Automated assay for urinary evaluation of aspirin response - Cardiology
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Cardiology
ASA
Automated assay for urinary
A
evaluation of aspirin response AS
ASA
ASA
A
AS
ASA
ASAKey Features of Randox TxBCardio
Automated Randox TxBCardio Assay
immunoturbidimetric Urine-based testing
Details
assay
• Facilitates easier sample collection Methodology
• The Randox TxBCardio assay and storage Latex-enhanced immunoturbidimetric
allows response to aspirin therapy
• Avoids the potential issues Sample Type
to be tested on automated
associated with the in-vivo platelet Urine
clinical chemistry analysers in
the laboratory, without the need effects of blood draws Reagent Format
for any additional, dedicated Liquid ready-to-use
equipment • TxBCardio results are reported Expiry
by expressing the concentration in Stable to expiry date when stored at
• With an assay time of as little as relation to the level of creatinine +2 to +8°C
ten minutes, Randox TxBCardio in the sample. This standardises
results and rules out the effect of
Assay Range
offers a more convenient, efficient
400-6000 pg/ml
option for the evaluation of aspirin urine concentration
therapy effectiveness in the general
QC Material
patient population Three levels of controls available
Applications available for an Calibrator Information
• High throughput screening can
extensive range of clinical TxBCardio Calibrator Series available
be implemented using Randox
chemistry analysers
TxBCardio Cat. No.:
• D
etailing instrument specific TBX2759 R1 1 x 9ml
settings for the convenient use of R2 1 x 4.7ml
Measurement of Randox TxBCardio on a variety of
11dhTxB2 systems
Additional Randox TxBCardio
• The primary target of aspirin Liquid ready-to-use Products
therapy is TxA₂, however this has format
Product Description Cat. No. Size
a very short half-life which makes TxBCardio TBX5125 3 x 3ml
accurate measurement problematic • Delivering optimum convenience Control Level 1
and ease of use TxBCardio TBX5126 3 x 3ml
Control Level 2
• When TxA₂ degrades it is
TxBCardio TBX5127 3 x 3ml
converted into a number of Control Level 3
metabolites, the most abundant of Complementary Controls TxBCardio TBX3132 6 x 3ml
Calibrator Series
which is 11dhTxB₂ and Calibrator available TxBCardio TBX2814 1 x 100ml
Sample Diluent
• Randox TxBCardio specifically
measures the 11dhTxB₂ metabolite • Providing a complete diagnostic For research use only in the USA. Not for
and therefore offers a highly testing package use in diagnostic procedures in the USA
accurate method for the analysis of
TxA₂ production in patientsDid you know, up to
25-30% of patients on
What is aspirin resistance
low dose aspirin therapy or non-responsiveness?
are affected by aspirin
“resistance”?
Aspirin is the foundation of antiplatelet Low-dose aspirin
therapy and is widely prescribed in the therapy is internationally
primary and secondary prevention of established as the primary
cardiovascular disease. However, not measure undertaken in
all patients receiving aspirin therapy the secondary prevention
respond in the same way with many of cardiovascular events -
suffering from a lack of aspirin effect, however, not all patients
also known as aspirin “resistance”. respond the same to
Clinical research has shown that aspirin therapy.
patients who have a sub-optimum
response to their aspirin therapy are
over three times more likely to die
from a heart attack or stroke than
those who respond positively to such
therapy.
Clinical aspirin
The identification of these patients resistance is the
can be significantly improved through failure of aspirin
to prevent clinical
the use of Randox TxBCardio. Results
atherothromboembolic
generated by the Randox TxBCardio ischemic events in
assay can be used to enable timely patients who have been
intervention by clinicians with patients prescribed aspirin1.
deemed to be at increased risk. Patient
management can then be altered
via improved patient compliance,
• Conservative estimates • All aspirin resistant patients,
increased aspirin dosage levels and/ indicate that the prevalence regardless of underlying
or combination therapies with other of aspirin non-responsiveness clinical symptoms, were at
drugs. (or resistance) is 25-30% of greater risk of death, ACS or
all patients on aspirin therapy a new cerebrovascular event2
Randox TxBCardio offers a rapid, • A recent meta-analysis • Aspirin resistant patients
convenient and highly accurate option covering 20 studies and 2930 have been shown to be at
for the evaluation of aspirin response. patients found that 28% were 2-fold increased risk of a
aspirin resistant2 cardiovascular event and 3.5-
fold increased risk of death3What are the potential causes
of aspirin non-responsiveness?
educed bioavailability of
R Genetic factors that make What is
aspirin1
• Inadequate intake of aspirin (poor
patients less sensitive to the
atherothrombotic effects of
11-dehydro
compliance)
• Inadequate dose of aspirin5
aspirin1
• Polymorphisms of COX-1, COX-
Thromboxane B2?
