Application and Clinical Analysis of Remote Fetal Heart Rate Monitoring Platform in Continuous Fetal Heart Rate Monitoring Images
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Hindawi Journal of Healthcare Engineering Volume 2021, Article ID 5517692, 11 pages https://doi.org/10.1155/2021/5517692 Research Article Application and Clinical Analysis of Remote Fetal Heart Rate Monitoring Platform in Continuous Fetal Heart Rate Monitoring Images Xuan Yang , Ke Zhang, and Jianhu He Women’s Hospital School of Medicine Zhejiang University, HangZhou, ZheJiang 310006, China Correspondence should be addressed to Xuan Yang; yangxuan@zju.edu.cn Received 6 February 2021; Revised 3 March 2021; Accepted 12 March 2021; Published 22 March 2021 Academic Editor: Zhihan Lv Copyright © 2021 Xuan Yang et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. Fetal heart sound is an important part of fetal monitoring and has attracted extensive research and attention from scholars at home and abroad in recent years. The fetal heart rate, extracted from the fetal heart sound signal, is one of the important indicators that reflect the health of the fetus in the womb. In this study, a maternal-fetal Holter monitor based on f ECG technology was used to collect maternal heart rate, fetal heart rate, and uterine contractions signals, isolate the fetal heart rate, and design an algorithm to extract the fetal heart rate baseline, acceleration, variation, wake-up cycle, and nonlinear parameters. Using statistical methods to analyze the average value and range of various characteristic parameters of fetal heart rate under continuous long-term monitoring, the results show that the baseline has a downward trend from 10 o’clock in the night to 4 o’clock in the morning and is the lowest around 2 o’clock in the morning. The area and acceleration time were significantly higher than those in the suspicious group. However, there was no significant difference in the number of acceleration values between the two groups; the proportion of small mutations in the normal group was lower than that of the suspicious group and the proportion of medium mutations was higher than that of the suspicious group. There is no statistically significant difference in maternal age, gestational age at childbirth, pregnancy comorbidities, and complication rates in the five-level interpretation system of ACOG (2009), RCOG (2007), SOGC (2007), and the United States (2007). The difference of pregnancy and parity in various images was statistically significant, P < 0.05. The second type of fetal heart rate monitoring images appeared in the highest among the diagnostic standards, and the difference in the second type of fetal heart rate monitoring images between the various diagnostic standards was statistically significant, P ≤ 0.001. 1. Introduction monitor and diagnose the fetal heart rate of pregnant women [2]. Not only the workload of the department doctors is In recent years, with the full liberalization of the national overloaded, at the same time, the actual fetal heart rate second-child policy and the gradual increase of elderly monitoring needs of pregnant women outside working pregnant women, the work pressure of the hospital’s fetal hours cannot be guaranteed. In response to this, it is one of heart rate monitoring department has also increased [1]. the important tasks of our information construction to How to find a way that is convenient and guarantees the establish a new model based on the cloud platform, with the health and safety of pregnant women and the service di- “Internet + medical” model and the use of modern infor- agnosis and treatment model to reduce the pressure of the mation technology for remote fetal heart rate monitoring fetal heart care unit in the hospital is a hot issue that ev- and diagnosis. eryone is concerned about. At present, the existing tradi- The normal fetal heart rate not only reflects the healthy tional diagnosis and treatment model is based on the heart movement function of the fetus but also reflects the hospital as the main body and the working hours of the control function of the fetal nervous system [3]. The oc- hospital. At the same time, the doctors in the fetal heart currence of fetal ischemia or hypoxia in the mother’s womb monitoring room operate the local fetal heart rate monitor to will cause abnormal fetal heart rate. Once the fetus is in a

2 Journal of Healthcare Engineering state of hypoxia for a long time, it will cause irreversible vascular resistance to the placental blood supply. As the damage. Clinically, the abnormality of the fetal state is gestational age increases, placental vascular resistance de- mainly judged by the fetal heart rate baseline variability, fetal creases, blood supply increases, and the S/D ratio decreases. heart rate variability deceleration, late deceleration, etc. When placental resistance increases and blood supply de- With the in-depth study of fetal heart function in the ac- creases, then the S/D ratio increases. The results of this study ademic field, the fetal heart rate is also used to calculate the show that the higher the S/D value of late umbilical artery Tei index and the KI index. At present, the monitoring of blood flow, the higher the score of the fetal heart monitoring fetuses is mainly done in larger hospitals. In the face of the imaging scoring method, the higher the risk of adverse birth huge number of pregnant women, limited medical resources conditions, and the worse the neonatal outcome. are facing new challenges. In addition, the current moni- toring method has two drawbacks: one is inconvenient to use 2. Related Work and the other is that it cannot monitor the fetus in real time. In this case, remote fetal monitoring equipment has broad The methods of obtaining fetal heart rate mainly include the application prospects. The fetal heart rate, extracted from heart sound transducer method, fetal electrocardiogram fetal heart sounds, is an important part of fetal monitoring method, and ultrasound Doppler method [5]. The