Association of Chromosome 9p21 With Subsequent Coronary Heart Disease Events - ETIS
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Circulation: Genomic and Precision Medicine
ORIGINAL ARTICLE
Association of Chromosome 9p21 With
Subsequent Coronary Heart Disease Events
A GENIUS-CHD Study of Individual Participant Data
BACKGROUND: Genetic variation at chromosome 9p21 is a recognized Riyaz S. Patel, MD*
risk factor for coronary heart disease (CHD). However, its effect on disease Amand F. Schmidt, PhD*
progression and subsequent events is unclear, raising questions about its Vinicius Tragante, PhD*
value for stratification of residual risk. et al
METHODS: A variant at chromosome 9p21 (rs1333049) was tested
for association with subsequent events during follow-up in 103 357
Europeans with established CHD at baseline from the GENIUS-CHD
(Genetics of Subsequent Coronary Heart Disease) Consortium (73.1%
male, mean age 62.9 years). The primary outcome, subsequent CHD
death or myocardial infarction (CHD death/myocardial infarction),
occurred in 13 040 of the 93 115 participants with available outcome
data. Effect estimates were compared with case/control risk obtained
Downloaded from http://ahajournals.org by on June 27, 2019
from the CARDIoGRAMplusC4D consortium (Coronary Artery Disease
Genome-wide Replication and Meta-analysis [CARDIoGRAM] plus The
Coronary Artery Disease [C4D] Genetics) including 47 222 CHD cases and
122 264 controls free of CHD.
RESULTS: Meta-analyses revealed no significant association between
chromosome 9p21 and the primary outcome of CHD death/myocardial
infarction among those with established CHD at baseline (GENIUS-
CHD odds ratio, 1.02; 95% CI, 0.99–1.05). This contrasted with a *Drs Patel, Schmidt, and Tragante are
strong association in CARDIoGRAMPlusC4D odds ratio 1.20; 95% CI, joint first authors
1.18–1.22; P for interactionPatel et al; Chromosome 9p21 and Subsequent CHD Events
U RESULTS
sing a case-control approach, a large number
of common genetic variants have now been
In total, 49 studies from the GENIUS-CHD consor-
associated with coronary heart disease (CHD)
tium contributed to the federated analysis resulting
through genome-wide association studies, in an ef-
in a sample size of 103 357 individuals of European
fort largely led by the CARDIoGRAMPlusC4D consor-
descent with established CHD and available genotype
tium (Coronary Artery Disease Genome-wide Rep-
data at the 9p21 locus. Of these, 93 115 individuals
lication and Meta-analysis [CARDIoGRAM] plus The
had available data for the primary composite outcome
Coronary Artery Disease [C4D] Genetics).1 Among
of subsequent CHD death/myocardial infarction (MI),
these variants, the chromosome 9p21 locus was the
of whom 13 040 experienced these events. Contrib-
first to be discovered and the variant with the largest
uting study details are provided in Table. Participant
individual effect and is the most widely replicated ge-
characteristics are representative for populations with
netic risk factor for CHD.2–4 Multiple studies including
established CHD with a weighted mean age of 62.9
case-control and prospective cohort studies in general
years; 73.1% male. As expected, risk factor preva-
populations have reliably confirmed its effect on risk
lence was high in this population, including diabetes
of CHD among otherwise healthy individuals.5
mellitus (24.4%), hypertension (59.1%), and current
However, it is uncertain whether variants at the 9p21
smoking (25.7%). Statin use at enrollment varied by
locus also affect risk of recurrent or subsequent events,
including mortality in those with established CHD. Elu- study, ranging from 5.2% to 97.3%, with a median
cidation of this hypothesis would help to better under- of 61.5% (Table).
stand its mechanism and estimate its incremental value The rs1333049 single nucleotide polymorphism
for stratification of residual risk. Prior studies have shown was genotyped in 42 studies, with the remaining 7
conflicting results, although most have been underpow- studies using highly correlated proxies (R2>0.90);
ered. A literature-based meta-analysis indicated a null rs10757278 (4 studies) or rs4977574 (3 studies) when
association of chromosome 9p21 variants with subse- the primary single nucleotide polymorphism was
quent CHD events but was based on summary, not indi- unavailable. Genotyping details are provided in Table I
vidual level data, with varying outcome definitions.6,7 in the Data Supplement. For rs1333049, the average
The new collaborative GENIUS-CHD (Genetics of risk allele frequency across the participating studies
Subsequent Coronary Heart Disease) consortium, was 0.518 ranging from 0.453 to 0.587 (Figure I in
the Data Supplement).
Downloaded from http://ahajournals.org by on June 27, 2019
described in this issue of the journal, was established to
investigate genetic determinants of disease progression From CARDIOGRAMplusC4D, after excluding 6
following an index CHD event.8 cohorts which had contributed data to both consortia,
In this article, we use the GENIUS-CHD resource to: (1) data were available for association with chromosome
examine the association of variants at the 9p21 locus on 9p21 from 41 studies, including 47 222 cases with CHD
risk of subsequent CHD events in individuals with estab- and 122 264 controls free of any CHD.
lished CHD; (2) compare these to the association between Power to detect different effect sizes, including the
chromosome 9p21 and any CHD observed in the CARDIo- effect size identified in CARDIoGRAMplusC4D, using a
GRAMPlusC4D consortium; and (3) explore the potential 2-sided alpha of 0.05, are provided in Table II in the
impact on these estimates of biases that might affect genet- Data Supplement.
ic association studies of disease outcome and prognosis.
Chromosome 9p21 Association With
Subsequent CHD Events
METHODS
In accordance with Transparency and Openness Promotion Study-specific results for the association between chro-
Guidelines, the data, analytic methods, and study materi- mosome 9p21 and risk of the primary outcome of CHD
als will be made available to other researchers for purposes death or MI among individuals with established CHD
of reproducing the results or replicating the procedure. at baseline, adjusted for age and sex are presented in
Participating studies received local institutional review board Figure II in the Data Supplement.
approval and included patients who had provided informed The per-allele odds ratio (OR) for the primary out-
consent at the time of enrollment. The central analysis sites come during follow-up was 1.02 (95% CI, 0.99–1.05).
also received waivers from their local institutional review
The effect estimate again for the primary outcome,
board for collating and analysing summary level data from
based on a time to event analysis and using a Cox
these individual studies. Details about the GENIUS-CHD
consortium and study inclusion criteria have been published regression model, was also similar with a hazard ratio
separately in this issue of the journal,8 whereas for this study of 1.02 (95% CI, 0.99–1.04; Figure III in the Data
full details about data sources, genetic variant selection, Supplement).
