Assessing the Potential of National Strategies for Electronic Health Records for Population Health Monitoring and Research - CDC
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Assessing the Potential of
January 2006
National Strategies for
Electronic Health Records for
Population Health
Monitoring and Research
Series 2, Number 143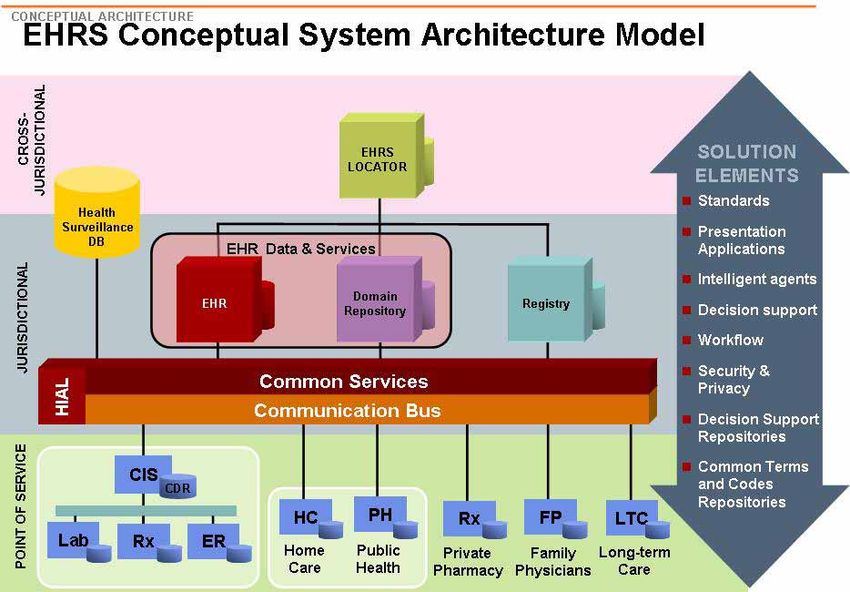
Copyright information All material appearing in this report is in the public domain and may be reproduced or copied without permission; citation as to source, however, is appreciated. Disclaimer The findings and conclusions in this report are those of the author and do not necessarily represent the views of the Centers for Disease Control and Prevention. Suggested citation Friedman DJ. Assessing the potential of national strategies for electronic health records for population health monitoring and research. National Center for Health Statistics. Vital Health Stat 2(143). 2006. Library of Congress Cataloging-in-Publication Data Assessing the potential of national strategies for electronic health records for population health monitoring and research. p. ; cm.— (DHHS publication ; no. (PHS) 2006–1343) (Vital and health statistics. Series 2 ; no. 143) ‘‘January 2006.’’ Author: Daniel J. Friedman. Includes bibliographical references. ISBN 0–8406-0607–9 1. Medical informatics. 2. Medical records—Data processing. I. Friedman, Daniel J. II. National Center for Health Statistics (U.S.) III. Series. IV. Series: Vital and health statistics. Series 2, Data evaluation and methods research ; no. 143. [DNLM: 1. Public Health Informatics—organization & administration. 2. Forms and Records Control—organization & administration. 3. Medical Records Systems, Computerized. 4. National Health Programs—trends. 5. Research Design—trends. W2 A N148vb no.143 2006] R858.A87 2006 651.5’04261—dc22 2006014105 For sale by the U.S. Government Printing Office Superintendent of Documents Mail Stop: SSOP Washington, DC 20402-9328 Printed on acid-free paper.
Series 2, Number 143 Assessing the Potential of National Strategies for Electronic Health Records for Population Health Monitoring and Research Data Evaluation and Methods Research U.S. DEPARTMENT OF HEALTH AND HUMAN SERVICES Centers for Disease Control and Prevention National Center for Health Statistics Hyattsville, Maryland January 2006 DHHS Publication No. (PHS) 2007-1343

National Center for Health Statistics Edward J. Sondik, Ph.D., Director Jennifer H. Madans, Ph.D., Acting Co-Deputy Director Michael H. Sadagursky, Acting Co-Deputy Director Jennifer H. Madans, Ph.D., Associate Director for Science Jennifer H. Madans, Ph.D., Acting Associate Director for Planning, Budget, and Legislation Michael H. Sadagursky, Associate Director for Management and Operations Lawrence H. Cox, Ph.D., Associate Director for Research and Methodology Margot A. Palmer, Director for Information Technology Margot A. Palmer, Acting Director for Information Services Linda T. Bilheimer, Ph.D., Associate Director for Analysis and Epidemiology Charles J. Rothwell, M.S., Director for Vital Statistics Jane E. Sisk, Ph.D., Director for Health Care Statistics Jane F. Gentleman, Ph.D., Director for Health Interview Statistics Clifford L. Johnson, Director for Health and Nutrition Examination Surveys
Acknowledgments
T
his project was supported by the
Centers for Disease Control and
Prevention (CDC) Contract
No. 200-2004-M-09141 and Contract
No. 200-2005-M-13604. The contents of
this publication are solely the
responsibility of the author and do not
necessarily represent the official views
of CDC. The author would like to thank
Dr. Edward J. Sondik, Director of the
National Center for Health Statistics,
CDC, and Edward L. Hunter, Associate
Director of the National Center for
Health Statistics, CDC, for their
encouragement, support, and guidance
throughout this project. Additionally, the
author would also like to thank Dr. R.
