Article Type: Original Investigation Longitudinal Associations Between Low Serum Bicarbonate and Linear Growth In Children With Chronic Kidney Disease
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Kidney360 Publish Ahead of Print, published on February 9, 2022 as doi:10.34067/KID.0005402021
American Society of Nephrology
1401 H St NW, Suite 900
Washington, DC 20005
Phone: 202-640-4660 | Fax 202-637-9793
vramsey@kidney360.org
How to Cite this article: Denver Brown, Megan Carroll, Derek Ng, Rebecca Levy, Larry Greenbaum, Frederick Kaskel, Susan Furth, Bradley
Warady, Michal Melamed, and Andrew Dauber, Longitudinal Associations Between Low Serum Bicarbonate and Linear Growth In Children With
Chronic Kidney Disease, Kidney360, Publish Ahead of Print, 10.34067/KID.0005402021
Article Type: Original Investigation
Longitudinal Associations Between Low Serum Bicarbonate and Linear Growth In Children With Chronic
Kidney Disease
DOI: 10.34067/KID.0005402021
Denver Brown, Megan Carroll, Derek Ng, Rebecca Levy, Larry Greenbaum, Frederick Kaskel, Susan Furth, Bradley Warady, Michal Melamed, and
Andrew Dauber
Key Points:
*Poor linear growth is common in children with CKD and identifying modifiable risk factors is crucial to improving pediatric CKD care.
*Our study shows a negative longitudinal association between metabolic acidosis and linear growth in children with varying CKD severity.
*We found that persistent use of alkali therapy was associated with improved linear growth in children with CKD.
Abstract:
Background: Poor linear growth is a consequence of chronic kidney disease (CKD) that has been linked to adverse outcomes. Metabolic acidosis (MA)
has been identified as a risk factor for growth failure. We investigated the longitudinal relationship between MA and linear growth in children with CKD
and examined whether treatment of MA modified linear growth. Methods: To describe longitudinal associations between MA and linear growth, we used
serum bicarbonate levels, height measurements and standard deviation (z-scores) of children enrolled in the prospective cohort study, Chronic Kidney
Disease in Children. Analyses were adjusted for covariates recognized as correlating with poor growth including demographic characteristics, glomerular
filtration rate (GFR), proteinuria, calcium, phosphate, parathyroid hormone, and CKD duration. CKD diagnoses were analyzed by disease categories, non-
glomerular or glomerular. Results: The study population included 1082 children with CKD: 808 with non-glomerular etiologies and 274 with glomerular
etiologies. Baseline serum bicarbonate levels {less than/equal to}22mEq/L were associated with worse height z-scores in all children. Longitudinally,
serum bicarbonate levels {less than/equal to}18mEq/L and 19-22mEq/L were associated with worse height z-scores in children with non-glomerular
CKD causes, with adjusted mean values of -0.39, (95%CI: -0.58, -0.20) and -0.17, (95%CI: -0.28, -0.05), respectively. Children with non-glomerular
disease and more severe GFR impairment had a higher risk for worse height z-score. A significant association was not found in children with glomerular
diseases. We also investigated the potential effect of treatment of MA on height in children with a history of alkali therapy use finding that only persistent
users had a significant positive association between their height z-score and higher serum bicarbonate levels. Conclusions: We observed a longitudinal
association between MA and lower height z-score. Additionally, persistent alkali therapy use was associated with better height z-scores. Future clinical
trials of alkali therapy need to prospectively evaluate this relationship.
Disclosures: M. Carroll reports the following: Ownership Interest: Verily Life Sciences; and Research Funding: Verily Life Sciences. A. Dauber
reports the following: Ownership Interest: Biomarin, Novo Nordisk, Ascendis; and Research Funding: Biomarin. L. Greenbaum reports the following:
Consultancy: Arrowhead Pharmaceuticals, CorMedix, Novartis, Advicenne, Alexion, Roche, Aurinia, NephroDI Therapeutics, Abbvie, Otsuka, Natera;
Research Funding: Alexion, Advicenne, Abbvie, Apellis, Aurinia, Reata Pharmaceuticals, Horizon Pharmaceuticals, Vertex; Honoraria: Alexion; Advisory
or Leadership Role: Alexion; and Other Interests or Relationships: DSMB payments: Alnylam, Relypsa, Travere, UCSD, Akebia. R. Kaskel reports the
following: Research Funding: NIDDK; and Advisory or Leadership Role: Frost Valley YMCA; Nephcure Inc. M. Melamed reports the following:
Advisory or Leadership Role: American Board of Internal Medicine Nephrology Exam Committee; and Other Interests or Relationships: New York
Society of Nephrology; American Society of Nephrology. D. Ng reports the following: and Consultancy: Ashvattha Therapeutics. B. Warady reports the
following: Consultancy: Amgen, Reata, Bayer, Relypsa, UpToDate, Lightline Medical; Research Funding: Baxter Healthcare; Honoraria: Relypsa, Reata,
Amgen, Bayer, UpToDate; and Advisory or Leadership Role: North American Pediatric Renal Trials and Collaborative Studies, National Kidney
Foundation, NTDS Board of Directors, Midwest Transplant Network Governing Board. The remaining authors have nothing to disclose.
Funding: Developmental and Translational Nephrology Training Grant:, T32 DK007110; HHS | NIH | Eunice Kennedy Shriver National Institute of
Child Health and Human Development (NICHD):, K12HD001399
Copyright 2022 by American Society of Nephrology.Author Contributions: Denver Brown: Conceptualization; Data curation; Funding acquisition; Investigation; Methodology; Supervision; Writing -
original draft; Writing - review and editing Megan Carroll: Data curation; Formal analysis; Methodology; Software; Validation; Writing - original draft;
Writing - review and editing Derek Ng: Data curation; Formal analysis; Methodology; Software; Writing - original draft; Writing - review and editing
Rebecca Levy: Methodology; Writing - review and editing Larry Greenbaum: Methodology; Writing - original draft; Writing - review and editing
Frederick Kaskel: Methodology; Writing - original draft; Writing - review and editing Susan Furth: Conceptualization; Methodology; Writing - review and
editing Bradley Warady: Conceptualization; Methodology; Resources; Writing - review and editing Michal Melamed: Conceptualization; Methodology;
Supervision; Writing - original draft; Writing - review and editing Andrew Dauber: Data curation; Investigation; Methodology; Supervision; Writing -
original draft; Writing - review and editing
Data Sharing Statement:
Clinical Trials Registration:
Registration Number:
Registration Date:
The information on this cover page is based on the most recent submission data
from the authors. It may vary from the final published article. Any fields remaining
blank are not applicable for this manuscript.Longitudinal Associations Between Low Serum Bicarbonate and Linear Growth In
Children With Chronic Kidney Disease
Denver D. Brown,1* Megan Carroll2*, Derek K. Ng2, Rebecca V. Levy3, Larry A. Greenbaum 4,
Frederick J. Kaskel5, Susan L. Furth6, Bradley A. Warady7, Michal L. Melamed 8+, Andrew
Dauber9+ for the CKiD Study Investigators
1. Division of Nephrology, Children’s National Hospital, Washington, DC
2. Johns Hopkins Bloomberg School of Public Health, Baltimore, MD
3. Division of Pediatric Nephrology, University of Rochester Medical Center, Rochester, NY
4. Division of Pediatric Nephrology, Emory University School of Medicine and Children's
Healthcare of Atlanta, Atlanta, GA
5. Division of Pediatric Nephrology, The Children’s Hospital at Montefiore, Bronx, NY
6. Division of Pediatric Nephrology, The Children's Hospital of Philadelphia, Philadelphia, PA
7. Division of Pediatric Nephrology, Children’s Mercy Hospital, Kansas City, MO
8. Department of Medicine, Albert Einstein College of Medicine, Bronx, NY
9. Division of Endocrinology, Children’s National Hospital, Washington, DC
* Co-First Authors
+ Co-Last Authors
Address correspondence to: Dr. Denver D. Brown, Division of Nephrology, Children’s National
Hospital, 111 Michigan Ave, NW, Washington, DC
Email: ddbrown@childrensnational.orgKey Points
• Poor linear growth is common in children with CKD and identifying modifiable risk
factors is crucial to improving pediatric CKD care.
