ALASKA ID ECHO: HCV HIV PREP STIS - VIRAL HEPATITIS EPIDEMIOLOGY FEBRUARY 14, 2023
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Alaska ID ECHO: HCV‐HIV‐PrEP‐STIs
Viral Hepatitis Epidemiology
February 14, 2023
This program is supported by a grant from the Northwest Portland Area Indian Health Board and
funding is provided from the HHS Secretary’s Minority HIV/AIDS Fund.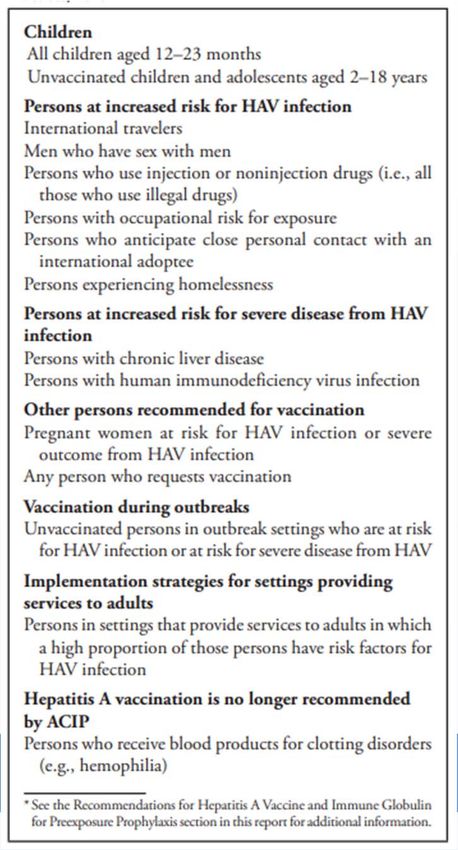
Viral Hepatitis Epidemiology Stephanie Massay, MPH, MT(ASCP) Epidemiology Specialist I Morrow Toomey, Public Health Informaticist Feb. 14, 2023
WHERE HEPATITIS WORK HAPPENS AT DOHImmunization
Program
Section of Epidemiology Other Sections
Immunization Infectious • Alaska State Public
HIV/STI Program Program Disease Program Health Labs,
Fairbanks
• Kayli Helvie, • Vacant, Public • Jamie Allison,
VHPC • Section of Public
Linkage to Care Health
Specialist, Health Nursing
Coordinator • Stephanie
Perinatal Hep B Massay, VPD • Office of
Case Manager Coordinator Substance Misuse
• Vacant, Health and Addiction
Program Prevention
Associate (OSMAP)
PRIORITY POPULATIONS BY HEPATITIS TYPE AND
MEASURE
Incidence (Acute) Prevalence (Chronic) Mortality
Hepatitis A People who use drugs
People experiencing N/A
homelessness
Hepatitis B People who inject Asian and Pacific Asian and Pacific
drugs Islander Islander
Black, non-Hispanic Black, non-Hispanic
Hepatitis C People who inject drugs People who inject American Indian/
drugs, Alaska Native
Black, non-Hispanic Black, non-Hispanic
People born 1945-1965 People born 1945-
People with HIV 1965
Viral Hepatitis National Strategic Plan:2021-2025
Acute Hepatitis A Surveillance


NUMBER OF REPORTED CASES OF HEPATITIS A VIRUS INFECTION – ALASKA, 1970-2022* *2022 counts are provisional and may be updated

CHARACTERISTICS OF REPORTED CASES OF HEPATITIS A
INFECTION – ALASKA, 2008-2022*
Number
Total 27
Race/ethnicity
Alaska Native 7
Non-Native 15
Unknown 5
Age (years)
0-14 2
15-24 0
25-44 9
45+ 16
Region
Anchorage/MatSu 14
Gulf Coast 6
Interior 0
Northern 0
Southeast 6
Southwest 1
Travel Associated
Imported International 13
Imported Out-of-State 6
Vaccination Status-VacTrAK
Unvaccinated 24
Vaccinated 2
Unknown 1
*2022 counts are provisional and may be updated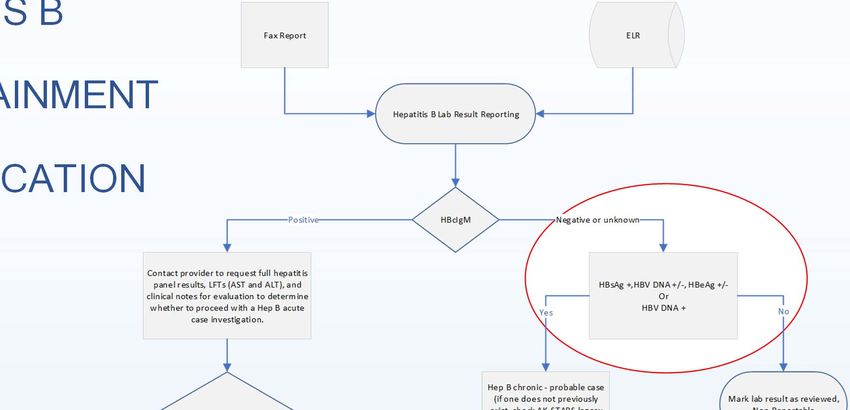
HEPATITIS A, ACUTE: PROCESS FOR CASE ASCERTAINMENT AND CLASSIFICATION https://www.cdc.gov/hepatitis/statistics/surveillanceguidance/docs/viral-hepatitis-surveillance-figure-2-2_508.pdf
HEPATITIS A, ACUTE LABORATORY EVIDENCE
Confirmatory laboratory evidence:
