Angiotensin receptor-neprilysin inhibitors: Comprehensive review and implications in hypertension treatment - Nature
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Hypertension Research (2021) 44:1239–1250
https://doi.org/10.1038/s41440-021-00706-1
REVIEW ARTICLE
Review series - New Horizons in the Treatment of Hypertension
Angiotensin receptor-neprilysin inhibitors: Comprehensive review
and implications in hypertension treatment
Koichi Yamamoto1 Hiromi Rakugi1
●
Received: 30 April 2021 / Revised: 16 June 2021 / Accepted: 21 June 2021 / Published online: 21 July 2021
© The Japanese Society of Hypertension 2021
Abstract
Angiotensin receptor-neprilysin inhibitors (ARNIs) are a new class of cardiovascular agents characterized by their dual
action on the major regulators of the cardiovascular system, including the renin–angiotensin system (RAS) and the
natriuretic peptide (NP) system. The apparent clinical benefit of one ARNI, sacubitril/valsartan, as shown in clinical trials,
has positioned the drug class as a first-line therapy in patients with heart failure, particularly with reduced ejection fraction.
Accumulating evidence also suggests that sacubitril/valsartan is superior to conventional RAS blockers in lowering blood
pressure in patients with hypertension. To decide whether to apply an ARNI to treat hypertension clinically, it is important to
1234567890();,:
1234567890();,:
understand the potential properties of the drug in modulating multiple factors inside and outside the cardiovascular system
beyond its effect on reducing peripheral blood pressure. In this context, ARNIs are distinct from preexisting antihypertensive
medications in terms of the multiple actions of NPs in various organs and the pharmacological potential of neprilysin
inhibitors to modulate multiple cardiac and noncardiac peptides. In particular, analysis of the clinical trials of sacubitril/
valsartan implies that ARNIs can provide additional clinical benefits independent of their original purpose, including
alleviation of glycemic control and renal impairment in patients with heart failure. Understanding the potential mechanisms
of action of ARNIs will help interpret the relevance of their additional benefits beyond lowering blood pressure in
hypertension. This review summarizes the comprehensive clinical evidence and relevance of ARNIs by specifically focusing
on the potential properties of this new drug class in treating patients with hypertension.
Keywords ARNI Heart failure Hypertension Natriuretic peptides
● ● ●
Introduction system (RAS) and the natriuretic peptide (NP) system. In
addition to the clinically promising benefit of inhibition of
In both developing and developed countries, heart failure the angiotensin II type 1 receptor (AT1), a robust increase in
(HF) has been increasingly prevalent and is now a large cardioprotective NPs by the inhibition of the degrading
social and medical burden, referred to as the HF pandemic enzyme neprilysin by sacubitril/valsartan, the only clinically
[1, 2]. Recently, the clinical application of new classes of applied ARNI, has been shown to be beneficial in patients
cardiovascular agents has rapidly advanced the treatment of with HF, particularly those with reduced ejection fraction
HF, including sodium–glucose cotransporter-2 (SGLT2) (EF), in recent clinical trials [5–7]. Several clinical trials
inhibitors [3], hyperpolarization-activated cyclic nucleotide- have also shown that sacubitril/valsartan is superior to
gated (HCN) channel blockers [4], and angiotensin preexisting RAS inhibitors in reducing blood pressure (BP)
receptor-neprilysin inhibitors (ARNIs). ARNIs are char- in hypertensive patients [8–15]. To consider the clinical
acterized by their dual action on the major regulators of the application of ARNI to treat hypertension, it is important to
cardiovascular system, including the renin–angiotensin understand the potential properties of the drug in modulat-
ing multiple factors inside and outside the cardiovascular
system beyond its effect on reducing peripheral BP. In this
context, ARNIs are distinct from preexisting anti-
* Koichi Yamamoto hypertensive medications in terms of the multiple actions of
kyamamoto@geriat.med.osaka-u.ac.jp
NPs in various organs and the pharmacological potential of
1
The Department of Geriatric and General Medicine, Osaka neprilysin inhibitors to modulate multiple cardiac and
university Graduate School of Medicine, Suita, Osaka, Japan noncardiac peptides.1240 K. Yamamoto, H. Rakugi
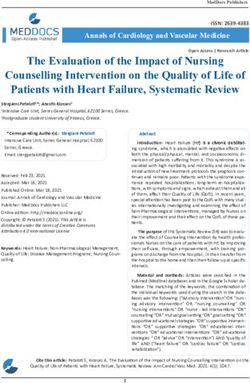
In this review, we will summarize the comprehensive and NPRC, which have distinct roles in the signaling and
clinical evidence and relevance of ARNIs, focusing parti- metabolism of NPs. NPRA, the receptors for ANP and BNP,
cularly on the potential properties of this new drug class in and NPRB, the receptor for CNP, trigger biologically and
treating patients with hypertension. physiologically potent cellular signaling, primarily through
the generation of cyclic guanosine monophosphate (cGMP)
(Fig. 1) [26–29]. By increasing cellular cGMP levels, NPs
Pharmacological property of ARNIs contribute to the regulation of systemic homeostasis and
metabolism, including vasodilation, increased renal perfu-
Sacubitril/valsartan (formerly called LCZ696) consists of an sion, natriuresis, antihypertrophic and antifibrotic actions,
ARB, valsartan, and a neprilysin inhibitor, sacubitril reduced water and salt intake, and lipolysis (Fig. 1) [26–30].
(AHU377), in a 1:1 molecular ratio [16–18]. AHU377 is In contrast, NPRC serves as a clearance receptor for NPs by
converted by enzymatic cleavage of its ethyl ester into the proteolyzing the peptides after internalization. Therefore, the
active neprilysin-inhibiting metabolite LBQ657. Given the net effect of the NP system is determined by the balance
extensive clinical use of ARBs, with abundant evidence of between the production and enzymatic degradation of NPs
their benefit, the pharmacological novelty of this ARNI and their signal transduction and degradation via their
primarily depends on the inhibition of neprilysin, a mem- receptors (Fig. 1). Among the other substrates of neprilysin,
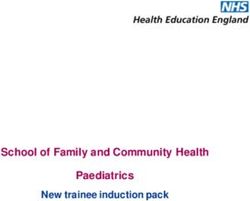
brane metallo-endopeptidase. Neprilysin cleaves peptides at bradykinin, and substance P are associated with a clinically
the amino side of hydrophobic residues, and its diverse relevant symptom of neprilysin inhibition, angioedema,
targets include not only NPs but also glucagon, glucagon- when combined with another enzyme inhibitor class of these
like peptide-1 (GLP-1), bradykinin, substance P, neuro- peptides, the angiotensin-converting enzyme (ACE) inhibi-
tensin, oxytocin, enkephalins, angiotensin I, endothelin-1, tors [21] (Fig. 2). The development of omapatrilat, which is
adrenomedullin, amyloid β, and others [19]. Basic and an inhibitor of both ACE and neprilysin, was terminated
clinical studies have indicated the many modulating effects because of the high incidence of angioedema [31] despite the
of neprilysin inhibitors on its substrates GLP-1 [20], bra- potential benefit shown in the clinical trials for HF with
dykinin, substance P [21], angiotensin I [22], endothelin-1 reduced EF (HFrEF) [32, 33]. Neprilysin also catalyzes the
[23], adrenomedullin [24], and amyloid β [25]. Nevertheless, conversion of angiotensin I into angiotensin 1–7, and a
the protective effect of neprilysin inhibitors on HF is pri- theoretical increase in the cascade from angiotensin I to
marily attributed to the inhibition of the degradation of NPs, angiotensin II by neprilysin inhibitors implies the potential
which consist of atrial NP (ANP), brain NP (BNP), and benefit of the combination of these drugs with ARBs
C-type NP (CNP) (Fig. 1). ANP and BNP, which are called (Fig. 2). Other substrates of neprilysin, including GLP-1 and
cardiac NPs, are released from the atrial and ventricular amyloid β, can be potentially associated with the clinical
walls, respectively, primarily triggered by wall stretching effect of ARNIs, and this issue will be discussed in later
[26, 27]. In contrast, the primary sources of CNP are the sections (Fig. 2).