Gibson Parrish, Dr. Steven J. Steindel
(CDC) and Dr. David A. Ross (Public
Health Informatics Institute) for their
patience and contribution of time and
advice. The project would not have been
possible without the generosity and
honesty of the ninety-six experts in
Australia, Canada, England, New
Zealand, and the U.S., who provided
lengthy and detailed interviews and who
consistently agreed to answer follow-up
questions. Twelve experts also provided
thorough and extremely helpful reviews
of earlier drafts of this report, and their
remarkable generosity in donating their
time and expertise is also very much
appreciated. Throughout the course of
this project, experts in the five countries
who had previously been strangers to
the author became colleagues, and
colleagues became friends. Of course,
the responsibility for any errors,
misunderstandings, misrepresentations,
and hare-brained ideas lies with the
author alone.
iii
Content
Acknowledgments . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . iii
Summary . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . vii
Highlights. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . xii
Abstract . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1
Chapter 1. Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1
Purpose . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1
Central Concepts . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2
Chapter 2. Methods . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5
Environmental Scan of Related Developments . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5
Expert Interviews. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5
Chapter 3. Factors Impacting on National Strategies for Electronic Health Records . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 7
Population Health Status . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 7
Health Expenditures . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 7
Health Systems . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 7
Public Opinion. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 7
Chapter 4. Nation Snapshots: Australia, Canada, England, and New Zealand . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 14
England . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 14
Australia. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 22
Canada . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 27
New Zealand . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 33
Chapter 5. Common Themes in Interviews with Expert Informants in Australia, Canada, England, and New Zealand . . . . . . . . 41
Potential Contribution . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 41
Constraints . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 43
Chapter 6. Common Themes in Interviews with Expert Informants in the U.S. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 49
Potential Contribution . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 49
Scenarios . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 51
Constraints . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 52
Chapter 7. Fundamental Issues in the Relationship of National Strategies for Electronic Health Records to Population
Health Monitoring and Research . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 54
Definitional Issues . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 54
Numerator and Denominator Issues . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 54
Overarching Issues . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 57
Success Factors . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 58
References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 61
Acronyms and Glossary . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 71
Tables
2.1 Requested and completed key informant interviews, by country . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6
2.2 Types of key informants, by country . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6
3.1 Population health status, by country . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 9
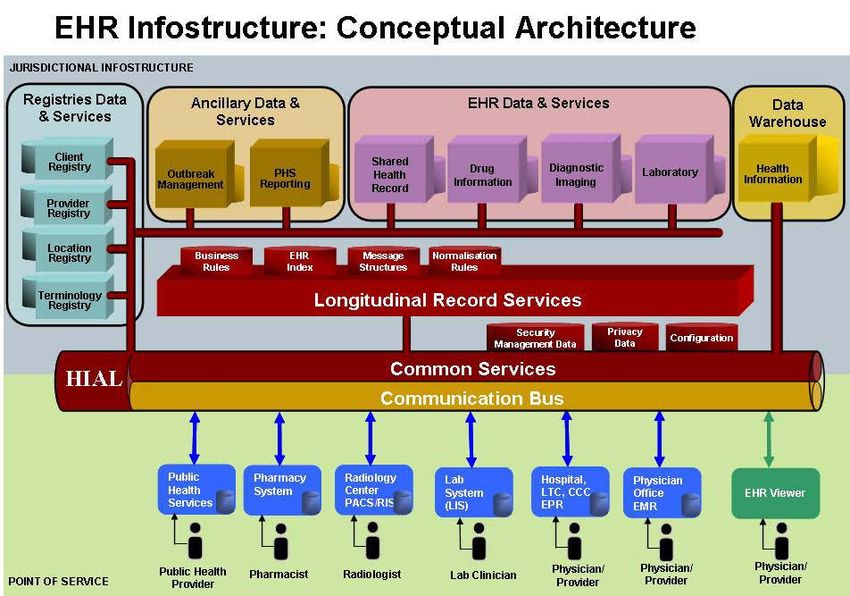
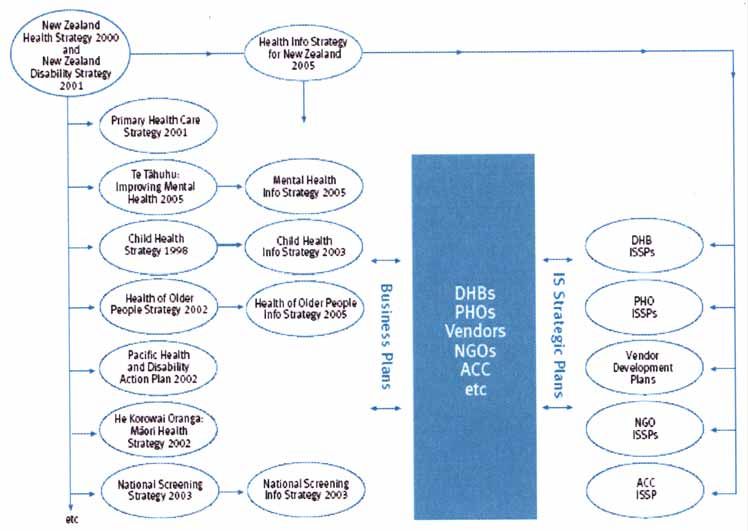
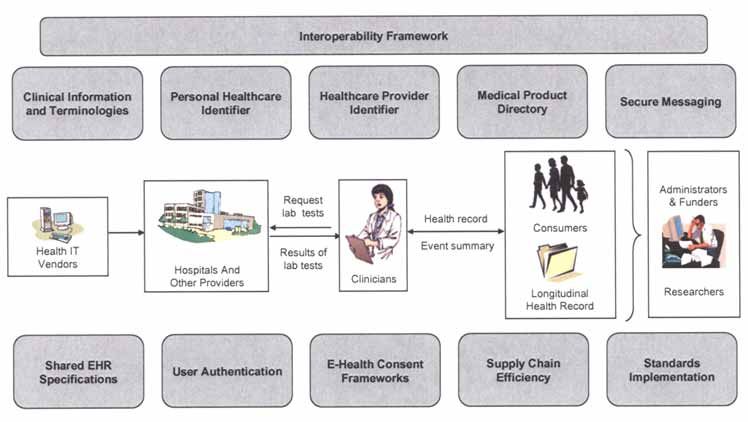
v3.2 Health expenditures, by country . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 9 3.3 Health system context, by country . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 10 3.4 Health system structure, by country . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 11 3.5 Health system process and performance, by country . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 12 3.6 Public opinion about health systems, by country: 2004 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 13 4.1 National strategies for electronic health records, by country: 2005 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 39 Figures 1.1 Influences on the population’s health . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3 4.1 England’s National Health Service integrated model for information . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 20 4.2 Data flows for England’s Secondary Uses Service . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 22 4.3 Key elements of Australia’s HealthConnect . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 24 4.4 Initiatives of Australia’s National E-Health Transition Authority . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 28 4.5 Key elements of Canada’s Electronic Health Record Solution Conceptual System Architecture model . . . . . . . . . . . . . . 30 4.6 Canada’s full featured Electronic Health Record Jurisdictional Infostructure . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 31 4.7 New Zealand’s linkage between health strategies and information strategies . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 34 4.8 New Zealand’s distributed Electronic Health Records model . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 36 Apppendices Appendix 1. Structured Search Criteria . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 72 General Considerations for Structured Searches . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 72 Preliminary Search Algorithms . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 72 Documentation. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 72 Appendix 2. Journals and Newsletters Reviewed . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 73 Appendix 3. Typical Interview Guide (English Expert) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 74 Introduction and Background . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 74 Questions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 74 Appendix 4. Key Informants. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 76 4-A. Key Informants Australia. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 76 4-B. Key Informants Canada . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 77 4-C. Key Informants England . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 78 4-D. Key Informants New Zealand . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 79 4-E. Key Informants United States . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 80 4-F. Consultations . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 82 4-G. Reviewers . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 83 vi
Summary
Assessing the Potential of National Strategies for Electronic Health Records for
Population Health Monitoring and Research
January 2006
Rationale (see Chapter 1) Methods (see Chapter 2) strategies for electronic health records
for health event and disease detection
Healthcare costs continue to increase. This study: for the purposes of immediate public
The media, the public, and health health interventions, such as case-based
1. Reviewed national strategies for
professionals now recognize that surveillance, syndromic surveillance,
electronic health records in Australia,
unnecessary morbidity, mortality, and and bioterrorism surveillance.