• Immunoglobulin M (IgM) antibody to hepatitis A virus (anti-HAV)
positive, OR
• Nucleic acid amplification test (NAAT; such as Polymerase
Chain Reaction [PCR] or genotyping) for hepatitis A virus RNA
positive
https://ndc.services.cdc.gov/case-definitions/hepatitis-a-acute-2019/HEPATITIS A, ACUTE CASE CLASSIFICATION
Confirmed
• A case that meets the clinical criteria and is IgM anti-HAV positive §, OR
• A case that has hepatitis A virus RNA detected by NAAT (such as PCR or
genotyping), OR
• A case that meets the clinical criteria and occurs in a person who had
contact (e.g., household or sexual) with a laboratory-confirmed hepatitis A
case 15-50 days prior to onset of symptoms.
§ And not otherwise ruled out by IgM anti-HAV or NAAT for hepatitis A virus
testing performed in a public health laboratory.
https://ndc.services.cdc.gov/case-definitions/hepatitis-a-acute-2019/Assess patient
immunization status,
travel history, and
job history as food
handler. Provide
education on control
HEPATITIS A measures.
CASE INVESTIGATION
Determine
household and other
close contacts i.e.,
Assess immunization status
attends or works at
a daycare, food
• Demographic information worker
• Clinical details, including
• Date of onset of illness
• Symptoms (e.g., fever, headache, Confirmed
malaise, anorexia, nausea, vomiting,
diarrhea, abdominal pain, dark urine, Has the person(s)
received at least one
acholic stool, jaundice) dose HAV vaccine?
• Laboratory results No
• Vaccination status Administer a dose of HAV vaccine or IG
according to PEP guidelines for age w/I
• Risk factors and occupation 14 days.
Yes
• Contact investigation and prophylaxis
No additional doses
needed.Acute & Chronic Hepatitis B Surveillance
NUMBER OF REPORTED CASES OF ACUTE
HEPATITIS B VIRUS INFECTION – ALASKA, 1980-
2022*
Acute Hepatitis B Laboratory Evidence: HBsAg positive, AND
Immunoglobulin M (IgM) antibody to hepatitis B core antigen (IgM anti-HBc) positive (if done)
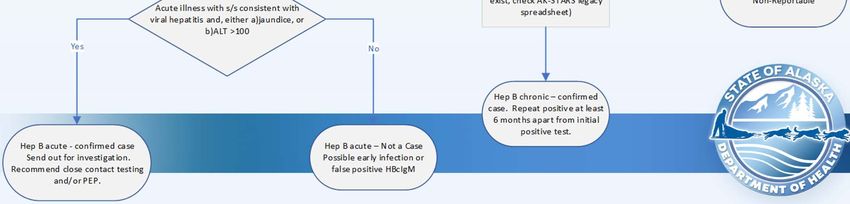
*2022 counts are provisional, unpublished data and may be updatedHEPATITIS B CASE ASCERTAINMENT & CLASSIFICATION
HEPATITIS B CASE ASCERTAINMENT & CLASSIFICATION
HEPATITIS B, ACUTE LABORATORY EVIDENCE
• HBsAg positive, AND
• Immunoglobulin M (IgM) antibody to hepatitis B core antigen
(IgM anti-HBc) positive (if done)
https://ndc.services.cdc.gov/case-definitions/hepatitis-b-acute-2012/HEPATITIS B, ACUTE CASE CLASSIFICATION
Confirmed
• A case that meets the clinical case definition, is laboratory
confirmed, and is not known to have chronic hepatitis B.
