ARE MD-PHD PROGRAMS MEETING THEIR GOALS? AN ANALYSIS OF CAREER CHOICES MADE BY GRADUATES OF 24 MD-PHD PROGRAMS
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Career Choice
Are MD–PhD Programs Meeting Their Goals?
An Analysis of Career Choices Made by
Graduates of 24 MD–PhD Programs
Lawrence F. Brass, MD, PhD, Myles H. Akabas, MD, PhD, Linda D. Burnley,
David M. Engman, MD, PhD, Clayton A. Wiley, MD, PhD, and Olaf S. Andersen, MD
Abstract
Purpose Results appointments in nonclinical departments,
MD–PhD training programs provide an The average program enrolled 90 trainees, increasing time to graduation, and
integrated approach for training required 8.0 years to complete, and had an expanding residency choices that include
physician–scientists. The goal of this attrition rate of 10%. Nearly all (95%) of disciplines historically associated with
study was to characterize the career path those who graduated entered residencies. clinical practice rather than research.
taken by MD–PhD program alumni Most (81%) were employed in academia,
during the past 40 years and identify research institutes, or industry; 16% were Conclusions
trends that affect their success. in private practice. Of those in academia, Most MD–PhD program graduates follow
82% were doing research and at least career paths generally consistent with their
61% had identifiable research funding. training as physician–scientists. However,
Method Whereas two-thirds devoted more than the range of their professional options is
In 2007 and 2008, 24 programs 50% effort to research, only 39% devoted broad. Further thought should be given to
enrolling 43% of current trainees and more than 75% effort. Many with designing their training to anticipate their
representing half of the National laboratory-based PhDs reported doing career choices and maximize their
Institutes of Health-funded MD–PhD clinical, as well as basic and translational, likelihood of success as investigators.
training programs submitted anonymous research. Emerging trends include
data on 5,969 current and former decreasing numbers of graduates who
trainees. forego residencies or hold primary doi: 10.1097/ACM.0b013e3181d3ca17
The concept of the MD–PhD program academic medical centers, universities, Sciences (NIGMS)4 and competitively
as an integrated approach to training and research institutes such as the awarded individual fellowships that are
physician–scientists dates back to the National Institutes of Health (NIH). It offered by some of the NIH institutes. In
late 1950s. Although a long tradition was also expected that links would exist addition to assisting with program costs,
exists of physicians becoming between program graduates’ medical NIH funding has helped standardize
investigators as well as clinicians, MD– training, clinical activities, and research training approaches and provides a
PhD programs were established with the interests and that each of these would regular source of external review as
realization that the standard four-year inform the others in ways that could not programs compete to obtain and
medical school curriculum is neither be experienced by scientists who were not continue their MSTP status.
intended nor sufficient to train trained as physicians.1
physician–investigators who are as Because MD–PhD programs commonly
proficient in the lab as they are in the MD–PhD programs are not the only provide full tuition and stipend support
clinic. As the term is now commonly available approach for training future to their trainees, they collectively
applied, a physician–scientist or, more physician–scientists, but they have, in many represent a large investment of
broadly, a physician–investigator, is a respects, become the most visible.2–4 In an institutional, federal, and societal
physician who is committed to the quest MD–PhD curriculum, students complete resources. Therefore, it is reasonable to
for new knowledge and new approaches the requirements for both the MD and ask whether they are meeting their goals.
to disease diagnosis, treatment, and the PhD, usually by starting with the first This was last done in the 1990s.4 –6 Recent
prevention, and who devotes far more of two years of medical education and then debates at national conferences and in the
his or her time to these activities than to focusing on graduate school before literature about the best ways and times
routine clinical care. It was expected from returning to complete the medical degree. to train physicians to be investigators7 led
the start that most graduates of MD–PhD Although initially available at only a few us to believe it is time to evaluate MD–
programs would be employed by universities, MD–PhD programs are now PhD programs again. To our knowledge,
offered at most U.S. and a few Canadian the present study, which analyzes the data
medical schools. These programs vary provided to us by 24 MD–PhD programs
Please see the end of this article for information considerably in size and resources. Since in 2007 and early 2008, represents the
about the authors.