heart and directly reflects the health of the fetus in the mother’s sound transducer method uses an electronic earpiece to body [4]. The fetal heart rate reflects the activity of the fetal obtain the fetal heartbeat signal. The heart sound transducer heart, which is mainly regulated by the heart’s own rhythm, method is very safe. It only uses the sound produced by the central nervous system, and hemodynamics. Therefore, the fetal heart itself. However, due to the weak fetal heart sound, periodic changes of the fetal heart rate not only reflect the the sound of the internal organs of the mother is easily mixed activity of the fetal heart but also indicate the ability to and the accuracy is insufficient. The fetal electrocardiogram regulate the developmental state. Fetal heart rate is of great method is divided into a direct method and an indirect significance in the clinical work of obstetrics. After obtaining method. The direct method uses electrodes to insert the the fetal heart rate data, the clinical obstetrician generally fetus’s scalp to obtain the fetal bioelectric signal. This conducts a comprehensive evaluation of the fetal heart rate method has the highest accuracy rate, but an invasive curve. Using the identifiable fetal heart rate parameters in measurement method has a certain risk to the fetus [6]. The the fetal heart rate monitoring curve, you can understand the indirect method uses multiple electrodes attached to the state of the fetus in the uterus and then determine the mother’s abdomen to obtain the weak ECG signal of the prognosis of the perinatal baby and provide a basis for fetus in the womb. This method is easy to mix in the guiding the treatment of the perinatal baby. mother’s ECG signal and is not accurate. The ultrasound The mother-fetal Holter monitor can continuously Doppler method uses an ultrasound probe to transmit ul- monitor and track the fetal heart rate in real time and then trasound to the fetus and obtains the fetal signal based on the initially calculate the parameters such as acceleration, de- reflected wave [7]. This method is highly accurate and celeration, and the number of mutations. The retrospective noninvasive. analysis of the fetal heart rate data obtained by the mother- At present, the research direction of scholars on fetal fetal Holter monitor to extract more effective fetal heart rate heart sound monitoring technology is mainly three parts: fetal characteristic parameters is of great help to the under- heart signal collection, noise reduction processing, and fetal standing of prenatal fetal development and the classification heart rate extraction [8–11]. In terms of signal acquisition, of fetal types. This is also important for further analysis of there are mainly fetal heart sounds, fetal ECG, and ultrasound perinatal outcomes and early warning of the occurrence of Doppler, etc., which can be divided into two major categories: fetal distress. After the remote fetal heart rate monitoring active and passive according to the extraction method [12]. platform was launched, 1,200 pregnant women in early The active type is mainly the ultrasonic Doppler extraction pregnancy were invited to participate in the trial of the method that is currently popular on the market. Ultrasound is research group, and the system was gradually introduced to transmitted to the pregnant woman’s abdomen in advance, the market. Based on the data from the cloud platform, our and the fetal heart rate information is obtained through the hospital is initially establishing a continuous health moni- reflected wave [13]. Relevant scholars use the Doppler toring model of comprehensive indicators for pregnant principle and dynamic weighting matrix to obtain the fetal women and fetuses and establishing a correlation with the heart rate and effectively improve the signal-to-noise ratio of Apgar score of newborns. The relationship between fetal the received signal [14, 15]. Pregnant women do not need to heart rate baseline and monitoring time was analyzed, and go to the hospital frequently to pay expensive fees and can the relationship between fetal heart rate baseline, baseline learn about the status of the fetus in time at home. Related variability, and acceleration parameters and gestational age scholars also use the Doppler principle to obtain more de- was studied. The long-term fetal heart rate monitoring of tailed information on fetal heart sounds [16]. Passive ex- NST suspicious fetuses showed abnormal characteristics in traction mainly includes two extraction methods: fetal ECG terms of baseline fetal heart rate variability and fetal heart and fetal heart sounds. Fetal ECG is a multichannel extraction rate acceleration, including reduced fetal heart rate baseline method that uses multiple electrodes to extract electrical variability, decreased proportion of normal variability, and signals on the skin of pregnant women. decreased area of fetal heart rate acceleration. Umbilical Researchers use smart sensors to obtain fetal heart artery blood flow S/D represents the ratio of placental sounds and build a wireless platform to realize real-time

Journal of Healthcare Engineering 3 monitoring of fetal heart rate [17]. Among the above- heart rate device to the cloud platform through a 4G or WIFI mentioned three collection methods, the ultrasound network. At the same time, the doctor side of the cloud Doppler collection of fetal heart signals is active, and ul- platform obtains the fetal heart rate data, analyzes and di- trasound needs to be transmitted to the pregnant woman’s agnoses, and then transmits the diagnosis result. The abdomen in advance, which has defects. Ultrasound changes pregnant woman informs the analysis result or reminds the the intrauterine environment of the fetus, and long-term use pregnant woman to go to the hospital for examination will affect the fetus, so the advice given by professional doctors immediately. This kind of “one-to-one” closed-loop man- is not to use it for a long time. The collection method of fetal agement of