• Reduced absorption or increased 2 or thromboxane A2-synthase
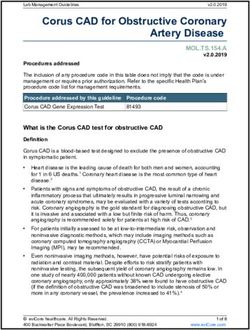
metabolism of aspirin • Polymorphisms of glycoprotein • Aspirin’s therapeutic effect primarily
receptors (e.g. Ia/IIa) inhibits the COX-1 pathway and
Increased turnover of results in decreased production of
Thromboxane A2 (TxA2). (Fig. 1)
platelets Competitive interference by
• Increased release of platelets from other non-steroid
bone marrow in response to stress, • Aspirin also inhibits the COX-2
anti-inflammatory drugs pathway, but to a much lesser extent
(e.g. after coronary artery bypass
(NSAIDS)1 than COX-1. Low-dose aspirin
surgery) introduces newly formed blocks more than 95% of platelet
platelets, unexposed to aspirin into • For example, ibuprofen,
COX-1 activity.
blood6 indometacin
The resulting decrease in the levels of
Diet and lifestyle factors Alternative pathways of TxA2 reduces the ability of platelets to
• Smoking9 platelet activation6 aggregate and therefore the likelihood of
• Excessive physical exercise or • Generation of thromboxane by blood clots in atherosclerotic arteries.
mental stress10 pathways not blocked by aspirin Measurement of TxA2 as an assessment
(e.g. COX-2) of aspirin response is not practical
Reduced efficacy of due to its very short half-life in blood.
aspirin with prolonged Hypercholesterolemia7 However, TxA2 is rapidly hydrolyzed
non-enzymatically to form TxB2. (Fig. 1)
administration
Diabetes mellitus8
(tachyphylaxis)8
Fig. 1: Diagram of the cyclooxygenase (COX-1) platelet activation pathway
Low-dose
COX-2 aspirin
TxA2 PGH2 ARACHIDONIC PGH2 TxA2
TX-synthase ACID TX-synthase
COX-1
TxB2
Urinary II-dehydro thromboxane B2Although it is possible to
measure TxB2 in serum or
plasma, much of this TxB2
is due to ex-vivo platelet
activation during sample
testing, or intra-renal
production.
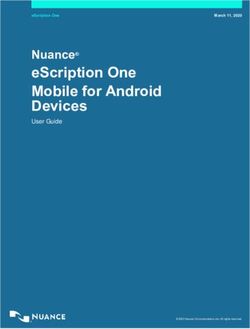
Fig. 2a: Aspirin effect correlates to low urinary 11dhTxB2
However, once cleared through the
kidneys, TxB2 forms a number of TxB 2 TxB 2
metabolites, the most abundant of TxA 2
TxA 2
TxB 2
which is 11-dehydro Thromboxane B2 Platelets Liver
(11dhTxB2).
LOW
11dhTxB2
11dhTxB2
• 11dhTxB2 has a long circulating Urinary II-dehydro TxA2
thromboxane B2
half-life and is extremely stable Kidney
in urine, hence making it a highly TxB2
valuable and practical measure of 11dhTxB2
TxA2 production
11dhTxB2
11dhTxB2
11dhTxB2
• Low levels of urinary 11dhTxB2 Urine
correlate to low levels of TxA2
production, and hence a clinically
acceptable level of aspirin
response (Fig. 2a) Fig. 2b: Lack of Aspirin effect correlates to high urinary 11dhTxB2
• High levels of urinary 11dhTxB2
correlate to higher levels of TxA2
production, and hence a lack of
TxB 2
TxB 2 TxB 2
TxB 2
response to the prescribed aspirin
TxA 2
TxA 2 TxA 2
TxA 2
TxB 2
therapy (Fig. 2b)
TxB 2
Platelets Liver
HIGH
11dhTxB2
11dhTxB2
• Large multi-national clinical trials
11dhTxB2
11dhTxB2
11dhTxB2
have shown that 11dhTxB2 is Urinary II-dehydro TxA2
thromboxane B2
an excellent measure of aspirin
Kidney
response and increased levels TxB2
correlate with significantly 11dhTxB2
11dhTxB2
increased risk of cardiovascular
11dhTxB2
11dhTxB2
11dhTxB2
11dhTxB2
11dhTxB2
11dhTxB2
events & death 3 11
11dhTxB2
11dhTxB2
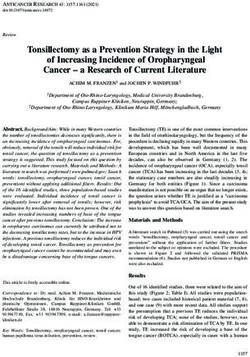
UrineThe HOPE study (Eikelboom et al 2002)3
Methods Results
Sub-study of the Canadian-based HOPE trial (Heart Patients in the upper quartile also had a 2-fold higher
Outcome Prevention Evaluation). risk of Myocardial Infarction and a 3.5-fold higher risk
of cardiovascular death. (Fig. 4)
Baseline urinary 11dhTxB2 samples were measured
in 976 aspirin-treated patients at high risk of
cardiovascular events.