outcomes and statistical analyses are available in the Data In contrast, a meta-analysis of CARDIOGRAMIplus
Supplement. C4D data (excluding studies also contributing data to
Circ Genom Precis Med. 2019;12:e002471. DOI: 10.1161/CIRCGEN.119.002471 April 2019 162Downloaded from http://ahajournals.org by on June 27, 2019
Table. Overview of Studies Contributing to Chromosome 9p21 Analysis and Participant Characteristics
Diabetes Total Statin Prior Prior
Total N Study CHD Male, mellitus, Smoking, Systolic BP, Cholesterol, use, Creatinine, Revasc, MI, PubMED
Alias Cohort genotyped Design Type % Age, y, SD BMI (SD) % % SD SD % SD % % ID
4C Clinical Cohorts in 1538 Cohort CAD 62.1 62.2 (11.95) 30.2 (5.67) 23.4 … 133.9 (23.7) 4.69 (1.10) 26.4 99.3 (83.2) 22.6 15.5 …
Coronary disease
Collaboration (4C)
AGNES Arrhythmia Genetics in 1316 Cohort ACS 79.3 57.7 (10.81) 26.5 (3.87) 7.6 59.3 … 5.28 (1.04) 9.8 … … … 20622880
the Netherlands
ANGES Angiography and 588 Cohort Mixed 65.5 64.1 (9.55) 28.1 (4.36) 30.8 14.7 … 4.84 (0.84) 69.4 83.0 (32.0) 42.4 24.7 21640993
Genes Study
ATVB Italian Atherosclerosis, 1465 Cohort ACS 90.4 40.0 (4.40) 26.8 (4.07) 8.4 78.7 132.3 (20.6) 5.76 (1.39) 56.2 … … … 21757122
Thrombosis and
Vascular Biology Group
CABGenomics Coronary Artery Bypass 1542 Cohort Mixed 80.1 64.7 (10.08) 29.7 (5.71) 10.1 11.2 … 4.21 (0.95) 75.2 … … 42.8 25649697
Genomics
CDCS Coronary Disease 1800 Cohort ACS 71.5 67.5 (11.96) 27.3 (4.66) 15.4 5.8 129.2 (21.6) 5.00 (1.09) 46.5 100.5 (40.0) 26.9 30.3 20400779
Cohort Study
Patel et al; Chromosome 9p21 and Subsequent CHD Events
COROGENE Corogene Study 1489 Cohort ACS 70.9 64.7 (11.87) 27.6 (4.84) 18.2 34.4 … 4.63 (0.99) 5.2 84.0 (44.3) … … 21642350
CTMM Circulating Cells 605 Cohort Mixed 68.9 63.0 (9.83) 27.6 (4.45) 20.7 20.7 135.4 (19.1) 4.43 (1.05) … 86.4 (34.9) … 30.1 23975238
CURE Cure-Genetics Study 4242 RCT ACS 59.3 64.7 (10.99) 27.9 (4.44) 19.9 22.6 135.7 (21.9) … … 93.0 (33.9) 13.9 31.8 11102254
EGCUT Estonian Biobank 2408 Cohort CAD 51.0 67.1 (10.88) 28.9 (5.16) 18.7 19.2 135.6 (18.0) 5.64 (1.17) 27.3 … 15.7 36.0 24518929
EMORY Emory Cardiovascular 2411 Cohort Mixed 70.1 64.5 (11.06) … 30.7 9.8 … 4.49 (1.02) 76.0 99.0 (45.1) 61.7 27.9 20729229
Biobank
Circ Genom Precis Med. 2019;12:e002471. DOI: 10.1161/CIRCGEN.119.002471
ERICO Estratégia de Registro 438 Cohort ACS 55.5 63.8 (13.36) 27.0 (5.06) 39.1 31.0 99.2 (38.4) … 23.8 … 11.3 25.9 23644870
de Insuficiência
Coronariana
FINCAVAS Finnish Cardiovascular 1671 Cohort Mixed 69.4 60.9 (11.03) 27.8 (4.35) 18.4 24.3 140.2 (22.1) 4.74 (0.90) 57.3 90.8 (66.8) 32.6 39.0 16515696
Study
FRISCII FRISCII Study 3106 RCT ACS 69.4 66.2 (9.80) 26.8 (3.87) 12.7 27.1 143.3 (22.4) 5.80 (1.12) 12.3 90.6 (18.8) 12.1 27.2 10475181
GENDEMIP Genetic Determination 1267 Cohort ACS 75.8 56.4 (8.63) 28.6 (4.68) 18.8 60.8 137.0 (20.8) 5.51 (1.17) 16.6 … 29.7 41.6 23249639
of Myocardial
Infarction in Prague
GENEBANK Cleveland Clinic 2345 Cohort Mixed 74.3 61.5 (11.06) 29.4 (5.44) 11.8 16.8 132.7 (21.1) 4.46 (0.93) 71.8 … 65.3 56.1 21475195
Genebank Study
GENESIS-PRAXY Gender and Sex 784 Cohort ACS 69.2 48.3 (5.62) … 13.8 44.2 139.5 (26.5) 4.85 (1.18) 93.1 75.9 (19.7) 11.3 11.4 22607849
Determinants of
Cardiovascular Disease:
From Bench to Beyond-
Premature Acute
Coronary Syndrome
April 2019
(Continued )
163Downloaded from http://ahajournals.org by on June 27, 2019
Table. Continued
Diabetes Total Statin Prior Prior
Total N Study CHD Male, mellitus, Smoking, Systolic BP, Cholesterol, use, Creatinine, Revasc, MI, PubMED
Alias Cohort genotyped Design Type % Age, y, SD BMI (SD) % % SD SD % SD % % ID
GENOCOR Genetic Mapping 497 Cohort Mixed 86.7 65.2 (8.45) … 13.3 64.4 129.5 (20.3) 4.70 (0.92) 72.1 94.8 (27.2) 13.7 63.2 22717531
for Assessment of
Cardiovascular Risk
GoDARTS incident Genetics of Diabetes 1003 Cohort CAD 62.0 71.1 (10.62) 29.7 (5.64) 77.9 … 126.7 (NA) 4.62 (1.02) 50.8 108.0 (64.6) 0.2 1.3 …
Audit and Research in
Tayside Scotland (I)
GoDARTS prevalent Genetics of Diabetes 2000 Cohort CAD 66.5 69.1 (9.20) 30.3 (5.43) 77.8 14.9 136.2 (19.7) 4.37 (0.83) 66.8 101.6 (34.5) 31.4 48.9 …
Audit and Research in
Tayside Scotland (P)
GRACE_B Global Registry of 699 Cohort ACS 75.4 65.7 (12.01) 27.0 (4.35) 81.3 49.9 138.8 (25.3) 5.33 (1.19) 79.3 102.8 (61.9) … 80.1 20231156
Acute Coronary
Events–Belgium
GRACE_UK Global Registry of Acute 1086 Cohort ACS 69.1 64.4 (12.04) 28.0 (5.15) 15.0 69.5 137.8 (27.1) 5.19 (1.29) 16.8 105.0 (40.0) 20.4 32.0 20231156
Coronary Events - UK
IDEAL Incremental Decrease 6223 RCT ACS 81.8 61.2 (9.32) 27.4 (3.80) 11.4 20.3 136.8 (19.8) 5.03 (0.98) 76.9 100.1 (16.7) 41.3 … 16287954
Patel et al; Chromosome 9p21 and Subsequent CHD Events
in End Points Through
Aggressive lipid
Lowering
INTERMOUNTAIN Intermountain Heart 6763 Cohort Mixed 66.7 61.2 (11.05) 29.5 (6.08) 20.3 10.2 141.8 (24.4) 4.96 (1.12) 38.7 99.6 (66.6) … 6.6 20691829
Collaborative Study
INVEST International Verapamil 2145 RCT CAD 56.6 68.7 (9.38) … 23.9 12.8 148.6 (18.1) … 52.8 … 47.6 … 21372283
SR Trandolopril Study
Circ Genom Precis Med. 2019;12:e002471. DOI: 10.1161/CIRCGEN.119.002471
Genetic Substudy
JUMC Krakow-GENIUS-CHD 704 Cohort Mixed 71.6 68.3 (10.25) 26.3 (4.46) 36.9 27.5 148.1 (23.8) 5.02 (1.06) 88.3 89.9 (37.5) 50.1 39.7 28444280
KAROLA Karola Study 1147 Cohort Mixed 84.6 58.6 (8.13) 27.0 (3.26) 18.5 32.4 119.9 (15.5) 4.46 (0.84) 77.4 82.4 (26.5) 42.8 21.6 24829374
LIFE-Heart Leipzig (LIFE) Heart Study 4330 Cohort Mixed 75.5 64.0 (11.15) 29.0 (4.68) 34.4 29.0 138.3 (21.8) 5.24 (1.18) 38.9 87.3 (34.6) … 0.1 22216169
LURIC The Ludwigshafen Risk 2175 Cohort Mixed 76.5 63.8 (9.85) 27.5 (3.89) 44.3 23.9 142.3 (24.1) 4.94 (0.99) 58.9 88.7 (38.5) 48.7 57.4 11258203
and Cardiovascular
Health Study
NE_POLAND North East Poland 603 Cohort ACS 75.0 62.4 (11.86) 24.8 (3.79) 22.2 48.1 138.9 (27.4) 5.04 (1.05) 80.7 91.6 (36.3) 1.3 10.6 26086777
Myocardial Infarction
Study
NEAPOLIS Neapolis Campania Italia 1380 Cohort Mixed 74.4 67.6 (10.49) 28.0 (4.18) 43.0 26.8 129.4 (14.2) 4.57 (1.02) 82.5 101.0 (68.1) 41.5 40.8 24262617
OHGS Ottawa Heart 393 Cohort Mixed 73.0 65.3 (11.07) 28.6 (5.00) 6.9 19.5 131.9 (19.0) 5.53 (1.03) 92.4 89.8 (21.1) 28.2 21.9 …
Genomics Study
PLATO The Study of Platelet 9814 RCT ACS 69.5 62.6 (10.95) 28.2 (4.51) 22.8 35.2 135.6 (21.8) 5.42 (1.23) 79.7 85.6 (26.3) 15.1 20.6 19332184
Inhibition and Patient
Outcomes
April 2019
PMI Post Myocardial 783 Cohort ACS 78.3 62.7 (10.29) 26.5 (3.82) 12.0 28.2 117.0 (15.6) 5.98 (1.19) 46.0 87.8 (27.8) … 17.2 12771003
Infarction Study
164
(Continued )Downloaded from http://ahajournals.org by on June 27, 2019
Table. Continued
Diabetes Total Statin Prior Prior
Total N Study CHD Male, mellitus, Smoking, Systolic BP, Cholesterol, use, Creatinine, Revasc, MI, PubMED
Alias Cohort genotyped Design Type % Age, y, SD BMI (SD) % % SD SD % SD % % ID
POPular The Popular study 997 RCT ACS 74.3 63.8 (10.40) … 18.9 27.5 145.0 (22.1) 4.25 (0.64) 80.7 92.7 (26.8) 33.1 43.7 26542508