https://ndc.services.cdc.gov/case-definitions/hepatitis-b-acute-2012/Assess patient clinical details,
date of illness onset,
immunization status, risk
behaviors/exposures. Provide
HEPATITIS B, education on control
measures.
ACUTE CASE
INVESTIGATION Determine sexual,
household and other
(needle‐sharing)
Assess immunization status
contacts
• Demographic information
• Clinical details, including
• Date of onset of illness
• Symptoms, including jaundice
Unvaccinated persons should receive both Has the person(s)
HBIG and hepatitis B vaccine as soon as No completed the hepatitis B
possible (preferably within 24 hours) vaccine series?
• Laboratory results
• Vaccination status
• Risk behaviors/exposures Yes
• Contact investigation and prophylaxis
Non‐responders should receive HBIG X1 Vaccinated Responder
No Yes No PEP treatment
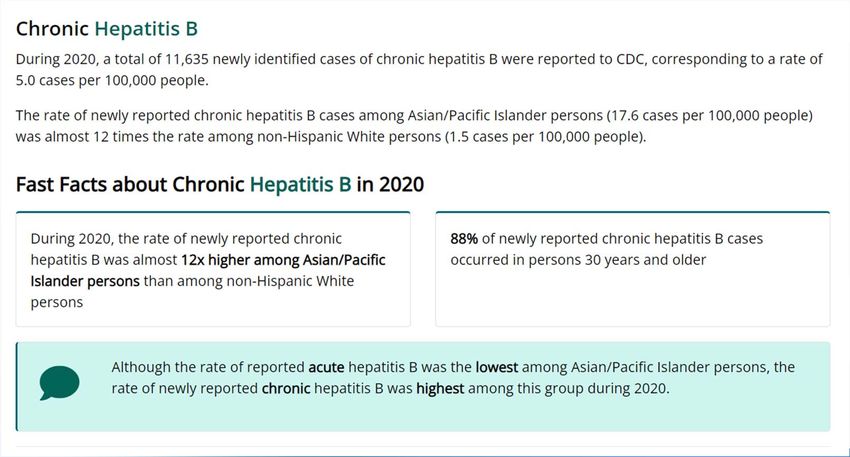
and initiate revaccination or HBIG X2 HBsAb >10 miu/mL??CHRONIC HEPATITIS B SURVEILLANCE DATA –
UNITED STATES
https://www.cdc.gov/hepatitis/statistics/2020surveillance/hepatitis-b.htm#anchor_03752NUMBER OF NEWLY IDENTIFIED CHRONIC
HEPATITIS B CASES – UNITED STATES, 2009-2020
45000
40000
Number of chronic hepatitis B cases
35000
30000
25000
20000
15000
10000
5000
0
2009 2010 2011 2012 2013 2014 2015 2016 2017 2018 2019 2020
Year
https://www.cdc.gov/hepatitis/statistics/SurveillanceRpts.htmNUMBER OF NEWLY IDENTIFIED CASES OF
CHRONIC HEPATITIS B VIRUS INFECTION – ALASKA,
2010-2022*
*2022 counts are provisional, unpublished data and may be updatedHEPATITIS B CASE ASCERTAINMENT & CLASSIFICATION
HEPATITIS B, CHRONIC LABORATORY EVIDENCE
• Immunoglobulin M (IgM) antibodies to hepatitis B core antigen
(IgM anti-HBc) negative AND a positive result on one of the
following tests: hepatitis B surface antigen (HBsAg), hepatitis B
e antigen (HBeAg), or nucleic acid test for hepatitis B virus DNA
(including qualitative, quantitative and genotype testing), OR
• HBsAg positive or nucleic acid test for HBV DNA positive
(including qualitative, quantitative and genotype testing) or
HBeAg positive two times at least 6 months apart (Any
combination of these tests performed 6 months apart is
acceptable)
https://ndc.services.cdc.gov/case-definitions/hepatitis-b-chronic-2012/HEPATITIS B, CHRONIC CASE CLASSIFICATION
Probable
A person with a single HBsAg positive or HBV DNA positive
(including qualitative, quantitative and genotype testing) or HBeAg
positive lab result and does not meet the case definition for acute
hepatitis B.