doctors and patients allows doctors to directly ECG requires multiple electrodes to be placed on the surface manage and track their patients remotely. The storage of the of the pregnant woman’s skin. The collection position has a cloud platform can accept all patients’ medical history data greater impact on the accuracy of the measurement results. and avoid the trouble caused by loss of paper data, so that Large deviations may even result in the inability to collect doctors have a comprehensive understanding of the whole useful signals [18]. The multichannel acquisition method pregnancy of pregnant women. increases the difficulty of the user, so this article adopts the method of directly acquiring the original fetal heart sound 3.1. Smart Fetal Heart Rate Device. The hospital research signal, which provides convenience for the user and elimi- group uses an ultrasonic fetal heart rate monitor based on a nates the negative impact of the Doppler method. smart terminal, which is composed of smart hardware, Domestic clinical NST monitoring time and interpre- straps, and smart terminals. After connecting the fetal tation standards are both 20 minutes. If it is suspicious, heartbeat smart hardware with a smart terminal (smart- further evaluation is required; that is, NST is reexamined; if phone, tablet computer, etc.), the fetal heartbeat and APP NST is still suspicious after reexamination, NST needs to be applications will automatically start. It is an electronic reexamined and further ultrasound examination is required. medical device that can monitor, record, remotely consult, The hospital conducts NST several times a day. Such re- and share. peated inspections increase the psychological pressure of pregnant women to a certain extent and occupy some (1) Applicable people: medical resources. NST suspicious fetuses can be normal (a) Pregnant women who are more than 12 weeks in a quiet state, so it is difficult to distinguish normal fetuses pregnant (usually it is easier to find a stable fetal with suspicious monitoring characteristics from them. heart rate after 16 weeks). Therefore, it may be necessary to carry out long-term (b) High-risk mothers, such as pregnancy-induced monitoring of fetuses with suspicious NST, in order to more hypertension, pregnant women who have had an accurately assess the fetal situation through longer artificial abortion, spontaneous abortion, or monitoring. abnormal fetal position. In the method of calculating the fetal heart rate, the (c) Pregnant women who want to know the health of researchers used a relatively simple method, that is, calcu- their fetus at all times. lating the time interval between two fetal heart signal peaks (d) It is not convenient for pregnant women who and further calculating the number of peaks within one frequent the hospital. minute to represent the fetal heart rate. Relevant scholars use the time window method [19–21]. First, they calculate the (2) How to use: number of crests in a fixed-length time window and then (a) Download the software and search the product calculate the number of windows within one minute and name through the application store to get the multiply it by the number of crests to express the fetal heart APP. rate. In order to meet the requirements of real-time cal- (b) Connect the probe, open the application soft- culation, the window continuously slides backward in units ware, and turn on the Bluetooth function of the of one second. In addition, the researchers used a short-time mobile phone. Fourier transform to extract the instantaneous fetal heart (c) To find the fetal heart rate, place the probe on the rate, and the researchers used the autocorrelation calculation abdomen and move it slowly. After the fetal heart to also extract the instantaneous fetal heart rate [22–24]. rate is found, the mobile phone application will These methods need to be based on the relatively stable display the monitoring data, and the pregnant period of the fetal heart sound signal and are more sensitive woman can record the fetal heart rate and upload to noise. the recording to the cloud to wait for the di- agnosis result after the specified time. 3. Design and Function of Remote Fetal Heart Rate Monitoring Platform 3.2. System Architecture. The system adopts a multilayer With the rapid development of the Internet and mobile architecture, using fetal heart monitoring equipment tech- communication technology, more and more smart wearable nology, cloud technology, mobile wireless communication devices and smart medical devices have begun to enter technology, Bluetooth communication technology, remote ordinary households. Pregnant women can easily transmit data transmission technology, etc. to realize the design and the fetal heart rate data collected by the smart medical fetal application of the remote fetal heart rate monitoring

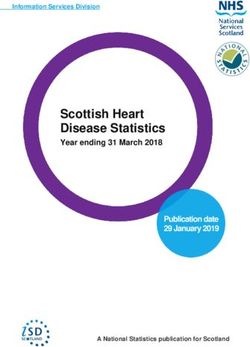
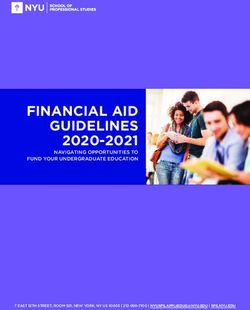
4 Journal of Healthcare Engineering platform, and the basic fetal heart rate of pregnant women, direct and the earliest method to analyze FHR. The time- acceleration times, deceleration times, high and low change domain analysis method and the morphological method period minutes, long mutation period and amplitude, short have similarities. Clinical obstetricians analyze the physio- mutation period and amplitude, fetal movement, and other logical state of the fetus in the uterus based on the mor- parameters are monitored and recorded together. At the phological characteristics of the fetal heart monitoring chart. same time, functions such as display, storage, printing, and The morphological parameters are mostly features that can recall can be realized. The specific architecture is shown in be subjectively observed from the monitoring chart, such as Figure 1. acceleration and baseline trends. This parameter is also a time-domain feature. The time-domain analysis method directly extracts the waveform characteristics from the FHR 3.3. Self-Measurement for Pregnant Women. Pregnant signal, such as the fetal