vascular endothelium and brain [28, 29]. There are three
types of receptors for NPs: NP receptor A (NPRA), NPRB,
Fig. 1 The signaling network of
natriuretic peptides (NPs) and
neprilysin. ANP atrial natriuretic
peptide, BNP brain natriuretic
peptide, CNP C-type natriuretic
peptide, NPRA NP receptor A,
NPRB NP receptor A, NPRC
NP receptor C, GC guanylate
cyclase, GTP guanosine
triphosphate, cGMP cyclic
guanosine monophosphateAngiotensin receptor-neprilysin inhibitors: Comprehensive review and implications in hypertension. . . 1241
Neprilysin sensitive plasma biomarkers of HF [52]. In response to
treatment with S/V, alterations in these biomarkers reflect a
unique signature of pharmacological and therapeutic effects
Angiotensin I NPs GLP-1 Bradykinin Amyloidβ
Insulin-B chain Substance P of the drug. In PARDIGM-HF, median plasma NT-proBNP
VIP
levels in patients treated with S/V were significantly lower
1 month after randomization than in those treated with
BP elevation Cardio protection Glycemic control Angioedema Alzheimer disease
enalapril, and NT-proBNP decreased to ≤1000 pg/ml in
BP reduction
Renal protection
Vasodilation pathology 31% versus 17% of patients treated with S/V versus ena-
Glycemic control
Lipolysis
lapril [43]. In contrast, plasma BNP levels were higher in
patients given S/V after randomization than in those given
Fig. 2 Theoretical relationship between major substrates of neprilysin
enalapril. This paradoxical response of these biomarkers to
and clinical manifestations. BP blood pressure, NPs natriuretic pep-
tides, GLP-1 glucagon-like peptide-1, VIP vasoactive intestinal treatment with S/V was also seen in the later RCT of
polypeptide HFrEF, PIONEER-HF (comparison of sacubitril-valsartan
versus enalapril on effect on NT-proBNP in patients stabi-
lized from an acute HF episode) [6]. In this RCT, the effect
Evidence of the effect on HF of S/V on the time-averaged proportional change in the NT-
proBNP concentration from baseline was compared to that
The apparent benefit of sacubitril/valsartan (S/V) in treating of enalapril in patients with acute decompensated HFrEF.
HFrEF was first shown in a randomized clinical trial (RCT) The results showed that the reduction in the NT-proBNP
named the Prospective Comparison of ARNi with ACE-I to concentration was significantly greater in the S/V group
Determine Impact on Global Mortality and Morbidity in than in the enalapril group, whereas the reduction in BNP
Heart Failure (PARADIGM-HF) [5]. This was a prospective did not differ between the treatment groups [6]. The sec-
multicenter trial in which 8442 patients with HFrEF (EF ≤ ondary analysis of PIONEER-HF showed that S/V
40%) who were classified as New York Heart Association improved the clinical composite outcome of death from any
(NYHA) class 2–4 under sufficient control with β-blockers cause, rehospitalization for HF, left ventricular assist device
and an ACE inhibitor or an ARB were randomly assigned to implantation, and listing for cardiac transplantation [53].
treatment with either S/V 200 mg twice daily or an ACE These clinical benefits of S/V were observed regardless of
inhibitor, enalapril, 10 mg twice daily [5]. The primary the prior use of RAS inhibitors [54].
composite outcome of death resulting from cardiovascular In contrast to the obvious benefits of S/V in HFrEF, the
causes or hospitalization for HF occurred in 914 patients clinical effects of the drug on HF with preserved EF
(21.8%) in the S/V group and 1117 patients (26.5%) in the (HFpEF) remain poorly established. Given the findings in
enalapril group (hazard ratio in the S/V group, 0.80; 95% the phase II trial showing that S/V reduced NT-proBNP at
confidence interval [CI], 0.73–0.87; p < 0.001). There was 12 weeks compared with valsartan in patients with HFpEF
also a reduction in death from any cause, death from car- [55], an RCT named the Prospective Comparison of ARNI
diovascular causes, hospitalization for HF, and the symp- with ARB Global Outcomes in HF with Preserved Ejection
toms and physical limitations of HF in those treated with Fraction (PARAGON-HF) trial was designed to investigate
S/V [5]. Subsequent subanalyses of PARDIGM-HF data the effect of ARNI on clinical outcomes in patients with
have also shown that S/V was superior to enalapril in HFpEF. A total of 4822 HF patients with NYHA class 3–4,
alleviating the worsening of surviving patients with HF EF of 45% or higher, elevated levels of natriuretic peptides,
[34], alleviating the clinical worsening of HF treated in the and structural heart disease were randomly assigned to
outpatient setting [35], hospital readmission at 30 days receive S/V 200 mg twice daily or valsartan 160 mg twice
following HF hospitalization [36], recurrent hospitalizations daily [56]. S/V did not significantly reduce the primary
and CV deaths [37], and quality of life [38]. The treatment composite outcome of total hospitalizations for HF and
benefit of S/V over enalapril was evident irrespective of the death from cardiovascular causes (rate ratio, 0.87; 95%
cause of cardiac death [39], age [40], severity of HF [41], confidence interval [CI], 0.75–1.01; p = 0.06). Regarding
baseline EF [42], baseline plasma N-terminal pro BNP (NT- secondary outcomes, S/V was associated with greater
proBNP) level [43], the presence of prediabetes or diabetes improvement in NYHA class and in the Kansas City Car-
[44], recent hospitalization due to HF [45], baseline treat- diomyopathy Questionnaire (KCCQ) score, a patient-
ment of HF [46], baseline BP [47], the presence of hypo- reported outcome of symptoms and physical limitations,
tension [48], dose reduction of the treatment drugs [49], than valsartan. The prespecified subgroup analysis of the
geographic variations [50], and etiology of HF [51]. primary outcome showed that S/V reduced risk in females
BNP77–108 and the biologically inactive fragment NT- [56, 57] and patients with a median EF (57%) or lower [56].
proBNP1-76, both cleaved from pro-BNP1–108, serve as The combined analysis of PARADIGM-HF and1242 K. Yamamoto, H. Rakugi PARAGON-HF data showed that the treatment benefit of valsartan achieved greater ambulatory BP reductions at S/V over valsartan was modified by LVEF, and a benefit nighttime than during daytime, the reduction under S/V appeared to be present primarily in individuals with EF being greater, consistent with the notion that diuretic- below the normal range (
Table 1 The summary of randomized clinical trials of sacubitril/valsartan versus ARBs in patients with hypertension
Patient background S/V Comparator Duration for evaluation BP lowering effect Specific findings besides BP lowering effect Ref.
Patients with mild to 200 mg (n = 188) Olmesartan 20 mg (n = 8 weeks 24‐h mean ambulatory SBP were observed in the S/V group N/A [8]
moderate essential 187) vs. the olmesartan group (−4.3 mmHg vs. −1.1 mmHg,
hypertension P < 0.001). Reductions in 24‐h mean ambulatory diastolic BP
(>18 years) and PP and office SBP and DBP were significantly greater
with S/V vs. olmesartan.
Asian patients with 200 mg (n = 479) Olmesartan 20 mg (n = 8 weeks S/V 200 and 400 mg provided a significantly greater N/A [9]
mild-to-moderate 400 mg 486) reduction in sitting SBP than olmesartan 20 mg at week 8
hypertension (n = 473) (between-treatment difference: −2.33 mmHg or −3.52
mmHg, respectively) Greater reductions in sitting SBP with
S/V were observed in elderly patients, and those with ISH.
Both doses of sacubitril/valsartan provided significantly
greater reductions from baseline in nighttime mean
ambulatory BP vs.