Confirmed
A person who meets either of the above laboratory criteria for
diagnosis.
https://ndc.services.cdc.gov/case-definitions/hepatitis-b-chronic-2012/HEPATITIS B,
CHRONIC CASE
INVESTIGATION
• Demographic information
• Laboratory results
• Pregnancy status. All HBsAg-positive pregnant
women should be reported to the Alaska
Perinatal Hepatitis B Prevention Program so that
they can be tracked and their infants can receive
appropriate case management
https://health.alaska.gov/dph/Epi/iz/Pages/hbv/default.aspxHepatitis B Perinatal Surveillance
If you provide PRENATAL CARE:
Universal screening for pregnant persons for HBsAg is recommended during each
pregnancy
• Report all HBsAg-positive test results including pregnant status to the AK-SOE
DOH within 2 working days.
• Perform HBV DNA testing for HBsAg--positive pregnant persons at 26-28 weeks
to guide the use of maternal antiviral therapy during pregnancy. AASLD suggests
maternal antiviral therapy when HBV DNA is >200,000 IU/mL
• Case management for HBsAg-positive mothers and babies: Send HBsAg-positive
test results along with prenatal records to the planned birthing facility. Alaska Perinatal
Hepatitis B
If you provide PEDIATRIC CARE: Prevention Program
Know maternal HBsAg status for all infants to whom you provide care
• Provide immunoprophylaxis for infants born to infected mothers, including PH 907-269-8088
hepatitis B vaccine and hepatitis B immune globulin within 12 hours of birth
• Routine vaccination of all infants with the hepatitis B vaccine series, with the first
dose administered within 24 hours of birth
• Complete HepB vaccine series and post-vaccination serologic testing (PVST) for
all infants born to HBsAg-positive women.
https://www.cdc.gov/hepatitis/hbv/perinatalxmtn.htm#patient.Prevention of hepatitis A
virus infection in the United
States: Recommendations
of the Advisory Committee
on Immunization
Practices, 2020*
Recommendations for routine HepA
vaccination among children, adolescents,
and adults
MMWR, July 3, 2020. Vol 69, No 5.HepA Vaccine Coverage by Region, 2 Doses, among 2
Year Olds, Alaska, December 31, 2022, VacTrAK Data
100%
90%
80%
70%
60%
50%
40%
30%
20%
10%
0%
Alaska Southwest Northern Interior Anchorage/MatSu Gulf Coast Southeasthttps://www2.cdc.gov/vaccines/ed/ciinc/archives/22/04/downloads/Current_Issues_4_22.pdf
HepB Vaccine Coverage by Age and Dose Number, Alaska,
December 31, 2022, VacTrAK Data
100%
90%
80%
70%
60%
50%
40%
30%
20%
10%
0%
One Month Six Months One Year Two Years
Child's Age
1 Dose 2 Doses 3 DosesHepB Vaccine Coverage by Region and Dose Number, among 2
Year Olds, Alaska, December 31, 2022, VacTrAK Data
100%
90%
80%
70%
60%
50%
40%
30%
20%
10%
0%
Alaska Southwest Northern Interior Anchorage/MatSu Gulf Coast Southeast
1 Dose 2 Doses 3 DosesVaccine Eligibility – Adults 19+
Formed in 2014 to facilitate the universal
purchase of vaccines for all children and
adults in the state of Alaska.
It does this by collecting payments from
health plans, insurance companies, and
other payers and remitting those funds to
the state.