heart rate amplitude, average value, women can monitor and measure their own fetal heart rate and acceleration duration, which has the advantages of clear at any time by turning on their mobile phones and fetal heart physical meaning and intuitiveness. Time-domain analysis rate monitors at home or in other places with a network methods often use methods such as peak detection, analysis environment. After the pregnant woman connects the device of variance, and histograms for analysis. Since the param- by turning on the Bluetooth of the mobile phone and the eters obtained by the time domain analysis method are easier client app, they read the information promptly and then look to understand and accept by clinicians, the parameters for the fetal heart rate, and the fetal heart rate monitor provided by the currently widely used electronic fetal heart displays the test data, then records the qualified data for a rate monitors are mostly time domain or morphological specified time, and finally uploads the cloud platform to wait parameters. for the doctor to remotely diagnose. It saves pregnant In electronic fetal heart rate monitoring, the baseline of women from the trouble of traveling to and from the fetal heart rate is defined as the average fetal heart rate within hospital and waiting for treatment and brings safety and 10 minutes of fetal heart rate fluctuations within 5 bpm, and convenience to the health of pregnant women and fetuses. the segments with acceleration, deceleration, and significant variation are excluded. The baseline must be a segment that 3.4. Doctor Remote Diagnosis and Other Functions. lasts for more than 2 minutes in any 10 minutes. The seg- Doctors can log in to the cloud platform through the mobile ment can be discontinuous; otherwise, the baseline is un- client or PC to view the fetal heart rate monitoring infor- certain during the observation period. In this case, the mation of pregnant women they manage anytime and baseline can be determined by referring to the previous 10 anywhere. Through the push of mobile phone messages, the minutes of images. Figure 2 is a block diagram of the ex- doctor can open and view the monitoring data recorded by traction of baseline feature parameters of fetal heart rate the pregnant women. The system can display important data monitoring. such as basal fetal heart rate, acceleration and deceleration Clinically, the heart rate chart of the fetus is traced and times and changes, high and low changes in minutes, long remembered through the mother-fetal Holter monitor, mutation period and amplitude, short mutation period and showing a fluctuating curve, subjectively assessed by ob- amplitude, fetal movement, and other important data to stetric experts whether it is normal. The baseline fetal heart doctors in each time period, providing clinical information rate refers to the imaginary line in the center of the graph. for reference; it is convenient for doctors to remotely di- Therefore, the baseline extraction method is not unique. This agnose patients. research proposes an algorithm similar to scanning Similarly, the system also has the function of remote extraction. consultation and message, because the initial design of the The fetal heart rate signal after preprocessing is platform is based on the contracting system between doctors N and patients. After the patient signs the informed consent bmp(k) � gi (k). (1) form, the doctor and the patient basically maintain a one-to- i�1 one relationship throughout the pregnancy. You can leave a message in the system when you have doubts, so that the We divide it into signal M segments with a fixed length of doctor can receive information pushes or return the con- one minute and discard those with a length of less than one sultation results after opening the doctor’s terminal to accept minute. The h-th segment is d(h) and folded into matrix the consultation, so that pregnant women can receive de- A. Matrix A is a matrix with (M-9) rows and 10 columns, and tailed guidance services. And the platform also provides each row of the matrix is a fetal heart rate signal with a fixed pregnant women’s social circle, so that pregnant women can length of ten minutes. The baseline value after average share their experiences and conditions during pregnancy optimization processing is and promote their health during pregnancy. Sum iA biA � . (2) GiA 4. Fetal Heart Rate Feature Parameter Extraction and Analysis 4.2. Extraction and Analysis of Fetal Heart Rate Acceleration 4.1. Extraction and Analysis of Baseline Parameters of Fetal and Deceleration Parameters. Fetal heart rate is stimulated Heart Rate. The time-domain analysis method is the most by contractions, fetal movement, sound, palpation, etc.; it
Journal of Healthcare Engineering 5 Internet Remote patient Secure data monitoring server Contraction Piezoelectric interface pressure sensor ultrasonic sensor Intelligent terminal Bluetooth Baseline fetal heart rate Other nodes Fetal heart rate nonlinear parameters Fetal heart rate Fetal heart rate acceleration, variability, wake- deceleration sleep cycle Figure 1: Architecture diagram of remote fetal heart rate monitoring platform. Start End A fluctuating curve Signal input Parameter output Signal preprocessing Parameter calculation Subjective No Baseline recognition evaluation by Is the signal valid? and extraction Fetal heart rate monitoring obstetric experts Remote fetal heart data output monitoring platform Yes Figure 2: The structure diagram of the baseline feature parameter extraction of fetal heart monitoring. will accelerate or slow down for a short time and then return is caused by the compression of the umbilical cord and the to the baseline level. This phenomenon is called a transient excitement of the vagus nerve during contractions. change in fetal heart rate, which is used to judge the fetal The expression of the total area of fetal heart rate ac- intrauterine. celeration is Accelerated fetal heart rate indicates that the fetus is in n−1 wj good condition. As an