
Importantly, Immutep’s collaboration with GSK remains in place and GSK2831781 continues to be under an exclusive license with GSK. GSK
further reporting,
continues assessment
to have full responsibility forand analysesofofthisthe
the development efficacy
LAG-3 antibody and safety
program data isand
and Immutep evaluating
eligible the biology to
to receive development-based
determine
milestonenext steps
payments for the GSK2831781
and sales-based royalties. development program.
The discontinuation of the GSK trial has no impact on Immutep’s three other product candidates all of which have different mechanisms of
Importantly, Immutep’s
action, including collaboration
efti. Immutep’s cash runway iswith GSK remains in place and GSK2831781 continues to be under
also unimpacted.
an exclusive license with GSK. GSK continues to have full responsibility for the development of this
LAG-3 antibody program and Immutep is eligible to receive development-based milestone payments
OUTLOOK
and sales-based royalties.
Immutep is advancing strongly towards another step change in 2021. We continue to be in a very strong financial and operational position,
following the encouraging clinical results announced for efti in 2020.
The discontinuation of the GSK trial has no impact on Immutep’s three other product candidates all of
We have increasing confidence in efti and accordingly, over the last six months we have announced or commenced three new efti trials, or trial
which have different
extensions, mechanisms
with up to 386 of action,
patients in different including efti. Immutep’s cash runway is also unimpacted.
cancer indications.
Our business development activity has also advanced with a second collaboration with MSD and a new LAG-3 agreement with LabCorp.
16
16
OUTLOOK
Immutep is advancing strongly towards another step change in 2021. We continue to be in a very
strong financial and operational position, following the encouraging clinical results announced for efti
in 2020.
We have increasing confidence in efti and accordingly, over the last six months we have announced
or commenced three new efti trials, or trial extensions, with up to 386 patients in different cancer
indications.
Our business development activity has also advanced with a second collaboration with MSD and a
new LAG-3 agreement with LabCorp.
Engagement with regulatory bodies remains a key priority, along with strengthening our IP position and
upscaling the manufacturing of efti to prepare for the future. This has already resulted in efti receiving
Fast Track designation in 1st line HNSCC from the US FDA, given its encouraging data and potential
to meet an unmet medical need.
17COMPANY CALENDER
What’s next
JUNE 4TH 2021 - JUNE 8TH 2021
ASCO 2021 Annual Meeting
Immutep will participate in this year`s virtual ASCO 2021 Annual Meeting.
https://meetings.asco.org/am/virtual-welcome
JUNE 10TH 2021 - JUNE 18TH 2021
BIO International Convention - Bio Digital 2021
Immutep will participate in the new virtual event format.
https://www.bio.org/events/bio-digital
JULY 13TH 2021 - JULY 15TH 2021
Non-Small Cell Lung Cancer (NSCLC) Drug Development Summit
Immutep will participate in the digital Non-Small Cell Lung Cancer (NSCLC) Drug Development Summit.
Frédéric Triebel, CSO & CMO of Immutep speaks on the subject: A Soluble LAG-3 Protein (Eftilagimod
Alpha) with an Anti-PD-1 Antibody (Pembrolizumab): Results of a Phase II Study in NSCLC
https://nsclc-drug-development.com/
SEPTEMBER 17TH 2021 - SEPTEMBER 21ST 2021
ESMO 2021 Congress
Immutep will participate in the virtual ESMO 2021 congress.
https://www.esmo.org/meetings/esmo-congress-2021
NOVEMBER 10TH 2021 - NOVEMBER 14TH 2021
SITC - 36th Annual Meeting & Pre-Conference Programs (SITC 2021)
The company will have presentations at the conference and representatives will be attending.
Venue: Walter E. Washington Convention Center in Washington, D.C.
18IMMUTEP
Fast Facts
Listings Market Capitalisation
Australian Securities Exchange (ASX), NASDAQ A$299.2 million (US$227.5 million)
(as of 12 April 2021)
Stock Codes
ASX: IMM, NASDAQ: IMMP Cash & Term Deposits
~A$54.9 million (~US$42.3 million) (as of 31
Issued Capital – Ordinary Shares December 2020)
672.4 million (as of 12 April 2021)
Board of Directors Senior Management
Russell J Howard, PhD Prof Dr Frédéric Triebel
Non-executive Chairman Chief Medical Officer and Chief Scientific Officer
Mr Marc Voigt Deanne Miller
Executive Director and Chief Executive Officer Chief Operating Officer, General Counsel and
Company Secretary
Mr Pete A Meyers
Non-executive Director
Grant Chamberlain
Non-executive Director
www.immutep.com
19FOLLOW IMMUTEP’S PROGRESS Immutep is dedicated to maintaining consistent and clear communica- tions with our investors. In addition to our newsletter, we encourage our shareholders to continue following Immutep’s pro- gress in a number of ways: www.immutep.com Our website is a treasure trove for those in search of details about our company, our management team, and archived infor- mation. We encourage everyone to check it out regularly. www.clinicaltrials.gov Immutep registers all of our clinical trials, and the details of enrolling doctors, on the ClinicalTrials.gov website, a service of the United States National Institutes of Health. This register is the largest such repository of clinical trial information around the world. Our ClinicalTrials.gov ID for our trials are as follows: • TACTI-mel trial is NCT02676869 • AIPAC trial is NCT02614833 • TACTI-002 trial is NCT03625323 T ACTI-003 trial is NCT04811027 Twitter https://twitter.com/Immutep Facebook https://www.facebook.com/Immutep/ LinkedIn https://www.linkedin.com/company/857541/ Immutep Limited, Level 12, 95 Pitt Street, Sydney NSW 2000 ABN: 90 009 237 889 This investor update was authorised for release by the CEO of Immutep Lmited.
You can also read