Providers who serve uninsured adults
can opt-in to participate in the program to
give state-supplied vaccine instead of The following payers are not participating in AVAP:
purchasing vaccine privately
• Medicaid
2023 Adult assessment rate $1.51
• Medicare
• AlaskaCare Retiree Plan
Hepatitis A and B pediatric and adult • Veterans Affairs (VA)
vaccines are both on the state-supplied Note: Per Alaska Administrative Code 7 AAC 27.149(2), only Alaska
formulary residents are eligible for AVAP (or State) vaccine.
https://www.akvaccine.org/akvaccine.nsf/pages/for-providers.htmlHepatitis C, Acute and Chronic 2020 Case Definitions
HEPATITIS C CLINICAL CRITERIA
• Jaundice, OR
• Peak elevated total bilirubin levels ≥ 3.0 mg/dL, OR
• Peak elevated serum alanine aminotransferase (ALT) levels >200 IU/L,
AND
• The absence of a more likely diagnosis (which may include evidence of
acute liver disease due to other causes or advanced liver disease due to
pre-existing chronic Hepatitis C virus (HCV) infection or other causes, such
as alcohol exposure, other viral hepatitis, hemochromatosis, etc.)
Note. All criteria applies to individuals who are > 36 months of age, unless
known to have been exposed non-perinatally.
https://ndc.services.cdc.gov/case-definitions/hepatitis-c-acute-2020/HEPATITIS C LABORATORY EVIDENCE
Confirmatory laboratory evidence
• Positive hepatitis C virus detection test: Nucleic acid test (NAT) for HCV
RNA positive (including qualitative, quantitative, or genotype testing), OR
• A positive test indicating presence of hepatitis C viral antigen(s) (HCV
antigen)
Presumptive laboratory evidence
• A positive test for antibodies to hepatitis C virus (anti-HCV)
https://ndc.services.cdc.gov/case-definitions/hepatitis-c-acute-2020/HEPATITIS C, ACUTE 2020 CASE CLASSIFICATION
Probable
• A case that meets clinical criteria and has presumptive laboratory evidence, AND
• Has no documentation of anti-HCV or RNA test conversion within 12 months, AND
• Does not have an HCV RNA detection test reported.
Confirmed
• A case that meets clinical criteria and has confirmatory laboratory evidence, OR
• A documented negative HCV antibody followed within 12 months by a positive HCV antibody test
(anti-HCV test conversion) in the absence of a more likely diagnosis, OR
• A documented negative HCV antibody OR negative hepatitis C virus detection test (in someone
without a prior diagnosis of HCV infection) followed within 12 months by a positive hepatitis C virus
detection test (HCV RNA test conversion) in the absence of a more likely diagnosis.
https://ndc.services.cdc.gov/case-definitions/hepatitis-c-acute-2020/HEPATITIS C, CHRONIC 2020 CASE CLASSIFICATION
Probable
• A case that does not meet OR has no report of clinical criteria, AND
• Has presumptive laboratory evidence, AND
• Has no documentation of anti-HCV or RNA test conversion within 12 months,
AND
• Does not have an HCV RNA detection test reported.
Confirmed
• A case that does not meet OR has no report of clinical criteria, AND
• Has confirmatory laboratory evidence, AND
• Has no documentation of anti-HCV or HCV RNA test conversion within 12
months.
https://ndc.services.cdc.gov/case-definitions/hepatitis-c-chronic-2020/HEPATITIS C SURVEILLANCE NOTES • HCV case counts are provisional and may be updated as we receive additional laboratory information. • Negative RNA results are not currently reportable to the State of Alaska, which limits our ability to determine whether probable cases represent a current or past infection. We are currently working with facilities to voluntarily increase negative HCV RNA reporting while also working to update reporting regulations • Recent years’ data are thought to be influenced by the COVID- 19 pandemic.
Hepatitis C, Acute Surveillance
Figure 3.1 – Part 1 of 2
Number of reported cases* of acute hepa s C virus infec on and es mated infec ons†
United States, 2013–2020
Estimated acute infections† Reported acute cases*
70,000
60,000
Number of acute cases
50,000
40,000
30,000
20,000
10,000
0
2013 2014 2015 2016 2017 2018 2019 2020
Year
Source: CDC, National Notifiable Diseases Surveillance System.