• Our study shows a negative longitudinal association between metabolic acidosis
and linear growth in children with varying CKD severity.
• We found that persistent use of alkali therapy was associated with improved
linear growth in children with CKD.
Abstract
Background: Poor linear growth is a consequence of chronic kidney disease (CKD) that has
been linked to adverse outcomes. Metabolic acidosis (MA) has been identified as a risk factor
for growth failure. We investigated the longitudinal relationship between MA and linear growth in
children with CKD and examined whether treatment of MA modified linear growth.
Methods: To describe longitudinal associations between MA and linear growth, we used serum
bicarbonate levels, height measurements and standard deviation (z-scores) of children enrolled
in the prospective cohort study, Chronic Kidney Disease in Children. Analyses were adjusted for
covariates recognized as correlating with poor growth including demographic characteristics,
glomerular filtration rate (GFR), proteinuria, calcium, phosphate, parathyroid hormone, and CKD
duration. CKD diagnoses were analyzed by disease categories, non-glomerular or glomerular.
Results: The study population included 1082 children with CKD: 808 with non-glomerular
etiologies and 274 with glomerular etiologies. Baseline serum bicarbonate levels ≤22mEq/L
were associated with worse height z-scores in all children. Longitudinally, serum bicarbonate
levels ≤18mEq/L and 19-22mEq/L were associated with worse height z-scores in children with
non-glomerular CKD causes, with adjusted mean values of -0.39, (95%CI: -0.58, -0.20) and -
0.17, (95%CI: -0.28, -0.05), respectively. Children with non-glomerular disease and more severe
GFR impairment had a higher risk for worse height z-score. A significant association was not
found in children with glomerular diseases. We also investigated the potential effect of treatment
of MA on height in children with a history of alkali therapy use finding that only persistent users
had a significant positive association between their height z-score and higher serum
bicarbonate levels.
Conclusions: We observed a longitudinal association between MA and lower height z-score.
Additionally, persistent alkali therapy use was associated with better height z-scores. Future
clinical trials of alkali therapy need to prospectively evaluate this relationship.Introduction Linear growth impairment is a consequence of chronic kidney disease (CKD) that has been associated with profound risk for adverse outcomes.[1-3] In an early investigation from the Pediatric Growth and Development Special Study, every 1 standard deviation (SD) decrease in height was an associated 14% increased risk for death.[1] Similarly, in the North American Pediatric Renal Trials and Collaborative Studies, compared to children with heights ≥1st percentile, children with heights below the 1st percentile had a two-fold higher risk of death.[4] Poor growth also has profound psychosocial impact. Children with CKD who suffer from short stature report lower physical functioning scores on health-related quality of life assessment tools.[2, 3] Higher parental scores of physical and social functioning have been associated with increases in height z-score.[3] Since growth failure is estimated to affect up to 35% of the pediatric CKD population[5], it is important to understand factors that contribute to short stature in order to better manage these patients. The etiology of growth failure in pediatric CKD is complex but numerous studies point to metabolic acidosis (MA) as a contributing factor.[6-11] The theorized mechanism involves disturbances of growth hormone (GH), and its mediating hormone, insulin-like growth factor-1 (IGF-1).[12-14] MA has been reported to impair GH secretion, reduce hepatic IGF-I mRNA, and alter concentration of and sensitivity to IGF-1. Baseline data from the Chronic Kidney Disease in Children (CKiD) study, shows that as many as one third of children with mild to moderate CKD have low serum bicarbonate levels, a proxy for MA.[7, 15, 16] In a cross-sectional analysis of the CKiD cohort, Rodig et al., found that children with a serum bicarbonate of
mL/min/1.73m2. CKiD has enrolled children 6 months old to 16 years old at study entry; our study required a minimum age of 2 years old (minimum age for standing height measurements). In the first year, participants are seen twice then annually thereafter. At each study visit demographic and clinical data are obtained; this includes growth measurements and serum samples for measurement of kidney function and related biomarkers. A full description of the CKiD study and cohort has been previously published.[18] All participants and families provided informed assent or consent. All protocols were approved by the Institutional Review Board. Primary Exposure: Serum Bicarbonate Serum bicarbonate results were obtained and measured at local study site laboratories. Low serum bicarbonate was defined as ≤22mEq/L and normal defined as >22mEq/L.[19] For both baseline and longitudinal analyses, abnormal serum bicarbonate was further clinically categorized as ≤18mEq/L (very low) and19-22mEq/L (low). We also looked at height z-score on serum bicarbonate as a continuous predictor in specified analyses. Primary Outcome: Linear Growth A wall-mounted stadiometer was used to measure height (i.e., linear growth) at study visits. Final recorded height was based on averaging two separate measurements, to the nearest 0.1cm. If the measures differed by more than 0.3cm, a third measurement was made and an average of all three measurements used. Height was converted to height z-scores (i.e., standard deviations) and percentiles according to CDC estimates for the normal population adjusted for age and gender.[20] Longitudinal analyses included participant-visits during regular study follow-up among those < 20 years of age with complete data on serum bicarbonate (exposure) and height z-score (primary outcome). Stratification and Covariate Definitions The CKD diagnoses were broadly classified into two primary disease categories: non- glomerular or glomerular (specific CKD diagnoses are described in Supplemental Table 1), and all analyses were stratified as such. In longitudinal analyses, participants were also stratified by GFR, ≥45mL/min/m2 (mild-moderate CKD) and
Missing covariate data were imputed using multiple imputation by chained equations (MICE) methods to limit the impact of missing follow-up data. The method used Gibbs sampling to perform 5 imputations of missing values for the “target covariate” based on values from all other covariates in the dataset. Missing values were imputed separately for those with non-glomerular and glomerular diagnoses. Statistical Methods Median, interquartile ranges, and proportions described the demographic, clinical history, growth and kidney disease characteristics of the cohort at participants’ first available visit. To characterize the association between serum bicarbonate and linear growth, we used repeated measures linear regression models with height z-score as the outcome and bicarbonate from the previous year as a categorical exposure. Models were stratified by diagnosis and were unadjusted (i.e., no covariates), partially adjusted (specifically, age, sex, abnormal birth history, mid-parental height and previous levels of eGFR and proteinuria), and fully adjusted (the same covariates with the addition of calcium, phosphate, iPTH, and CKD duration). Generalized estimating equations (GEE) were used to account for longitudinal measurements within an individual. As a supplementary analysis, we investigated serum bicarbonate as a predictor of growth velocity z-scores. Additionally, we characterized the relationship between serum bicarbonate and height z-score among participants 13 years and younger (i.e., pre-pubertal age range) by longitudinal alkali therapy use. Specifically, the unit of analysis was pairs of visits, we restricted to participants who reported using alkali therapy at the first visit, and compared those who discontinued use (i.e., used alkali therapy at the previous visit, but not at the current visit) to those who were persistent users (i.e., used alkali therapy at both the previous and current visit). For children with varying alkali therapy use during yearly follow-up (i.e., discontinued user during follow-up who became a persistent user or persistent user who became a discontinued user), they could contribute data to both groups. GEE were also used to account for correlated repeated measures within an individual. Estimates of differences are presented with two-sided 95% confidence intervals: differences were statistically significant if the interval did not contain the null value (0) which corresponds to p