1964, NIH support has been available most exhaustive look to date at the career
Correspondence should be addressed to Dr. Brass, through institutional Medical Scientist paths of MD–PhD program alumni. The
University of Pennsylvania, Room 915 BRB-II, 421
Curie Blvd., Philadelphia, PA 19104; telephone: (215) Training Program (MSTP) grants from participating programs collectively enroll
573-4669; e-mail: brass@mail.med.upenn.edu. the National Institute of General Medical approximately 40% of the estimated
Academic Medicine, doi: 10.1097/ACM.0b013e3181d3ca17 1Career Choice
5,000 MD–PhD students currently in required to track their graduates and Program characteristics and trainees
training and together represent nearly report on their activities every five years. The 24 programs that participated in the
half of the 42 programs that were In other words, they were more likely survey ranged in size in AY2008 from 31
receiving NIGMS MSTP grants at the than other programs to have the to 184 trainees; the average was 90
time the data were collected. The data necessary data on hand. trainees. Thirty-seven percent of trainees
that were provided allow us to address in AY2008 were women, but this
issues raised in recent editorials calling Each program submitted basic proportion varied considerably (range
for an evaluation of MD–PhD training information, including the number of 20%–60%). The unweighted average
programs,7,8 as well as concerns that trainees in AY2008, the number of time to complete both degrees for
physician–investigators are a vanishing students entering the program in graduates in AY1998 –2007 was 8.0 ⫾ 0.4
species.1 AY1998 –2007, the number of students years (mean ⫾ 1 SD; 7.8 years when
resigning without one or both degrees weighted by program size, range 7.2–8.5
from AY1998 to AY2007, the percentage years). On average, 10% of the 2,562
Method of trainees in AY2008 who were women, students who enrolled from AY1998 to
We sent a request for data to the directors the average number of years to complete AY2007 withdrew without completing
and administrators of 25 MD–PhD both degrees for graduates in AY1998 – both degrees (range 3%–34%, 1 SD ⫽
programs, which we selected from among 2007, and the discipline in which the PhD 7%). We found no relationship between
participants at the 2007 national was awarded. program size and either the time to
conference of MD–PhD programs. We degree or the attrition rate from the same
tried to achieve as much diversity as Program directors and administrators
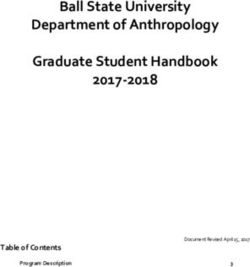
program (Figures 1A and 1B). Although
possible in program size and location. also provided information about alumni,
we were not provided information about
This was not a prospective study; rather, including all graduates from program
students’ reasons for withdrawing, our
we asked the program leaders to provide inception when possible. Program leaders
personal experience as program directors
as much data as possible from the obtained this information from a
and administrators suggests that most of
inception of their program through the combination of alumni questionnaires,
those who withdraw from MD–PhD
end of academic year (AY) 2007 (the 12 alumni Web sites, and searches of public
programs complete medical school. Fewer
months ending in June 2007). Current databases such as the NIH Computer
complete graduate school alone or drop out
students were defined as those enrolled at Retrieval of Information on Scientific
completely. Despite a recent report that
the time that the survey was completed, Projects database. The identities of
women are less likely than men to complete
which was during AY2008. Twenty-four individual trainees and alumni were not
MD–PhD programs,9 we found no
programs agreed to participate*; one available to us, and therefore we were not
relationship between the attrition rate from
program was unable to comply within able to obtain additional primary data
individual programs and the percentage of
the designated time frame. Twenty of the ourselves.
trainees enrolled in the programs who were
participating programs were among the women (Figure 1C).
42 programs receiving NIGMS MSTP Statistical analysis
grants. Our decision to overrepresent We calculated values in Figure 1 for r2, Information on PhD disciplines was
NIGMS-funded programs arose in part the square of the Pearson correlation provided for 1,957 trainees enrolled in
because they tend to be the larger coefficient, using functions built into AY2008, including 306 first- and second-
programs and in part because they are Microsoft Excel 2008 (Microsoft year students who had not yet declared a
Corporation, Redmond, Washington). discipline (a common practice in many of
the programs). Of the 1,651 students who
* The 24 programs that participated are located at
the Albert Einstein College of Medicine of Yeshiva Results had declared a discipline, 1,422 (86%)
University; Baylor College of Medicine; Case Western were enrolled in PhD programs within
Reserve University School of Medicine; Emory Twenty-four MD–PhD programs the broad arc of biomedical disciplines.
University School of Medicine; Harvard Medical provided information about 5,969 Another 151 (9%) were in engineering.
School; Johns Hopkins University School of Medicine; individuals, including 2,023 current
Medical College of Wisconsin; Northwestern The others were working in diverse
University Feinberg School of Medicine; University of
trainees, 1,143 recent graduates who were disciplines including health policy,
California, San Diego, School of Medicine; University still in residencies or postdoctoral epidemiology, public health,
of California, San Francisco, School of Medicine; fellowships, and 2,803 older alumni who
University of Colorado Denver School of Medicine;
anthropology, sociology, chemistry,
University of Iowa Roy J. and Lucille A. Carver
had completed all phases of postgraduate mathematics, philosophy, marine
College of Medicine; University of Maryland School training. This represents 43% of the 4720 biology, population health, psychology,
of Medicine; University of Medicine and Dentistry of trainees enrolled in 2008 (www.aamc.org/ and the history and sociology of science.
New Jersey–Robert Wood Johnson Medical School; data/facts/enrollmentgraduate/start.htm)
University of Michigan Medical School; University
of Pennsylvania School of Medicine; University of and may represent a similar proportion
Pittsburgh School of Medicine; University of of alumni, although the total number of Positions of program alumni
Rochester School of Medicine and Dentistry; graduates is currently unknown. Because Twenty-two programs provided
University of Texas Medical School at Houston;
University of Texas Southwestern Medical Center at
some of the programs were unable to information about then-current or last
Dallas Southwestern Medical School; University of supply answers to all of the survey known positions of 2,413 alumni who
Wisconsin School of Medicine and Public Health; questions, in the following presentation had completed all phases of postgraduate
Vanderbilt University School of Medicine; of the results we have indicated the training. Our results show that 80% of
Washington University in St. Louis School of
Medicine; and Weill Cornell Medical College of number of programs and/or alumni that graduates were employed full-time in
Cornell University. answered each question. academic centers (1,625, or 67%),
2 Academic Medicine, doi: 10.1097/ACM.0b013e3181d3ca17Career Choice
Figure 1 Relationships among MD–PhD program size, time to degree, attrition rates, and the percentage of trainees who are women. (A) The
relationship between program size in academic year (AY) 2008 and time to degree for students entering in AY1998 –2007 using data from 23 MD–
PhD programs (r2 ⫽ 0.018). (B) The relationship between program size in AY2008 and attrition rate over the period from AY1998 to AY2007 using
data from 24 programs (r2 ⫽ 0.034). (C) The proportion of trainees in AY2008 who are women and the attrition rate over the period from 1998 to
2007 using data from 24 programs (r2 ⫽ 0.043).