Canada, England, and New Zealand,
healthcare costs resulting from adverse
and especially the implications of
events and medical errors are serious
those strategies for population health Key concepts (see Chapter 1)
problems. The U.S. and other developed
monitoring by producing health
nations are adopting health information This report defines the electronic
statistics and by encouraging
technology as a tool for rationalizing health record as an electronic repository
research employing health statistics.
complicated healthcare systems, improving of patient-centric data that are
The review relied on reports,
the quality of patient care, moderating identifiable, longitudinal and preferably
presentations, Web pages, and
healthcare costs, and reducing the life-long, cross-provider, cross-provider
articles, which were publicly
incidence of adverse events. Electronic site, and cross the spectrum of
available before January 2006.
health records constitute the core of health healthcare, including primary care, acute
Structured and directed Web and
information technology. The U.S., hospital care, long-term care, and home
literature searches were conducted.
Australia, Canada, England, and New care. In contrast, this report defines the
See Chapters 2, 3, and 4.
Zealand are all developing national electronic patient record as the
2. Identified the potential contribution
strategies for electronic health records, electronic record of the periodic care
of national strategies for electronic
accompanied by substantial investments of provided mainly by one institution.
health records to population health
public and private sector funds in Widely accepted definitions of electronic
monitoring and research and barriers
implementing those strategies. health records and electronic patient
to achieving that potential. The
records do not exist internationally, and
identification of the potential
Purpose (see Chapter 1) contribution and barriers relied on
comparisons of different usages of the
terms should focus on specified
The Centers for Disease Control interviews with 96 experts with
functions rather than assuming
and Prevention’s National Center for national and sub-national
comparability based on the terms
Health Statistics commissioned this responsibilities for strategies for
themselves.
report to assess the potential electronic health records, for
Population health encompasses the
contribution of national strategies for population health monitoring and
level and distribution of disease,
electronic health records to population research, and for related research in
functional status, and well-being within
health monitoring and research. The U.S., Australia, Canada, England, and
a group. Population health monitoring is
report focuses on those types of New Zealand. The interviews were
the collection and analysis of data to
population health monitoring that qualitative and were conducted via
detect and describe changes in the
generate health statistics for measuring telephone using structured interview
population’s health or factors that affect
the population’s health, rather than those guides. See Chapters 2, 5, and 6.
the population’s health.
types of population health monitoring 3. Delineated fundamental issues that
Health statistics are ‘‘numerical
used to detect health events and diseases must be confronted to maximize the
data that characterize the health of a
for the purposes of immediate public contribution of national strategies in
population and the influences that affect
health interventions. the development of electronic health
its health.’’1 The types of population
records for population health
monitoring and research. See 1
Parrish RG, Friedman DJ, Hunter EL (2005).
Disclaimer: The findings and conclusions in this Chapter 7. Defining health statistics and their scope. In:
report are those of the author and do not necessarily Friedman DJ, Hunter EL, Parrish RG (editors),
represent the views of the Centers for Disease This study did not explore issues Health Statistics: Shaping Policy and Practice to
Control and Prevention. relating to the potential of national Improve the Population’s Health. New York City
(NY): Oxford University Press;3.
viihealth monitoring that typically generate judgments, which may change over electronic health records contain
health statistics are reportable diseases time. National strategies in Australia, structured data. In Australia and Canada,
and registries, administrative health data, Canada, England, and New Zealand are consensus has not yet been achieved on
and population-based surveys; nonhealth developing and evolving, and passing unique patient identification, or whether
data sources also provide health through stages of conceptualization, unique identification will apply to
statistics, especially relating to the design, pilot testing, and residents who encounter the healthcare
influences on the population’s health. implementation. Only England has system or to all residents.