Patients aged 18–75 100 mg (n = 156) Valsartan 80 mg (n = 8 weeks The average reduction in mean sitting DBP across the doses Plasma ANP concentrations increased with all three doses of [10]
years with mild-to- 200 mg 163) of S/V versus the comparator dose of valsartan showed S/V compared with the comparator dose of valsartan
moderate (n = 169) 400 mg 160 mg (n = 166) 320 significantly greater reductions with S/V.
hypertension (n = 172) mg (n = 164) Scubitril
200 mg (n = 165)
Placebo (n = 173)
Asian patients (65 100 mg titrated to Olmeartan 10 mg titrated 14 weeks S/V provided superior sitting SBP reductions vs. olmesartan N/A [11]
years) with systolic 200 mg after to (22.71 vs. 16.11 mmHg, respectively); similarly, reductions
hypertension 4 weeks. Up-titrated 20 mg after 4 weeks. from baseline in other BP and PP assessments were
to 400 mg for Up-titrated to 40 mg for significantly greater with sacubitril/valsartan. At week 14,
patients with patients with BP > 140/ despite more patients requiring up-titration in the olmesartan
BP > 140/90 mm Hg 90 mm Hg at 10 weeks group, sitting BP and sitting PP reductions from baseline
at 10 weeks (n = (n = 292) were significantly greater with S/V.
296)
Older patients with 200 mg titrated to Olmeartan 20 mg titrated 12 weeks for titration At week 12, reductions were significantly greater with S/V in The reduction in the mean plasma NT-proBNP from baseline [12]
systolic hypertension 400 mg after 4 weeks to 40 mg after 4 weeks 12 weeks to 52 weeks for central aortic systolic pressure (−3.7 mmHg), central aortic to week 12 was greater in patients treated with S/V (34%)
and pulse pressure (n = 229) (n = 225) add-on treatment with PP (−2.4 mmHg), mean 24-h ambulatory brachial systolic compared with olmesartan (20%). An increase in the urine
>60 mm Hg amlodipine and pressure (−4.1 mmHg) and central aortic systolic pressure cGMP/creatinine ratio was observed at week 52 but not at
(60 years) hydrochlorothiazide (−3.6 mmHg). Differences in 24-h ambulatory pressures week 12 in the S/V-treated patients.
were pronounced during sleep. After 52 weeks, more patients
required add-on antihypertensive therapy with olmesartan
(47%) versus S/V (32%)
Asian patients with 400 mg Valsartan 320 mg Double-blind crossover Compared with valsartan, S/V was associated with greater Compared with valsartan, S/V was associated with a [13]
salt sensitive treatment for 28 days reductions in office and ambulatory BP on day 28 significant increase in natriuresis and diuresis on day 1, but
hypertension not on day 28. Compared with valsartan, S/V significantly
Angiotensin receptor-neprilysin inhibitors: Comprehensive review and implications in hypertension. . .
(>18years) (n = 70) reduced plasma NT-proBNP on day 28.
Patients with mild-to- 400 mg Valsartan (320 mg) 8 weeks There were greater reductions in sitting office SBP and 24-h N/A [14]
moderate systolic alone or valsartan with ambulatory SBP with S/V than with valsartan (−5.7 and
hypertension placebo or 50, 100, 200, −3.4 mmHg, respectively). The SBP reduction with S/V was
or 400 mg sacubitril similar to co-administered free valsartan and sacubitril 200
mg.
Patients with essential 200 mg titrated to Olmeartan 20 mg titrated 12 weeks for single Reductions in SBP were significantly greater with S/V at MRI-based LVMI decreased to a greater extent in the S/V [15]
hypertension stage 1 400 mg after 2 weeks to 40 mg after 2 weeks treatment period 52 weeks but not at 12 weeks. Reduction in Central SBP and group compared to the olmesartan group from baseline to 12
and 2 and elevated (n = 57) (n = 57) 12–52 weeks for add- DBP were not different between S/V and olmesartan at and 52 weeks after adjustment for SBP. The change in aortic
brachial PP on period 12 weeks and 52 weeks. Reductions in central PP was local distensibility and PWV were not different between the
(50 mmHg) significantly greater with S/V at 52 weeks but not at two groups.
12 weeks.
S/V sacubitril/valsartan, BP blood pressure, SBP systolic BP, DBP diastolic BP, ANP atrial natriuretic peptide, BNP brain natriuretic peptide, PP pulse pressure, LVMI left ventricular mass index,
PWV pulse wave velocity
12431244 K. Yamamoto, H. Rakugi
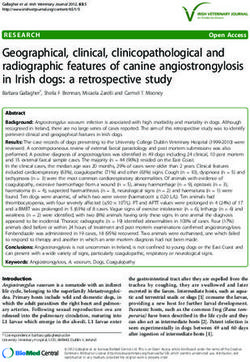
Table 2 The influence of sacubitril/valsartan on cardiovascular increase in eGFR and UACR following treatment with
structures and hemodynamics in patients with hypertension
S/V can be explained by the molecular mechanism of the
Peripheral BP Superior to ARB inhibition of the RAS and the activation of NPs in mod-
24 h-amubulatory BP Superior to ARB (particularly at night) ulating renal hemodynamics [92, 93]. Inhibition of the
Central BP Superior to ARB RAS by valsartan induces dilation of efferent arterioles,
Left ventricular hypertrophy Superior to ARB leading to decreased intraglomerular pressure and GFR. In
Arterial stiffness Equivalent to ARB contrast, NPs predominantly induce dilation of afferent
arterioles, leading to increases in renal perfusion flow and
BP blood pressure, ARB angiotensin II type1 blocker
GFR [94]. Therefore, the increase in the bioavailability of
NPs by sacubitril would contribute to the increase in GFR
Evidence of an influence on renal function along with the increased glomerular filtration of albumin
in patients treated with S/V [92, 93] (Fig. 3). The direct
Renal impairment and hypertension are closely inter- effect of NPs on kidney function, including increased
related, and the protection of renal function is one of the glomerular permeability and blockade of tubular protein
expected roles of antihypertensive medications [82]. It is reabsorption, might also contribute to the increased
of interest to clarify whether ARNIs have an additional UACR induced by S/V [92, 93, 95, 96] In contrast to the
benefit on renal function beyond that provided by classical clear evidence of the renal effect of S/V in HF patients,
RAS inhibitors that are positioned as a first-line therapy in the effect in non-HF patients is not clearly supported by
hypertensive patients with diabetic kidney disease or clinical studies. In the United Kingdom Heart and Renal
nondiabetic kidney disease with proteinuria [83–87]. The Protection (UK HARP)‐III trial, 414 participants with
analysis of RCTs has consistently revealed the specific chronic kidney disease who had an eGFR of 20 to 60 mL/
effect of S/V on renal function in patients with HF who min/1.73 m2 were randomly assigned to S/V 200 mg twice
are at high risk of renal insufficiency [88]. In the daily and irbesartan 300 mg once daily. As a result, there
PARADIGM-HF trial, the decrease in eGFR during was no difference in measured GFR at 12 months of
48 months’ follow-up was less under S/V compared with treatment: 29.8 [SE, 0.5] among participants assigned S/V
enalapril (−1.61 ml/min/1.73 m2/year vs. −2.04 ml/min/ versus 29.9 [SE, 0.5] mL/min/1.73 m2 among those
1.73 m2/year, p < 0.001) despite a modest but greater assigned irbesartan. There was also no significant differ-
increase in urinary albumin/creatinine ratio (UACR) ence in estimated GFR at 3, 6, 9, or 12 months and no
under S/V than enalapril (1.20 mg/mmol vs. 0.90 mg/ clear difference in UACR between treatment arms despite
mmol, p < 0.001) in patients with HFrEF [89]. This see- the greater decline of BP in S/V patients [97]. Never-
mingly paradoxical effect of S/V on eGFR and UACR theless, it should be noted that the relatively short
was consistent with the findings of an RCT named the observation period in this study compared to the clinical
Prospective Comparison of ARNI with ARB on Man- trials for HF might have affected the results [97]. There is
agement Of heart failUre with preserved ejectioN fracTion no previous or ongoing clinical trial to measure the effect
(PARAMOUNT) trial [55]. In this phase II clinical trial of S/V vs. other antihypertensive drugs on long-term renal
where the efficacy of S/V on the reduction of NT-proBNP function in hypertensive patients. It was reported that
was proven in patients with HFpEF in comparison to 8 weeks of treatment with S/V effectively reduced BP,
valsartan, eGFR declined less under S/V than under val- with no clinically meaningful changes in creatinine,
sartan (−1.5 vs. −5.2 mL/min per 1.73 m2; p = 0.002); potassium, blood urea nitrogen, or eGFR, in Japanese
however, UACR increased in the S/V group (2.4–2.9 mg/ patients with hypertension and renal dysfunction (eGFR ≥