research institutes such as the NIH (105, to research: Nearly two-thirds (521, or Interestingly, even though the vast
or 4%), or in industry (189, or 8%), each 64%) reported committing at least half of majority of trainees completed their PhD
of which is an outcome consistent with their time to research activities, but only studies in basic biomedical or
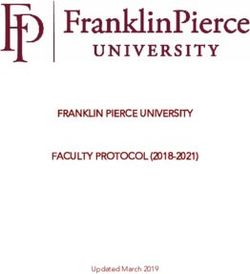
the goals of MD–PhD training. Of the 39% (317) devoted at least three-quarters engineering disciplines, 736 alumni of 14
remainder, 386 (16%) were in private of their time; 19% (155) reported programs gave a variety of answers to a
practice. spending one-quarter or less (Figure 2A). question about the kinds of research that
they do. The choices provided were basic,
Because of concerns about possible translational, clinical, and health services.
ascertainment bias arising from the More than one answer was allowed, and
greater ease in tracking individuals more than one was commonly given.
employed in universities and research
Table 1
Primary Department of MD–PhD Although relatively few program
institutes, we also analyzed the data Program Alumni in Academia* graduates were engaged in health services
focusing solely on the 16 programs able research at the time of the survey, nearly
to provide information on at least 98% MD–PhD program equal numbers reported doing basic,
(n ⫽ 1,927) of their alumni. The alumni
translational, and clinical research
Department No. (%)
numbers we obtained are essentially (Figure 2B).
identical to those derived from the larger Internal medicine 427 (26.3)
...............................................................................................
data set: 68% employed in academia, 4% Pediatrics 203 (12.5) Information about research funding was
...............................................................................................
in research institutes, 8% in industry, and Pathology 192 (11.8) available for 1,120 alumni of 17 programs
...............................................................................................
16% in private practice. Neurology 153 (9.4) who were in academia. Of these, at least
...............................................................................................
Surgery 116 (7.2) 685 (61%) had funding; 154 (14%) said
Information about primary ...............................................................................................
Psychiatry 85 (5.2) that they did not. Of the 281 (25%) for
appointments was provided to us for ............................................................................................... whom no data were available, nearly half
1,621 alumni of 22 programs working in Ophthalmology 61 (3.8)
............................................................................................... (131, or 12%) reported research activities
academia (Table 1). Collectively, internal Anesthesiology 50 (3.1)
............................................................................................... and may have had research support that
medicine, pediatrics, pathology, and Radiology 43 (2.7)
............................................................................................... was not reported, which means that the
neurology accounted for 975 (60%) of Dermatology 43 (2.7) correct proportion of those in academia
the alumni in academia, but most alumni ...............................................................................................
Radiation oncology 24 (1.5) who have research funding may be as
(1,428, or 88%) held primary ...............................................................................................
Obstetrics–gynecology 19 (1.2) much as 73% (61% plus 12%). Note that
appointments in clinical departments. ...............................................................................................
Emergency medicine 7 (0.4) many of the individuals working at
Many also had secondary appointments ............................................................................................... institutes or in industry would also be
in basic science departments. Physical medicine and 5 (0.3)
rehabilitation expected to be doing research, but they
...............................................................................................
Research activities of program alumni Nonclinical 175 (10.8)
were not included in this analysis, so the
............................................................................................... overall percentage of alumni doing
At least 921 (82%) of 1,118 alumni (of 17 Unknown 18 (1.1)
............................................................................................... research may be even higher than
programs) in academia indicated that Total 1,621 (100.0) suggested by our analysis of those in
they were doing research; 141 (13%) * Summary of data provided by 22 MD–PhD programs academia.
reported that they were not, and no data on 1,621 alumni, each of whom had completed
were available for 56 (5%). However, postgraduate training and was employed full-time in
considerable variation existed in the academia at the time that the survey data were Trends over time
collected in 2007–2008. “Surgery” includes all of
amount of time that 814 alumni of 16 the related disciplines. “Nonclinical” includes, but is As noted above, our data show that most
programs were willing or able to devote not limited to, basic science departments. MD–PhD graduates enter academia and
Academic Medicine, doi: 10.1097/ACM.0b013e3181d3ca17 3Career Choice
Figure 2 MD–PhD program graduates’ responses to questions about their recent research activities. (A) How much time do you devote to research?
Responses from 814 alumni of 16 programs who are now in academia. (B) Which kinds of research do you do? Data from 736 alumni of 14
programs; more than one answer was allowed.
have their primary appointment in a For an analysis of changes over time, we There has also been a decline in the
clinical department. The choices that divided the data on program alumni into number of graduates choosing
senior students make for their next step arbitrary cohorts of approximately 10 residencies in internal medicine,
after graduation strongly affect where years based on graduation year. Several neurology, pathology, and pediatrics—
they are likely to end up and may affect trends were evident. The percentage of disciplines that have historically provided
the likelihood that they will choose and graduates choosing to forgo a residency a protected environment for the
succeed in a research-oriented career. in favor of a postdoctoral fellowship, development of physician–scientist
Table 2 summarizes the choices made by which has never been a common choice, careers—and an increase in those
939 recent graduates of 21 programs. Of has declined to 4% to 5% (Figure 3A). selecting dermatology, ophthalmology,
these, 892 (95%) chose to continue their radiation oncology, and surgery (Figure
clinical training. Only 47 (5%) elected to 3B). Others have noted similar trends in
do a postdoctoral fellowship without Table 2 residency choice by all medical school
postgraduate clinical training. Among Residency Choice of Recent MD–PhD graduates.9 –11
those opting for a residency, internal Alumni Still in Training*
medicine was the most popular choice Is choice of residency field predictive of
MD–PhD alumni
(270, or 29%), and, collectively, internal in training
whether MD–PhD program graduates
medicine plus pediatrics, pathology, and Department No. (%) will stay on track to become
neurology accounted for 518 (55%) investigators or enter private practice?