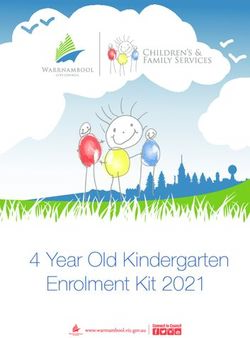
CKD etiology. In both primary disease groups, baseline serum bicarbonate ≤22mEq/L was associated with lower height measurements, worse height z-scores, and a higher number of patients on GH therapy. Regarding alkali therapy, in patients with non-glomerular disease, serum bicarbonate ≤22mEq/L was associated with a borderline higher rate of reported alkali therapy use while it trended in this direction in children with glomerular disease but was not statistically significant. For patients with non-glomerular diseases, 45% (360/808) had a baseline bicarbonate of ≤22mEq/L and 34% (122/360) of those patients reporting treatment with alkali therapy. For children with glomerular diseases, 35% (97/274) had a baseline bicarbonate of ≤22mEq/L and 16% (16/97) endorsed alkali therapy treatment. Reported GH therapy use was low in the overall analyzed cohort at 9%. For longitudinal analyses, we grouped serum bicarbonate from the previous study visit (i.e., lagged values) by clinically relevant categories as very low (≤18mEq/L), low (19-22mEq/L), and normal (>22mEq/L) and examined the distribution of height z-scores across bicarbonate groups. This was done to examine the clinical utility of bicarbonate levels in predicting future height outcomes. Figure 1 demonstrates that, longitudinally, worse serum bicarbonate levels were associated with worse height z-scores in all children with CKD, independent of CKD etiology. In fully adjusted models, current serum bicarbonate and growth measurements were utilized. In these analyses we continued to find that very low and low bicarbonates were associated with significantly worse height z-scores in children with non-glomerular CKD, fully adjusted mean - 0.39, (95%CI: -0.58, -0.20) and -0.17, (95%CI: -0.28, -0.05), respectively (Table 2a). When restricted to patients who had measured GFR available, we found this association continued to persist and was more pronounced (Table 2b). Height z-scores were overall higher in children with glomerular CKD compared to those with non-glomerular CKD (Figure 1). In examining whether lower serum bicarbonate was linked to worse height z-score in children with glomerular diseases, the only significant association noted was in unadjusted analyses of children with serum bicarbonate 19-22mEq/L (Table 2a and b). In sensitivity analyses excluding the children who reported GH use, associations were unchanged for children with non-glomerular CKD. Due to the small number of children with a glomerular diagnosis, data from low bicarbonate groups were combined and height z-scores in children with serum bicarbonate ≤22mEq/L were compared with children with normal bicarbonates with no significant relationship observed. (Supplemental Table 2). In analyses stratified by GFR, both estimated (Table 3a) and measured (Table 3b), using ≥45 (mild to moderate CKD) and
higher serum bicarbonate in the previous year. In fully adjusted models, we observed that a
1mEq increase in serum bicarbonate was associated with increases in height z-scores in all
children with CKD; however, this relationship was not significant.
In a categorical exploratory analysis of the entire cohort restricted to pre-pubertal aged children,
low serum bicarbonate levels were linked to lower height z-scores, achieving significance in the
very low serum bicarbonate category when eGFR was used for fully adjusted models. When
measured GFR was utilized, this relationship was significant in fully adjusted models for both
very low and low serum bicarbonates (Supplemental Tables 4a and b).
Finally, we investigated the effect of treatment of MA on height z-score in pre-pubertal aged
children (Table 4a and 4b). We examined current height z-score as a function of change in
serum bicarbonate in participants reporting alkali therapy use at the previous study visit. Height
outcome was separated by current reported alkali therapy use (i.e., “persistent” use if still being
treated with alkali therapy versus “discontinued” use for those no longer reporting use of alkali
therapy). In these models that utilized bicarbonate in a “lagged” manner, persistent alkali
therapy users had a significant positive association between their height z-score and serum
bicarbonate levels; the significance of this association was lost when measured GFR was
utilized. Independent of the GFR used, there was a positive but not significant relationship in
discontinued users.
Discussion
Using annual serum bicarbonate values over a robust duration of follow-up, our data suggests a
longitudinal association between MA and lower height z-score. After adjusting for demographic
characteristics, markers of CKD severity, and pertinent clinical variables, serum bicarbonate
≤22mEq/L was associated with lower height z-scores with the worst height z-scores observed in
the lowest bicarbonate category (≤18mEq/L). This association reached significance among
children with non-glomerular CKD only. Though overall height z-scores were reduced in all
children with CKD, children with non-glomerular diseases had greater deficits in height z-score
than children with glomerular diseases. Not unexpectedly, use of measured GFR data showed
similar associations compared to use of eGFR except when measured GFR was dichotomized
as >45 and ≤45mL/min/1.73m2. In these analyses, in participants with non-glomerular diseases,
very low serum bicarbonate was associated with worse height z-score across both measured
GFR groups compared to analyses that utilized eGFR where this association was only seen in
children in the ≤45 group. This is noteworthy because while use of measured GFR is not routine
clinical practice, it is more accurate than eGFR suggesting that the association of worse height
z-scores with MA may be present in the milder CKD group. Finally, and of clinical relevance is
that our data suggest that alkali therapy use as a marker of treatment of MA, was associated
with improved height z-score, particularly in persistent users.
We found height outcome differences between children with non-glomerular and glomerular
etiologies of CKD. Observed differences in linear growth could be attributed to sample size
differences between the groups, later age of CKD onset in children with glomerular disease (i.e.
less time during which the sequelae of CKD can affect active linear growth), older age of the
5participants with glomerular disease, and previously published evidence that indicates these primary disease groups may not be similarly affected by CKD comorbidities.[16, 23] Our findings are, in part, in line with previous baseline investigations of the relationship between low serum bicarbonate and growth. In a prior cross-sectional study using the CKiD cohort, Rodig et al., observed that baseline height was lower in children with a baseline serum bicarbonate of
agents.[7, 16] Data from our current investigation suggests that long term use of alkali therapy
may have beneficial effects on height in children with CKD. However, clinical trials of alkali
therapy in children with varying severity of impaired kidney function are needed to better inform
practitioners of the potential benefits of treatment, as no such trial exists to date.