mmol), whereas it remained stable in the valsartan group 15 andAngiotensin receptor-neprilysin inhibitors: Comprehensive review and implications in hypertension. . . 1245
Fig. 3 The influence of ARBs or Baseline ARB ARNI
ARNIs on renal hemodynamics vasodilation Intraglomerular Intraglomerular
and function. ARB angiotensin pressure pressure
II receptor blocker, ARNI Efferent artery Afferent artery
angiotensin receptor-neprilysin
inhibitor
glomerular
permeability
Albumin Albumin
excretion excretion
the PARADIGM-HF trial, S/V did not reduce the pre- Interestingly, Jordan et al. indicated that S/V modestly
specified exploratory outcome of new-onset diabetes that increased abdominal subcutaneous adipose tissue lipolysis
occurred in 84 patients during the course of the assessed by glycerol concentration in obese patients with
PARADIGM-HF trial [5, 99]. However, a post hoc analysis hypertension in the above-mentioned study [100], con-
in 3778 patients with known diabetes or an HbA1c ≥ 65% sistent with the findings that NPs promote lipid mobiliza-
at screening showed a certain benefit of S/V on glycemic tion and oxidation in humans [103, 104]. In contrast, the
control [99]. HbA1c levels were lower in the S/V group same group reported that S/V did not affect exercise-
than in the enalapril group over the 3-year follow-up induced lipolysis or substrate oxidation compared to
(between-group reduction 0.14%, 95% CI 0.06–0.23, p = amlodipine in obese patients with hypertension [105]. They
0.0055), while the degree of the reduction was modest in also reported that S/V treatment for 8 weeks did not alter
both groups (0.16% (SD 1.40) in the enalapril group and the abdominal subcutaneous adipose tissue transcriptome
0.26% (SD 1.25) in the S/V group during the first year of or the expression of proteins involved in lipolysis, NP
follow-up). The new use of insulin was 29% lower in signaling, or oxidative metabolism in obese hypertensive
patients receiving S/V (114 [7%] patients) than in patients patients [106]. Therefore, further investigation is required
receiving enalapril (153 [10%]; hazard ratio 0.71, 95% CI to elucidate whether and how S/V mediates clinically
0.56–0.90, p = 0.0052) [99]. The effect of S/V on glycemic relevant adipose tissue lipolysis. NP-independent pathways
control was not assessed in other large-scale RCTs in could involve the restoration of other neprilysin-targeted
patients with HF. Jordan et al. reported that S/V improved peptides, including glucagon-like peptide-1 (GLP-1), bra-
insulin sensitivity compared to amlodipine in patients with dykinin, insulin-B chain, and vasoactive intestinal poly-
obesity and hypertension [100]. In this study, 8 weeks of peptide (VIP), which potentially contribute to improved
treatment with 400 mg S/V (n = 50) but not amlodipine glycemic control [102] (Fig. 2). Indeed, it was reported that
(n = 48) increased the insulin sensitivity index, as assessed S/V increased plasma GLP-1 concentrations in patients
by the hyperinsulinemic euglycemic glucose clamp without with HF [107, 108].
any alteration in body weight. The molecular mechanisms Moreover, S/V was reported to decrease plasma uric acid
by which neprilysin inhibition improves glucose metabo- concentration in patients with HF in the PARADIGM-HF
lism could involve NP-dependent and independent path- and PARAGON-HF trials [109, 110]. Nevertheless, it is
ways, though clinical data to directly support this remains conceivable that the favorable influence of S/V on uric acid
insufficient (Fig. 2). Epidemiological studies have shown is attributed not to the direct effect on uric acid but to the
that increased levels of NPs or genetic variants associated indirect effect via the improvement of HF control
with the increased production of NPs are associated with a [109, 110]. There is no evidence that S/V alters the plasma
reduced risk of new-onset diabetes [101, 102]. Although uric acid concentration in hypertensive patients. Regarding
the molecular mechanisms that could directly explain the the effect of ARNIs on plasma lipid profile, little evidence is
favorable relationship between NPs and glycemic control available except from the PARAGIGM-HF trial, in which
remain to be elucidated, basic studies have suggested that S/V modestly increased HDL cholesterol by 0.02 mmol/L
NPs have various metabolic actions in organs, including compared with enalapril without alterations in LDL or tri-
the liver, skeletal muscles, and adipose tissues [101]. glyceride levels.1246 K. Yamamoto, H. Rakugi
Evidence of a potential influence on reduce BP and ameliorate cardiac remodeling raises the
cognitive function possibility of utilizing ARNIs in the treatment of patients
with hypertension in real-world clinical practice. The excel-
Finally, it should be noted that amyloid β (Aβ) peptides are lent antihypertensive effect of the ARNI over conventional
substrates of neprilysin, and neprilysin inhibitors theoreti- RAS inhibitors is attributed to the NP-induced natriuretic
cally increase Aβ concentrations, raising the concern that effect that could also contribute to normalization of the cir-
long-term neprilysin inhibition might induce Aβ accumu- cadian rhythm of BP in hypertensive patients. Nevertheless,
lation, a central etiology of Alzheimer’s disease (AD) [25] it is desirable to discover the superior clinical benefits of
(Fig. 2). In a human study, 14 days of treatment with S/V in ARNI over pre-existing antihypertensive drug classes in
healthy volunteers increased nonpathologic, soluble Aβ treating hypertension beyond its effect on lowering BP. In
1–38 by 42%, but not aggregable, pathologic Aβ forms Aβ this context, the potential BP-independent effects of NPs and
1–40 and Aβ 1–42 in cerebrospinal fluid (CSF) compared to other substrates modulated by neprilysin inhibition on organ
placebo [111]. Schoenfeld et al. reported that S/V impaired protection have been suggested by a variety of basic studies
the clearance of Aβ1–42, Aβ1–40, and Aβ1–38 compared to and clinical trials of HF. Particularly, it is important to clarify
valsartan on day 1 but not on day 15 of consecutive oral whether the beneficial effects of ARNIs on renal function and
administration in cynomolgus monkeys, whereas S/V glycemic control in patients with HF are clinically relevant in
increased newly generated Aβ forms in CSF on days 1 and the treatment of hypertension. Finally, given the lifelong
15 [112]. They also showed that 39 weeks of treatment with duration of hypertension treatment, further investigations are
S/V revealed no evidence of brain Aβ deposition in the necessary to eliminate the possibility that ARNIs contribute
cynomolgus monkey [112]. to the development of dementia.
In the PARADIGM-HF trial, there was no evidence that
S/V increased dementia-related adverse effects (AEs) Acknowledgements We thank Hiroko Yamamoto for the creation of
the illustrations in Fig. 3.
compared to enalapril, and the incidence of AEs was similar
to that in other recent trials on HFrEF [113]. An ongoing
Author contributions KY wrote the manuscript. HR gave advice on
clinical trial is planned to investigate the effect of S/V writing the manuscript.
compared to valsartan on cognitive function in patients with
HFpEF for 3 years using a comprehensive battery of tests Compliance with ethical standards
that evaluate longitudinal changes in cognitive domains,
including memory, executive function, and attention [114]. Conflict of interest KY received lecture fees from Daiichi Sankyo
In terms of hypertension, the effect of antihypertensive unrelated to the submitted work. HR received lecture fees from Daiichi
Sankyo Co Ltd., Takeda Pharmaceutical Co Ltd., and MSD unrelated
treatment on cognitive function remains controversial, as
to the submitted work. KY and HR received grants from Astellas
suggested by the study where active treatment modestly Pharma, Bayer Yakuhin, Daiichi Sankyo, Dainippon Sumitomo
decreased incident dementia not in an independent analysis Pharma, Kyowa Hakko Kirin, Mitsubishi Tanabe Pharma, Mochida
but in a meta-analysis of placebo-controlled RCTs of Pharmaceutical, MSD, Nippon Boehringer Ingelheim, Novartis
Pharma, Sanofi, Takeda Pharmaceutical, and Teijin Pharma unrelated
hypertension [115]. In addition, in the subanalysis of the
to the submitted work.