important part of the fetal electronic S1 � |b(i) − bmp(i)|. (3) monitoring image, acceleration is a phenomenon in which j�0 i�1+wj −aj the fetal heart rate rises rapidly, which is manifested in the image as a protrusion whose duration and heart rate am- We use the total length L of the acceleration time of the plitude both reach a certain threshold. fetal heart rate obtained above and the total area S of the At present, the analysis of fetal heart rate acceleration is acceleration of the fetal heart rate. The unit acceleration rate mainly to classify and count the acceleration by visual in- expression is spection, and the information contained in the acceleration S of the fetal heart rate signal is not sufficiently extracted. PAR � . (4) L Using digital signal processing technology to digitize the fetal heart rate signal can obtain more objective parameter Among them, PAR is the unit acceleration rate, which is values, which is helpful to obtain more comprehensive characterized by the acceleration amplitude of the fetal heart information. rate per unit time during the acceleration period of the fetal Fetal heart rate deceleration is divided into early de- heart rate monitoring. The unit acceleration rate PAR can be celeration and late deceleration. Early deceleration and late combined with specific parameters to obtain the number of deceleration mostly occur during delivery. This study only grids occupied by the acceleration area in the fetal heart rate discusses the variable deceleration that occurs before de- monitoring chart. The expression of the number of grids for livery. Clinically, it is believed that the variable deceleration acceleration per unit time is
6 Journal of Healthcare Engineering L Δt rate in e (k), and min(e (k)) is the minimum fetal heart rate in S� • • PAR. (5) e (k). max(b (k)) is the maximum baseline heart rate value Lt Δs corresponding to the effective signal e (k) of this segment, A total of 4 fetal heart rate acceleration parameters are and min(b (k)) is the minimum baseline heart rate value extracted. The acceleration ratio is the ratio of the length of corresponding to the effective signal e (k) of this segment. the acceleration time to the length of the effective super- intendent care. The number of acceleration values is the number of acceleration values that occur within an average 4.4. Extraction and Analysis of Nonlinear Parameters of Fetal of 20 minutes, and the acceleration duration is the duration Heart Rate. Approximate entropy reflects the difference of acceleration within an average of 20 minutes. The ac- between the approximate probability of a polyline segment celeration area is the number of grids of the recording paper connected by m points in the sequence and the approximate occupied by the acceleration coverage area in an average of probability of a polyline segment connected by m + 1 20 minutes. The recording paper is the fetal heart rate curve points, so it reflects when the dimensionality changes from printed by the clinical fetal heart rate monitor, and each grid m. When it is increased to m + 1, a new mode possibility is is 30 seconds long and 10 bpm high. The deceleration ratio is generated. Approximate entropy Ap En has three param- the ratio of the length of the deceleration time to the length eters, n is the data length, r is the similarity tolerance, and m of the effective supervisory time. is the number of data segments. r is generally used as a percentage of the standard deviation of the data. The smaller Ap En value indicates the data comparison rules; 4.3. Extraction and Analysis of Fetal Heart Rate Variability the larger the Ap En value, the greater the probability of and Wake-Sleep Cycle. The baseline variation of fetal heart generating a new pattern, so the sequence is more com- rate is the result of the interaction between the vagus nerve plicated. The characteristics of Ap En value can be used to and the sympathetic nerve. Sympathetic nerve excitement reflect the changes in the physiological characteristics of accelerates the fetal heart rate, and vagus nerve excitement fetal heart rate. In recent years, the application of nonlinear slows down the fetal heart rate. It is generally believed that if dynamics methods to analyze physiological signals has the fetal heart rate variability is reduced, the fetus’s intra- gradually matured. Fetal heart rate signals are generally uterine vascular reserve capacity is reduced, and there may considered to have chaotic components. Therefore, non- be acidosis. The study of the fetal wake-up cycle is very linear dynamics analysis is often more effective than important to determine whether the NST is reactive. If a common statistical methods or power spectrum analysis normal fetus is in a quiet sleep cycle during the NST test, it methods. This article uses Pincus’ approximate entropy is easy to be misdiagnosed as NST suspicious (or NST analysis method to study fetal heart rate parameters. We nonresponsive), thereby increasing the false positive rate. A analyze the correlation between the Ap En value of fetal normal fetus diagnosed as NST suspicious requires repeated heart rate and heart rate variability and the fetal type and inspections, which will waste a lot of medical resources. initially evaluate the clinical application value of this in- We receive the signal F (t) measured by the electronic dicator in the early diagnosis of fetal distress. fetal heart monitoring instrument. F (t) contains the Because the data length is too long, the calculation time mother’s heart rate signal, fetal heart rate signal, the number will be seriously extended, but the random 5-minute fetal of movements of the mother, and the uterine myoelectric heart rate data reflects less physiological information, and signal and separates the fetal heart rate signal from the signal the fetal heart rate baseline value step of 1 minute will ignore F (t). In the deceleration recognition module, the separated a lot of information. Therefore, the approximate entropy of fetal heart rate signal f (t) is preprocessed, and the decel- fetal heart rate variability with a relative time length of 2 eration definition is used to extract and identify the fetal hours and a step length of 10 seconds is more significant and heart rate deceleration segment. The following is the specific statistically significant between the two groups. identification method of deceleration. After filtering out the effective signal e (t), we use e (t) to calculate the characteristic parameter c to identify the fetal 5. Results of Clinical Analysis quiet sleep period. The first is to screen the effective signal 5.1. Interpretation of Fetal Cord Venous Blood pH Value and e (t). For the fetal heart rate signal g (k), we divide it into Fetal Heart Imaging Monitoring. 