PROSPER Prospective Study 439 RCT CAD 69.9 75.4 (3.31) 26.4 (3.87) 10.3 16.2 150.0 (21.6) 5.55 (0.83) … 109.4 (23.2) 26.0 85.9 10569329
of Pravastatin in the
Elderly at Risk
RISCA Recurrance and 1052 Cohort ACS 75.9 61.9 (11.40) 27.2 (4.43) 19.8 30.4 … … 46.6 100.6 (28.6) 28.2 27.9 18549920
Inflammation in
the Acute Coronary
Syndromes Study
SHEEP Stockholm Heart 1150 Cohort ACS 70.7 59.3 (7.21) 26.8 (4.02) 18.2 50.0 131.8 (20.6) 6.28 (1.16) … … … … 17667644
Epidemiology Program
SMART Second Manifestations 2485 Cohort Mixed 82.2 60.2 (9.26) 27.3 (3.63) 16.6 24.4 137.4 (19.8) 4.73 (0.96) 75.7 92.3 (22.7) … 43.6 10468526
of Arterial Disease
STABILITY Stabilization of 9287 RCT Mixed 82.0 64.7 (9.10) 29.9 (4.97) 38.4 21.4 131.7 (16.1) … 97.3 … 74.6 58.6 24678955
Atherosclerotic
Patel et al; Chromosome 9p21 and Subsequent CHD Events
Plaque by Initiation of
Darapladib Therapy
trial
THI Texgen 2729 Cohort ACS 75.3 63.6 (10.62) 29.6 (5.59) 30.5 21.3 … … 57.1 … 21.5 16.7 21414601
TNT Treating to New Targets 5104 RCT CAD 81.3 61.3 (8.73) 28.6 (4.59) 14.8 13.4 130.9 (16.8) 4.51 (0.61) 70.3 104.8 (17.3) … 57.3 15755765
TRIUMPH Translational Research 1974 Cohort ACS 72.4 59.8 (12.04) 29.5 (5.96) 28.6 37.4 117.8 (18.3) … 89.0 112.5 (76.7) 27.0 18.3 21772003
Investigating
Circ Genom Precis Med. 2019;12:e002471. DOI: 10.1161/CIRCGEN.119.002471
Underlying Disparities
in Acute Myocardial
Infarction Patient’s
Health Status
UCORBIO Utrecht Coronary 1073 Cohort Mixed 75.6 65.4 (10.26) 27.2 (4.34) 21.5 23.1 … 4.76 (1.18) 64.0 91.9 (42.9) … 28.9 …
Biobank
UCP Utrecht Cardiovascular 1500 Cohort Mixed 75.4 64.1 (9.96) … … … 153.4 (21.4) 5.50 (1.10) 27.1 94.7 (24.8) … … 25652526
Pharmacogenetics
Study
VHS Verona Heart Study 907 Cohort CAD 80.9 61.3 (9.78) 26.9 (3.57) 18.5 69.2 … 5.37 (1.10) 47.1 96.7 (32.2) 17.4 59.6 10984565
VIVIT Vorarlberg Institute for 1318 Cohort CAD 73.1 64.5 (10.44) 27.4 (4.14) 30.6 18.9 137.2 (19.2) 5.45 (1.14) 49.7 88.4 (32.7) 21.1 31.0 24265174
Vascular Investigation
and Treatment Study
WARSAW ACS Warsaw ACS Genetic 669 Cohort ACS 74.5 63.6 (11.72) 28.1 (4.72) 21.9 42.0 127.8 (22.6) 4.99 (1.07) … 93.5 (41.4) … 18.6 …
Registry
WTCCC WTCCC CAD Study 1924 Cohort Mixed 79.3 60.0 (8.13) 27.6 (4.20) 11.7 12.8 143.6 (22.0) 5.28 (0.98) 71.6 … 67.1 72.0 17634449
April 2019
Overview of studies contributing to chromosome 9p21 analysis and participant characteristics; alias denotes the abbreviated name of each study used in figures and tables; PubMed IDs are provided for individual
study descriptions; mean (SD) with proportions (%) are provided unless otherwise stated. ACS indicates acute coronary syndrome; BMI, body mass index; BP, blood pressure; CAD, coronary artery disease; FRISC-II, Fast
Revascularization during InStability in Coronary artery disease; GENIUS-CHD, Genetics of Subsequent Coronary Heart Disease; JUMC, Jagiellonian University Medical College; KAROLA, Langzeitfolge der Kardiologischen
165
Anschlussheilbehandlung; LIFE, The Leipzig Heart Study; MI, myocardial infarction; RCT, randomized controlled trial; and WTCCC, Wellcome Trust Case Control Consortium.Patel et al; Chromosome 9p21 and Subsequent CHD Events
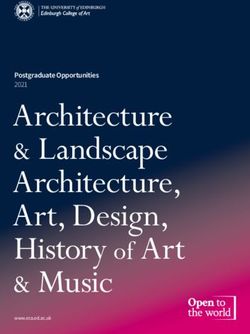
Figure 1. Association between chromosome 9p21 and subsequent coronary heart disease (CHD) events in all participants with baseline CHD
(GENIUS-CHD [Genetics of Subsequent Coronary Heart Disease]) compared with association in CHD cases and CHD-free controls (CARDIoGRAM-
PlusC4D).
For the CARDIoGRAMPlusC4D consortium (Coronary Artery Disease Genome wide Replication and Meta-analysis [CARDIoGRAM] plus The Coronary Artery Disease
[C4D] Genetics) meta-analysis estimate, 6 studies (LURIC, LIFE-Heart [The Leipzig Heart Study], GoDARTS [Genetics of Diabetes Audit and Research in Tayside Scot-
land], OHGS [Ottawa Heart Genomics Study], PROSPER [Prospective Study of Pravastatin in the Elderly at Risk], WTCCC [Welcome Trust Case Control Consortium])
were excluded as they were also included in GENIUS-CHD. Estimates for GENIUS-CHD are also presented by subtype of CHD at baseline, including acute coronary
syndrome (ACS), stable coronary artery disease (CAD) without prior myocardial infarction (MI; CAD/no MI), and stable CAD with prior MI (CAD/MI). All estimates
were adjusted for age and sex.
GENIUS-CHD), revealed a per-allele OR for a CHD event We further examined the effect of chromosome
similar to that reported previously (OR, 1.20; 95% CI, 9p21 on the primary outcome in prespecified subgroup
1.18–1.22). There was evidence of statistical hetero- analyses. We noted a borderline nominally significant
geneity between the estimates (interaction PPatel et al; Chromosome 9p21 and Subsequent CHD Events
Data Supplement). However, when ordered by date of 9p21 risk allele frequencies with advancing age, relative
first enrollment, there was no evidence for variation to younger carriers (Figure VI in the Data Supplement).
in effect by time of enrollment (Figure II in the Data
Supplement).
DISCUSSION
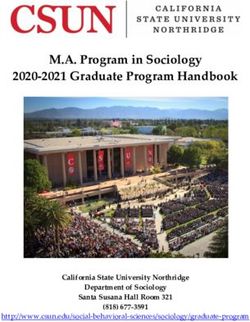
Secondary Outcomes In this study, we examined the effect of genetic varia-
tion at the chromosome 9p21 locus on risk of subse-
We additionally examined the association between chro- quent events in 103 357 individuals with established
mosome 9p21 and other subsequent events available for CHD using the newly formed GENIUS-CHD consor-
this analysis within the GENIUS-CHD Consortium, listed in tium.8 We found that (1) in contrast to the known
Table III in the Data Supplement, with summary estimates strong association with CHD observed in CARDIo-
provided in Figure 2. Of note, the per-allele effect of risk GRAMPlusC4D, there was a markedly attenuated and
variants at chromosome 9p21 on subsequent revascular- nonsignificant association with subsequent CHD events
ization during follow-up was 1.07 (95% CI, 1.04–1.09). in GENIUS-CHD; (2) effect estimates in GENIUS-CHD
The effect on the composite outcome of any cardiovas- were broadly consistent in stratified analyses based on
cular disease, which includes revascularization, was also features related to study design, patient characteris-
significant at 1.04 (95% CI, 1.02–1.07). However, there tics, and type of index CHD event; and (3) exploratory
was no clear evidence of association for the remaining analyses suggested that selection biases were unlikely
secondary outcomes, with only a marginal trend to pro- to explain the discrepancy. However, we did find evi-
tection for both subsequent heart failure (OR, 0.97; 95%, dence of an association between these variants and a
CI 0.93–1.01) and cardiovascular disease death (OR, 0.97; secondary outcome of future revascularization events.
95% CI, 0.94–1.01), as shown in Figure 2. Our findings, taken together with those from others,
support the view that chromosome 9p21 promotes
Selection Bias CHD through progressive stable atheroma rather than
through development of an unstable phenotype.