Internal medicine 270 (28.8)
recent graduates. The next most popular ............................................................................................... In Table 3, we present the outcomes
choice was surgery (107, or 11%), a Surgery 107 (11.4) data for 1,862 alumni of 22 programs
...............................................................................................
category that combines all of the surgery- Pediatrics 98 (10.4) who had completed all phases of
...............................................................................................
related disciplines. Pathology 79 (8.4)
...............................................................................................
postgraduate training, asking
Neurology 71 (7.6) retrospectively whether those who
...............................................................................................
Irrespective of their choice of residency, Radiology 61 (6.5) chose clinical training in a particular
...............................................................................................
the vast majority of the alumni included Psychiatry 54 (5.8) field eventually ended up in private
in Table 2 completed their PhD training ............................................................................................... practice. There was considerable
Dermatology 51 (5.4)
in a biomedical laboratory discipline. It ............................................................................................... variability: 8% of pathology graduates
Radiation oncology 32 (3.4)
is interesting to compare the residency ............................................................................................... ended up in private practice compared
choices of the whole group with the Ophthalmology 33 (3.5) with 62% of those who completed
...............................................................................................
choices made by the small number (21) Anesthesiology 19 (2.0) family medicine residencies. Overall,
...............................................................................................
of recent graduates in the survey who did Obstetrics–gynecology 10 (1.1) 14% (165 of 1,220) of graduates who
...............................................................................................
their PhD training in anthropology, Emergency medicine 7 (0.7) chose residencies in internal medicine,
...............................................................................................
demography, English, epidemiology, Postdoctoral training 47 (5.0) neurology, pediatrics, or pathology
health policy, history of science, or public without residency ended up in private practice, compared
...............................................................................................
health. In this group, internal medicine Total 939 (100.0) with 36% (120 of 338) of graduates
was overwhelmingly the most popular who chose dermatology,
* Summary of data provided by 21 MD–PhD programs
choice, with 62% (13) choosing it ophthalmology, or surgery (three of the
on 939 recent graduates who were still in
compared with 29% (Table 2) in the total postgraduate training at the time that the survey four areas noted above as showing an
pool of recent graduates. data were collected in 2007–2008. increase in popularity).
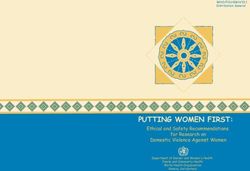
4 Academic Medicine, doi: 10.1097/ACM.0b013e3181d3ca17Career Choice Figure 3 Emerging trends in choices made by MD–PhD program alumni and in the length of time required to graduate from MD–PhD programs. (A) Trends in the choice to do a postdoctoral research fellowship and forego doing a residency. Analysis drawn from data on 3,172 alumni from 23 programs divided into cohorts: 1965–1978 (n ⫽ 144), 1979 –1988 (n ⫽ 551), 1989 –1998 (n ⫽ 1,160), and 1999 –2007 (1,317). (B) Trends in choosing a residency in internal medicine, neurology, pathology, or pediatrics compared with choosing a residency in dermatology, ophthalmology, radiation oncology, or surgery. Analysis drawn from data on 3,172 alumni from 23 programs divided into cohorts as shown in (A). (C) Trends in having a primary appointment in a basic science department. Analysis drawn from data provided by 22 programs divided into cohorts: 1965–1978 (n ⫽ 97), 1979 –1988 (n ⫽ 383), 1989 –1998 (n ⫽ 820), and 1999 –2007 (n ⫽ 306). (D) Trends in choosing a career in academia, a research institute, industry, or private practice. Analysis drawn from data provided by 22 programs divided into cohorts: 1965–1978 (n ⫽ 163), 1979 –1988 (n ⫽ 601), 1989 –1998 (n ⫽ 1,198), and 1999 –2007 (n ⫽ 306). (E) Average time to graduation. Trainees who graduated between 1998 and 2007 from the programs included in the present study required an average of 7.8 years (weighted) to complete both degrees. The data from studies completed in 1980, 1985, and 1995 are from the National Institute of General Medical Sciences.4 Academic Medicine, doi: 10.1097/ACM.0b013e3181d3ca17 5
Career Choice
data. Nonetheless, a number of the
Table 3 results that we obtained are in good
Residency Choice as a Predictor of Eventually Choosing Private Practice* agreement with those from the earlier
studies cited above. Given the size of the
MD–PhD program alumni
sample, our conclusions are likely to be
Total No. in private % in private applicable to MD–PhD programs as a
Department no. practice practice
whole and especially to those programs
Family medicine 13 8 62 with NIGMS MSTP funding, nearly half
.........................................................................................................................................................................................................
Emergency medicine 13 6 46 (20 of 42) of which were included in our
.........................................................................................................................................................................................................
Dermatology 70 31 44 survey. To what extent this heavy reliance
.........................................................................................................................................................................................................
Ophthalmology 101 44 44 on data from programs with MSTP
......................................................................................................................................................................................................... grants has affected the results will remain
Radiology 69 28 41
......................................................................................................................................................................................................... unclear until a fully inclusive MD–PhD
Obstetrics–gynecology 26 8 31
......................................................................................................................................................................................................... program graduates database—such as the
Surgery 167 45 27 one under consideration by the
.........................................................................................................................................................................................................
Anesthesiology 57 13 23 Association of American Medical
.........................................................................................................................................................................................................
Physical medicine and rehabilitation 5 1 20 Colleges (AAMC)—is launched. Until
.........................................................................................................................................................................................................
Internal medicine 578 93 16 then, important questions about
.........................................................................................................................................................................................................
Radiation oncology 27 4 15 comparative outcomes between programs
.........................................................................................................................................................................................................
Neurology 173 23 13
that receive MSTP support and those that
......................................................................................................................................................................................................... do not will have to wait.