Reference: Klevens RM, Liu, S, Roberts H, et al. Estimating acute viral hepatitis
infections from nationally reported cases. Am J Public Health 2014; 104:482.
* Reported confirmed cases. For the case definition, see https://ndc.services.cdc.gov/conditions/hepatitis-c-acute/ PMC3953761.
Centers for Disease Control and Prevention. Viral Hepatitis Surveillance Report –
† The number of estimated viral hepatitis infections was determined by multiplying the number of reported cases that United States,
met the classification criteria for a confirmed case by a factor that adjusted for underascertainment and underreporting. 2020. https://www.cdc.gov/hepatitis/statistics/2020surveillance/index.htm.
The 95% bootstrap confidence intervals for the estimated number of infections are displayed in the Appendix. Published September 2022.Figure 3.1 – Part 2 of 2
Number of reported cases* of acute hepa s C virus infec on and es mated infec ons†
United States, 2013–2020
Acute Hepatitis C 2013 2014 2015 2016 2017 2018 2019 2020
Reported acute cases* 2,138 2,194 2,436 2,967 3,216 3,621 4,136 4,798
†
Estimated acute infections 29,700 30,500 33,900 41,200 44,700 50,300 57,500 66,700
Source: CDC, National Notifiable Diseases Surveillance System.
Reference: Klevens RM, Liu, S, Roberts H, et al. Estimating acute viral hepatitis
infections from nationally reported cases. Am J Public Health 2014; 104:482.
* Reported confirmed cases. For the case definition, see https://ndc.services.cdc.gov/conditions/hepatitis-c-acute/ PMC3953761.
Centers for Disease Control and Prevention. Viral Hepatitis Surveillance Report –
† The number of estimated viral hepatitis infections was determined by multiplying the number of reported cases that United States,
met the classification criteria for a confirmed case by a factor that adjusted for underascertainment and underreporting. 2020. https://www.cdc.gov/hepatitis/statistics/2020surveillance/index.htm.
The 95% bootstrap confidence intervals for the estimated number of infections are displayed in the Appendix. Published September 2022.NUMBER OF NEWLY REPORTED HEPATITIS C, ACUTE
CASES BY YEAR, ALASKA, 2020-2022
Year Number of Probable and Confirmed
Hepatitis C, Acute Cases
2020 1
2021 2
2022 2Hepatitis C, Chronic Surveillance
Figure 3.8
Number of newly reported* chronic hepa s C virus infec on cases† by sex and age
United States, 2020
Male Female
2000
1800
1600
1400
Number of cases
1200
1000
800
600
400
200
0
1 3 5 7 9 11 13 15 17 19 21 23 25 27 29 31 33 35 37 39 41 43 45 47 49 51 53 55 57 59 61 63 65 67 69 71 73 75 77 79 81 83 85 87 89 91 93 95 97
Age (years)
* During 2020, cases of chronic hepatitis C were either not reportable by law, statute, or regulation; not reported; or
otherwise, unavailable to CDC from Arizona, Delaware, District of Columbia, Hawaii, Indiana, Kentucky, Nevada, Source: CDC, National Notifiable Diseases Surveillance System.
North Carolina, Rhode Island, and Texas.
Centers for Disease Control and Prevention. Viral Hepatitis Surveillance Report –
† Only confirmed, newly diagnosed, chronic hepatitis C cases are included. For the complete case definition, see United States,
https://ndc.services.cdc.gov/conditions/hepatitis-c-chronic/. 2020. https://www.cdc.gov/hepatitis/statistics/2020surveillance/index.htm.