Systolic Blood Pressure Intervention Trial, although inci-
dent dementia did not significantly differ between intensive Publisher’s note Springer Nature remains neutral with regard to
(target systolic BP < 120 mmHg) and standard anti- jurisdictional claims in published maps and institutional affiliations.
hypertensive treatment arms (target systolic BP < 140
mmHg), the incidence of mild cognitive impairment was References
more frequently observed in patients given the standard
treatment [116]. Therefore, the long-term effect of ARNIs 1. Shimokawa H, Miura M, Nochioka K, Sakata Y. Heart
failure as a general pandemic in Asia. Eur J Heart Fail. 2015;
on cognitive function needs to be clarified by carefully 17:884–92.
considering several factors that could potentially influence 2. Savarese G, Lund LH. Global public health burden of heart
cognitive function in hypertensive patients. failure. Card Fail Rev. 2017;3:7–11.
3. Zannad F, Ferreira JP, Pocock SJ, Anker SD, Butler J, Filippatos
G, et al. SGLT2 inhibitors in patients with heart failure with
reduced ejection fraction: a meta-analysis of the EMPEROR-
Perspective reduced and DAPA-HF trials. Lancet 2020;396:819–29.
4. Ide T, Ohtani K, Higo T, Tanaka M, Kawasaki Y, Tsutsui H.
Given the obvious clinical benefits of S/V shown in clinical Ivabradine for the treatment of cardiovascular diseases. Circ J.
2019;83:252–60.
trials, recent clinical guidelines for HF have positioned this
5. McMurray JJ, Packer M, Desai AS, Gong J, Lefkowitz MP,
ARNI as a first-line treatment choice in patients with HFrEF Rizkala AR, et al. Angiotensin-neprilysin inhibition versus
[117, 118]. In addition, the excellent capacity of S/V to enalapril in heart failure. N Engl J Med. 2014;371:993–1004.Angiotensin receptor-neprilysin inhibitors: Comprehensive review and implications in hypertension. . . 1247
6. Velazquez EJ, Morrow DA, DeVore AD, Duffy CI, Ambrosy subsequently to angiotensin-receptor/neprilysin-inhibitor treat-
AP, McCague K, et al. Angiotensin-neprilysin inhibition in acute ment in chronic systolic heart failure. Br J Clin Pharm.
decompensated heart failure. N Engl J Med. 2019;380:539–48. 2021;87:916–24.
7. Solomon SD, Vaduganathan M, Claggett BL, Packer M, Zile M, 25. Poorgolizadeh E, Homayouni Moghadam F, Dormiani K, Rezaei
Swedberg K. et al. Sacubitril/valsartan across the spectrum of N, Nasr-Esfahani MH. Do neprilysin inhibitors walk the line?
ejection fraction in heart failure. Circulation . 2020;141:352–61. Heart ameliorative but brain threatening! Eur J Pharm.
8. Cheung DG, Aizenberg D, Gorbunov V, Hafeez K, Chen CW, 2021;894:173851.
Zhang J. Efficacy and safety of sacubitril/valsartan in patients 26. Nakagawa Y, Nishikimi T, Kuwahara K. Atrial and brain
with essential hypertension uncontrolled by olmesartan: a ran- natriuretic peptides: hormones secreted from the heart. Peptides
domized, double-blind, 8-week study. J Clin Hypertens. 2019;111:18–25.
2018;20:150–8. 27. Sarzani R, Spannella F, Giulietti F, Balietti P, Cocci G, Bor-
9. Huo Y, Li W, Webb R, Zhao L, Wang Q, Guo W. Efficacy and dicchia M. Cardiac natriuretic peptides. Hypertens Cardiovasc
safety of sacubitril/valsartan compared with olmesartan in Asian Risk High Blood Press Cardiovasc Prev. 2017;24:115–26.
patients with essential hypertension: a randomized, double-blind, 28. Prickett TC, Circulating EAE. products of C-type natriuretic
8-week study. J Clin Hypertens. 2019;21:67–76. peptide and links with organ function in health and disease.
10. Ruilope LM, Dukat A, Bohm M, Lacourciere Y, Gong J, Lef- Peptides 2020;132:170363.
kowitz MP. Blood-pressure reduction with LCZ696, a novel 29. Moyes AJ, Hobbs AJ. C-type natriuretic peptide: a multifaceted
dual-acting inhibitor of the angiotensin II receptor and neprily- paracrine regulator in the heart and vasculature. Int J Mol Sci.
sin: a randomised, double-blind, placebo-controlled, active 2019;20:9.
comparator study. Lancet 2010;375:1255–66. 30. Hodes A, Lichtstein D. Natriuretic hormones in brain function.
11. Supasyndh O, Wang J, Hafeez K, Zhang Y, Zhang J, Rakugi H. Front Endocrinol. 2014;5:201.
Efficacy and safety of sacubitril/valsartan (LCZ696) compared 31. Kostis JB, Packer M, Black HR, Schmieder R, Henry D, Levy E.
with olmesartan in elderly Asian patients (>/=65 years) with Omapatrilat and enalapril in patients with hypertension: the
systolic hypertension. Am J Hypertens. 2017;30:1163–9. omapatrilat cardiovascular treatment vs. enalapril (OCTAVE)
12. Williams B, Cockcroft JR, Kario K, Zappe DH, Brunel PC, trial. Am J Hypertens. 2004;17:103–11.
Wang Q, et al. Effects of sacubitril/valsartan versus olmesartan 32. Packer M, Califf RM, Konstam MA, Krum H, McMurray JJ,
on central hemodynamics in the elderly with systolic hyperten- Rouleau JL, et al. Comparison of omapatrilat and enalapril in
sion: the PARAMETER study. Hypertension 2017;69:411–20. patients with chronic heart failure: the Omapatrilat Versus Ena-
13. Wang TD, Tan RS, Lee HY, Ihm SH, Rhee MY, Tomlinson B, lapril Randomized Trial of Utility in Reducing Events (OVER-
et al. Effects of sacubitril/valsartan (LCZ696) on natriuresis, TURE). Circulation 2002;106:920–6.
diuresis, blood pressures, and NT-proBNP in salt-sensitive 33. Rouleau JL, Pfeffer MA, Stewart DJ, Isaac D, Sestier F, Kerut
hypertension. Hypertension 2017;69:32–41. EK, et al. Comparison of vasopeptidase inhibitor, omapatrilat,
14. Izzo JL Jr, Zappe DH, Jia Y, Hafeez K, Zhang J. Efficacy and and lisinopril on exercise tolerance and morbidity in patients
safety of crystalline valsartan/sacubitril (LCZ696) compared with heart failure: IMPRESS randomised trial. Lancet
with placebo and combinations of free valsartan and sacubitril in 2000;356:615–20.
patients with systolic hypertension: the RATIO study. J Cardi- 34. Packer M, McMurray JJ, Desai AS, Gong J, Lefkowitz MP,
ovasc Pharm. 2017;69:374–81. Rizkala AR, et al. Angiotensin receptor neprilysin inhibition
15. Schmieder RE, Wagner F, Mayr M, Delles C, Ott C, Keicher C, compared with enalapril on the risk of clinical progression in
et al. The effect of sacubitril/valsartan compared to olmesartan surviving patients with heart failure. Circulation
on cardiovascular remodelling in subjects with essential hyper- 2015;131:54–61.
tension: the results of a randomized, double-blind, active- 35. Okumura N, Jhund PS, Gong J, Lefkowitz MP, Rizkala AR,
controlled study. Eur Heart J. 2017;38:3308–17. Rouleau JL, et al. Importance of clinical worsening of heart
16. Campbell DJ. Long-term neprilysin inhibition—implications for failure treated in the outpatient setting: evidence from the pro-
ARNIs. Nat Rev Cardiol. 2017;14:171–86. spective comparison of ARNI With ACEI to determine impact
17. Kario K. The sacubitril/valsartan, a first-in-class, angiotensin on global mortality and morbidity in heart failure trial (PARA-
receptor neprilysin inhibitor (ARNI): potential uses in hyper- DIGM-HF). Circulation 2016;133:2254–62.
tension, heart failure, and beyond. Curr Cardiol Rep. 2018;20:5 36. Desai AS, Claggett BL, Packer M, Zile MR, Rouleau JL,
18. Jhund PS, McMurray JJ. The neprilysin pathway in heart failure: Swedberg K, et al. Influence of sacubitril/valsartan (LCZ696) on
a review and guide on the use of sacubitril/valsartan. Heart 30-day readmission after heart failure hospitalization. J Am Coll
2016;102:1342–7. Cardiol. 2016;68:241–8.