Pediatrics 243 32 13
.........................................................................................................................................................................................................
Psychiatry 94 11 12 Nevertheless, we can draw several clear
.........................................................................................................................................................................................................
Pathology 226 17 8 conclusions from the data that are
* Summary of data provided by 22 MD–PhD programs on 1,862 alumni, each of whom had completed available. The first is that most MD–PhD
postgraduate training at the time of this study in 2007–2008. Note that overall, 16% of the alumni who had program graduates (80%) are in careers
completed training were in private practice at the time that the survey data were collected. The columns indicate generally consistent with the goal of MD–
the total number of alumni who completed a residency in each department and the number of those who
subsequently entered private practice. The percentage for each department is the number who entered private PhD training, which is to train physicians
practice divided by the total number who completed a residency in that department. who are committed to the quest for new
knowledge and new approaches to
disease diagnosis, prevention, and
An additional trend that emerged shows a fraction of total medical school treatment. This number is essentially the
steady decline in the proportion of graduates. In 2007, there were only 1,721 same as the 81% of 2000 –2006 MD–PhD
graduates working in academia whose applicants to MD–PhD programs, which graduates who reported in the AAMC
primary appointment is in a basic science represents about 4% of total medical graduation survey that they planned
department (Figure 3C). Overall, school candidates. Of these 1,721 substantial career involvement in
however, the proportion of graduates individuals, 536 matriculated.12 research.9 Approximately 67% are in
choosing careers in academia, research academia, a number that is also
institutes, or industry has changed little As program numbers increased, some remarkably similar to what has been
over almost 50 years (Figure 3D). schools and groups of schools made reported previously.4,6,13,14
efforts to analyze the careers of their
Finally, we asked whether there has been graduates.5,6,13,14 In 1998, NIGMS made A second conclusion is that most (82%)
a change in the time required to complete available some of the outcomes data that of the program graduates at academic
both degrees over the years that MD– had been reported by MSTP-funded medical centers are doing research and
PhD programs have been in existence. As institutions as part of their training grant have funding to support their efforts.
noted above, the unweighted average renewals.4 The results of these studies Presumably at least as many of the
time for graduates in AY1998 –2007 was showed, much as we have found, that the graduates at research institutes such as
nearly 8 years, which represents a majority of MD–PhD graduates are in the NIH are doing research as well. The
substantial increase from the 6.6 years academia. However, none of the previous data, however, also clearly show that the
noted in 19804 (Figure 3E). studies are recent, and none of them range of career choices among MD–PhD
address recent trends. Although an all- program graduates is very broad with
encompassing prospective database about respect to both research interests and
Discussion MD–PhD program graduates would be time spent on research. This diversity is
MD–PhD programs have expanded useful, none currently exists. not currently reflected in the curriculum
greatly in size and have become nearly design and admissions policies of MD–
ubiquitous since their beginnings about In an effort to obtain a snapshot within a PhD programs, which typically focus on
50 years ago at a handful of medical reasonable length of time, we asked the the recruitment and training of bench
schools. However, the number of 24 participating programs to provide scientists. The unstated assumption is
applicants to these programs each year information that they had already that if MD–PhD graduates start in
remains a small fraction of those applying collected. As a result, not all programs laboratory-based research, that is what
to medical school, and the number of could answer all questions about all they will continue to do—an assumption
MD–PhD graduates remains a small alumni, a recognized limitation of the that is challenged by the number of
6 Academic Medicine, doi: 10.1097/ACM.0b013e3181d3ca17Career Choice
graduates who have decided to do unsurprising given the challenges of Alternative paths to research careers
translational and clinical research. The predicting what a 21-year-old applicant If MD–PhD programs are to be viewed as
skill set needed to conduct well-designed will actually do when he or she is 30 to 40 an experiment in training physician–
research in humans is simply not years old. A retrospective analysis does investigators, then what is the
addressed in most graduate school suggest that some choices of a clinical appropriate comparison group? Most
training programs. field for residency are more likely than medical students are not planning
others to lead to a career in private research careers, so using all medical
Although there are no standard criteria practice (Table 3), but given the manner students as a control group is not
to identify a physician–scientist, given of data collection, we cannot determine especially helpful. In considering a
the complexity of modern research whether graduates chose to enter private smaller group, the subset of physicians
many of us advise our students and practice as a consequence of their who apply for NIH grants, Dickler and
prospective students that they will need residency choice or whether the choice of colleagues18 reported that MDs who
to spend 75% to 80% of their time on a residency was a consequence of a become investigators are less successful
research-related activities, leaving the decision not to pursue a career in than MD–PhDs and PhDs in obtaining a
remaining time for clinical care, research. We note that graduates of three first NIH research project grant (R01)
teaching, and other activities that will of the fields that have shown recent gains and, if funded once, are less likely to
hopefully integrate well with their in popularity (dermatology, receive a subsequent R01. They are also
research interests. However, our study ophthalmology, and surgery) had higher- more likely to do clinical rather than
data show that if the designation than-average rates of going into private basic research. There has also been a
physician–scientist is limited to those practice. But it is equally important to decrease in MDs serving on NIH study
who spend at least 75% of their time on note that at least some of the alumni who sections.19
research-related activities, then many chose those fields eschewed private
MD–PhD graduates fit this definition, practice and reported performing funded All of this makes perfect sense if
but many do not (Figure 2A). research. successful MD–PhD program candidates
are viewed as individuals who have gone
A third conclusion is that recent A final conclusion from the data is that through a rigorous vetting process that
concerns that the dropout rate from emphasizes early research experience and
MD–PhD program graduates pursue a
MD–PhD programs is very high and commitment as well as academic
broad range of types of research, perhaps
that many of those who stay in the excellence. It does not mean that
reflecting their training in both science
program until the end enter private attending an MD–PhD program is the
and medicine as well as their original
practice are not justified by the data. only way to become a physician–scientist.