Published September 2022.2020 2021 2022
Table of Demographics, Newly
3-14 1 (0.1%) 4 (0.5%) 2 (0.3%)
15-44 519 (65.8%) 517 (66.0%) 545 (72.7%)
Reported Chronic HCV Investigations
Age Range 45-60 159 (20.2%) 153 (19.6%) 116 (15.4%) by Year, Alaska, 2020‐2022
61+ 110 (13.9%) 108 (13.8%) 86 (11.5%)
Unknown 0 (0.0%) 1 (0.1%) 1 (0.1%)
Anchorage 339 (43.0%) 332 (42.4%) 282 (37.6%)
Mat-Su 123 (15.6%) 136 (17.4%) 136 (18.1%)
Gulf Coast 91 (11.53%) 100 (12.8%) 86 (11.4%)
Economic Region Interior 73 (9.3%) 60 (7.7%) 59 (7.9%)
Northern 21 (2.7%) 24 (3.0%) 13 (1.7%)
Southeast 79 (10.0%) 91 (11.6%) 107 (14.3%)
Southwest 35 (4.4%) 37 (4.7%) 44 (5.9%)
Unknown 28 (3.5%) 3 (0.4%) 23 (3.1%)
AI/AN 170 (21.5%) 245 (31.3%) 240 (32.0%)
Asian 6 (0.8%) 7 (0.9%) 5 (0.7%)
Black or African American 11 (1.4%) 22 (2.8%) 25 (3.3%)
Race NH/PI 3 (0.4%) 13 (1.7%) 11 (1.5%)
White 203 (25.7%) 291 (37.2%) 279 (37.2%)
Multi-Race 6 (0.8%) 31 (3.9%) 28 (3.7%)
Other 17 (2.1%) 23 (2.9%) 17 (2.3%)
Unknown 373 (47.3%) 151 (19.3%) 145 (19.3%)
Total Cases 789 783 750Hepatitis C Perinatal Surveillance
HEPATITIS C PERINATAL INFECTION CASE
DEFINITION
Clinical Criteria
Perinatal hepatitis C in pediatric patients may range from asymptomatic to fulminant hepatitis.
Laboratory Criteria For Diagnosis
HCV RNA positive test results for infants between 2 to 36 months of age; OR
HCV genotype test results for infants between 2 to 36 months of age; OR
HCV antigen test results for infants between 2 to 36 months of age.
Case Classification
Confirmed
Infant who has a positive test for HCV RNA nucleic acid amplification test (NAAT), HCV antigen, or
detectable HCV genotype at ≥2 months and ≤36 months of age and is not known to have been
exposed to HCV via a mechanism other than perinatal.
https://ndc.services.cdc.gov/case-definitions/hepatitis-c-perinatal-infection-2018/PERINATAL HEPATITIS C SURVEILLANCE NOTES • The CDC first published a surveillance definition for perinatal hepatitis C in 2018. • Nationally, due to the increasing number of HCV infections among women of childbearing age, perinatal transmission is increasing. • The risk of an HCV-infected mother transmitting infection to their infant is approximately 6% per pregnancy, although this risk nearly doubles if the mother is coinfected with HIV. Benova L, Mohamoud M, Calvert C et al. Vertical transmission of hepatitis C virus: systematic review and meta-analysis – PubMed (nih.gov)
Table 3.4
Number of newly reported cases* of perinatal hepatitis C virus infection, by state or jurisdiction
United States, 2020
State or Jurisdiction Perinatal Hepatitis C State or Jurisdiction Perinatal Hepatitis C State or Jurisdiction Perinatal Hepatitis C
Alabama — Louisiana 2 Oklahoma —
Alaska — Maine 7 Oregon 2
Arizona — Maryland 1 Pennsylvania 17
Arkansas 1 Massachusetts 3 Rhode Island U
California 7 Michigan 9 South Carolina —
Colorado 3 Minnesota 5 South Dakota —
Connecticut 1 Mississippi — Tennessee 9
Delaware 1 Missouri — Texas N
District of Columbia — Montana — Utah —
Florida 5 Nebraska — Vermont —
Georgia 2 Nevada 3 Virginia 5
Hawaii — New Hampshire — Washington 5
Idaho — New Jersey 8 West Virginia —
Illinois 5 New Mexico — Wisconsin 8
Indiana 16 New York 2 Wyoming —
Iowa — North Carolina — Total 165
Kansas — North Dakota —
Kentucky — Ohio 38
U: Unavailable. The data were unavailable.
* Reported confirmed cases. For case definition, see https://ndc.services.cdc.gov/conditions/hepatitis-c-perinatal- Source: CDC, National Notifiable Diseases Surveillance System.
infection/.