19. D’Elia E, Iacovoni A, Vaduganathan M, Lorini FL, Perlini S, 37. Mogensen UM, Gong J, Jhund PS, Shen L, Kober L, Desai AS,
Senni M. Neprilysin inhibition in heart failure: mechanisms and et al. Effect of sacubitril/valsartan on recurrent events in the
substrates beyond modulating natriuretic peptides. Eur J Heart prospective comparison of ARNI with ACEI to determine impact
Fail. 2017;19:710–7. on global mortality and morbidity in heart failure trial (PARA-
20. Packer M. Augmentation of glucagon-like peptide-1 receptor DIGM-HF). Eur J Heart Fail. 2018;20:760–8.
signalling by neprilysin inhibition: potential implications for 38. Chandra A, Lewis EF, Claggett BL, Desai AS, Packer M, Zile
patients with heart failure. Eur J Heart Fail. 2018;20:973–7. MR, et al. Effects of sacubitril/valsartan on physical and social
21. Campbell DJ. Neprilysin inhibitors and bradykinin. Front Med. activity limitations in patients with heart failure: a secondary
2018;5:257. analysis of the PARADIGM-HF trial. JAMA Cardiol.
22. Esser N, Zraika S. Neprilysin inhibitors and angiotensin(1-7) in 2018;3:498–505.
COVID-19. Br J Cardiol. 2020;27:109–11. 39. Desai AS, McMurray JJ, Packer M, Swedberg K, Rouleau JL,
23. Roksnoer LCW, Uijl E, de Vries R, Garrelds IM, Jan Danser Chen F, et al. Effect of the angiotensin-receptor-neprilysin
AH. Neprilysin inhibition and endothelin-1 elevation: focus on inhibitor LCZ696 compared with enalapril on mode of death in
the kidney. Eur J Pharm. 2018;824:128–32. heart failure patients. Eur Heart J. 2015;36:1990–7.
24. Arfsten H, Goliasch G, Bartko PE, Prausmuller S, Spinka G, Cho 40. Jhund PS, Fu M, Bayram E, Chen CH, Negrusz-Kawecka M,
A, et al. Increased concentrations of bioactive adrenomedullin Rosenthal A, et al. Efficacy and safety of LCZ696 (sacubitril-1248 K. Yamamoto, H. Rakugi
valsartan) according to age: insights from PARADIGM-HF. Eur 54. Ambrosy AP, Braunwald E, Morrow DA, DeVore AD, McCa-
Heart J. 2015;36:2576–84. gue K, Meng X, et al. Angiotensin receptor-neprilysin inhibition
41. Simpson J, Jhund PS, Silva Cardoso J, Martinez F, Mosterd A, based on history of heart failure and use of renin-angiotensin
Ramires F, et al. Comparing LCZ696 with enalapril according to system antagonists. J Am Coll Cardiol. 2020;76:1034–48.
baseline risk using the MAGGIC and EMPHASIS-HF risk 55. Solomon SD, Zile M, Pieske B, Voors A, Shah A, Kraigher-
scores: an analysis of mortality and morbidity in PARADIGM- Krainer E, et al. The angiotensin receptor neprilysin inhibitor
HF. J Am Coll Cardiol. 2015;66:2059–71. LCZ696 in heart failure with preserved ejection fraction: a phase
42. Solomon SD, Claggett B, Desai AS, Packer M, Zile M, Swed- 2 double-blind randomised controlled trial. Lancet
berg K, et al. Influence of ejection fraction on outcomes and 2012;380:1387–95.
efficacy of sacubitril/valsartan (LCZ696) in heart failure with 56. Solomon SD, McMurray JJV, Anand IS, Ge J, Lam CSP,
reduced ejection fraction: the prospective comparison of ARNI Maggioni AP, et al. Angiotensin-neprilysin inhibition in heart
with ACEI to determine impact on global mortality and mor- failure with preserved ejection fraction. N Engl J Med.
bidity in heart failure (PARADIGM-HF) trial. Circ Heart Fail. 2019;381:1609–20.
2016;9:e002744. 57. McMurray JJV, Jackson AM, Lam CSP, Redfield MM, Anand
43. Zile MR, Claggett BL, Prescott MF, McMurray JJ, Packer M, IS, Ge J, et al. Effects of sacubitril-valsartan versus valsartan in
Rouleau JL, et al. Prognostic implications of changes in N- women compared with men with heart failure and preserved
terminal Pro-B-type natriuretic peptide in patients with heart ejection fraction: insights from PARAGON-HF. Circulation
failure. J Am Coll Cardiol. 2016;68:2425–36. 2020;141:338–51.
44. Kristensen SL, Preiss D, Jhund PS, Squire I, Cardoso JS, Mer- 58. Selvaraj S, Claggett BL, Bohm M, Anker SD, Vaduganathan M,
kely B, et al. Risk related to pre-diabetes mellitus and diabetes Zannad F, et al. Systolic blood pressure in heart failure with
mellitus in heart failure with reduced ejection fraction: insights preserved ejection fraction treated with sacubitril/valsartan. J Am
from prospective comparison of ARNI with ACEI to determine Coll Cardiol. 2020;75:1644–56.
impact on global mortality and morbidity in heart failure trial. 59. Vaduganathan M, Claggett BL, Desai AS, Anker SD, Perrone
Circ Heart Fail. 2016;9:1. SV, Janssens S, et al. Prior heart failure hospitalization, clinical
45. Solomon SD, Claggett B, Packer M, Desai A, Zile MR, Swed- outcomes, and response to sacubitril/valsartan compared with
berg K, et al. Efficacy of sacubitril/valsartan relative to a prior valsartan in HFpEF. J Am Coll Cardiol. 2020;75:245–54.
decompensation: the PARADIGM-HF trial. JACC Heart Fail. 60. Cunningham JW, Vaduganathan M, Claggett BL, Zile MR,
2016;4:816–22. Anand IS, Packer M, et al. Effects of sacubitril/valsartan on N-
46. Okumura N, Jhund PS, Gong J, Lefkowitz MP, Rizkala AR, terminal Pro-B-type natriuretic peptide in heart failure with
Rouleau JL, et al. Effects of sacubitril/valsartan in the preserved ejection fraction. JACC Heart Fail. 2020;8:372–81.
PARADIGM-HF trial (prospective comparison of ARNI with 61. Kario K, Tamaki Y, Okino N, Gotou H, Zhu M, Zhang J.
ACEI to determine impact on global mortality and morbidity in LCZ696, a first-in-class angiotensin receptor-neprilysin inhibitor:
heart failure) according to background therapy. Circ Heart Fail. the first clinical experience in patients with severe hypertension.
2016;9:9. J Clin Hypertens. 2016;18:308–14.