1200 cases of parturients all signal segments min(k) with a fixed length of one minute. underwent umbilical vein blood gas analysis after the fetus We use the effective fetal heart rate signal e (t) to calculate was delivered. Basic and general comparisons found that the characteristic parameter c. A characteristic parameter c is there was a statistical difference in those with pH < 7.2 and calculated corresponding to the effective signal e (k) of each less than pH ≥ 7.2 (P � 0.01); those with a pH < 7.2 and minute length, as follows: higher surgical yield than pH ≥ 7.2 had statistical differences maxe(k) − minb(k), min[e(k) − b(k)] > 0, (P ≤ 0.001). The comparison of gestational age at delivery of c � max[e(k) − b(k)] − min[b(k) + e(k)], others, 1200 fetal umbilical vein pH values is shown in Figure 3. (6) Umbilical venous blood pH < 7.2 was diagnosed as fetal acidemia, the fetal heart rate monitoring images above where b (k) is the baseline heart rate corresponding to the category II in ACOG (2009) guidelines were abnormal, and heart rate signal e (k). max(e (k)) is the maximum fetal heart RCOG (2007) stipulated suspicious and pathological fetal
Journal of Healthcare Engineering 7 285 Gestational age at childbirth (day) 283 281 279 277 275 0 200 400 600 800 1000 1200 1200 fetal umbilical veins Figure 3: Comparison of gestational age at delivery of 1200 fetal umbilical vein pH values. 100 90 80 70 60 Rate (%) 50 40 30 20 10 0 Sensitivity Specificity Positive predictive value Negative predictive value False positive rate ACOG RCOG SOGC U.S. level 5 Figure 4: The predictive value of the second and above images of the four interpretation standards for continuous fetal heart rate monitoring during labor. heart monitoring images as abnormal images, and SOGC added together to obtain the total score. A receiver operating (2007) stipulates that atypical and abnormal fetal heart rate curve was used to analyze the diagnostic ability of the total monitoring images are abnormal images. The images above score on fetal acidemia. The receiver operating curve was blue in the five-level evaluation standard of the United States used to analyze the diagnostic ability of the total score for the (2007) are abnormal images. The positive predictive value of newborn’s adverse birth conditions. The area under the the four interpretation standards is very low, while the curve was 0.62, which means that the diagnostic accuracy negative predictive value is high, as shown in Figure 4. rate was 62.0%. According to the receiver operating curve analysis result, when the total score is ≥5.5, the sum of sensitivity and specificity is the highest. The receiver op- 5.2. Correlation Analysis of Abnormal Image Scoring Method erating curve is shown in Figure 5. of Continuous Monitoring during Delivery and Newborn Birth Conditions. Umbilical venous blood pH
8 Journal of Healthcare Engineering 1 0.8 Sensitivity 0.6 0.4 0.2 0 0 0.1 0.2 0.3 0.4 0.5 0.6 0.7 0.8 0.9 1 Specificity Figure 5: Receiver operating curve. 25 20 Logistic regression value 15 10 5 0 –5 B Wald value P value OR value ACOG RCOG SOGC U.S. level 5 Figure 6: Multivariate logistic regression analysis results of the four diagnostic criteria of 1200 cases of continuous fetal heart monitoring images during labor and the maternal clinical conditions. monitoring. Class I fetal heart monitoring images are 5.4. Correlation Analysis of Combined Fetal Heart Monitoring considered normal images, and Class II and III fetal heart and Other Fetal Monitoring on Adverse Fetal Outcomes. monitoring images are considered abnormal images; The adverse fetal outcome is the dependent variable. The SOGC (2007) normal and atypical images are considered third type of image of the better fetal monitoring grading normal images, and abnormal images are used as ab- system in the previous statistical analysis is abnormal. The normal images; RCOG (2007) normal and suspicious score obtained by the fetal heart monitoring scoring method images are used as normal images, and pathology is used is combined with the uterine artery PI, RI, and S/D in the as abnormal images. Taking the age, gestation, and second and third trimesters. The PI, RI, and S/D values of parity, gestational week of delivery, pregnancy compli- umbilical artery in late and full-term pregnancy and full- cations and complications, umbilical cord condition, term biophysical scores were used as independent variables birth sex, birth weight, amniotic fluid state, amniotic to perform multivariate logistic regression analysis, and the fluid volume, and labor process as independent variables, regression equations were included as fetal heart monitoring and whether the fetal heart rate monitoring image is image scores and late cord blood flow S/D values. The results normal dependent variables, multivariate logistic re- show that the higher the score obtained from the fetal heart gression analysis was performed. The results showed that monitoring image, the higher the late cord blood flow S/D the fewer the births, the greater the possibility of ab- value, and the higher the risk of poor birth conditions of the normal fetal heart monitoring images, as shown in newborn, as shown in Figure 7. The magnetic resonance Figure 6. images of 4 fetuses in this study are shown in Figure 8.