Using a case-control design, 488 of these patients had
Conclusions
a cardiovascular event (MI, stroke or cardiovascular
death) during five years of follow-up, which were
compared with 488 sex and age matched control
patients who had no event.
In aspirin-treated patients, urinary concentrations of
11dhTxB2 predict future risk of myocardial infarction
and cardiovascular death.
The associated risk was strong, graded and
Results
independent of conventional vascular risk factors.
These findings indicate that 11dhTxB2 can be used to
Patients in the upper quartile of urinary 11dhTxB2 identify patients who are relatively resistant to aspirin
had a composite risk (MI, stroke, cardiovascular death and who may benefit from additional anti-platelet
within five years) of 1.8 times-higher than those in the therapies or treatments, which may be more effective.
lower quartile. (Fig. 3)
Fig. 3: Increasing levels of 11dhTxB2 correlates to Fig. 4: Adjusted odds ratio of future MI and CV death
increasing risk of MI, Stroke or CV death according to baseline 11dhTxB2
2
1.8
Odds ratio for MI, Stroke or CV death
1.6 1.8 4
1.4 3.5
1.2 1.4 3 3.5
1.3
Adjusted Odds Ratio
1 2.5
0.8 1 2
0.6 1.5 2
0.4 1
1
0.2 0.5
0 33.8 0 Control MI CV Death
Urinary 11dhTxB2 (ng/mmol creatinine) Outcome after 5-year follow-upThe CHARISMA study
(Eikelboom et al 2008)11
Results
Age, female sex, history of peripheral artery
disease, current smoking, and oral hypoglycaemic
Methods
or angiotensin-converting enzyme inhibitor were
independently associated with high concentrations
of 11dhTxB2.
Pre-defined sub-study from the CHARISMA trial – a Aspirin (ASA) >150mg/d, history of NSAIDS, history
multi-centre, multi-national, randomised, parallel group, of hypercholesterolemia and statin treatment were
double-blind trial of clopidogrel vs placebo in high-risk associated with low concentrations of 11dhTxB2.
patients at risk of atherothrombotic events. (Fig. 6)
A total of 3261 patients from 224 sites in 12 Randomisation to clopidogrel did not reduce the
countries provided first-morning urine samples at least hazard of cardiovascular events in patients with the
one month after randomisation. highest quartile of 11dhTxB2. However, statin therapy
was found to reduce levels.
Designed as a follow-up to the HOPE study, in order
to establish if the findings on 11dhTxB2 could be
Conclusions
externally validated in an independent data set.
In aspirin-treated patients, urinary 11dhTxB2 is an
externally valid and potentially modifiable determinant
of stroke, MI or cardiovascular death.
Results CHARISMA also supports previous work
demonstrating higher doses of aspirin (e.g. raising
High levels of 11dhTxB2 are independently associated from 81mg to >150mg) can be used to lower levels
with increased risk of serious cardiovascular events. of 11dhTxB2 and therefore modify patient risk.
(Fig. 5) Statin therapy appears to be more effective than
clopidogrel for the reduction of high 11dhTxB2 levels.
This may be due to the anti-inflammatory effect of
certain statins noted in recent studies.