While our study has several strengths, there are limitations. Nutritional data in this cohort was
incomplete so we were unable to fully account for its effect on height. We do include data on
underweight children (based on BMI; Tables 1a and 1b). Only 4% of the entire cohort is
underweight reflecting the likely low occurrence of severe malnutrition. Serum bicarbonate was
used as an indicator of MA in this study because serum pH data was not available; it is possible
that serum bicarbonate was not equivalent to actual acid/base status. Additionally, we were not
able to assess true duration of alkali therapy as exact start dates were unknown, and for those
with historical use, we were unable to determine when the alkali agent was discontinued.
Important to note is that we were unable to confirm adherence with alkali therapy in those who
reported use. Another limitation is that we were also only able to account for the previous year’s
level of bicarbonate and other covariates measured one year prior. It would have been
preferable to account for longer duration of clinical covariates in a marginal structural model
framework, but data were limited to account for longer than one year earlier. An additional
limitation is the inclusion of the small number of children on GH in primary analyses, however,
sensitivity analyses showed no significant changes in study conclusions when these patients
were excluded. Finally, we are aware that results may be affected by confounding by indication
as children with more severe acidosis and complications were more likely to be prescribed alkali
therapy.
Despite its limitations, to our knowledge, our study is the first to examine the longitudinal
relationship between MA and linear growth, as well as the potential effect of acidosis correction,
in a multi-ethnic cohort of children with varying CKD severity. Since there are safe and effective
therapies to treat metabolic acidosis, an increased understanding of this relationship may inform
treatment practices and prove crucial to improving pediatric CKD care. While our observed
associations were small by number, our findings of the negative correlation between low serum
bicarbonate and linear growth in children with CKD, as well as the suggested height benefits of
alkali therapy are important given the profound impact impaired growth may have in this
vulnerable population. Future clinical trials of alkali therapy need to prospectively evaluate this
relationship and other important disease outcomes in children with MA and chronically impaired
kidney function.
Disclosures
M. Carroll reports the following: Ownership Interest: Verily Life Sciences; and Research
Funding: Verily Life Sciences. A. Dauber reports the following: Ownership Interest: Biomarin,
Novo Nordisk, Ascendis; and Research Funding: Biomarin. L. Greenbaum reports the following:
Consultancy: Arrowhead Pharmaceuticals, CorMedix, Novartis, Advicenne, Alexion, Roche,
Aurinia, NephroDI Therapeutics, Abbvie, Otsuka, Natera; Research Funding: Alexion,
Advicenne, Abbvie, Apellis, Aurinia, Reata Pharmaceuticals, Horizon Pharmaceuticals, Vertex;
7Honoraria: Alexion; Advisory or Leadership Role: Alexion; and Other Interests or Relationships:
DSMB payments: Alnylam, Relypsa, Travere, UCSD, Akebia. R. Kaskel reports the following:
Research Funding: NIDDK; and Advisory or Leadership Role: Frost Valley YMCA; Nephcure
Inc. M. Melamed reports the following: Advisory or Leadership Role: American Board of Internal
Medicine Nephrology Exam Committee; and Other Interests or Relationships: New York Society
of Nephrology; American Society of Nephrology. D. Ng reports the following: and Consultancy:
Ashvattha Therapeutics. B. Warady reports the following: Consultancy: Amgen, Reata, Bayer,
Relypsa, UpToDate, Lightline Medical; Research Funding: Baxter Healthcare; Honoraria:
Relypsa, Reata, Amgen, Bayer, UpToDate; and Advisory or Leadership Role: North American
Pediatric Renal Trials and Collaborative Studies, National Kidney Foundation, NTDS Board of
Directors, Midwest Transplant Network Governing Board. The remaining authors have nothing
to disclose.
Funding
This work was supported by the Developmental and Translational Nephrology Training Grant
(T32 DK007110) and HHS | NIH | Eunice Kennedy Shriver National Institute of Child Health and
Human Development (NICHD) (K12HD001399).
Acknowledgements
Data in this manuscript were collected by the Chronic Kidney Disease in children prospective
cohort study (CKiD) with clinical coordinating centers (Principal Investigators) at Children’s
Mercy Hospital and the University of Missouri – Kansas City (Bradley Warady, MD) and
Children’s Hospital of Philadelphia (Susan Furth, MD, PhD), Central Biochemistry Laboratory
(George Schwartz, MD) at the University of Rochester Medical Center, and data coordinating
center (Alvaro Muñoz, PhD and Derek Ng, PhD) at the Johns Hopkins Bloomberg School of
Public Health. The CKiD Study is funded by the National Institute of Diabetes and Digestive and
Kidney Diseases, with additional funding from the National Institute of Child Health and Human
Development, and the National Heart, Lung, and Blood Institute (U01-DK-66143, U01-DK-
66174, U24-DK-082194, U24-DK-66116). The authors thank Ankur Patel for assistance in
preparing revisions of this manuscript. The CKID website is located at
https://www.statepi.jhsph.edu/ckid and a list of CKiD collaborators can be found at
https://statepi.jhsph.edu/ckid/site-investigators/.
Author Contributions
Denver Brown: Conceptualization; Data curation; Funding acquisition; Investigation;
Methodology; Supervision; Writing - original draft; Writing - review and editing. Megan Carroll:
Data curation; Formal analysis; Methodology; Software; Validation; Writing - original draft;
Writing - review and editing. Derek Ng: Data curation; Formal analysis; Methodology; Software;
Writing - original draft; Writing - review and editing Rebecca Levy: Methodology; Writing - review
and editing. Larry Greenbaum: Methodology; Writing - original draft; Writing - review and editing.
Frederick Kaskel: Methodology; Writing - original draft; Writing - review and editing. Susan
Furth: Conceptualization; Methodology; Writing - review and editing. Bradley Warady:
Conceptualization; Methodology; Resources; Writing - review and editing. Michal Melamed:
Conceptualization; Methodology; Supervision; Writing - original draft; Writing - review and
8editing. Andrew Dauber: Data curation; Investigation; Methodology; Supervision; Writing -
original draft; Writing - review and editing.
Supplemental Materials
Supplemental Table 1. Distribution of diagnoses within non-glomerular and glomerular
participants
Supplemental Table 2. Unadjusted, partially adjusted, and fully adjusted models of height z-
score on serum bicarbonate, using a categorical predictor AMONG NON-rGH users. Missing
data were imputed for covariates in the partially and fully adjusted models.
Supplemental Table 3. Unadjusted, minimally adjusted, and fully adjusted models of height z-
score on previous visits’ serum bicarbonate. Generalized estimating equations used to account
for repeated measures within an individual.
Supplemental Table 4a (among children < 13 with adjustment of glomerular/non-glomerular
diagnosis as a covariate and eGFR. Missing data were imputed for covariates in the partially
and fully adjusted models.
Supplemental Table 4b (among children < 13 with adjustment of glomerular/non-glomerular
diagnosis as a covariate and measured GFR. Missing data were imputed for covariates in the
partially and fully adjusted models.