Journal of Healthcare Engineering 9 20 15 Logistic regression value 10 5 0 B Wald value P value OR value 95%Cl in OR S/D value of late cord blood flow Fetal heart rate monitor graph score Figure 7: Multivariate logistic regression analysis results of 1200 cases of intrapartum continuous fetal heart monitoring images combined with measurement of uterine artery blood flow, umbilical artery blood flow, and biophysical score. (a) (b) (c) (d) Figure 8: Magnetic resonance images of 4 fetuses. 6. Conclusion groups based on the NST test results of clinical prenatal electronic fetal heart monitoring. Using long-term moni- Through the data analysis capabilities of the smartphone 4G toring data, the baseline, acceleration, variation, wake-up network and the fetal heart rate monitoring cloud platform, period, and nonlinear parameters of fetal heart rate are the fetal heart rate sensing device can continuously track and extracted as characteristic parameters. According to the intelligently remind pregnant women and fetuses during difference between the above characteristic parameters in their stay at home. On the one hand, pregnant women and the normal group and the suspicious group, we analyze the their family members can intuitively understand fetal de- trend of the fetal heart rate characteristic parameters with velopment and health-related data through mobile phones. the monitoring time and gestational week. The frequency of On the other hand, they can continuously record the variable deceleration and the degree of prolonged deceler- monitored data into the pregnant women’s personal in- ation are closely related to the adverse neonatal outcome. It formation through mobile and WIFI networks and store, is recommended that the index of the degree of variable track, and correspond to the data through the cloud plat- deceleration should be included in the interpretation form. The doctor’s analysis makes medical assessments of standard of intrapartum fetal heart rate monitoring. For the health of pregnant women and fetuses. If abnormalities prolonged deceleration, not only the extension of the de- are found, they will use smartphones to remind pregnant celeration duration but also the comprehensive extending women of some precautionary measures they need to take or deceleration should be considered. require pregnant women to go to designated medical in- With the healthy delivery of pregnant women monitored stitutions for in-depth examination and observation. In this by a large number of platforms, the remote fetal heart rate project, the fetuses are divided into normal and suspicious monitoring platform is gradually accepted and used by more
10 Journal of Healthcare Engineering pregnant women, which not only reduces the pressure of [4] S. Widadi, Z. A. Manzila, and I. Ahmad, “Aroma electric hospital admissions and pregnant women’s waiting but also therapy equipment with atmega8-based heart rate monitor- optimizes the process, saves time, and saves resources for ing,” Journal of Robotics and Control (JRC), vol. 1, no. 2, pregnant women. At the same time, the one-to-one service pp. 49–54, 2020. system makes full use of the fragmented time of offline [5] H. Niela-Vilen, A. Rahmani, P. Liljeberg, and A. Axelin, “Being “A Google Mom” or securely monitored at home: women’s insurance hospitals at all levels and the resources of perceptions of remote monitoring in maternity care,” Journal community responsible doctors. The hierarchical manage- of Advanced Nursing, vol. 76, no. 1, pp. 243–252, 2020. ment of pregnant women, community responsible doctors, [6] J. Zhou, “Artificial intelligence driven wireless network re- and specialist doctors is helpful for exploring the estab- mote monitoring based on Diffie-Hellman parameter lishment of a family contract-style home. The continuous method,” Computer Communications, vol. 160, pp. 132–138, health management model combining online and offline for 2020. pregnant women provides a reference basis. In the initial [7] B. Venkataramanaiah and J. Kamala, “ECG signal processing design and application stage, the original connection and and KNN classifier-based abnormality detection by VH- transmission of the fetal heart rate sensing device and the doctor for remote cardiac healthcare monitoring,” Soft mobile phone were completed through the audio headset Computing, vol. 24, no. 22, pp. 17457–17466, 2020. cable. Due to the forward-looking nature of the development [8] R. Li, H. Qi, Y. Ma et al., “A flexible and physically transient team, taking into account the fact that later smartphones will electrochemical sensor for real-time wireless nitric oxide monitoring,” Nature Communications, vol. 11, no. 1, pp. 1–11, gradually cancel the audio jack, such as the Apple 7th 2020. generation, the device is improved in time to adopt the [9] Y. Lu, X. Zhang, L. Jing, X. Li, and X. Fu, “Estimation of the Bluetooth transmission method, avoiding the disadvantage foetal heart rate baseline based on singular spectrum analysis of not being able to connect the phone and the instrument and empirical mode decomposition,” Future Generation with a data cable. However, since doctors also have time to Computer Systems, vol. 112, pp. 126–135, 2020. rest, it is indeed impossible to fully achieve