47. Bohm M, Young R, Jhund PS, Solomon SD, Gong J, Lefkowitz 62. Kario K, Sun N, Chiang FT, Supasyndh O, Baek SH, Inubushi-
MP, et al. Systolic blood pressure, cardiovascular outcomes and Molessa A, et al. Efficacy and safety of LCZ696, a first-in-class
efficacy and safety of sacubitril/valsartan (LCZ696) in patients angiotensin receptor neprilysin inhibitor, in Asian patients with
with chronic heart failure and reduced ejection fraction: results hypertension: a randomized, double-blind, placebo-controlled
from PARADIGM-HF. Eur Heart J. 2017;38:1132–43. study. Hypertension 2014;63:698–705.
48. Vardeny O, Claggett B, Kachadourian J, Pearson SM, Desai AS, 63. Li Q, Li L, Wang F, Zhang W, Guo Y, Wang F, et al. Effect and
Packer M, et al. Incidence, predictors, and outcomes associated safety of LCZ696 in the treatment of hypertension: a meta-
with hypotensive episodes among heart failure patients receiving analysis of 9 RCT studies. Medicine. 2019;98:e16093.
sacubitril/valsartan or enalapril: the PARADIGM-HF trial (pro- 64. De Vecchis R, Soreca S, Ariano C. Anti-hypertensive effect of
spective comparison of angiotensin receptor neprilysin inhibitor sacubitril/valsartan: a meta-analysis of randomized controlled
with angiotensin-converting enzyme inhibitor to determine trials. Cardiol Res. 2019;10:24–33.
impact on global mortality and morbidity in heart failure). Circ 65. Geng Q, Yan R, Wang Z, Hou F. Effects of LCZ696 (sacubitril/
Heart Fail. 2018;11:e004745. valsartan) on blood pressure in patients with hypertension: a
49. Vardeny O, Claggett B, Packer M, Zile MR, Rouleau J, Swed- meta-analysis of randomized controlled trials. Cardiology
berg K, et al. Efficacy of sacubitril/valsartan vs. enalapril at 2020;145:589–98.
lower than target doses in heart failure with reduced ejection 66. Kurtz TW, Dominiczak AF, DiCarlo SE, Pravenec M, Morris
fraction: the PARADIGM-HF trial. Eur J Heart Fail. RC Jr. Molecular-based mechanisms of Mendelian forms of salt-
2016;18:1228–34. dependent hypertension: questioning the prevailing theory.
50. Kristensen SL, Martinez F, Jhund PS, Arango JL, Belohlavek J, Hypertension 2015;65:932–41.
Boytsov S, et al. Geographic variations in the PARADIGM-HF 67. John SW, Krege JH, Oliver PM, Hagaman JR, Hodgin JB, Pang
heart failure trial. Eur Heart J. 2016;37:3167–74. SC, et al. Genetic decreases in atrial natriuretic peptide and salt-
51. Balmforth C, Simpson J, Shen L, Jhund PS, Lefkowitz M, sensitive hypertension. Science 1995;267:679–81.
Rizkala AR, et al. Outcomes and effect of treatment according to 68. Rubattu S, Calvieri C, Pagliaro B, Volpe M. Atrial natriuretic
etiology in HFrEF: an analysis of PARADIGM-HF. JACC Heart peptide and regulation of vascular function in hypertension and
Fail. 2019;7:457–65. heart failure: implications for novel therapeutic strategies. J
52. Sbolli M, deFilippi C. BNP and NT-proBNP interpretation in the Hypertens. 2013;31:1061–72.
neprilysin inhibitor era. Curr Cardiol Rep. 2020;22:150. 69. Volpe M, Rubattu S, Burnett J Jr. Natriuretic peptides in cardi-
53. Morrow DA, Velazquez EJ, DeVore AD, Desai AS, Duffy CI, ovascular diseases: current use and perspectives. Eur Heart J.
Ambrosy AP, et al. Clinical outcomes in patients with acute 2014;35:419–25.
decompensated heart failure randomly assigned to sacubitril/ 70. Yano Y, Kario K. Nocturnal blood pressure and cardiovascular
valsartan or enalapril in the PIONEER-HF trial. Circulation disease: a review of recent advances. Hypertens Res.
2019;139:2285–8. 2012;35:695–701.Angiotensin receptor-neprilysin inhibitors: Comprehensive review and implications in hypertension. . . 1249
71. Uzu T, Kimura G. Diuretics shift circadian rhythm of blood angiotensin-neprilysin inhibition in heart failure. JACC Heart
pressure from nondipper to dipper in essential hypertension. Fail. 2018;6:489–98.
Circulation 1999;100:1635–8. 90. Voors AA, Gori M, Liu LC, Claggett B, Zile MR, Pieske B, et al.
72. Hughes AD, Nielsen H, Sever PS. The effect of atrial natriuretic Renal effects of the angiotensin receptor neprilysin inhibitor
peptide on human isolated resistance arteries. Br J Pharm. LCZ696 in patients with heart failure and preserved ejection
1989;97:1027–30. fraction. Eur J Heart Fail. 2015;17:510–7.
73. Melo LG, Veress AT, Ackermann U, Sonnenberg H. Chronic 91. Mc Causland FR, Lefkowitz MP, Claggett B, Anavekar NS,
regulation of arterial blood pressure by ANP: role of endogenous Senni M, Gori M, et al. Angiotensin-neprilysin inhibition and
vasoactive endothelial factors. Am J Physiol. 1998;275: renal outcomes in heart failure with preserved ejection fraction.
H1826–1833. Circulation 2020;142:1236–45.
74. Bolli P, Muller FB, Linder L, Raine AE, Resink TJ, Erne P, et al. 92. Pontremoli R, Borghi C, Filardi PP. Renal protection in chronic
The vasodilator potency of atrial natriuretic peptide in man. heart failure: focus on sacubitril/valsartan. Eur Heart J Cardiovasc
Circulation 1987;75:221–8. Pharmacother. 2021. https://doi.org/10.1093/ehjcvp/pvab030.
75. O’Rourke M. Arterial stiffness, systolic blood pressure, and 93. Tersalvi G, Dauw J, Martens P, Mullens W. Impact of sacubitril-
logical treatment of arterial hypertension. Hypertension valsartan on markers of glomerular function. Curr Heart Fail
1990;15:339–47. Rep. 2020;17:145–52.
76. Izzo JL Jr. Arterial stiffness and the systolic hypertension syn- 94. Nishikimi T, Maeda N, Matsuoka H. The role of natriuretic
drome. Curr Opin Cardiol. 2004;19:341–52. peptides in cardioprotection. Cardiovasc Res. 2006;69:318–28.
77. Roman MJ, Devereux RB, Kizer JR, Lee ET, Galloway JM, Ali 95. Jacobs EM, Vervoort G, Branten AJ, Klasen I, Smits P, Wetzels
T, et al. Central pressure more strongly relates to vascular disease JF. Atrial natriuretic peptide increases albuminuria in type I
and outcome than does brachial pressure: the Strong Heart Study. diabetic patients: evidence for blockade of tubular protein reab-
Hypertension 2007;50:197–203. sorption. Eur J Clin Investig. 1999;29:109–15.
78. Muiesan ML, Salvetti M, Monteduro C, Bonzi B, Paini A, Viola 96. Theilig F, Wu Q. ANP-induced signaling cascade and its
S, et al. Left ventricular concentric geometry during treatment implications in renal pathophysiology. Am J Physiol Ren Phy-
adversely affects cardiovascular prognosis in hypertensive siol. 2015;308:F1047–1055.
patients. Hypertension 2004;43:731–8. 97. Haynes R, Judge PK, Staplin N, Herrington WG, Storey BC,
79. Koren MJ, Devereux RB, Casale PN, Savage DD, Laragh JH. Bethel A, et al. Effects of sacubitril/valsartan versus irbesartan in
Relation of left ventricular mass and geometry to morbidity and patients with chronic kidney disease. Circulation
mortality in uncomplicated essential hypertension. Ann Intern 2018;138:1505–14.
Med. 1991;114:345–52. 98. Ito S, Satoh M, Tamaki Y, Gotou H, Charney A, Okino N, et al.