Supplemental Table 5. List of principal site investigators of the Chronic Kidney Disease in
Children (CKiD) cohort study.
9References
1. Wong, C.S., et al., Anthropometric measures and risk of death in children with end-stage renal
disease. Am J Kidney Dis, 2000. 36(4): p. 811-9.
2. Gerson, A.C., et al., Health-related quality of life of children with mild to moderate chronic kidney
disease. Pediatrics, 2010. 125(2): p. e349-57.
3. Al-Uzri, A., et al., The impact of short stature on health-related quality of life in children with
chronic kidney disease. J Pediatr, 2013. 163(3): p. 736-41.e1.
4. NAPRTCS: 2008 Annual Report. 2008: Rockville, MD.
5. Seikaly, M.G., et al., Chronic renal insufficiency in children: the 2001 Annual Report of the
NAPRTCS. Pediatr Nephrol, 2003. 18(8): p. 796-804.
6. Furth, S.L., et al., Adverse clinical outcomes associated with short stature at dialysis initiation: a
report of the North American Pediatric Renal Transplant Cooperative Study. Pediatrics, 2002.
109(5): p. 909-13.
7. Rodig, N.M., et al., Growth in children with chronic kidney disease: a report from the Chronic
Kidney Disease in Children Study. Pediatr Nephrol, 2014. 29(10): p. 1987-95.
8. Harambat, J., et al., Metabolic acidosis is common and associates with disease progression in
children with chronic kidney disease. Kidney Int, 2017.
9. McSherry, E. and R.C. Morris, Jr., Attainment and maintenance of normal stature with alkali
therapy in infants and children with classic renal tubular acidosis. J Clin Invest, 1978. 61(2): p.
509-27.
10. Caldas, A., et al., Primary distal tubular acidosis in childhood: clinical study and long-term follow-
up of 28 patients. J Pediatr, 1992. 121(2): p. 233-41.
11. Sharma, A.P., et al., Bicarbonate therapy improves growth in children with incomplete distal
renal tubular acidosis. Pediatr Nephrol, 2009. 24(8): p. 1509-16.
12. Chan, W., K.C. Valerie, and J.C. Chan, Expression of insulin-like growth factor-1 in uremic rats:
growth hormone resistance and nutritional intake. Kidney Int, 1993. 43(4): p. 790-5.
13. Challa, A., et al., Metabolic acidosis inhibits growth hormone secretion in rats: mechanism of
growth retardation. Am J Physiol, 1993. 265(4 Pt 1): p. E547-53.
14. Brüngger, M., H.N. Hulter, and R. Krapf, Effect of chronic metabolic acidosis on the growth
hormone/IGF-1 endocrine axis: new cause of growth hormone insensitivity in humans. Kidney
Int, 1997. 51(1): p. 216-21.
15. Furth, S.L., et al., Metabolic abnormalities, cardiovascular disease risk factors, and GFR decline in
children with chronic kidney disease. Clin J Am Soc Nephrol, 2011. 6(9): p. 2132-40.
16. Brown, D.D., et al., Low Serum Bicarbonate and CKD Progression in Children. Clin J Am Soc
Nephrol, 2020. 15(6): p. 755-765.
17. Andrade, O.V., F.O. Ihara, and E.J. Troster, Metabolic acidosis in childhood: why, when and how
to treat. J Pediatr (Rio J), 2007. 83(2 Suppl): p. S11-21.
18. Furth, S.L., et al., Design and methods of the Chronic Kidney Disease in Children (CKiD)
prospective cohort study. Clin J Am Soc Nephrol, 2006. 1(5): p. 1006-15.
19. KDOQI, Clinical Practice Guidelines for Bone Metabolism and Disease in Children with Chronic
Kidney Disease. American journal of kidney diseases : the official journal of the National Kidney
Foundation., 2005. 46: p. S1–S122.
20. Kuczmarski, R.J., et al., 2000 CDC Growth Charts for the United States: methods and
development. Vital Health Stat 11, 2002(246): p. 1-190.
21. Seikaly, M.G., et al., Stature in children with chronic kidney disease: analysis of NAPRTCS
database. Pediatr Nephrol, 2006. 21(6): p. 793-9.
1022. Pierce, C.B., et al., Age- and sex-dependent clinical equations to estimate glomerular filtration
rates in children and young adults with chronic kidney disease. Kidney Int, 2021. 99(4): p. 948-
956.
23. Warady, B.A., et al., Predictors of Rapid Progression of Glomerular and Nonglomerular Kidney
Disease in Children and Adolescents: The Chronic Kidney Disease in Children (CKiD) Cohort. Am J
Kidney Dis, 2015. 65(6): p. 878-88.
24. Franke, D., et al., Patterns of growth after kidney transplantation among children with ESRD. Clin
J Am Soc Nephrol, 2015. 10(1): p. 127-34.
25. Santos, F. and J.C. Chan, Renal tubular acidosis in children. Diagnosis, treatment and prognosis.
Am J Nephrol, 1986. 6(4): p. 289-95.
26. Gadola, L., et al., Calcium citrate ameliorates the progression of chronic renal injury. Kidney Int,
2004. 65(4): p. 1224-30.
27. Tanner, G.A., Potassium citrate/citric acid intake improves renal function in rats with polycystic
kidney disease. J Am Soc Nephrol, 1998. 9(7): p. 1242-8.
28. Mahajan, A., et al., Daily oral sodium bicarbonate preserves glomerular filtration rate by slowing
its decline in early hypertensive nephropathy. Kidney Int, 2010. 78(3): p. 303-9.
29. Wiegand, A., et al., Preservation of kidney function in kidney transplant recipients by alkali
therapy (Preserve-Transplant Study): rationale and study protocol. BMC Nephrol, 2018. 19(1): p.
177.
30. Tangri, N., et al., Metabolic acidosis is associated with increased risk of adverse kidney outcomes
and mortality in patients with non-dialysis dependent chronic kidney disease: an observational
cohort study. BMC Nephrol, 2021. 22(1): p. 185.
31. Djamali, A., et al., Metabolic Acidosis 1 Year Following Kidney Transplantation and Subsequent
Cardiovascular Events and Mortality: An Observational Cohort Study. Am J Kidney Dis, 2019.
32. Suzuki, K., et al., Incidence of latent mesangial IgA deposition in renal allograft donors in Japan.
Kidney Int, 2003. 63(6): p. 2286-94.
33. Bhattacharjee, P., et al., The clinicopathologic manifestations of Plasmodium vivax malaria in
children: a growing menace. J Clin Diagn Res, 2013. 7(5): p. 861-7.
34. Lv, J., et al., Corticosteroid therapy in IgA nephropathy. J Am Soc Nephrol, 2012. 23(6): p. 1108-
16.