To explore the potential for index event bias, we The chromosome 9p21 locus is the most widely repli-
looked for differences in associations between chro- cated genetic risk locus for CHD identified to date, with
mosome 9p21 and known cardiovascular risk factors an estimated 15% to 35% increased risk in carriers of
Downloaded from http://ahajournals.org by on June 27, 2019
in the United Kingdom Biobank, among the subset the variant allele in prospective population and case-
of participants with established CHD, compared with control studies.5 However, studies examining the effect
the full UKB cohort (Table IV in the Data Supplement). on subsequent CHD events in people with known CHD
Although there were differences between the groups at baseline have reported conflicting results.10–14 Our
in the prevalence or values of the tested risk factors, group previously examined this in a literature-based
we did not find clear evidence to indicate a distortion meta-analysis, based on 15 studies with median sample
in associations between chromosome 9p21 and age, size of 1750 individuals, accruing 25 163 cases of estab-
blood pressure, diabetes mellitus, or smoking. There lished CHD, and reported no clear evidence of an effect
was, however, a small difference for body mass index, of variants at chromosome 9p21 on the risk of subse-
with a greater statistical association between the chro- quent events.6 An analysis by the CHARGE consortium
mosome 9p21 risk allele and lower body mass index (The Cohorts for Heart and Aging Research in Genomic
identified in those with established CHD than in the Epidemiology) of 2953 MI survivors also reported no
general population (nominal interaction P value 0.02, association with subsequent mortality.7 However, the
Table IV in the Data Supplement). limited size of most prior studies and the limitations
We also observed that the chromosome 9p21 risk of literature meta-analyses indicate that many possible
allele frequency in those surviving with CHD, both in explanations, including errors in risk allele coding and
UKB (0.529) and in GENIUS-CHD (0.518, Figure I in the selection biases, could not be adequately explored, pre-
Data Supplement), was higher than the general popula- cluding meaningful interpretations for any mechanistic
tion in the UKB (0.481) and European reference popula- or clinical implications.
tions from the 1000 Genomes (Phase 3),9 (0.472). This The emergence of the GENIUS-CHD Consortium has
difference in frequency confirms the association of chro- now permitted a robust evaluation of the role of chro-
mosome 9p21 with CHD and also indicated absence mosome 9p21 in subsequent CHD event risk, revealing
of a crude survival bias with loss of large numbers of a clear lack of association with a common compos-
risk allele carriers to fatal events before entry into CHD ite coronary end point. This is in marked contrast to
cohorts. We did, however, observe a trend to an age findings from studies comparing cases to CHD-free
association in those with established CHD, as well as the controls, as confirmed through meta-analysis of CAR-
general population in the UKB, with lower chromosome DIoGRAMPlusC4D data. Furthermore, we were able to
Circ Genom Precis Med. 2019;12:e002471. DOI: 10.1161/CIRCGEN.119.002471 April 2019 167Patel et al; Chromosome 9p21 and Subsequent CHD Events
add to previous findings by showing that the type of findings potentially argue against important selection
CHD at baseline, whether acute coronary syndrome or biases in the analysis for the primary outcome, they
stable CHD with or without prior MI, does not alter this are relatively insensitive assessments and may not fully
association. We also interrogated several widely pro- elucidate such biases.
posed explanations that could account for our findings Possible biological explanations could also exist for
through prespecified subgroup analyses and confirmed our findings. Pathological studies indicate differences
that most of these, specifically older age, medication between chronic stable atherosclerotic plaques that
use at baseline (statin or antiplatelet), study size or cause ischemia through progressive vessel occlusion
follow-up duration, did not appreciably alter the asso- and vulnerable plaques with thin caps, prone to sudden
ciation findings. Our finding of a possible interaction plaque rupture, unheralded MI, and coronary deaths.19
with sex, warrants further investigation but should be In a seminal study dissecting the phenotype of CHD, a
considered hypothesis-generating given the borderline lack of effect for chromosome 9p21 and MI was noted,
evidence of an interaction. when both cases and controls had underlying athero-
Selection bias (ie, index event bias or collider-strat- sclerosis.20 Our group and others have in parallel shown
ification bias) could potentially explain reversed or that chromosome 9p21 robustly associates with athero-
attenuated associations in disease progression studies sclerotic phenotypes,21 whereas functional studies have
like this, operating by inducing relationships between also implicated this region with molecular activity that
(otherwise independent) risk factors through the selec- drives atheroma.22 Furthermore, in this study, we show
tion of individuals with disease.15,16 Specifically, individ- that the only outcome positively associated with chro-
uals surviving a first event consequent on exposure to a mosome 9p21 is incident revascularization, perhaps
particularly strong risk factor may have lower levels of reflecting more severe atherosclerosis burden. Collec-
exposure to other individually weaker, independent risk tively, these data support the concept that chromosome
factors, which can then attenuate the association of the 9p21 promotes progressive atheroma formation and
risk factor of interest with subsequent events. However, does not confer risk via plaque rupture.
the distribution of common risk factors by chromosome In this context, it is worth noting that chromosome
9p21 genotype did not differ when compared between 9p21 associates more robustly with CHD in case-con-
the general population and the subset with CHD in the trol studies than in prospective cohort studies.7 The
UKB, using interaction tests. The only exception was for difference, as proposed by others, could hypothetical-
body mass index, a potentially differential association ly be accounted for by incidence-prevalence bias, with
Downloaded from http://ahajournals.org by on June 27, 2019
with chromosome 9p21 in those with CHD compared chromosome 9p21 carriers more likely to survive a
with the general population was noted. However, the CHD event and thus be over represented among CHD
effect size was small in both populations and on its cases (the opposite to survival bias described above).7
own is unlikely to indicate presence of substantial index This becomes more likely as stated above if chro-
event bias. mosome 9p21 drives a more progressive and stable
Selection bias may also theoretically occur by focus- atheroma phenotype. If this holds true, then among
ing on subjects surviving a first event, where chro- survivors with established CHD, one might expect that
mosome 9p21 risk allele carriers at risk of fatal CHD chromosome 9p21 carriers could hold a small favor-
events are lost before enrollment into CHD cohorts, able advantage over those who experience CHD in its
thereby diluting the future impact of the variant on absence, due instead to other more dangerous or vul-
subsequent CHD events. In this scenario, we would nerable characteristics, and despite undergoing more
expect a lower risk allele frequency in those surviv- subsequent revascularization, these chromosome
ing CHD and entering CHD cohorts, but we found no 9p21 carriers do not experience more dangerous or
evidence for this. Among those with CHD in the UKB, fatal events.
and among the whole UKB cohort, we did find a pro- These findings have important implications. Clini-
gressive loss of risk allele carriers with increasing age, cally, they indicate that a degree of caution should be
consistent with prior findings of a greater association applied when considering or evaluating patients for
with CHD, among younger individuals in case-control chromosome 9p21 to predict disease progression or
studies.5 Given patients with CHD are generally older, residual risk. They also highlight the need to appreci-
it is possible that a subtle survival bias may still be ate important biases that may inflate or attenuate asso-
influencing our findings, although all analyses were ciation findings in the setting of subsequent events for
adjusted for age. However, based on simulation mod- individuals with established disease. Mechanistically,
eling, sample size, and projected single nucleotide these findings support existing and emerging efforts
polymorphism effect size, we and others have previ- seeking to elucidate the mechanism of the most robust
ously estimated that selection biases are only minimal- genetic discovery for CHD in recent decades.
ly operating in this context and would be unlikely to There are important limitations to consider. First,
account for our observed findings.17,18 Although our among individuals in GENIUS with established CHD,
Circ Genom Precis Med. 2019;12:e002471. DOI: 10.1161/CIRCGEN.119.002471 April 2019 168Patel et al; Chromosome 9p21 and Subsequent CHD Events
the timing of the first CHD event or age of onset was view that chromosome 9p21 promotes CHD through
often unknown, so we could not account for this vari- progressive stable atheroma rather than through devel-
able in our analyses. However, the lack of association in opment of an unstable phenotype.
the acute coronary syndrome studies, which had docu-
mented timing of the first event, suggests this did not
impact the findings. Second, we had limited informa- ARTICLE INFORMATION
tion on whether subsequent revascularization events Received February 4, 2019; accepted March 18, 2019.
were late staged procedures, which would count as The Data Supplement is available at https://www.ahajournals.org/doi/sup-
pl/10.1161/CIRCGEN.119.002471.