80. Sutton-Tyrrell K, Najjar SS, Boudreau RM, Venkitachalam L, Safety and efficacy of LCZ696, a first-in-class angiotensin
Kupelian V, Simonsick EM, et al. Elevated aortic pulse wave receptor neprilysin inhibitor, in Japanese patients with hyper-
velocity, a marker of arterial stiffness, predicts cardiovascular tension and renal dysfunction. Hypertens Res. 2015;38:269–75.
events in well-functioning older adults. Circulation 99. Seferovic JP, Claggett B, Seidelmann SB, Seely EW, Packer M,
2005;111:3384–90. Zile MR, et al. Effect of sacubitril/valsartan versus enalapril on
81. Desai AS, Solomon SD, Shah AM, Claggett BL, Fang JC, Izzo J, glycaemic control in patients with heart failure and diabetes: a
et al. Effect of sacubitril-valsartan vs enalapril on aortic stiffness post-hoc analysis from the PARADIGM-HF trial. Lancet Dia-
in patients with heart failure and reduced ejection fraction: a betes Endocrinol. 2017;5:333–40.
randomized clinical trial. JAMA. 2019;1–10. https://doi.org/10. 100. Jordan J, Stinkens R, Jax T, Engeli S, Blaak EE, May M, et al.
1001/jama.2019.12843. Improved insulin sensitivity with angiotensin receptor neprilysin
82. Adamczak M, Zeier M, Dikow R, Ritz E. Kidney and hyper- inhibition in individuals with obesity and hypertension. Clin
tension. Kidney Int Suppl 2002;62–7. https://doi.org/10.1046/j. Pharm Ther. 2017;101:254–63.
1523-1755.61.s80.28.x. 101. Coue M, Moro C. Natriuretic peptide control of energy balance
83. Kidney Disease: Improving Global Outcomes Diabetes Work G. and glucose homeostasis. Biochimie 2016;124:84–91.
KDIGO 2020 clinical practice guideline for diabetes manage- 102. Seferovic JP, Solomon SD, Seely EW. Potential mechanisms of
ment in chronic kidney disease. Kidney Int. 2020;98:S1–S115. beneficial effect of sacubitril/valsartan on glycemic control. Ther
84. Kidney Disease: Improving Global Outcomes Blood Pressure Adv Endocrinol Metab. 2020;11:2042018820970444.
Work G. KDIGO 2021 clinical practice guideline for the man- 103. Birkenfeld AL, Boschmann M, Moro C, Adams F, Heusser K,
agement of blood pressure in chronic kidney disease. Kidney Int. Franke G, et al. Lipid mobilization with physiological atrial
2021;99:S1–S87. natriuretic peptide concentrations in humans. J Clin Endocrinol
85. Taal MW, Brenner BM. Renoprotective benefits of RAS inhi- Metab. 2005;90:3622–8.
bition: from ACEI to angiotensin II antagonists. Kidney Int. 104. Birkenfeld AL, Budziarek P, Boschmann M, Moro C, Adams F,
2000;57:1803–17. Franke G, et al. Atrial natriuretic peptide induces postprandial
86. Xie X, Liu Y, Perkovic V, Li X, Ninomiya T, Hou W, et al. lipid oxidation in humans. Diabetes 2008;57:3199–204.
Renin–angiotensin system inhibitors and kidney and cardiovas- 105. Engeli S, Stinkens R, Heise T, May M, Goossens GH, Blaak EE,
cular outcomes in patients with CKD: a Bayesian network meta- et al. Effect of sacubitril/valsartan on exercise-induced lipid
analysis of randomized clinical trials. Am J Kidney Dis. metabolism in patients with obesity and hypertension. Hyper-
2016;67:728–41. tension 2018;71:70–77.
87. Ruggenenti P, Cravedi P, Remuzzi G. Mechanisms and treatment 106. Stinkens R, van der Kolk BW, Jordan J, Jax T, Engeli S, Heise T,
of CKD. J Am Soc Nephrol. 2012;23:1917–28. et al. The effects of angiotensin receptor neprilysin inhibition by
88. McAlister FA, Ezekowitz J, Tonelli M, Armstrong PW. Renal sacubitril/valsartan on adipose tissue transcriptome and protein
insufficiency and heart failure: prognostic and therapeutic expression in obese hypertensive patients. Sci Rep. 2018;8:3933.
implications from a prospective cohort study. Circulation 107. Nougue H, Pezel T, Picard F, Sadoune M, Arrigo M, Beauvais F,
2004;109:1004–9. et al. Effects of sacubitril/valsartan on neprilysin targets and the
89. Damman K, Gori M, Claggett B, Jhund PS, Senni M, Lefkowitz metabolism of natriuretic peptides in chronic heart failure: a
MP, et al. Renal effects and associated outcomes during mechanistic clinical study. Eur J Heart Fail. 2019;21:598–605.1250 K. Yamamoto, H. Rakugi
108. Vodovar N, Nougue H, Launay JM, Solal AC, Logeart D. 114. Efficacy and safety of LCZ696 compared to valsartan on cog-
Sacubitril/valsartan in PARADIGM-HF. Lancet Diabetes Endo- nitive function in patients with chronic heart failure and pre-
crinol. 2017;5:495–6. served ejection fraction (PERSPECTIVE). ClinicalTrials.gov
109. Mogensen UM, Kober L, Jhund PS, Desai AS, Senni M, Kris- Identifier: NCT02884206
tensen SL, et al. Sacubitril/valsartan reduces serum uric acid 115. Peters R, Beckett N, Forette F, Tuomilehto J, Clarke R, Ritchie
concentration, an independent predictor of adverse outcomes in C. et al. Incident dementia and blood pressure lowering in the
PARADIGM-HF. Eur J Heart Fail. 2018;20:514–22. Hypertension in the Very Elderly Trial cognitive function
110. Selvaraj S, Claggett BL, Pfeffer MA, Desai AS, Mc Causland assessment (HYVET-COG): a double-blind, placebo controlled
FR, McGrath MM, et al. Serum uric acid, influence of sacubitril- trial. Lancet Neurol. 2008;7:683–689.
valsartan, and cardiovascular outcomes in heart failure with 116. Group SMIftSR, Williamson JD, Pajewski NM, Auchus AP,
preserved ejection fraction: PARAGON-HF. Eur J Heart Fail. Bryan RN, Chelune G, et al. Effect of intensive vs standard
2020;22:2093–101. blood pressure control on probable dementia: a randomized
111. Langenickel TH, Tsubouchi C, Ayalasomayajula S, Pal P, clinical trial. JAMA 2019;321:553–61.
Valentin MA, Hinder M, et al. The effect of LCZ696 (sacu- 117. Writing C, Maddox TM, Januzzi JL, Jr, Allen LA, Breathett K,
bitril/valsartan) on amyloid-beta concentrations in cere- Butler J, et al. 2021 Update to the 2017 ACC expert consensus
brospinal fluid in healthy subjects. Br J Clin Pharm. decision pathway for optimization of heart failure treatment:
2016;81:878–90. answers to 10 pivotal issues about heart failure with reduced
112. Schoenfeld HA, West T, Verghese PB, Holubasch M, Shenoy N, ejection fraction: a report of the American College of Cardiology
Kagan D, et al. The effect of angiotensin receptor neprilysin Solution Set Oversight Committee. J Am Coll Cardiol.
inhibitor, sacubitril/valsartan, on central nervous system 2021;77:772–810.
amyloid-beta concentrations and clearance in the cynomolgus 118. Seferovic PM, Ponikowski P, Anker SD, Bauersachs J, Chioncel
monkey. Toxicol Appl Pharm. 2017;323:53–65. O, Cleland JGF, et al. Clinical practice update on heart failure
113. Cannon JA, Shen L, Jhund PS, Kristensen SL, Kober L, Chen F, 2019: pharmacotherapy, procedures, devices and patient man-
et al. Dementia-related adverse events in PARADIGM-HF and agement. An expert consensus meeting report of the Heart
other trials in heart failure with reduced ejection fraction. Eur J Failure Association of the European Society of Cardiology. Eur J
Heart Fail. 2017;19:129–37. Heart Fail 2019;21:1169–86.You can also read