11Table 1a. Descriptive characteristics of study population with a non-glomerular CKD diagnosis overall
and by bicarbonate levels at baseline. % (N) or median [IQR]
Serum bicarbonate (mEq/L)
Overall >22 19-22 ≤18
Characteristics N = 808 N = 448 N = 274 N = 86 p-value
Demographics
Age 8.09 [4.38, 12.72] 8.69 [4.79, 13.2] 6.87 [3.76, 10.86] 9.13 [4.23, 14.07]Table 1b. Descriptive characteristics of study population with a glomerular CKD diagnosis overall and by
bicarbonate levels at baseline. % (N) or median [IQR]
Serum bicarbonate (mEq/L)
Overall >22 19-22 ≤18 p-
Characteristics N = 274 N = 177 N = 77 N = 20 value
Demographics
Age 14.2 [10.8, 15.8] 14.4 [11.9, 15.9] 12.1 [8.7, 14.9] 15.0 [12.1, 16.0] 0.001
Male sex 53% (146) 51% (91) 57% (44) 55% (11) 0.693
RaceTable 2a. Unadjusted, partially adjusted, and fully adjusted models of height z-score on serum
bicarbonate, using a categorical predictor. Missing data were imputed for covariates in the partially and
fully adjusted models. Bold indicates p < 0.05.
Serum Bicarbonate N Unadjusted Partially Adjusted Fully Adjusted
(mEq/L) Mean (95% CI) Mean1 (95% CI) Mean2 (95% CI)
Non-Glomerular 3239
Diagnosis
>22 Reference Reference Reference
19-22 -0.27 (-0.40, -0.14) -0.17 (-0.28, -0.05) -0.17 (-0.28, -0.05)
≤18 -0.58 (-0.79, -0.38) -0.38 (-0.57, -0.19) -0.39 (-0.58, -0.20)
Glomerular
853
Diagnosis
>22 Reference Reference Reference
19-22 -0.28 (-0.52, -0.04) -0.07 (-0.25, 0.11) -0.07 (-0.25, 0.10)
≤18 -0.38 (-0.92, 0.16) 0.16 (-0.31, 0.62) 0.14 (-0.33, 0.61)
1 Adjusted for age, sex, abnormal birth history, mid-parental height, and previous levels of eGFR and UP/C
2 Adjusted for age, sex, abnormal birth history, mid-parental height, and previous levels of eGFR, UP/C, calcium, phosphate,
iPTH and CKD duration in years
Table 2b. Unadjusted, partially adjusted, and fully adjusted models of height z-score on serum
bicarbonate, using a categorical predictor restricted to person-visits with directly measured GFR only.
Missing data were imputed for covariates in the partially and fully adjusted models. Bold indicates p <
0.05.
Serum Bicarbonate N Unadjusted Partially Adjusted Fully Adjusted
(mEq/L) Mean (95% CI) Mean1 (95% CI) Mean2 (95% CI)
Non-Glomerular 1413
Diagnosis
>22 Reference Reference Reference
19-22 -0.32 (-0.47, -0.16) -0.19 (-0.34, -0.05) -0.20 (-0.34, -0.05)
≤18 -0.68 (-0.94, -0.42) - 0.53 (-0.76, -0.30) -0.53 (-0.77, -0.29)
Glomerular
403
Diagnosis
>22 Reference Reference Reference
19-22 -0.43 (-0.78, -0.08) - 0.07 (-0.38, 0.23) -0.03 (-0.31, 0.26)
≤18 -0.33 (-0.91, 0.25) 0.16 (-0.35, 0.66) 0.16 (-0.37, 0.69)
1 Adjusted for age, sex, abnormal birth history, mid-parental height, and previous levels of GFR and UP/C
2 Adjusted for age, sex, abnormal birth history, mid-parental height, and previous levels of GFR, UP/C, calcium and phosphate,
iPTH and CKD duration in years
15Table 3a. Unadjusted, partially adjusted, and fully adjusted models of height z-score on serum
bicarbonate, stratified by eGFR < and ≥ 45 ml/min/1.73m2, using a categorical predictor. Missing data
were imputed for covariates in the partially and fully adjusted models. Bold indicates p < 0.05.
Serum Bicarbonate N Unadjusted Partially Adjusted Fully Adjusted
(mEq/L) Mean (95% CI) Mean1 (95% CI) Mean2 (95% CI)
Non-Glomerular 3239
eGFR < 45 eGFR ≥ 45 eGFR < 45 eGFR ≥ 45 eGFR < 45 eGFR ≥ 45
Diagnosis
>22 mEq/L 2014 Ref Ref Ref Ref Ref Ref
970 -0.34 -0.11 -0.29 -0.03 -0.28 -0.03
19-22 mEq/L
(-0.50, -0.18) (-0.29, 0.08) (-0.43, -0.14) (-0.20, 0.14) (-0.43, -0.14) (-0.20, 0.13)
255 -0.63 -0.31 -0.52 -0.21 -0.51 -0.25
≤18 mEq/L
(-0.85, -0.40) (-0.63, 0.01) (-0.74, -0.30) (-0.51, 0.09) (-0.73, -0.28) (-0.55, 0.06)
Glomerular 853
Diagnosis3
>22 mEq/L 609 Ref Ref Ref Ref Ref Ref
244
-0.12 -0.29 0.07 -0.12 0.10 -0.12
≤22 mEq/L
(-0.42, 0.18) (-0.60, 0.02) (-0.20, 0.34) (-0.35, 0.11) (-0.17, 0.36) (-0.35, 0.11)
1 Adjusted for age, sex, abnormal birth history, mid-parental height, and previous levels of eGFR and UP/C
2 Adjusted for age, sex, abnormal birth history, mid-parental height, and previous levels of eGFR, UP/C, calcium, phosphate,
iPTH and CKD duration in years
Table 3b. Unadjusted, partially adjusted, and fully adjusted models of height z-score on serum
bicarbonate, stratified by measured GFR < and ≥ 45 ml/min|1.73m2, using a categorical predictor.
Missing data were imputed for covariates in the partially and fully adjusted models. Bold indicates p <
0.05.
N Unadjusted Partially Adjusted Fully Adjusted
Serum Bicarbonate
Mean (95% CI) Mean1 (95% CI) Mean2 (95% CI)
Non-Glomerular 1413
iGFR < 45 iGFR ≥ 45 iGFR < 45 iGFR ≥ 45 iGFR < 45 iGFR ≥ 45
Diagnosis
>22 mEq/L 904 Ref Ref Ref Ref Ref Ref
407 -0.35 -0.17 -0.29 -0.04 -0.29 -0.03
19-22 mEq/L
(-0.55, -0.14) (-0.41, 0.07) (-0.48, -0.10) (-0.25, 0.18) (-0.48, -0.09) (-0.24, 0.18)
102 -0.62 -0.68 -0.54 -0.61 0.52 -0.66
≤18 mEq/L
(-0.93, -0.31) (-1.09, -0.28) (-0.81, -0.26) (-0.99, -0.23) (-0.81, -0.24) (-1.03, -0.28)
Glomerular 403
Diagnosis3
>22 mEq/L 293 Ref Ref Ref Ref Ref Ref
110
-0.08 -0.45 0.14 -0.21 0.06 -0.16
≤22 mEq/L
(-0.46, 0.29) (-0.96, 0.07) (-0.22, 0.50) (-0.65, 0.22) (-0.31, 0.42) (-0.55, 0.23)
1 Adjusted for age, sex, abnormal birth history, mid-parental height, and previous levels of GFR and UP/C
2 Adjusted for age, sex, abnormal birth history, mid-parental height, and previous levels of GFR, UP/C, calcium, phosphate, iPTH
and CKD duration in years.