A numerator is ‘‘the upper portion moved to implementation of a national
of a fraction, used to calculate a rate or strategy for electronic health records. Potential contributions of
a ratio.’’2 Numerators represent the Australia has conducted local pilot electronic health records to
aspect of the population’s health being testing and is now designing its national
population health monitoring
measured, such as a health event, strategy. Canada is conducting local
disease, condition, functional status, or pilot testing through strategic and research (see Chapters 5
well-being. A denominator is ‘‘the lower investments and is now designing its and 6)
portion of a fraction used to calculate a national strategy. New Zealand is Experts interviewed in Australia,
rate or ratio. The population. . . at risk conceptualizing its national strategy. Canada, England, New Zealand, and the
in the calculation of a rate or ratio.’’3 Review of publicly available U.S. identified potential contributions of
Denominators represent the population reports, presentations, Web sites, and electronic health records to population
in which the particular aspect of articles, and interviews with experts, health monitoring to produce health
population health is being measured. reveal that population health monitoring statistics and research employing health
Population-based health statistics require and research is explicitly secondary to statistics. Examples of these potential
both a known numerator and a known the primary uses of clinical care and contributions include the following.
denominator. management in the investigated national Integrating healthcare performance
strategies for electronic health records measurement with population health
National strategies in Australia, (see Chapters 4 and 5). Only England monitoring, such as the development of
Canada, England, and New has conceptualized, designed, and is integrated systems for measuring
now implementing the use of electronic
Zealand (see Chapters 3, 4, healthcare system performance at
health records for population health individual and provider group levels,
and 5) monitoring and research: the National with provider and provider group
Chapter 4 provides overviews of Health Service Secondary Uses Service measurements systematically aggregated
national strategies for electronic health has been established to ‘‘provide the to the population level.
records in Australia, Canada, England, NHS with higher quality data to enable Developing entirely new data for
and New Zealand, including the locus of investigation of trends and emerging population health monitoring and
responsibilities, current status and plans, health needs which can inform public research and entirely new options for
electronic health record definition, health policy and planning.’’4 Canada’s population health monitoring and
national health information infrastructure strategy includes communicable disease research, including:
elements related to electronic health surveillance.
records, electronic health records Consensus within nations does not + Establishing new disease and health
storage, patient confidentiality and exist on key issues underlying the use of condition registries yielding
participation, patient identification, and electronic health records for population previously unavailable population-
uses for population health monitoring health monitoring and research. These based morbidity and disease
and research. See Table S.1 for an issues include but are not limited to prevalence data;
abbreviated summary of the four whether and how national strategies for + Tracking how people move through
national strategies. electronic health records should support and beyond the healthcare system;
National strategies for electronic population health monitoring and + Ongoing linking of clinically rich
health records reflect the political, research, the parameters of patient data with population health
healthcare and systems, and market confidentiality and participation, the monitoring data from registries and
systems of individual countries (see harmonization of clinical data standards reportable disease systems,
Chapters 3 and 4). National strategies with population health monitoring data administrative health data,
for electronic health records also reflect standards, and the extent to which population-based surveys, and
both technical decisions and political complementary data sources; and
4
NHS Connecting for Health (2005 Oct). The + Using electronic health records as
National Programme for IT implementation guide: sampling frames for population
2
Last JM, Spasoff RM, Harris SS, Thuriaux Designed for the NHS by the NHS. Guidance to health monitoring and research.
MC, eds. (2001). A dictionary of epidemiology. support trusts when implementing National
NewYork City (NY): Oxford University Press;126. Programme products and services. Version 3.
3
Ibid;49. London (UK): NHS Connecting for Health:27.
viiiShifting predominant paradigms for research if they are associated with a Overarching issues
population health and clinical research, geographically based denominator with
Even if national strategies for
through erasing current distinctions known characteristics, and especially
electronic health records successfully
between clinical data and population demographic characteristics.
address issues relating to generating
health data.
Numerator and denominator issues numerators and denominators, the
penetration of electronic health records,
Fundamental issues in the In order to be most useful for
data quality and completeness, consent,
relationship between national generating valid population-based health
and unique patient identification, other
statistics, national strategies for
strategies for electronic health overarching issues remain that may limit
electronic health records should confront
records and population health the following numerator and
the utility of electronic health records
monitoring and research for population health monitoring and
denominator issues:
research.
(see Chapter 7) Penetration of electronic health
Population health and healthcare:
records: Electronic health records must
Numerators and denominators as Healthcare is only one of many
either penetrate an entire geographically
necessary conditions influences on population health. Given
based population, or a truly random
the multitude and variety of influences
Data derived from electronic health subset of that population with known
on population health, data collected
records may prove useful for multiple characteristics, or a non-random subset
through electronic health records in
purposes in addition to the clinical care of that population with known
healthcare settings may not adequately
of individual patients, including characteristics that can be linked to a
represent the full range of population
detecting health events and diseases for population denominator with known
health and the influences on it. In
the purposes of immediate public health characteristics.
addition to electronic health records,
interventions, identifying adverse events, Data quality and completeness:
population health monitoring and
monitoring the quality of clinical care, Numerator and denominator data
research may continue to require
and managing the provision of health produced by electronic health records
collection of data from other sources
care and health care resources. But in must meet the same professional
and through other mechanisms.
order for data derived from electronic standards of validity, reliability, and
Structured data in electronic health
health records to be used to characterize completeness as currently met by
records: Electronic health records will
the health of population, three population health monitoring data sets
only be useful for population health
conditions must be met. These three such as births, cancer incidence, and
monitoring and research if they contain
conditions relate to the known population-based surveys.
or can yield structured data that can be
numerators and denominators needed to Consent: Patient control of what
coded, classified, and statistically
produce population-based health data are entered into electronic health
analyzed.
statistics. records and used for population health
Analysis: In order to cull needed
monitoring and research may adversely
1. First, electronic health records must data in the needed formats from the
affect the quality and completeness of
produce numerator data about health huge amount of data in electronic health
numerator and denominator data.
events, conditions, diseases, records, public health practitioners will
Unique patient identification: Some
functional health status, well-being, need new technologies and
form of unique identification of
or influences on population health. methodologies.
individual patients is necessary if
2. Second, denominator data must exist Cultural changes: Cultural changes
electronic health records are to provide
that describes the population in terms will need to occur among public health
data for population health monitoring
of size, geographic location, and basic practitioners, clinicians, and the public if
and research. Unique patient
demographic characteristics for the electronic health records are to be used
identification could occur through
numerator data produced by electronic for population health monitoring and
numbering systems, or through
health records. Denominators are research.