part of the index CHD event or unplanned and symp-
tom driven and thereby a true subsequent event, which
Authors
may have diluted the effect estimate. Third, although
Riyaz S. Patel, MD*; Amand F. Schmidt, PhD*; Vinicius Tragante, PhD*; Ray-
we did not observe a specific interaction for statin or mond O. McCubrey, MS; Michael V. Holmes, MD, PhD; Laurence J. Howe,
aspirin use, we cannot rule out an effect of combined PhD; Kenan Direk, PhD; Axel Åkerblom, MD, PhD; Karin Leander, PhD; Salim
or additional medication usage attenuating the asso- S. Virani, MD, PhD; Karol A. Kaminski, MD, PhD; Jochen D. Muehlschlegel,
MD, MMSc; Marie-Pierre Dubé, PhD, Hooman Allayee, PhD; Peter Almgren,
ciation signal, given the high prevalence of second- MSc; Maris Alver, MSc; Ekaterina V. Baranova, MSc; Hassan Behlouli, PhD; Bram
ary prevention drug use in this setting compared with Boeckx, PhD; Peter S. Braund, PhD; Lutz P. Breitling, MD; Graciela Delgado,
general population cohorts. Fourth, our analyses were MSc; Nubia E. Duarte, PhD; Line Dufresne, MSc; Niclas Eriksson, PhD; Luisa
Foco, PhD; Crystel M. Gijsberts, MD, PhD; Yan Gong, PhD; Jaana Hartiala, PhD;
restricted to participants of European descent as most Mahyar Heydarpour, PhD; Jaroslav A. Hubacek, DSc; Marcus Kleber, PhD; Daniel
of the included studies only recruited these individu- Kofink, PhD; Pekka Kuukasjärvi, MD, PhD; Vei-Vei Lee, MS; Andreas Leiherer,
als, and so we were markedly underpowered to explore PhD; Petra A. Lenzini, MS; Daniel Levin, PhD; Leo-Pekka Lyytikäinen, MD; Nicola
Martinelli, MD, PhD; Ute Mons, PhD, Christopher P. Nelson, PhD; Kjell Nikus,
associations in other ethnic groups. Unfortunately, MD, PhD; Anna P. Pilbrow, PhD; Rafal Ploski, MD, PhD; Yan V. Sun, PhD; Michael
this remains a wider problem of genetic research and W.T. Tanck, PhD; W.H.Wilson Tang, MD; Stella Trompet, PhD; Sander W. van der
global efforts are ongoing to address this imbalance. Laan, PhD; Jessica van Setten; Ragnar O. Vilmundarson, MSc; Chiara Viviani An-
selmi, PhD; Efthymia Vlachopoulou, PhD; Eric Boerwinkle, PhD; Carlo Briguori,
Finally, variability of follow-up duration across studies MD, PhD; John F. Carlquist, PhD; Kathryn F. Carruthers, MPhil; Gavino Casu,
is an analytical challenge and could have impacted our MD; John Deanfield, MD; Panos Deloukas, PhD; Frank Dudbridge, PhD; Natalie
findings, through misclassification. However, a sensi- Fitzpatrick, MSc; Bruna Gigante, MD, PhD; Stefan James, MD, PhD; Marja-Liisa
Lokki, PhD; Paulo A. Lotufo, MD, PhD; Nicola Marziliano, PhD; Ify R. Mordi, MD;
tivity analysis stratifying on the follow-up duration of Joseph B. Muhlestein, MD; Chris Newton Cheh, MD; Jan Pitha, PhD; Christoph
individual studies (Patel et al; Chromosome 9p21 and Subsequent CHD Events
sion of Heart & Lungs, University Medical Center Utrecht, 3508GA, Utrecht, the statistics and Epidemiology, Texas Heart Institute, Houston (V.-V.L.). Vorarlberg
Netherlands, Email F.W.Asselbergs@umcutrecht.nl Institute for Vascular Investigation and Treatment (VIVIT), Feldkirch, Austria
(A.L., C.H.S., H.D.). Private University of the Principality of Liechtenstein, Tri-
esen, Liechtenstein (A.L., C.H.S., H.D.). Medical Central Laboratories, Feld-
Affiliations kirch, Austria (A.L.). Department of Genetics, Statistical Genomics Division
Institute of Cardiovascular Science, Faculty of Population Health Science (P.A.L., S.C.) and Department of Medicine, Cardiovascular Division Washington
(R.S.P., A.F.S., L.J.H., K.D., J.D., A.D.H., F.W.A.) and Institute of Health Infor- University School of Medicine, St Louis, MO (S.C.). Division of Molecular and
matics, Faculty of Population Health Science, University College London, Unit- Clinical Medicine, School of Medicine, University of Dundee, Scotland, United
ed Kingdom (N.F., C.H.S., A. Timmis, H.H., F.W.A.). Bart’s Heart Centre, St Kingdom (D. Levin, I.R.M., C.C.L.). Department of Clinical Chemistry, Fimlab
Bartholomew’s Hospital, London, United Kingdom (R.S.P., J.D., A. Timmis). Laboratories, Tampere, Finland (L.-P.L., T.L.). Department of Medicine, Univer-
Division Heart and Lungs, Department of Cardiology (A.F.S., V.T. D.K., F.W.A.), sity of Verona, Italy (N. Martinelli, D.G., O.O.). Department of Cardiology,
Laboratory of Experimental Cardiology (C.M.G., B.D.H.), Department of Clini- Heart Center (K.N.), Department of Clinical Physiology (M. Kähönen), Depart-
cal Chemistry and Hematology (B.G., I.E.H.), Department of Clinical Chemistry, ment of Cardio-Thoracic Surgery, Heart Center, Tampere University Hospital,
UMC Utrecht, Netherlands (G. Pasterkamp). Intermountain Heart Institute, In- Finland (J.O.L). The Christchurch Heart Institute, University of Otago Christ-
termountain Medical Center, Salt Lake City, UT (R.O.M., J.F.C., J.B.M., J.L.A.). church, New Zealand (A.P.B., A.M.R., V.A.C.). Department of Medical Genetics
Clinical Trial Service Unit and Epidemiological Studies Unit, Nuffield Depart- (R.P.) and Department of Cardiology, Medical University of Warsaw, Poland
ment of Population Health (M.V.H.), Medical Research Council Population (G.O.). Department of Epidemiology, Emory University Rollins School of Public
Health Research Unit (M.V.H.), and National Institute for Health Research Ox- Health (Y.V.S.), Department of Biomedical Informatics (Y.V.S.), and Division of
ford Biomedical Research Centre (M.V.H.), University of Oxford, United King- Cardiology, Department of Medicine, Emory Clinical Cardiovascular Research
dom. Uppsala Clinical Research Center (A.A., N.E., S.J., E.H., C.H., B.L., D. Institute, Emory University School of Medicine, Atlanta, GA (A.S.-T., P.B.S.,
Lindholm, A. Siegbahn, L.W.), Department of Medical Sciences, Cardiology A.A.Q.). Clinical Epidemiology and Biostatistics (M.W.T.T.) and AMC Heart
(A.A., E.H., C.H., D. Lindholm), Department of Medical Sciences, Cardiology Center (A.A.M.W., C.R.B.), Clinical and Experimental Cardiology, Amsterdam
(S.J., B.L., L.W.), and Department of Medical Sciences, Clinical Chemistry (A. Cardiovascular Sciences, Amsterdam UMC, Department of Respiratory Medi-
Siegbahn), Uppsala University, Sweden. Institute of Environmental Medicine, cine, Academic Medical Center, University of Amsterdam, the Netherlands
Karolinska Institutet, Stockholm, Sweden (K.L., U.d.F.). Section of Cardiology, (A.H.M.-v.d.Z.). Department of Cellular and Molecular Medicine, Lerner Re-
Michael E. DeBakey Veterans Affairs Medical Center, Section of Cardiovascular search Institute (W.H.W.T., S.L.H.), Department of Cardiovascular Medicine,
Research, and Department of Medicine, Baylor College of Medicine, Houston, Heart and Vascular Institute and Center for Clinical Genomics (W.H.W.T.), and
TX (S.S.V., C.M.B.). Department of Population Medicine and Civilization Dis- Department of Cardiovascular Medicine, Heart and Vascular Institute and Cen-
ease Prevention (K.A.K.), Department of Cardiology (K.A.K., A. Szpakowicz), ter for Microbiome and Human Health, Cleveland Clinic, OH (S.L.H.). Section
and Department of Forensic Medicine, Medical University of Bialystok, Poland of Gerontology and Geriatrics, Department of Internal Medicine (S.T.), and
(W.P., G.T.). Department of Anesthesiology, Perioperative and Pain Medicine, Department of Cardiology (S.T., J.W.J.), Leiden University Medical Center. Lab-
Brigham and Women’s Hospital (M.H.), Harvard Medical School, Boston, MA oratory of Clinical Chemistry and Hematology, Division Laboratories, Pharma-
(J.D.M., M.H. S.C.B.). Montreal Heart Institute (J.-C.T.) and Faculty of Medicine cy, and Biomedical Genetics (S.W.v.d.L.), Department of Vascular Surgery, Uni-
(J.-C.T.), Université de Montréal, QC, Canada (M.-P.D.). Departments of Pre- versity Medical Center Utrecht, University Utrecht, the Netherlands (G.J.d.B.).