Fig. 5: Adjusted odds ratio of composite risk for future Fig. 6: Effect of ASA dose on urinary 11dhTxB2
MI, Stroke or CV death according to baseline 11dhTxB2 concentrations
62
Adjusted Composite Risk of Stroke, MI or CV death
1.8 60
59.8
Median IIdhTxB2 (ng/mmol) creatinine
1.6 58 (n=765)
1.66 58.7
1.4 56 (n=2018)
1.2 54
1 52
0.8 1 50
50.3
0.6 48 (n=475)
0.4 46
0.2 44
0 Lowest quartile Highest quartile 0Randox TxB Utilising TxBCardio to
Cardio assay optimise patient therapy
Aspirin is the foundation of
antiplatelet therapy and is
widely prescribed in the primary Test Results
and secondary prevention of
cardiovascular disease. Aspirin “non-
responsiveness” is a serious clinical > 1500 pg/mg*
≤ 1500 pg/mg*
problem and is estimated to affect up No aspirin
aspirin Effect
to 25-30% of patients on low dose Effect
aspirin therapy.
• The target of the Randox
TxBCardio assay, 11dhTxB2,
has been clinically validated Aspirin Ensure
as a independent predictor of Ingested Compliance
myocardial infarction (2-fold risk)
and cardiovascular death (3.5-fold
risk) in patients suffering from a
lack of aspirin effect
Check for concomitant Ibuprofen
Step or NSAID usage
• Patients receiving aspirin, with 1 - this can inhibit effect of aspirin
elevated TxBCardio, can be
designated as “non-responsive”
to aspirin and an individualised Step Modify aspirin dose
approach to patient management 2
Retest
can then be used to reduce their
cardiovascular risk Step Check for elevated cholesterol
3 - this is after aspirin’s effect
• Randox TxBCardio is an
automated clinical chemistry Lower and Control Cholesterol
assay for the urinary assessment
of 11dhTxB2. The assay can
be used on a wide range of Step
Consider underlying condition
analysers commonly found in 4 i.e. Pre-Diabetes/Diabetes
most biochemistry laboratories
If results remain > 1500 pg/mg* with no aspirin effect consider changing dose;
additional and/or alternative anti-platelet therapy
* pg 11dhTxB2 / mg Creatinine
References
1. Hankey GJ et al. Aspirin resistance. Lancet. 2006 Feb 5. De Gaetano G et al. Aspirin resistance: a revival of platelet 9. Sane DC et al. Frequency of aspirin resistance in patients
18;367(9510): 606-17. Review. aggregation tests? J Thromb Haemost 2003;1: 2048–50. with congestive heart failure treated with antecedent
aspirin. Am J Cardiol 2002;90: 893–5.
2. Krasopoulos G et al. Aspirin “resistance” and risk of 6. Rocca B et al. Cyclooxygenase-2 expression is induced
cardiovascular morbidity: systematic review and meta- during human megakaryopoiesis and characterizes newly 10. Mustonen P et al. Epinephrine – via activation of p38-MAPK
analysis. BMJ. 2008;336(7637):195-8. formed platelets. Proc Natl Acad Sci USA 2002;99: – abolishes the effect of aspirin on platelet deposition to
7634–9. collagen.Thromb Res 2001;104: 439–49.
3. Eikelboom JW et al. Aspirin-resistant thromboxane
biosynthesis and the risk of myocardial infarction, stroke, 7. Szczeklik A et al. Inhibition of thrombin generation by 11. Eikelboom et al. Incomplete inhibition of thromboxane
or cardiovascular death in patients at high risk for aspirin is blunted in hypercholesterolemia. Arterioscler biosynthesis by acetylsalicylic acid: determinants and effect
cardiovascular events. Circulation. 2002;105(14):1650-5. Thromb Vasc Biol 1996;16: 948–54. on cardiovascular risk. Circulation. 2008:118(17):1705-12.
4. Snoep JD et al. Association of laboratory-defined aspirin 8. Fitzgerald R et al. Aspirin resistance: Effect of clinical,
resistance with a higher risk of recurrent cardiovascular biochemical and genetic factors. Pharmacol Ther.
events: a systematic review and meta-analysis. Arch Intern 2011;130(2):213-25.
Med. 2007 13-27;167(15):1593-9.
LT296 APR14
Randox Laboratories Limited, 55 Diamond Road, Crumlin, County Antrim, BT29 4QY, United Kingdom
T +44 (0) 28 9442 2413 F +44 (0) 28 9445 2912 E marketing@randox.com I www.randox.com
Information correct at time of print. Randox Laboratories Limited is a subsidiary of Randox Holdings Limited a company registered within Northern Ireland with company number N.I. 614690. VAT Registered Number: GB 151 6827 08.
Product availability may vary from country to country. Please contact your local Randox representative for information. Products may be for Research Use Only and not for use in diagnostic procedures in the USA.You can also read