algorithmic probabilistic or deterministic
typically defined at some geographic Incentives for the adoption and use
linkage of a specified set of identifier
level in health statistics. of electronic health records: Issues of
variables, or through a master patient
3. Third and finally, a match must exist providing and aligning incentives to
index. To the extent that health statistics
between the numerator and the clinicians for adopting and using
extend beyond health events, diseases,
denominator; in other words, the electronic health records for the
and conditions treated through the
numerator must be drawn from the secondary uses of population health
healthcare system, unique identification
population denominator. monitoring and research will be even
of patients rather than unique
more daunting than for the primary uses
Data derived from electronic health identification of each person in the
of clinical care.
records can only be useful for population may limit the development of
population health monitoring and population-based health statistics.
ixTransformative limits of electronic + greater central coordination of the Tipping factors maximize the
health records health system. potential for the successful use of
electronic health records for population
No single answer can be provided Health information system enabling
health monitoring and research. Tipping
to questions about the potential factors include:
factors include:
contribution of national strategies for
+ a closer relationship between the
electronic health records for population + a form of reimbursement for
provision of health care information
health monitoring and research. Answers physicians that could mandate the
for clinical and administrative
will depend upon at least four questions: nature, contents, and use of
purposes from data sources and the
electronic health records, such as
1. Does the particular data collection conduct of population health
salary-based reimbursement or other
stream include reportable diseases monitoring;
systems where physicians are
and registries, administrative health + reduced fragmentation among
required to follow established
data, or population-based surveys? population health monitoring data
uniform recording protocols;
2. Are electronic health records collections;
+ mandated implementation of
envisioned as supplementing current + clinician incentives for adopting and
implementation of electronic health
data collection streams, or replacing using electronic health records; and
records with mandated standards;
current data collection streams, or + cultural changes among clinicians
and
as a data source for linkage with supporting the use of electronic
+ confluence of strong governmental
current data collection streams? health records for population health
leadership of the healthcare sector
3. Do electronic health records meet monitoring.
and greater governmental
current population health
Threshold factors are factors coordination or control of the
monitoring criteria for data quality
without which the successful use of healthcare sector, which may be
and completeness?
electronic health records for population promoted through the existence of a
4. Will population-based
health monitoring and research may fail. predominant payer for healthcare or
implementation of electronic health
A business threshold factor is the a predominantly single payer
records lead to new population
explicit inclusion of population health system.
health monitoring criteria for data
monitoring and research as integral
quality and completeness, different
from those currently employed?
components of the national strategy for Conclusions (see Chapter 7)
electronic health records.
System threshold factors include In 2006, it is still too early to
Success factors
mandates within the national strategy for ascertain the actual potential of national
A definitive analysis identifying the strategies for electronic health records
electronic health records for:
factors leading to the successful use of for population health monitoring and
electronic health records for population + integrated electronic provision of research. With the exception of England,
health monitoring and research is not data and integrated data flows from the development of national strategies
possible given the current status of diverse healthcare sources for remains in germinal stages. Even in
national strategies for electronic health clinical, reimbursement, England, implementation is in an early
records. However, this report provides administrative, and population health stage. An evidence base does not exist
cautious speculation—intended to monitoring purposes; from which to judge how successfully
provoke discussion and debate—about + use of structured data for electronic national strategies for electronic health
factors maximizing the potential use of health records; records can support population health
electronic health records for population + the development of data standards monitoring and research. As indicated
health monitoring and research. jointly useful for clinical, by the National Health Service
Enabling factors increase the reimbursement, administrative, and Information Authority, ‘‘data needed to
likelihood of the successful use of population health monitoring support secondary information
electronic health records for population purposes; purposes. . . should be derivable from
health monitoring and research. + clear definitions of the data required data that is collected as part of the
Health system enabling factors to be collected for population health operational care process. . . However,
include: monitoring and clear rules for the critical aspects of this hypothesis remain
derivation of those data from operationally untested.’’5
+ greater funding of the healthcare
electronic health records; and
system by the government; 5
NHS Information Authority, National Dataset
+ some form of unique patient
+ a low percentage of individuals Development Programme (2002 Sep). Emerging
identification and the use of unique
without health insurance; a higher dataset issues: enabling the derivation of
patient identification, encrypted or ‘‘business’’ information from electronic records.
ratio of general practitioners to
unencrypted, for all electronic Draft 0.5 London (UK): NHS Information
specialists; and
provision of data. Authority: 3–4.
xTable S.1. National strategies for electronic health records, by country: 2005
Australia Canada England New Zealand
Locus of national HealthConnect Canada Health Infoway National Health Service (NHS) New Zealand Health Information
responsibilities (Department of Health and Ageing); Connecting for Health Service (Ministry of Health)
National E-Health Transition Authority
Stages* Design Design, with broad national target dates Implementation, with specific national Conceptualization
for implementation target dates
Current status – Initial national strategy published in – Initial national strategy published in – National strategy iteratively developed National strategy published in 2005
2004 2003, with updated strategy to be since 1998
– Local pilots implemented and evaluated published in 2006 – Local pilots implemented and evaluated
– Locus of responsibility for national – Strategic investments in key elements – Implementation of electronic patient
strategy evolving of supporting national health information records occurring regionally
– Key elements of supporting national infrastructure, including: registries – Implementation of electronic health
health information infrastructure being (client, provider, and location), record occurring nationally
specified, including: interoperability interoperable electronic health record
framework, health record design, systems, infostructure, innovation and
clinical terminologies, clinical adoption, and public health surveillance
information, healthcare identifier, and
E-health consent
Patient identification Under discussion and development, with Under discussion and development, with National Health Service number National Health Index number
possibility of adaptation of elements of emphasis on development of jurisdictional
national health insurance number unique identifiers and inter-jurisdictional
identifier
Patient confidentiality and – Initial conceptualization of opt-in Support for ‘‘lockbox,’’ enabling patients – ‘‘Sealed envelope,’’ enabling patients to Not ascertained from publicly
consent consent for participation in electronic to ‘‘mask’’ information at their request designate information not to be shared available materials
health records beyond their immediate clinician
– Consent options currently under – Pseudo-anonymized and anonymized
reconsideration and in development data can be shared for population
health monitoring
Population health monitoring – Initial conceptualization of National Data Investment in communicable disease Secondary Uses Service implemented, Emphasis on national data
Store of electronic health records, surveillance as part of national strategy with emphasis on uses of electronic collections
enabling uses of largely de-identified health records and other data streams for
data for population health monitoring population health monitoring
– Does not appear as current priority
secondary use
* Stages not intended to represent a continuum.