ventive Medicine and Biochemistry and Molecular Medicine (H.A., J.H.) and Durrer Centre of Cardiogenetic Research, ICIN-Netherlands Heart Institute,
Institute for Genetic Medicine (J.H.), Keck School of Medicine of USC, Los Netherlands (J.v.S., F.W.B.). Ruddy Canadian Cardiovascular Genetics Centre
Angeles, CA. Department of Clinical Sciences, Lund University, Malmö, Swe- (R.O.V., A.F.R.S.), University of Ottawa Heart Institute (R.M.), Department of
den (P.A., O.M.). Estonian Genome Center, Institute of Genomics (A.M.) and Biochemistry, Microbiology and Immunology (R.O.V., A.F.R.S.), and Depart-
Downloaded from http://ahajournals.org by on June 27, 2019
Department of Biotechnology, Institute of Molecular and Cell Biology, Univer- ments of Medicine and Biochemistry, Microbiology and Immunology, Univer-
sity of Tartu, Estonia (M.A., A.M.). Division of Pharmacoepidemiology and sity of Ottawa, ON, Canada (R.M.). Department of Cardiovascular Medicine,
Clinical Pharmacology (E.V.B., O.H.K., A.H.M.-v.d.Z.), Department of Neurolo- Humanitas Clinical and Research Center, Milan, Italy (C.V.A., G.C). Transplan-
gy and Neurosurgery, Brain Centre Rudolf Magnus and Julius Center for Health tation Laboratory, Medicum (E.V., M.-L.L.), Heart and Lung Center, Helsinki
Sciences and Primary Care (A. Algra), Department of Radiology (P.A.d.J.), and University Hospital University of Helsinki, Finland (J.S.). University of Texas
Julius Center for Health Sciences and Primary Care (Y.v.d.G.), University Medi- School of Public Health, Houston (E.B.). Clinica Mediterranea, Naples, Italy
cal Center Utrecht, the Netherlands. Department of Vascular Medicine, Univer- (C.B.). Cardiology Division, Department of Internal Medicine (J.F.C., J.B.M.,
sity Medical Center Utrecht and Utrecht University, the Netherlands (F.L.J.V.). J.L.A.), Department of Biomedical Informatics, University of Utah, Salt Lake
Centre for Outcomes Research and Evaluation, Research Institute of the McGill City (B.D.H.). Cardiovascular Sciences (K.F.C.) and Emeritus Professor of Cardi-
University Health Centre (H.B., L.D., L.P., J.M.B.). Research Institute of the Mc- ology (K.A.A.F.), University of Edinburgh. ATS Sardegna, ASL 3, Nuoro (G.
Gill University Health Centre (J.C.E.). Division of Cardiology, Department of Casu, N. Marziliano). William Harvey Research Institute, Barts and the London
Medicine, Royal Victoria Hospital (J.C.E., G.T.), Department of Medicine (L.P., Medical School (P.D.) and Centre for Genomic Health (P.D.), Queen Mary Uni-
J.M.B.), and Preventive and Genomic Cardiology, McGill University Health Cen- versity of London. Centro de Pesquisa Clinica, Hospital Universitario, Universi-
tre, Montreal, QC, Canada (L.D., J.C.E., G.T.). Laboratory for Translational Ge- dade de Sao Paulo, Brazil (P.A.L.). Cardiovascular Research Center and Center
netics, Department of Human Genetics (B.B., D. Lambrechts) and Departement for Human Genetic Research, Massachusetts General Hospital, Boston and
of Cardiovascular Sciences, KU Leuven, Belgium (F.V.d.W.). Laboratory for Program in Medical and Population Genetics, Broad Institute, Cambridge, MA
Translational Genetics, VIB Center for Cancer Biology, VIB, Belgium (B.B., D. (C.N.C.). Department of Medicine and Cardiology, Academic Teaching Hospi-
Lambrechts). Department of Cardiovascular Sciences (P.S.B., C.P.N., N.J.S.) and tal Feldkirch, Austria. Heart Center Leipzig (A. Teren), LIFE Research Center for
Department of Health Sciences, University of Leicester, United Kingdom. BHF Civilization Diseases (A. Teren, R.B., M. Scholz, J.T.), and Institute for Medical
Cardiovascular Research Centre (F.D.) and National Institute of Health Research Informatics, Statistics and Epidemiology, University of Leipzig, Germany (M.
(NIHR) Leicester Biomedical Research Centre (P.S.B., C.P.N.), Glenfield Hospital, Scholz). Respiratory Oncology Unit, Department of Respiratory Medicine, Uni-
Leicester, United Kingdom. Division of Clinical Epidemiology and Aging Re- versity Hospitals KU Leuven, Belgium (E.W.). Princess Al-Jawhara Al-Brahim
search, German Cancer Research Center (DKFZ), Heidelberg (L.P.B., U.M., Centre of Excellence in Research of Hereditary Disorders, Jeddah, Saudi Arabia
H.B.). Vth Department of Medicine, Medical Faculty Mannheim, Heidelberg (A.A.M.W.). Robertson Center for Biostatistics (I.F.) and Institute of Cardiovas-
University, Mannheim, Germany (G.D., M. Kleber, W.M.). Heart Institute, Uni- cular and Medical Sciences, University of Glasgow, United Kingdom (D.J.S.,
versity of Sao Paulo, Brazil (N.E.D., A.C.P.). Institute for Biomedicine, Eurac N.S.). CNR Institute of Clinical Physiology, Pisa, Italy (M.G.A., C.C.). Cardiology
Research, Affiliated Institute of the University of Lübeck, Bolzano, Italy (L.F.). Department, Parma University Hospital, Italy (D.A.). Centre de recherche de
Department of Pharmacotherapy and Translational Research and Center for l’Institut Universitaire de cardiologie et de pneumologie de Québec (B.J.A.) and
Pharmacogenomics (Y.G., R.M.C.-D., J.A.J.), Division of Cardiovascular Medi- Department of Medicine, Faculty of Medicine, Université Laval, Canada
cine, College of Medicine, University of Florida (J.A.J., C.J.P.). Centre for Ex- (B.J.A.). St. Antonius Hospital, Department of Cardiology, Nieuwegein, the
perimental Medicine, Institut for Clinical and Experimental Medicine, Prague, Netherlands (T.O.B., B.K.M., J.M.t.B.). Department of Anesthesia, Pain and
Czech Republic (J.A.H., J.P.). Department of Cardio-Thoracic Surgery (P.K.), Critical Care, Beth Israel Deaconess Medical Center, Boston, MA (S.C.B.). Ser-
Department of Clinical Chemistry (L.-P.L., T.L.), Department of Cardiology vice de cardiologie, Département multidisciplinaire de cardiologie, Instituteitut
(K.N.), Department of Clinical Physiology (M. Kähönen), and Department of universitaire de cardiologie et de pneumologie de Québec, Canada (P.B.). Unité
Cardio-Thoracic Surgery, Finnish Cardiovascular Research Center, Faculty of d’évaluation cardiovasculaire, Institut national d’excellence en santé et en ser-
Medicine and Life Sciences, University of Tampere (J.O.L.). Department of Bio- vices sociaux (INESSS), Montreal Canada (P.B.). Instituteitut universitaire de
Circ Genom Precis Med. 2019;12:e002471. DOI: 10.1161/CIRCGEN.119.002471 April 2019 170Patel et al; Chromosome 9p21 and Subsequent CHD Events
cardiologie et de pneumologie de Québec, Laval University, Québec City, Can- National Institutes of Health/ National Institutes of Aging grant AG051633; Dr
ada (P.B.). Institute of Clinical Chemistry and Laboratory Medicine, University Sandesara is supported by the Abraham J. & Phyllis Katz Foundation (Atlanta,
Hospital Regensburg, Germany (R.B.). Department of Biomedical Sciences, GA); The Emory Cardiovascular Biobank is supported by NIH grants
Humanitas University, Milan, Italy (G. Condorelli). Heart Health Research 5P01HL101398-02, 1P20HL113451-01, 1R56HL126558-01, 1RF-
Group, University of Auckland, New Zealand (R.N.D.). Drexel University Col- 1AG051633-01, R01 NS064162-01, R01 HL89650-01, HL095479-01,
lege of Medicine, Philadelphia, PA (H.D.). Department of Vascular Medicine, 1U10HL110302-01, 1DP3DK094346-01, 2P01HL086773-06A1; this Estonian
Academic Medical Center, Amsterdam, the Netherlands (G.K.H.). Einthoven Biobank was funded by EU H2020 grant 692145, Estonian Research Council
Laboratory for Experimental Vascular Medicine, LUMC, Leiden (J.W.J.). Inter- Grant IUT20-60, IUT24-6, PUT1660, PUT735 and European Union through the
university Cardiology Institute of the Netherlands, Utrecht, the Netherlands European Regional Development Fund Project No.2014-2020.4.01.15-0012
(J.W.J.). Department of Internal Medicine, Jagiellonian University Medical Col- GENTRANSMED, NIH-GIANT, ERA-CVD grant Detectin-Heart failure and
lege, Kraków, Poland (M.P.K., M. Sanak, W.S.). Cardiology Centre, Institute for 2R01DK075787-06A1; GENESIS-PRAXY (Gender and Sex Determinants of
Clinical and Experimental Medicine, Prague, Czech Republic (J.K.). Department Cardiovascular Disease: From Bench to Beyond-Premature Acute Coronary
of Cardiology and Internal Diseases, Military Institute of Medicine, Warsaw, Syndrome) is funded by the Canadian Institutes of Health Research and Heart
Poland (M. Kiliszek). Department of Internal Medicine, Skåne University Hospi- and Stroke Foundations of Alberta, NWT & Nunavut, British Columbia and
tal, Malmö, Sweden (O.M.). Pat Macpherson Centre for Pharmacogenetics and Yukon, Nova Scotia, Ontario, and Quebec (HSFC); The GENDEMIP study (Ge-
Pharmacogenomics, Division of Molecular and Clinical Medicine, Ninewells netic Determination of Myocardial Infarction in Prague) was supported by Proj-
Hospital and Medical School, Dundee (C.N.P.). Cardiovascular Research Insti- ect (MH, Czech Republic) No. 00023001 (Institute of Clinical and Experimental
tute, National University of Singapore (A.M.R.). Department of Cardiology, Medicine, Prague); GoDARTS (Genetics of Diabetes Audit and Research in Tay-