goals when choosing to apply to MD–
We found that most MD–PhD students From our experience as program
PhD programs. Our survey shows that
complete the program, and most directors, we have found that MD–PhD
instead of becoming basic scientists with
alumni are not in private practice. The programs are particularly well suited to
only a distant memory of their medical
average attrition rate of students who individuals who decide early enough in
entered programs in AY1998 –2007 was training, many MD–PhD program their college careers that they have a
10%, very similar to the 12% reported graduates are conducting translational commitment to discovery in medicine
by Fang and Meyer15 for MSTP-funded and patient-oriented research as well as and are fortunate enough to receive
trainees who matriculated between basic research. In keeping with this trend, guidance that includes information about
1980 and 1988, but considerably lower discussions at the annual meetings of physician–scientist training programs.
than the 29% that was reported in 2008 program directors and administrators There will always be a need for alternative
by Andriole and colleagues.9 The suggest that many MD–PhD programs pathways to capture the “late bloomers”
attrition rate varied from 3% to 34% are paying increased attention to the need because there are not currently (and
among the schools in this study, a for their students to be trained (or at least likely never will be) enough MD–PhD
variation that deserves closer scrutiny exposed) to the skills needed for program graduates to maintain the ranks
to establish cause. Our study does not translational and clinical research. Our of active physician–scientists. However,
directly address gender differences survey did not address the question of in general, avoiding an MD–PhD
regarding attrition—whether women whether MD–PhD trainees receive the program is not a strategy that shortens
are less likely than men to persist in a formal training in the design and the time to an independent career, even
physician–scientist career.9,16,17 Gender implementation of human studies that taking into account the rising time to
was not included in the information is increasingly being viewed as essential graduation that we noted for such
supplied on each trainee. At the for clinical investigators. Although the programs. The average age at first R01
program level, however, we did not find training they receive in the scientific was the same (43 years) for both MDs
a correlation between the percentage of method will be helpful, if MD–PhD and MD–PhDs in 2007.20 This suggests
trainees who are women and the graduates are to be successful in this that if one intends to be a
attrition rate from the program. realm as well as in the laboratory, physician–scientist at the time of entry to
additional thought should be given to medical school, skipping graduate school
Overall, we found that 16% of the MD– what they will need to know and when will not save time—presumably because
PhD alumni who completed they should learn it. Timing is an independent research career requires
postgraduate training eventually entered especially important given the need to an extended period of mentored research
private practice, a number that is larger resist making a lengthy training training, whether it is completed during
than one might hope but is perhaps program even longer. medical school or after residency.
Academic Medicine, doi: 10.1097/ACM.0b013e3181d3ca17 7Career Choice
Research careers require research Zemlo and colleagues.19 Nonetheless, a requires continuing attention by
training, which is not usually part of the recent survey of clinical department individual program leaders, and efforts
medical school curriculum. One chairs still reported a large number of should be directed toward both the
alternative path is offered by the Howard vacant positions for physician– selection and the nurturing of trainees.
Hughes Medical Institute-sponsored NIH investigators able to do clinical
Cloister Program, which participants research.22 Finally, the time required to complete an
typically complete after their third year of MD–PhD program is increasing, a trend
medical school. Fang and Meyer15 found The distribution among clinical fields that bodes ill for reversing the ever-
that participants in the Cloister Program chosen by MD–PhD program graduates increasing age at first faculty
were more likely to hold research- has also gradually changed over the past appointment and first R01.2 The average
oriented faculty positions at medical 50 years. Like Andriole and colleagues,9 time to graduation has risen from 6.6
schools than were unsuccessful applicants we found that the proportion choosing years4 to 7.8 years (weighted by program
to the program, but they were less likely internal medicine, neurology, pathology, size) since the early years of MD–PhD
to hold such positions than were the and pediatrics has declined, whereas training programs, which is an 18%
graduates of MSTP-funded programs. those choosing fields such as increase (Figure 3E). This trend may in
Other alternative pathways include dermatology, ophthalmology, radiation part reflect the increasing demands of
obtaining mentored research training or oncology, and surgery has increased medical education. If so, some thought
even attending graduate school after (Figure 3B). In other words, more of the should be given to the education
completing postgraduate clinical training. recent graduates of MD–PhD programs requirements of physician–scientists
Our anecdotal impression is that fewer are choosing clinical training in versus those who will become full-time
are choosing these last two alternatives, at disciplines outside those that have clinicians. Some of the upward trend may
least as a means to move toward an historically been the most willing to also reflect increasing training
independent laboratory-based research provide the large amounts of protected requirements for PhD students25 and a
career. Currently, most of those whose time required to do meaningful research. diminished willingness to cross-count
goal is to focus exclusively on patient- To the extent that residency choice is a credits for work done toward each
oriented rather than basic research obtain predictor of which department MD–PhD degree. Data to substantiate these
the required clinical research training program graduates eventually join, a possibilities were not obtained for this
postresidency, usually in programs that review performed 20 years from now is study but need to be collected in the near
lead to a master’s degree rather than a likely to find that a far broader range of future. Because graduates of MD–PhD
PhD. clinical departments have become the program typically complete six or more
“home” for MD–PhD program alumni. If years of postgraduate training, they have
Trends over time so, then the critical question is, what will a long additional training period before
We observed several notable trends in the they be doing in those departments? their first faculty appointment. If an
data on program alumni. The proportion unacceptable total duration of training is
of graduates that choose to forego Although the reasons underlying this to be avoided, more attention must be
residency training has always been shift can be debated, the change may paid to the requirements at each phase of
relatively small. It seems to be declining result in either a continued positive training that contribute to the whole. Too
further, as is the proportion of alumni outcome (i.e., a wonderful opportunity often, each step on this path to
working in academia with their primary to extend inquiry into new fields) or a independence is overseen by a different
appointment in a nonclinical department very undesirable outcome (i.e., more organization or certification group, and
(Figure 3C). The decline in primary basic investigators leaking out of the pipeline). these groups rarely communicate with
science appointments occurred during a It is too soon to tell, but, as we already each other. For this reason and others, it
period that saw a large growth in both the noted, the data from this retrospective is easy to argue for much better vertical
faculty size21 and the research portfolios study clearly show that graduates of some integration in the training of physician–
of clinical departments. One might residency fields have been far more likely scientists. A call to make this and other
speculate that clinical department chairs than others to eventually become private changes is part of a recent report from
view MD–PhD investigators as a safer bet practitioners (Table 3). Private practice the Association of Professors of
than investigators with a PhD but no fits nobody’s definition of a desirable Medicine.26
MD—individuals with an MD–PhD can outcome for MD–PhD program alumni.