xiHighlights
Assessing the potential of National Strategies for Electronic Health Records for
Population Health Monitoring and Research
January 2006
Why NCHS commissioned this What this study did What this study found
study This study: National strategies for electronic
Healthcare costs continue to health records reflect the political,
1. Reviewed national strategies for
increase. The media, the public, and healthcare, and market systems of
electronic health records in Australia,
health professionals now recognize that individual countries. National strategies
Canada, England, and New Zealand,
unnecessary morbidity, mortality, and for electronic health records also reflect
and especially the implications of
healthcare costs resulting from adverse both technical decisions and political
those strategies for population health
events and medical errors are serious judgments, which may change over
monitoring by producing health
problems. The U.S. and other developed time. National strategies are developing
statistics and by encouraging research
nations are adopting health information and evolving, and passing through
employing health statistics. The
technology as a tool for rationalizing stages of conceptualization, design, pilot
review relied on reports,
complicated healthcare systems, testing, and implementation. Only
presentations, Web pages, and
improving the quality of patient care, England has moved to implementation.
articles, which were publicly
moderating healthcare costs, and Population health monitoring and
available before January 2006. See
reducing the incidence of adverse research, and especially health statistics,
Chapters 2 and 4.
events. Electronic health records are explicitly secondary to the primary
constitute the core of health information 2. Identified the potential contribution uses of clinical care and management in
technology. The U.S., Australia, Canada, of national strategies for electronic all national strategies for electronic
England, and New Zealand are all health records for population health health records. Only England has
developing national strategies for monitoring and research and barriers conceptualized, designed, and is now
electronic health records, accompanied to achieving that potential. The implementing the use of electronic
by substantial investments of public and identification of the potential health records for population health
private sector funds in implementing contribution and barriers relied on monitoring and research. Canada’s
those strategies. interviews with 96 experts in U.S., strategy does include communicable
The Centers for Disease Control Australia, Canada, England, and New disease surveillance, but not broader
and Prevention’s National Center Health Zealand. See Chapters 2, 5, and 6. population health monitoring for
Statistics commissioned this report to developing health statistics.
3. Delineated fundamental issues that
assess the potential contribution of This study identifies definitional
must be confronted to maximize the
national strategies for electronic health issues, numerator and denominator
contribution of national strategies for
records for population health monitoring issues, and overarching issues that must
electronic health records to
and research. The report focuses on be evaluated in assessing the potential
population health monitoring and
those types of population health of national strategies for electronic
research, and especially to health
monitoring that generate health statistics health records for population health
statistics. See Chapter 7.
for measuring the population’s health, monitoring and research. It also
rather than those types of population This study did not explore issues delineates success factors that increase
health monitoring used to detect health relating to the potential of national the potential for those national strategies
events and diseases for the purposes of strategies for electronic health records to contribute to population health
immediate public health interventions. for health event and disease detection monitoring and research, including
for the purposes of immediate public threshold, enabling, and tipping factors.
health interventions, such as case-based Finally, this study offers a sobering
surveillance, syndromic surveillance, assessment of the barriers that must be
and bioterrorism surveillance. overcome if national strategies for
electronic health records can contribute
to population health monitoring and
research, and especially to health
statistics.
xiiObjectives
This report assesses the potential of
national strategies for electronic health
Assessing the Potential of
records for population health monitoring and
research.
National Strategies for Electronic
Methods Health Records for Population
This study: 1. Reviewed national
strategies for electronic health records in
Australia, Canada, England, and New
Health Monitoring and Research
Zealand, through written materials available
before January 2006. 2. Identified the by Daniel J. Friedman, Ph.D., Population and Public Health
potential of national strategies for electronic
health records for population health
Information Services
monitoring and research through interviews
with 96 experts in the U.S., Australia,
Canada, England, and New Zealand.
3. Delineated fundamental issues that must
Chapter 1. collections mandates from state and
federal health agencies;
be confronted to maximize the contribution
of national strategies for electronic health
Introduction + multiple uses for collected data and
‘‘repurposing’’ of data integrated at
records to population health monitoring and
research.
the point of data collection; and
I
nitiated in October 2004, this project + greater utility and utilization of
builds upon two previous reports collected data for healthcare
Results
that portray a new landscape for providers, health agencies, and other
National strategies for electronic health
records reflect the political, healthcare, and
health statistics: Shaping a Health analysts and users.
market systems of individual countries. Statistics Vision for the 21st Century:
The Final Report, a joint report Both reports describe general
National strategies also reflect technical
decisions and political judgments. National strategies for achieving that more
developed by the National Committee
strategies are evolving, and passing through on Vital and Health Statistics, the rational future, revolving around
stages of conceptualization, design, pilot conceptual and practical integration of
testing, and implementation. Only England
Centers for Disease Control and
health statistics into the developing U.S.
has moved to implementation. Prevention’s National Center for Health
national health information infrastructure
Population health monitoring and Statistics, and the U.S. Department of
research are secondary to the primary uses (NHII). In related articles, Detmer
Health and Human Services’ Data
of clinical care and management in all (2003), Lumpkin and Deering (2005),
Council (Friedman, Hunter, Parrish
national strategies for electronic health
2002); and Information for Health: A and Lumpkin and Richards (2002) also
records. Only England has conceptualized, conceptualized the potential relationship
designed, and is implementing the use of Strategy for Building the National
Health Information Infrastructure, a between health statistics and the national
electronic health records for population
health monitoring and research. Canada’s health information infrastructure.
report released by the National
strategy includes communicable disease Committee on Vital and Health Statistics
surveillance, but not broader population
health monitoring for developing health
(2001). The two reports describe a more Purpose
statistics. rational future for population-based
The purpose of this report is to
This study identifies definitional, health data collection and analysis in the
numerator, denominator, and overarching assess the potential of national strategies
U.S., distinguished by:
issues that must be evaluated in assessing for electronic health records for
the potential of national strategies for + increased integration of presently population health monitoring and
electronic health records for population distinct data collections, especially research. The emphasis in this report is
health monitoring and research. It delineates those in which healthcare providers upon those types of population health
success factors that increase the potential
for those national strategies to contribute to
now respond to different but monitoring typically used to develop
population health monitoring and research. overlapping data collection mandates health statistics, such as population-
Finally, this study assesses barriers that from a single state health agency; based registries, population-based
must be overcome if national strategies for + decreased burden on healthcare surveys, and administrative health data,
electronic health records can contribute to providers responding to data rather than those types of population
population health monitoring and research,
and especially to health statistics.