the anytime/ [10] S. W. Bahrum, S. Syarif, M. Ahmad, and N. A. Mappaware, anywhere service model advertised by the platform. Con- “Combining intermittent auscultation and contraction pal- sidering that if the number of users on the platform increases pation monitoring with cardiotocography in inpartu in the later period, a working model of doctors on duty will mothers,” Enfermerı́a Clı́nica, vol. 30, pp. 547–549, 2020. be established in the cloud to provide pregnant women with [11] M. B. Mohamed, M. Yoshizawa, N. Sugita, S. Yamaki, and all the time. K. Ichiji, “Noncontact monitoring of heart rate responses to taste stimuli using a video camera,” Indonesian Journal of Electrical Engineering and Computer Science, vol. 18, no. 1, Data Availability pp. 293–300, 2020. [12] J. Peng, Y. Huang, K. Yu, R. Fan, and J. Zhou, “Maternal The data used to support the findings of this study are health care wearing equipment based on fetal information available from the corresponding author upon request. monitoring,” Journal of Infection and Public Health, vol. 13, no. 12, pp. 2009–2013, 2020. Conflicts of Interest [13] P. K. Choudhary, B. S. Bhati, and S. Bishnoi, “Role of non stress test in monitoring antenatal fetal well being in high risk The authors declare that they have no known competing pregnancy,” Indian Journal of Obstetrics and Gynecology financial interests or personal relationships that could have Research, vol. 7, no. 2, pp. 201–206, 2020. appeared to influence the work reported in this paper. [14] J. Rong, C. Wang, and Y. Lu, “Application research of fetal monitor based on SOPC technology,” International Core Acknowledgments Journal of Engineering, vol. 6, no. 7, pp. 179–184, 2020. [15] L. Hruban, P. Janků, K. Jordanova et al., “The effect of This work was supported by the Zhejiang Science and transient fetal bradycardia and other heart rate changes Technology Plan Project: The Continuous Health Moni- during and after external cephalic version on perinatal out- toring Platform for Pregnant Women and Fetuses, No. comes,” European Journal of Obstetrics & Gynecology and 2014C33082. Reproductive Biology, vol. 245, pp. 39–44, 2020. [16] X. Liu, F. Wang, X. Ding, Y. Chen, and L. Wang, References “Strengthening the maternal and child health system in re- mote and low-income areas through multilevel governmental [1] R. Pilarczyk, M. Strózik, and L. Hirnle, “Diagnostic equiva- collaboration: a case study from nujiang prefecture in China,” lency of mobile CTG devices and remote analysis to con- Public Health, vol. 178, pp. 23–30, 2020. ventional on-site nonstress test,” Advances in Clinical and [17] A. Gracia-Perez-Bonfils, O. Martinez-Perez, E. Llurba, and Experimental Medicine, vol. 29, no. 1, pp. 33–44, 2020. E. Chandraharan, “Fetal heart rate changes on the car- [2] A. Chaturvedi and M. Kumar, “Consistent observing of fetal diotocograph trace secondary to maternal COVID-19 infec- pulse and UteruswithDrawls,” European Journal of Molecular tion,” European Journal of Obstetrics & Gynecology and & Clinical Medicine, vol. 7, no. 4, pp. 145–150, 2020. Reproductive Biology, vol. 252, pp. 286–293, 2020. [3] X. Zhang, J. Sun, and C. Li, “Development and research of [18] T. Kupka, A. Matonia, M. Jezewski, K. Horoba, J. Wrobel, and exercise heart rate monitoring system under the concept of J. Jezewski, “Coping with limitations of fetal monitoring Internet of things telemedicine and mobile health,” Journal of instrumentation to improve heart rhythm variability assess- Medical Imaging and Health Informatics, vol. 11, no. 4, ment,” Biocybernetics and Biomedical Engineering, vol. 40, pp. 1106–1111, 2021. no. 1, pp. 388–403, 2020.
Journal of Healthcare Engineering 11 [19] A. J. Rosenbaum, R. M. Smith, E. M. Hade, A. Gupta, A. Yilmaz, and M. Cackovic, “Use and experiences with external fetal monitoring devices among obstetrical pro- viders,” The Journal of Maternal-Fetal & Neonatal Medicine, vol. 33, no. 14, pp. 2348–2353, 2020. [20] Y. Aggarwal, J. Das, P. M. Mazumder, R. Kumar, and R. K. Sinha, “Heart rate variability features from nonlinear cardiac dynamics in identification of diabetes using artificial neural network and support vector machine,” Biocybernetics and Biomedical Engineering, vol. 40, no. 3, pp. 1002–1009, 2020. [21] S. Lapointe, D. Rottembourg, and F. Dallaire, “Isolated fetal sinus bradycardia as a first sign of congenital hypopituita- rism,” CJC Open, vol. 2, no. 5, pp. 420–422, 2020. [22] I. Janczarek, W. Ke˛dzierski, I. Wilk, E. Wnuk–Pawlak, and A. Rakowska, “Comparison of daily heart rate variability in old and young horses: a preliminary study,” Journal of Vet- erinary Behavior, vol. 38, pp. 1–7, 2020. [23] J. Turner, L. Dunn, W. Tarnow-Mordi, C. Flatley, V. Flenady, and S. Kumar, “Safety and efficacy of sildenafil citrate to reduce operative birth for intrapartum fetal compromise at term: a phase 2 randomized controlled trial,” American Journal of Obstetrics and Gynecology, vol. 222, no. 5, pp. 401–414, 2020. [24] A. Pisesky, Z. C. Luo, E. Jaeggi, G. Ryan, J. Keunen, and T. Van Mieghem, “Umbilical and middle cerebral artery Doppler measurements in fetuses with congenital heart block,” Journal of the American Society of Echocardiography, vol. 34, no. 1, pp. 83–88, 2020.
You can also read