potentially generate clinical revenues; In 2007, Ahn and colleagues23 reported Limitations of this study
those with a PhD cannot. The increase in on the attitudes and career intentions of This study is the largest of its kind to
primary appointments in clinical current trainees; Andriole and date. It is not, however, without
departments may also speak to the colleagues’9 similar survey followed. limitations arising from the method used
commitment of MD–PhD graduates to These studies differ from ours in their to collect the data, and we would like to
pursue disease-related research that finds focus on career intentions rather than point some of those out. The study
a more comfortable home in clinical actual career choices, but it is worrisome includes data from only 24 programs,
departments. This would be consistent that, if true, their survey data raise albeit ones that included 40% of the MD–
with the high percentage of alumni who questions about some trainees’ PhD trainees in the United States at the
report involvement in translational and commitment to research careers.9,23,24 If time of the survey. The programs vary
clinical research (Figure 2B). A shift of MD–PhD programs continue to expand, widely in size and location, but 20 of the
physician–scientists to clinical admission of candidates who lack a participating programs had NIGMS
departments was also noted in 2000 by strong commitment is clearly an area that MSTP grants at the time of data
8 Academic Medicine, doi: 10.1097/ACM.0b013e3181d3ca17Career Choice
collection, and, as already noted, results Dr. Brass is professor, Department of Medicine and nigms.nih.gov/reports/mstpstudy/#10.
from the MSTP-supported programs may Department of Pharmacology, University of Accessed November 25, 2009.
Pennsylvania School of Medicine, Philadelphia, 5 Martin JB. Training physician–scientists for
prove to be different in meaningful ways the 1990s. Acad Med. 1991;66:123–129.
Pennsylvania, where he directs the MD–PhD
from the large number of programs that program. He was 2007 chair, MD–PhD Section, 6 Bradford WD, Anthony D, Chu CT, Pizzo
have not yet benefited from NIH support. Association of American Medical Colleges Group on SV. Career characteristics of graduates of a
These differences may prove to be quite Graduate Research, Education, and Training (AAMC Medical Scientist Training Program, 1970 –
GREAT Group). 1990. Acad Med. 1996;71:484 –487.
important when assessing the
7 Rosenberg LE. MD/PhD programs—A call
performance of individual programs, but Dr. Akabas is professor, Department of Physiology
for an accounting. JAMA. 2008;300:1208 –
and Biophysics, Albert Einstein College of Medicine,
they may not change the aggregate 1209.
Yeshiva University, Bronx, New York, where he
analysis by much. MSTP-supported directs the MD–PhD program. He is co-chair, Data 8 Whitcomb ME. The need to restructure MD–
programs tend to be larger on average and Analysis Committee, MD–PhD Section, AAMC PhD training. Acad Med. 2007;82:623–624.
than those without MSTP support. The GREAT Group. 9 Andriole DA, Whelan AJ, Jeffe DB.
Characteristics and career intentions of the
four smallest programs in this study Ms. Burnley is director, Administration and emerging MD/PhD workforce. JAMA. 2008;
enrolled only 31 to 34 trainees and had 36 Finance, Harvard–Massachusetts Institute of 300:1165–1173.
Technology Combined MD–PhD Program, Harvard
to 71 alumni at the time of the study. In Medical School, Boston, Massachusetts. She is co-
10 Dorsey ER, Jarjoura D, Rutecki GW.
contrast, even the four smallest of the NIH- Influence of controllable lifestyle on recent
chair, Data and Analysis Committee, MD–PhD
supported programs had more trainees Section, AAMC GREAT Group. trends in specialty choice by US medical
students. JAMA. 2003;290:1173–1178.
(52–66) and more alumni (60 –133). Dr. Engman is professor, Department of 11 Newton DA, Grayson MS. Trends in career
Pathology, Northwestern University, Feinberg School choice by US medical school graduates.
It is also worth emphasizing that the of Medicine, Chicago, Illinois, where he directs the JAMA. 2003;290:1179 –1182.
MD–PhD program. He was 2008 chair, MD–PhD 12 Garrison G. AAMC Data and MD–PhD
data on MD–PhD alumni were Section, AAMC GREAT Group. Students. Available at: www.aamc.org/
provided to us by the programs and not members/great/mdphd/presentations/
Dr. Wiley is professor, Department of Pathology,
directly by the alumni. Some programs garrisonhandout.pdf. Accessed December 13,
University of Pittsburgh School of Medicine,
did not include all alumni, and because Pittsburgh, Pennsylvania, where he directs the MD– 2009.
this was not a prospective survey, not PhD program. He was 2009 chair, MD–PhD Section, 13 Frieden C, Fox BJ. Career choices of
every question was asked by every AAMC GREAT Group. graduates from Washington University’s
Medical Scientist Training Program. Acad
program when they last surveyed their Dr. Andersen is professor, Department of Med. 1991;66:162–164.
alumni. However, it is somewhat Physiology and Biophysics, Weill Cornell Medical
14 McClellan DA, Talalay P. M.D.–Ph.D.
College, Cornell University, New York, New York,
reassuring that essentially identical where he directs the MD–PhD program. He was
training at the Johns Hopkins University
results were obtained when our analysis 2005 chair, MD–PhD Section, AAMC GREAT Group.