Keywords: Electronic health records Author may be contacted at danieljfriedman@verizon.net or danieljfriedman@hotmail.com.
c population health c health statistics Disclaimer: The findings and conclusions in this report are those of the author and do not necessarily
represent the views of the Centers for Disease Control and Prevention.
Page 1Page 2 [ Series 2, No. 143
health monitoring used to detect health Population health event, disease, condition, functional
events and diseases for the purposes of status, or well-being.
immediate public health interventions. Kindig and Stoddart define
population health as ‘‘the health
More specifically, this report has a Denominator
fourfold purpose: first, to describe the outcomes of a group of individuals,
current status of national strategies for including the distribution of such A denominator is ‘‘the lower
electronic health records and their outcomes within the group’’ (Kindig and portion of a fraction used to calculate a
supporting national health information Stoddart 2003, p. 381). Population rate or ratio. The population. . . at risk
infrastructures in Australia, Canada, health encompasses the level and in the calculation of a rate or ratio’’
England, and New Zealand, especially distribution of disease, functional status, (Last et al., 49). Denominators represent
as those national strategies relate to and well-being within a group (Parrish, the population in which the particular
population health monitoring to produce Friedman, and Hunter 2005, 18). See aspect of population health is being
health statistics and research employing Figure 1.1. measured.
health statistics; second, to summarize
themes about the potential contributions, Population health monitoring Health statistics
and barriers to those contributions, of Population health monitoring can be Health statistics are defined as
national strategies for electronic health defined as the collection and analysis of ‘‘numerical data that characterize the
records for population health monitoring data to detect and describe changes in health of a population and the influences
and research and barriers that emerged the population’s health and influences that affect its health’’ (Parrish,
from key informant interviews with on the population’s health. See Friedman, and Hunter 2005, 3). Health
experts in the same four countries; third Figure 1.1. Population health monitoring statistics are generated through
to summarize themes emerging from can occur through either (a) intermittent population health monitoring, and are
key informant interviews with U.S. but regularly scheduled primary employed for conducting population
experts; and fourth, to delineate major collection of data (that is, data health research. The types of population
fundamental issues in the relationship specifically collected for the purpose of health monitoring that typically generate
between national strategies for electronic population health monitoring) and the health statistics are reportable diseases
health records and population health and analysis of those data, or (b) ongoing and registries, administrative health data,
monitoring. This study did not explore primary collection data and their and population-based surveys, as well as
issues relating to the potential of national analysis, or (c) intermittent or ongoing nonhealth data sources (Bailey et al.
strategies for electronic health records for secondary collection of data (that is, 2005; Iezzoni, Shwartz, and Ash 2005,
health event and disease detection for the data not specifically collected for the 139–160; Koo, Wingo, and Rothwell
purposes of immediate public health purpose of population health 2005, 81–118; Madans and Cohen 2005,
interventions, such as case-based monitoring) and their analysis. Primary 119–138). This report focuses largely on
surveillance, syndromic surveillance, and collection of data for population health those types of population health
bioterrorism surveillance. monitoring typically occurs through monitoring that generate health statistics.
registries and mandated reports of Population-based health statistics
Central Concepts diseases and population-based surveys require both a known numerator and a
(Koo, Wingo, and Rothwell 2005; known denominator. In order to
Central concepts utilized Madans and Cohen 2005). Secondary characterize the health of a population
throughout this report are defined and collection of data for population health through health statistics, three
discussed here. These include monitoring typically occurs from necessary conditions relating to
population health, population health administrative health data and nonhealth numerators and denominators must be
monitoring, population health research, data sources (Bailey et al. 2005; Iezzoni, met. First, numerator data must exist
health statistics, electronic patient Schwartz, and Ash 2005). about a health event, condition,
records, shared electronic health disease, functional health status,
records, and national health
Population health research well-being, or an influence on
information infrastructure. Especially population health. Second,
important for understanding this Population health research is denominator data must exist that
report’s discussions of developments research on population health or those describe the population in terms of its
in Australia, Canada, England, and factors that affect population health. size, its geographic location, and its
New Zealand are the distinctions basic demographic characteristics.
between electronic patient records and Numerator Third and finally, a match must exist
shared electronic health records between the numerator and the
described below. Additional definitions A numerator is ‘‘the upper portion
of a fraction, used to calculate a rate or denominator; in other words, the
of terms and acronyms are provided in numerator must be drawn from the
the Glossary. a ratio’’ (Last et al., 126). Numerators
represent the aspect of the population’s population denominator.
health being measured, such as a healthSeries 2, No. 143 [ Page 3
Figure 1.1. Influences on the population’s health
SOURCE: Parrish RG, Friedman DJ, Hunter EL (2005). Defining health statistics and their scope. In: Friedman DJ, Hunter EL, Parrish RG (editors), Health Statistics:
Shaping Policy and Practice to Improve the Population’s Health. New York: Oxford University Press; 18.