Clinical Sciences, Lund University and Skåne University Hospital (J.G.S.) and side Scotland) was funded by the Wellcome Trust (072960/Z/03/Z,
Wallenberg Center for Molecular Medicine (J.G.S.), Lund University Diabetes 084726/Z/08/Z, 084727/Z/08/Z, 085475/Z/08/Z, 085475/B/08/Z) and as part of
Center (J.G.S.), Lund University, Lund, Sweden. Saint Luke’s Mid America Heart the EU IMI-SUMMIT programme. C.N.P. has received grant funding from the
Institute and the University of Missouri-Kansas City and Saint Luke’s Health Wellcome Trust to develop the GoDARTS cohort; Dr Mordi is supported by an
System, Kansas City, MO (J.A.S.). Institute of Laboratory Medicine, Clinical NHS Education of Scotland/Chief Scientist Office Postdoctoral Clinical Lecture-
Chemistry and Molecular Diagnostics, University Hospital, Leipzig (J.T.). De- ship (PCL 17/07); the GENECOR study (Genetic Mapping for Assessment of
partment of Cardiovascular Medicine, University of Münster, Germany (J.W.). Cardiovascular Risk) was supported in part by the Italian Ministry of Research’s
CARDIoGRAMPlusC4D. University of Groningen, University Medical Center, Fund for Basic Research (FIRB 2005); GRACE (Global Registry of Acute Coro-
Groningen, Netherlands (P.V.d.H.). Department of Pathology and Molecular nary Events–Belgium) UK was supported in part by an Educational Grant from
Medicine, McMaster University (G. Pare). Population Health Research Institute, Sanofi Aventis; Award from Chief Scientist Office, Scotland; INVEST-GENES
Hamilton, ON, Canada (G. Pare). Synlab Academy, Synlab Holding Deutschland (International Verapamil SR Trandolopril Study Genetic Substudy) was sup-
GmbH, Mannheim, Germany (W.M.). Clinical Institute of Medical and Chemi- ported by the National Institute of Health Pharmacogenomics Research Net-
cal Laboratory Diagnostics, Medical University of Graz, Austria (W.M.). work grant U01-GM074492, NIH R01 HL074730, University of Florida Oppor-
tunity Fund, BASF Pharma and Abbott Laboratories; Italian Atherosclerosis,
Thrombosis and Vascular Biology Group was supported by Epidemiologia e
Acknowledgments Genetica della Morte Improvvisa in Sardegna; The KAROLA study has received
The GENIUS-CHD (Genetics of Subsequent Coronary Heart Disease) collabora- financial support by the German Ministry of Education and Research
tors would like to express their immense gratitude to all patients who par- (01GD9820/0 and 01ER0814), by the Willy-Robert-Pitzer Foundation, and by
ticipated in each of the individual studies as well as the many personnel who the Waldburg-Zeil Clinics Isny; The KRAKOW GENIUS Study was supported by
helped with recruitment, collection, curation, management and processing of a grant from the Polish Ministry of Science and Higher Education, no.
Downloaded from http://ahajournals.org by on June 27, 2019
the samples and data. We also thank the CARDIoGRAMPlusC4D steering com- NN402083939 and the National Science Centre, no. 2013/09/B/NZ5/00770;
mittee for providing the summary data after excluding the cohorts already in LIFE-Heart was funded by the Leipzig Research Center for Civilization Diseases
GENIUS-CHD. (LIFE). LIFE is an organizational unit affiliated to the Medical Faculty of the
University of Leipzig. LIFE is funded by means of the European Union, by the
European Regional Development Fund (ERDF) and by funds of the Free State of
Sources of Funding Saxony within the framework of the excellence initiative; The LURIC study (The
The funder(s) of the study had no role in study design, data collection, data Ludwigshafen Risk and Cardiovascular Health Study) was supported by the
analysis, data interpretation, or writing of the report. Within GENIUS-CHD (Ge- Seventh Framework Program (AtheroRemo, grant agreement number 201668
netics of Subsequent Coronary Heart Disease), all participating investigators and RiskyCAD (Personalized Diagnostics and Treatment of High Risk Coronary
and sponsors who contributed data and analyses are acknowledged irrespec- Artery Disease Patients), grant agreement number 305739) of the European
tive of academic or industry affiliations. Specific funding statements: Dr Patel is Union; The NEAPOLIS CAMPANIA (Neapolis Campania Italia) study was supp-
funded by a British Heart Foundation Intermediate Fellowship (FS/14/76/30933). ported by European Research Council Advanced Grant (CardioEpigen, no.
This research was also supported by the National Institute for Health Research 294609);Italian Ministry of Health (PE-2013-02356818);Italian Ministry of Edu-
University College London Hospitals Biomedical Research Centre; Dr Schmidt is cation, University and Research (2015583WMX); The North East Poland Myo-
funded by BHF grant PG/18/5033837; Dr Holmes works in a unit that receives cardial Infarction Study was supported by grant N N 402 529139 from the
funding from the UK Medical Research Council and is supported by a British National Science Center (Poland); Dr Vilmundarson is supported by a graduate
Heart Foundation Intermediate Clinical Research Fellowship (FS/18/23/33512) fellowship of the University of Ottawa Heart Institute; OHGS (Ottawa Heart
and the National Institute for Health Research Oxford Biomedical Research Genomics Study) was funded in part by a Heart and Stroke Foundation grant;
Centre; The AGNES study (Arrhythmia Genetics in the Netherlands) was sup- Dr Stott was supported in part by an investigator initiated grant from Bristol
ported by research grants from the Netherlands Heart Foundation (2001D019, Myers Squibb USA; The PROSPER study (Prospective Study of Pravastatin in the
2003T302, 2007B202 and the PREDICT project (CVON 2012-10)), the Leducq Elderly at Risk) was supported by an investigator initiated grant obtained from
Foundation (grant 05-CVD) and the Center for Translational Molecular Medi- Bristol-Myers Squibb. Dr Jukema is an Established Clinical Investigator of the
cine (CTMM COHFAR); The Cleveland Clinic Genebank Study was supported in Netherlands Heart Foundation (grant 2001 D 032). Support for genotyping
part by NIH (National Institutes of Health) grants R0133169, R01ES021801, was provided by the seventh framework program of the European commission
R01MD010358, and R01ES025786, R01HL103866, R01DK106000, (grant 223004) and by the Netherlands Genomics Initiative (Netherlands Con-
R01HL126827, P20HL113452, P01HL098055, P01HL076491, and sortium for Healthy Aging grant 050-060-810); The RISCA (Recurrance and
R01HL103931; The 4C study (Clinical Cohorts in Coronary disease Collabora- Inflammation in the Acute Coronary Syndromes Study) was supported in part
tion) was supported in part by NIHR and Barts Charity; The Corogene study by FRSQ, HSFC, Merck Frost Canada, Pfizer Canada; The SHEEP study (Stock-
was supported by grants from Aarno Koskelo Foundation, Helsinki University holm Heart Epidemiology Program) was supported by grants from the Swedish
Central Hospital special government funds (EVO no. TYH7215, no. Council for Work Life and Social Research, and the Stockholm County Council;
TKK2012005, no. TYH2012209, no. TYH2014312), and Finnish Foundation The TNT trial (Treating to New Targets) was sponsored by Pfizer who granted
for Cardiovascular research; CABGenomics was supported by Stanton Sher- access to data, Genotyping of the samples was funded in part by grants from
nan, C. David Collard, Amanda A. Fox/R01 HL 098601 National Heart Long Genome Canada and Genome Quebec and the Canadian Institutes of Health
and Blood Institute; The CDCS (Coronary Disease Cohort Study) and PMI (Post Research (CIHR); Dr Arsenault holds a junior scholar award from the Fonds de
Myocardial Infarction Study) were funded by the Health Research Council and recherche du Quebec- Sante (FRQS); Dr Cresci is supported, in part, by the
Heart Foundation of New Zealand; Dr Samman-Tahnan is supported by the National Institutes of Health (Cresci R01 NR013396). The TRIUMPH study
Circ Genom Precis Med. 2019;12:e002471. DOI: 10.1161/CIRCGEN.119.002471 April 2019 171Patel et al; Chromosome 9p21 and Subsequent CHD Events
(Translational Research Investigating Underlying Disparities in Acute Myocar- 2. Helgadottir A, et al. A common variant on chromosome 9p21 affects
dial Infarction Patient’s Health Status) was sponsored by the National Institutes the risk of myocardial infarction. Science. 2007;316:1491–1493. doi:
of Health: Washington University School of Medicine SCCOR Grant P50 10.1126/science.1142842
HL077113; The Utrecht Cardiovascular Pharmacogenetics Study studies were 3. McPherson R, et al. A common allele on chromosome 9 associated
funded by the Netherlands Heart Foundation and the Dutch Top Institute Phar- with coronary heart disease. Science. 2007;316:1488–1491. doi:
ma Mondriaan Project; The Verona Heart Study was supported by the Carive- 10.1126/science.1142447
rona Foundation; Veneto Region; Italian Ministry of Education, University, and 4. Samani NJ, et al; WTCCC and the Cardiogenics Consortium. Genome-
Research (MIUR); LURM (Laboratorio Universitario di Ricerca Medica) Research wide association analysis of coronary artery disease. N Engl J Med.