School of Medicine, 1962–1991. Acad Med.
of outcomes was limited to just those 1992;67:36 –41.
Acknowledgments: The authors thank the MD– 15 Fang D, Meyer RE. Effect of two Howard
programs that submitted data on more Hughes Medical Institute research training
PhD program directors and administrators who
than 98% of their alumni. provided data for this survey. programs for medical students on the
likelihood of pursuing research careers. Acad
Funding/Support: None. Med. 2003;78:1271–1280.
Conclusions 16 Watt CD, Greeley SA, Shea JA, Ahn J.
Other disclosures: None. Educational views and attitudes, and career
In summary, this study shows that many goals of MD–PhD students at the University
Ethical approval: Not applicable.
MD–PhD program graduates are staying of Pennsylvania School of Medicine. Acad
on the physician–investigator career Disclaimer: This study was performed with the Med. 2005;80:193–198.
track. It provides an interim response to a support of the leadership of the National 17 Andrews NC. The other physician–scientist
Association of MD–PhD Programs and the problem: Where have all the young girls
recent call7 for evidence that MD–PhD gone? Nat Med. 2002;8:439 –441.
programs accomplish their mission: Association of American Medical Colleges Group
on Graduate Research, Education, and Training 18 Dickler HB, Fang D, Heinig SJ, Johnson E,
Clearly, they can and do. However, (GREAT Group) Section on MD–PhD Programs. Korn D. New physician–investigators
looking beyond the very positive receiving National Institutes of Health
However, the views expressed are those of the
conclusions driven by the aggregate research project grants: A historical
authors alone and do not necessarily reflect those
perspective on the “endangered species.”
analysis, the data collected in this survey of either organization.
JAMA. 2007;297:2496 –501.
also show that the range of eventual 19 Zemlo TR, Garrison HH, Partridge NC, Ley TJ.
professional “phenotypes” of program The physician–scientist: Career issues and
References challenges at the year 2000. FASEB J. 2000;14:221–
graduates is very broad. It is therefore
1 Goldstein JL, Brown MS. The clinical 230.
entirely legitimate to ask whether all of
investigator: Bewitched, bothered, and 20 National Institutes of Health, Office of
these phenotypes are consistent with the bewildered— but still beloved. J Clin Invest. Extramural Research. Average Age of
currently espoused goals of MD–PhD 1997;99:2803–2812. Principal Investigators. Available at: http://
training. Recognition of this point will 2 Ley TJ, Rosenberg LE. The physician–scientist report.nih.gov/NIH_Investment/PDF_
hopefully prompt further debate. career pipeline in 2005: Build it, and they will sectionwise/NIH_Extramural_DataBook_
come. JAMA. 2005;294:1343–1351. PDF/NEDB_SPECIAL_TOPIC-AVERAGE_
Whatever the outcome of those much- AGE.pdf. Accessed January 5, 2010.
3 Rosenberg LE. The physician–scientist: An
needed debates, continued attention will essential—and fragile—link in the medical 21 Association of American Medical Colleges.
need to be paid to the selection of the research chain. J Clin Invest. 1999;103:1621– U.S. faculty roster reports. Available at:
most appropriate candidates, the 1626. www.aamc.org/data/facultyroster/reports.htm.
mentoring and training of matriculants, 4 National Institute of General Medical Accessed December 13, 2009.
Sciences. MSTP study: The careers and 22 Fang D, Dickler H, Heinig SJ, Korn D.
and the care of program graduates as they professional activities of graduates of the Recruitment of New Physician Investigators in
traverse the challenging divide between NIGMS Medical Scientist Training Clinical Research: Findings From a Survey of
graduation and independence. Program. Available at: http://publications. Clinical Department Chairs at U.S. Medical
Academic Medicine, doi: 10.1097/ACM.0b013e3181d3ca17 9Career Choice Schools. Available at: https://services.aamc.org/ Attitudes, Goals, and Education) survey. Va: National Science Foundation, Division publications/index.cfm?fuseaction⫽Product. Acad Med. 2007;82:633–645. of Science Resources Statistics; 2006. displayForm&prd_id⫽211&cfid⫽1&cftoken⫽ 24 Ahn J, Watt CD, Greeley SA, Bernstein J. 26 Association of Professors of Medicine. 8A91BEF8-B9BB-BF89-888382FD9D06C5DD. MD–PhD students in a major training Recommendations for Revitalizing the Accessed December 13, 2009. program show strong interest in becoming Nation’s Physician–Scientist Workforce. 23 Ahn J, Watt CD, Man LX, Greeley SA, Shea surgeon–scientists. Clin Orthop Relat Res. Available at: www.im.org/PolicyAnd JA. Educating future leaders of medical August 2004;258 –263. Advocacy/PolicyIssues/Research/PSI/ research: Analysis of student opinions and 25 Thurgood L, Golladay MJ, Hill ST. U.S. Pages/default.aspx. Accessed December 13, goals from the MD–PhD SAGE (Students’ Doctorates in the 20th Century. Arlington, 2009. 10 Academic Medicine, doi: 10.1097/ACM.0b013e3181d3ca17
You can also read