Electronic patient records (EPRs) shared or interoperable across providers The definition of electronic health
and provider sites. As described by the record used in this report assumes that
This report adopts the definition of Institute of Medicine, by the National they are interoperable and capable of
electronic patient records used by the Health Service, and by numerous other being shared across healthcare providers
United Kingdom’s National Health sources, the electronic patient record can and provider sites.1 This report deals
Service in its Information for Health: include a wide range of functionalities principally with national strategies for
the ‘‘’Electronic Patient Record’ in support of the direct provision of care electronic health records and supporting
describes the record of the periodic care (Brennan 2005, 67–70; Institute of national health infrastructures (defined
provided mainly by one institution’’ Medicine 2003, 7–12). below).
(NHS Executive 1998 Sep, 25). In other This report seeks to synthesize the
words, as used here in contrast to the
Electronic health records perspectives of almost one hundred
shared electronic health record described experts in five countries. As the report
immediately below, the electronic (EHRs)
describes, the definition of electronic
patient record is the desktop record For the purposes of this report, health records differs across these
utilized by the clinician in providing, electronic health records are defined as countries. In extracting common themes
managing, and recording care for an electronic repository of patient-
individual patients. Also in contrast to centric data that are identifiable, 1
the shared electronic health record longitudinal and preferably life-long, ‘‘In healthcare, interoperability is the ability of
(defined below), the electronic patient different information technology systems and
cross-provider, cross-provider site, and software applications to communicate, to exchange
records can be specific to an individual cross the spectrum of healthcare, data accurately, effectively, and consistently, and
healthcare provider or an individual including primary care, acute hospital to use the information that has been exchanged’’
healthcare provider site, or it can be care, long-term care, and home care. (National Alliance for Health Information
Technology [hp]).Page 4 [ Series 2, No. 143
across countries from interviews with Health Information Technology in its but, more importantly, values, practices,
those informants and in identifying ‘‘The Decade of Health Information relationships, laws, standards, systems,
fundamental factors across countries Technology: Delivering Consumer- and applications that support all facets
enabling the use of electronic health centric and Information-rich of individual health, healthcare, and
records for population health monitoring Healthcare’’, and by Amatayakul in her public health. It encompasses tools such
and research, this report will use a Electronic Health Records: A Practical as clinical practice guidelines,
definition of electronic health records Guide for Professionals and educational resources for the public and
used throughout this report is similar to Organizations (Amatayakul 2004, 1–4; health professionals, geographic
the definition posited by the Institute of Medicine 2003, 7–12; information systems, health statistics at
International Standards Organization Thompson and Brailer 2004 Jul 21, 37). all levels of government, and many
Technical Committee 215 in its ‘‘Health It is essential to realize that ‘‘there forms of communication among users’’
Informatics—Electronic health is as yet no one internationally accepted (National Committee on Vital and
record—definition, scope, and context’’, definition of the electronic health Health Statistics 2001, 1). As initially
in which it the electronic health record record’’ or the electronic patient record conceptualized by the NCVHS, the
for integrated care (ICEHR) is described (Standards Australia 2005, v, 4). Many national health information infrastructure
as ‘‘a repository of information different terms describing systematic includes three main dimensions: the
regarding the health status of a subject electronic record keeping for patient healthcare provider, population health,
of care in computer processable form, information have been used at different and personal health dimensions
stored and transmitted securely, and times and in different countries by (National Committee on Vital and
accessible by multiple authorised users. different authors and different Health Statistics 2001, 14–16). These
It has a standardized or commonly organizations (Brailer 2003 Oct, 7; dimensions can also be seen as different
agreed logical information model which DeVault, Fischetti, Spears 2005, 4; ‘‘views.’’ The three dimensions can be
is independent of EHR systems. Its Schloeffel 2004 Sep 1). Some extended and re-conceptualized to
primary purpose is the support of definitions are broad and general (for include others dimensions or views,
continuing, efficient and quality example, see: Canadian Institute for such as research, public health,
integrated healthcare and it contains Health Information [hp] Partnership for healthcare delivery, and personal health
information which is retrospective, Health Information Standards, Glossary management (Detmer 2003).
concurrent, and prospective’’ (ISO TC of Terms; CEN/TC 251; Wyatt and Liu This report uses a narrower,
215/WG 1 2004 Jul 29; Schloeffel 2002). Other definitions include detailed component-based definition of national
2004). The definition is also similar to functionalities (for example, see: health information infrastructures,
that posited by the United Kingdom’s DeVault, Fischetti, Spears 2005). When focusing on electronic health records,
National Health Service in Information for comparing definitions of electronic often built upon electronic patient
Health: the EHR ‘‘is used to describe the patient records and electronic health records, and shared through inter
concept of a longitudinal record of records, it is essential to focus on the operability, electronic connectivity,
patient’s health and healthcare—from attributes described in the particular common standards for coding and
cradle to grave. It combines both the definitions rather than assuming that classification, nomenclature, and
information about patient contacts with commonalities exist between definitions messaging. Paraphrasing the NCVHS, a
primary healthcare as well as subsets of of electronic patient records or national health information
information associated with the outcomes electronic health records from different infrastructure, as defined for the
of periodic care held in the EPRs’’ (NHS sources (National Committee on Vital purposes of this report, refers to the
Executive 1998 Sep, 25; see also Brennan and Health Statistics 2005 Sep 9). technologies, relationships, laws,
2005, 81–3). standards, systems, and applications that
The definition of electronic health National health information support the development,
records employed in this report does not infrastructure (NHII) implementation, and dissemination of
necessarily include the actual desktop electronic health records.
electronic record used by clinicians for In Information for Health: A
direct care functions such as care Strategy for Building the National
management, clinical decision support, Health Information Infrastructure, the
and operations management and National Committee on Vital and Health
communication (DeVault, Fischetti, Statistics (NCVHS) described ‘‘the heart
Spears 2005 Nov, 8). As such, the of the vision for the NHII . . . [as]
definition of electronic health records sharing information and knowledge
used in this report differs from some appropriately so it is available to people
other definitions of electronic health when they need it to make the best
records, such as those of the Institute of possible health decisions’’ (National
Medicine in its ‘‘Key capabilities of an Committee on Vital and Health Statistics
electronic health record system’’, by the 2001, 1). According to the NCVHS,
Office of the National Coordinator for ‘‘the NHII includes not just technologiesYou can also read