3 For those with glomerular diagnoses, serum bicarbonate was dichotomized at 22mEq/L because there were n= 126 and 277
person-visits for those less than 45 ml/min|1.73m2 and greater than 45 ml/min|1.73m2, respectively
16Table 4a. Unadjusted and adjusted models of height z-score on previous visits serum bicarbonate
stratified by discontinued and persistent alkali therapy use based on two annual study visits. Generalized
estimating equations were used to account for repeated measures within an individual. Missing data were
imputed for covariates in the partially and fully adjusted models. Analysis used estimated GFR. Bold
indicates p < 0.05.
N Unadjusted Adjusted
Mean Difference (95% CI) Mean Difference a (95% CI)
Previous serum bicarbonate, per 1-unit
increase
Discontinued alkali therapy use over 1
86 +0.017 (-0.03, +0.065) +0.025 (-0.011, +0.062)
year
Persistent alkali therapy use over 1 year 653 +0.056 (+0.023, +0.089) +0.04 (+0.008, +0.073)
aAdjusted for age, sex, abnormal birth history, mid-parental height, and previous levels of eGFR, UP/C, calcium, and phosphate,
iPTH and CKD duration in years
Table 4b. Unadjusted and adjusted models of height z-score on previous visits serum bicarbonate
stratified by discontinued and persistent alkali therapy use based on two annual study visits. Generalized
estimating equations were used to account for repeated measures within an individual. Missing data were
imputed for covariates in the partially and fully adjusted models. Analysis used measured GFR. Bold
indicates p < 0.05.
N Unadjusted Adjusted
Mean Difference (95% CI) Mean Difference a (95% CI)
Previous serum bicarbonate, per 1-unit
increase
Discontinued alkali therapy use over 1
15 +0.042 (-0.171, +0.254) +0.078 (-0.035, +0.191)
year
Persistent alkali therapy use over 1 year 130 +0.061 (-0.005, +0.126) +0.043 (-0.013, +0.099)
aAdjusted for age, sex, abnormal birth history, mid-parental height, and previous levels of GFR, UP/C, calcium, and phosphate,
iPTH and CKD duration in years
17Figure 1
Figure 1. Distribution of height z-score by previous visit bicarbonate levels among person-visits
contributed by participants with (A) non-glomerular and (B) glomerular CKD diagnoses.Supplemental Materials: Table of Contents Supplemental Table 1. Distribution of diagnoses within non-glomerular and glomerular participants Supplemental Table 2. Unadjusted, partially adjusted, and fully adjusted models of height z-score on serum bicarbonate, using a categorical predictor AMONG NON-rGH users. Missing data were imputed for covariates in the partially and fully adjusted models. Supplemental Table 3. Unadjusted, minimally adjusted, and fully adjusted models of height z-score on previous visits’ serum bicarbonate. Generalized estimating equations used to account for repeated measures within an individual. Supplemental Table 4a (among children
Supplemental Table 1. Distribution of diagnoses within non-glomerular and glomerular participants
Non-Glomerular diagnoses Glomerular diagnoses
Primary diagnosis N % Primary Diagnosis N %
Aplastic/hypoplastic/dysplastic Focal segmental
197 24.5 79 28.8
kidneys glomerulosclerosis
Obstructive uropathy 192 23.9 Hemolytic uremic syndrome 52 19.0
Systemic immunological
Reflux nephropathy 140 17.4 37 13.5
disease (including SLE)
Congenital Urologic Disease
52 6.5 Chronic glomerulonephritis 22 8.0
(Bilateral Hydronephrosis)
Non-Glomerular Other 50 6.2 Familial nephritis (Alport's) 19 6.9
Polycystic kidney disease
38 4.7 IgA Nephropathy (Berger's) 17 6.2
(Autosomal recessive)
Membranoproliferative
Renal infarct 27 3.4 12 4.4
glomerulonephritis type I
Cystinosis 19 2.4 Henoch schonlein nephritis 9 3.3
Pyelonephritis/Interstitial
15 1.9 Other glomerular diagnosis 8 2.9
nephritis
Idiopathic cresentic
Perinatal Asphyxia 14 1.7 7 2.6
glomerulonephritis
Medullary cystic
disease/Juvenile 12 1.5 Membranous nephropathy 4 1.5
nephronophthisis
Syndrome of agenesis of
11 1.4 Congenital nephrotic syndrome 4 1.5
abdominal musculature
Membranoproliferative
Vactrel or Vater Syndrome 9 1.2 3 1.1
glomerulonephritis type II
Wilms' tumor 8 1.0 Sickle cell nephropathy 1 0.4
Branchio-oto-Renal
7 0.9
Disease/Syndrome
Polycystic kidney disease
7 0.9
(Autosomal dominant)
Methylmalonic Acidemia 5 0.6
Oxalosis 2 0.2Supplemental Table 2. Unadjusted, partially adjusted, and fully adjusted models of height z-score on
serum bicarbonate, using a categorical predictor AMONG NON-rGH users. Missing data were imputed
for covariates in the partially and fully adjusted models.
Serum Bicarbonate N Unadjusted Partially Adjusted Fully Adjusted
(mEq/L) Mean (95% CI) Mean1 (95% CI) Mean2 (95% CI)
Non-Glomerular 2635
Diagnosis
>22 Reference Reference Reference
19-22 -0.30 (-0.45, -0.15) -0.22 (-0.34, -0.09) -0.21 (-0.33, -0.08)
≤18 -0.53 (-0.75, -0.32) -0.34 (-0.53, -0.15) -0.31 (-0.51, -0.12)
Glomerular
800
Diagnosis3
>22 Reference Reference Reference
≤ 22 -0.21 (-0.45, 0.03) -0.03 (-0.22, 0.16) -0.02 (-0.20, 0.17)
1 Adjusted for age, sex, abnormal birth history, mid-parental height, and previous levels of eGFR and UP/C
2 Adjusted for age, sex, abnormal birth history, mid-parental height, and previous levels of eGFR, UP/C, calcium, phosphate,
iPTH and CKD duration in years.
3 For those with glomerular diagnoses, serum bicarbonate was dichotomized at 22mEq/L because there were n= 225 and 575
person-visits for those less than 45 ml/min|1.73m2 and greater than 45 ml/min|1.73m2, respectively
Supplemental Table 3. Unadjusted, minimally adjusted, and fully adjusted models of height z-score on
previous visits’ serum bicarbonate. Generalized estimating equations used to account for repeated
measures within an individual.