Center, University of Verona; The Warsaw ACS Registry (acute coronary syn- 2007;357:443–453. doi: 10.1056/NEJMoa072366
drome) is supported by grant N R13 0001 06 from The National Centre for 5. Palomaki GE, et al. Association between 9p21 genomic markers
Research and Development (NCBiR), Statutory Grant from Medical University and heart disease: a meta-analysis. JAMA. 2010;303:648–656. doi:
10.1001/jama.2010.118
of Warsaw; Dr Nelson is funded by the British Heart Foundation; Prof. Samani
6. Patel RS, et al. Genetic variants at chromosome 9p21 and risk of first
is funded by the British Heart Foundation and is a NIHR Senior Investigator.
versus subsequent coronary heart disease events: a systematic re-
Prof Hingorani is a NIHR Senior Investigator; Prof Asselbergs is supported by
view and meta-analysis. J Am Coll Cardiol. 2014;63:2234–2245. doi:
University College London Hospitals NIHR Biomedical Research Centre, EU/EF-
10.1016/j.jacc.2014.01.065
PIA Innovative Medicines Initiative 2 Joint Undertaking BigData@Heart grant
7. Dehghan A, et al. Genome-wide association study for incident myo-
n° 116074, the European Union’s Horizon 2020 research and innovation pro-
cardial infarction and coronary heart disease in prospective cohort
gramme under the ERA-NET Co-fund action N°01KL1802 (Druggable-MI-
studies: the CHARGE consortium. PLoS One. 2016;11:e0144997. doi:
gene) jointly funded by the Dutch Heart Foundation and Netherlands Organi- 10.1371/journal.pone.0144997
zation for Health Research and Development (ZonMw). 8. Patel RS, et al. Subsequent event risk in individuals with established coro-
nary heart disease: design and rationale of the GENIUS-CHD consortium.
Disclosures Circ Genom Precis Med. 2019;12:e002470.
9. Genomes Project C, et al. A global reference for human genetic variation.
Dr Patel has received speaker fees and honoraria from Amgen, Sanofi and Bayer Nature. 2015;526:68–74.
and research grant funding from Regeneron; Dr Holmes has collaborated with 10. Ellis KL, et al. A common variant at chromosome 9P21.3 is associated with
Boehringer Ingelheim in research, and in accordance with the policy of The Clini- age of onset of coronary disease but not subsequent mortality. Circ Cardio-
cal Trial Service Unit and Epidemiological Studies Unit (University of Oxford), did vasc Genet. 2010;3:286–293. doi: 10.1161/CIRCGENETICS.109.917443
not accept any personal payment; Dr Akerblom has received institutional re- 11. Gong Y, et al. Chromosome 9p21 haplotypes and prognosis in white
search grant and speakers fee from AstraZeneca, institutional research grant and black patients with coronary artery disease. Circ Cardiovasc Genet.
from Roche Diagnostics; Dr James has received grants from AstraZeneca, The 2011;4:169–178. doi: 10.1161/CIRCGENETICS.110.959296
Medicines Company, Swedish heart and lung foundation, Swedish research 12. Horne BD, et al. Association of variation in the chromosome 9p21 locus
council, Janssen; personal fees from Bayer; Dr Hagstrom declares being an with myocardial infarction versus chronic coronary artery disease. Circ Car-
expert committee member, lecture fees, and institutional research grant from diovasc Genet. 2008;1:85–92. doi: 10.1161/CIRCGENETICS.108.793158
Sanofi, and Amgen; institutional research grants from AstraZeneca, and Glaxo- 13. Virani SS, et al. Chromosome 9p21 single nucleotide polymorphisms are
SmithKline; expert committee member and lecture fees NovoNordisk and Beh- not associated with recurrent myocardial infarction in patients with estab-
ringer; Dr Held declares institutional research grant, advisory board member and lished coronary artery disease. Circ J. 2012;76:950–956.
speaker’s bureau from AstraZeneca; institutional research grants from Bristol- 14. Wauters E, et al. Influence of 23 coronary artery disease variants on recur-
Downloaded from http://ahajournals.org by on June 27, 2019
Myers Squibb Merck & Co, GlaxoSmithKline, Roche Diagnostics. Advisory board rent myocardial infarction or cardiac death: the GRACE Genetics Study.
for Bayer and Boehringer Ingelheim; Dr Lindholm has received institutional re- Eur Heart J. 2013;34:993–1001. doi: 10.1093/eurheartj/ehs389
search grants from AstraZeneca, and GlaxoSmithKline; Speaker fees from Astra- 15. Dahabreh IJ, et al. Index event bias as an explanation for the para-
Zeneca, Speaker fees from AstraZeneca; Dr Siegbahn has received institutional doxes of recurrence risk research. JAMA. 2011;305:822–823. doi:
research grants from AstraZeneca, Boehringer Ingelheim, Bristol-Myers Squibb/ 10.1001/jama.2011.163
16. Cole SR, et al. Illustrating bias due to conditioning on a collider. Int J Epi-
Pfizer, Roche Diagnostics, GlaxoSmithKline; Dr ten Berg reports receiving fees for
demiol. 2010;39:417–420. doi: 10.1093/ije/dyp334
board membership from AstraZeneca, consulting fees from AstraZeneca, Eli Lilly,
17. Anderson CD, et al. The effect of survival bias on case-control genetic
and Merck, and lecture fees from Daiichi Sankyo and Eli Lilly, AstraZeneca, Sanofi
association studies of highly lethal diseases. Circ Cardiovasc Genet.
and Accumetrics; Dr Wallentin reports institutional research grants, consultancy
2011;4:188–196. doi: 10.1161/CIRCGENETICS.110.957928
fees, lecture fees, and travel support from Bristol-Myers Squibb/Pfizer, AstraZen-
18. Hu YJ, et al. Impact of selection bias on estimation of subsequent event
eca, GlaxoSmithKline, Boehringer Ingelheim; institutional research grants from
risk. Circ Cardiovasc Genet. 2017;10.
Merck & Co, Roche Diagnostics; consultancy fees from Abbott; and holds a pat- 19. Falk E, et al. Update on acute coronary syndromes: the pathologists’ view.
ent EP2047275B1 licensed to Roche Diagnostics, and a patent US8951742B2 Eur Heart J. 2013;34:719–728. doi: 10.1093/eurheartj/ehs411
licensed to Roche Diagnostics; Dr Claes reports lecture fees, and an institutional 20. Reilly MP, et al.; Myocardial Infarction Genetics Consortium; Well-
research grant from Sanofi, and Amgen; institutional research grants from Astra- come Trust Case Control Consortium. Identification of ADAMTS7 as a
Zeneca, and GlaxoSmithKline; and lecture fees from NovoNordisk and AstraZen- novel locus for coronary atherosclerosis and association of ABO with
eca. Dr Asselbergs has received research funding from Regeneron, Pfizer, Sanofi. myocardial infarction in the presence of coronary atherosclerosis: two
The other authors report no conflicts. genome-wide association studies. Lancet. 2011;377:383–392. doi:
10.1016/S0140-6736(10)61996-4
21. Chan K, et al. Association between the chromosome 9p21 locus and an-
giographic coronary artery disease burden: a collaborative meta-analysis.
REFERENCES
J Am Coll Cardiol. 2013;61:957–970. doi: 10.1016/j.jacc.2012.10.051
1. Nikpay M, et al. A comprehensive 1,000 genomes-based genome- 22. Visel A, et al. Targeted deletion of the 9p21 non-coding coronary ar-
wide association meta-analysis of coronary artery disease. Nat Genet. tery disease risk interval in mice. Nature. 2010;464:409–412. doi:
2015;47:1121–1130. doi: 10.1038/ng.3396 10.1038/nature08801
Circ Genom Precis Med. 2019;12:e002471. DOI: 10.1161/CIRCGEN.119.002471 April 2019 172You can also read