N Unadjusted Partially Adjusted Fully Adjusted
Mean (95% CI) Mean1 (95% CI) Mean2 (95% CI)
Previous Serum Bicarbonate, per 1 mEq/L
increase
-0.003 -0.001 0.01
Non-glomerular diagnosis 3239
(-0.03, 0.02) (-0.02, 0.02) (-0.01, 0.03)
-0.01 0.02 0.03
Glomerular diagnosis 853
(-0.07, 0.04) (-0.04, 0.08) (-0.03, 0.09)
1 Adjusted for age, sex, abnormal birth history, mid-parental height, and previous levels of eGFR and UP/C
2 Adjusted for age, sex, abnormal birth history, mid-parental height, and previous levels of eGFR, UP/C, calcium, phosphate,
iPTH and CKD duration in yearsSupplemental Table 4a (among children 22 1150 Reference Reference Reference
19-22 606 -0.21 (-0.35, -0.07) -0.09 (-0.21, 0.04) -0.09 (-0.21, 0.03)
≤18 139 -0.49 (-0.75, -0.22) -0.25 (-0.49, 0.00) -0.25 (-0.50, -0.01)
1 Adjusted for diagnosis, age, sex, abnormal birth history, mid-parental height, and previous levels of eGFR and UP/C
2 Adjusted for diagnosis, age, sex, abnormal birth history, mid-parental height, and previous levels of eGFR, UP/C, calcium,
phosphate, iPTH and CKD duration in years.
Supplemental Table 4b (among children 22 544 Reference Reference Reference
19-22 261 -0.28 (-0.47, -0.09) -0.18 (-0.36, 0.00) -0.19 (-0.36, -0.01)
≤18 61 -0.53 (-0.87, -0.19) -0.37 (-0.67, -0.07) -0.39 (-0.69, -0.09)
1 Adjusted for diagnosis, age, sex, abnormal birth history, mid-parental height, and previous levels of GFR and UP/C
2 Adjusted for diagnosis, age, sex, abnormal birth history, mid-parental height, and previous levels of GFR, UP/C, calcium,
phosphate, iPTH and CKD duration in years.Supplemental Table 5. List of principal site investigators of the Chronic Kidney Disease in Children
(CKiD) cohort study.
Study Investigator(s) Institution City State/Province
University of Alabama at
Sahar Fathallah-Shaykh, MD Birmingham (Children’s of Birmingham AL
Alabama)
Anjali Nayak, MD; Martin
Phoenix Children’s Hospital Phoenix AZ
Turman, MD
Tom Blydt-Hansen, MD, British Columbia Children’s
Vancouver British Columbia, Canada
FRCPC Hospital
Cynthia Wong, MD; Steve Stanford University Medical
Palo Alto CA
Alexander, MD Center
University of California –
Ora Yadin, MD Los Angeles CA
Los Angeles (UCLA)
Elizabeth Ingulli, MD; University of California –
San Diego CA
Robert Mak, MD, PhD San Diego (UCSD)
Cheryl Sanchez-Kazi, MD Loma Linda University Loma Linda CA
Children’s National Medical
Asha Moudgil, MD Washington DC
Center
Nemours/Alfred l. duPont
Caroline Gluck, MD Wilmington DE
Hospital for Children
Carolyn Abitbol, MD;
Marissa DeFrietas, MD;
Chryso Katsoufis, MD; University of Miami Miami FL
Wacharee Seeherunvong,
MD
Children’s Healthcare of
Larry Greenbaum, MD, PhD Atlanta GA
Atlanta / Emory University
Lyndsay Harshman, MD University of Iowa Iowa City IA
Ann & Robert H. Lurie
Craig Langman, MD Children’s Hospital of Chicago IL
Chicago
University of Illinois at
Sonia Krishnan, MD Chicago IL
Chicago
Riley Hospital for Children
Amy Wilson, MD Indianapolis IN
at Indiana University Health
Stefan Kiessling, MD;
University of Kentucky Lexington KY
Margaret Murphy, PhD
Siddharth Shah, MD, Janice University of Louisville
Sullivan, MD; Sushil Gupta, (Novak Center for Louisville KY
MD Children’s Health)
Samir El-Dahr, MD; Stacy
Tulane University New Orleans LA
Drury, MD
Nancy Rodig, MD Boston Children’s Hospital Boston MA
University of Manitoba
Allison Dart, MD MSc, (Children’s Hospital
Winnipeg Manitoba, Canada
FRCPC Research Institute of
Manitoba)
Johns Hopkins University
Meredith Atkinson, MD (Johns Hopkins Children’s Baltimore MD
Center)
Arlene Gerson, PhD Baltimore MD
Children’s Hospital of
Tej Matoo, MD Michigan / Wayne State Detroit MI
University
Zubin Modi, MD University of Michigan Ann Arbor MI
Spectrum Health Hospitals /
Alejandro Quiroga, MD Helen DeVos Children's Grand Rapids MI
HospitalChildren’s Mercy Hospital -
Bradley Warady, MD Kansas City MO
Kansas City
Rebecca Johnson, PhD Children's Mercy Hospital Kansas City MO
Washington University in St.
Vikas Dharnidharka, MD Louis (St. Louis Children’s St. Louis MO
Hospital)
Stephen Hooper, PhD University of North Carolina Chapel Hill NC
Susan Massengill, MD Levine Children’s Hospital Charlottesville NC
Liliana Gomez-Mendez, MD East Carolina University Greenville NC
Dartmouth-Hitchcock
Matthew Hand, DO Lebanon NH
Medical Center
Rutgers-Robert Wood
Joann Carlson, MD New Brunswick NJ
Johnson Medical School
Hanan Tawadrous, MD; St. Joseph’s University
Paterson NJ
Roberto Jodorkovsky, MD Medical Center
University of New Mexico
Craig Wong, MD, MPH Albuquerque NM
Health Sciences Center
Albert Einstein College of
Frederick Kaskel, MD, PhD;
Medicine/Montefiore Bronx NY
Shlomo Shinnar, MD, PhD
Medical Center
Icahn School of Medicine at
Jeffrey Saland, MD New York NY
Mount Sinai
Marc Lande, MD; George University of Rochester
Rochester NY
Schwartz, MD Medical Center
State University of New
Anil Mongia, MD York, Downstate Medical Brooklyn NY
Center
Donna Claes, MD; Mark Cincinnati Children’s
Cincinnati OH
Mitsnefes, MD Hospital Medical Center
Case Western Reserve
Katherine Dell, MD University/Cleveland Clinic Cleveland OH
Children’s
Nationwide Children’s
Hiren Patel, MD Columbus OH
Hospital
Oklahoma University Health
Pascale Lane, MD Oklahoma City OK
Sciences Center
Hospital for Sick Children
Rulan Parekh, MD Toronto Ontario, Canada
(Sick Kids)
Amira Al-Uzri, MD, MCR; Oregon Health and Science
Portland OR
Kelsey Richardson, MD University
Susan Furth, MD, PhD; Children’s Hospital of
Philadelphia PA
Larry Copelovitch, MD Philadelphia
University of California –
Elaine Ku, MD, MAS San Francisco SF
San Francisco (UCSF)
University of Texas Health
Joshua Samuels, MD Houston TX
Science Center at Houston
Baylor College of Medicine
Poyyapakkam Srivaths, MD Houston TX
(Texas Children’s Hospital)
Samhar Al-Akash, MD Driscoll Children’s Hospital Corpus Christi TX
INOVA Children’s Hospital
Patricia Seo-Mayer, MD / Pediatric Specialists of Fairfax VA
Virginia
Victoria Norwood, MD University of Virginia Charlottesville VA
Joseph Flynn, MD Seattle Children’s Hospital Seattle WA
Medical College of
Cynthia Pan, MD Milwaukee WI
Wisconsin
Sharon Bartosh, MD University of Wisconsin Madison WIYou can also read