Centers for Disease Control and Prevention. Viral Hepatitis Surveillance Report –
—: No reported cases. The reporting jurisdiction did not submit any cases to CDC. United States,
2020. https://www.cdc.gov/hepatitis/statistics/2020surveillance/index.htm.
N: Not reportable. The disease or condition was not reportable by law, statue, or regulation in the reporting jurisdiction. Published September 2022.NEWLY REPORTED PERINATAL HEPATITIS C CASES
BY YEAR, ALASKA, 2018-2022
Year Number of Confirmed Perinatal
Hepatitis C Cases
2018 0
2019 2
2020 0
2021 3
2022 3Hepatitis C Screening
CDC RECOMMENDATIONS FOR HEPATITIS C
SCREENING AMONG ADULTS IN THE UNITED STATES
Universal hepatitis C screening:
• Hepatitis C screening at least once in a lifetime for all adults aged 18
years and older, except in settings where the prevalence of HCV infection
(HCV RNA-positivity) is less than 0.1%*
• Hepatitis C screening for all pregnant women during each pregnancy,
except in settings where the prevalence of HCV infection (HCV
RNA-positivity) is less than 0.1%*
https://www.cdc.gov/hepatitis/hcv/guidelinesc.htmCDC RECOMMENDATIONS FOR HEPATITIS C
SCREENING AMONG ADULTS IN THE UNITED STATES
• One-time hepatitis C testing regardless of age or setting prevalence among people with recognized
conditions or exposures:
• People with HIV
• People who ever injected drugs and shared needles, syringes, or other drug preparation equipment,
including those who injected once or a few times many years ago
• People with selected medical conditions, including:
• people who ever received maintenance hemodialysis
• people with persistently abnormal ALT levels
• Prior recipients of transfusions or organ transplants, including:
• people who received clotting factor concentrates produced before 1987
• people who received a transfusion of blood or blood components before July 1992
• people who received an organ transplant before July 1992
• people who were notified that they received blood from a donor who later tested positive for HCV
infection
• Health care, emergency medical, and public safety personnel after needle sticks, sharps, or mucosal
exposures to HCV-positive blood
• Children born to mothers with HCV infection
https://www.cdc.gov/hepatitis/hcv/guidelinesc.htmCDC RECOMMENDATIONS FOR HEPATITIS C
SCREENING AMONG ADULTS IN THE UNITED STATES
• Routine periodic testing for people with ongoing risk factors,
while risk factors persist:
• People who currently inject drugs and share needles, syringes, or other
drug preparation equipment
• People with selected medical conditions, including:
• people who ever received maintenance hemodialysis
• Any person who requests hepatitis C testing should receive it,
regardless of disclosure of risk, because many persons may be reluctant to
disclose stigmatizing risks
https://www.cdc.gov/hepatitis/hcv/guidelinesc.htmSummary • Hepatitis A and hepatitis B vaccines are extremely safe and effective but underutilized tools among unvaccinated populations • Implement standing orders to identify adults recommended for Hep A and Hep B vaccination and administer vaccination as part of routine services. This will provide the best chance for achieving elimination goals • Assist in improving surveillance efforts by documenting race, ethnicity, and pregnancy status on all viral hepatitis laboratory reports across health care facilities and laboratories • Scale up implementation of universal hepatitis C screening guidelines among all adults and pregnant women in a range of clinical and nonclinical settings, and provide linkage to care
Reporting Hepatitis
Laboratories Routine Reporting Within 2 Business Days
• Hepatitis type A, B, or C
Health Care Providers Routine Reporting Within 2 Business Days
• Hepatitis type A, B, or C
• Pregnancy in a person known to be infected with hepatitis B
Conditions Reportable in Alaska
To report a Public Health Emergency: Business Hours 907-269-8000
After Hours 800-478-0084Section of Epidemiology Contacts Stephanie Massay, Vaccine Preventable Disease Coordinator, ID Program 907-269-8011 Stephanie.Massay@alaska.gov Morrow Toomey, Public Health Informaticist, ID Program 907-269-8014 Morrow.Toomey@alaska.gov Jamie Allison, Nurse Consultant, Viral Hepatitis Prevention Coordinator, ID Program 907-334-0856 Jamie.Allison@alaska.gov Kayli Helvie, Linkage to Care Coordinator, STI/HIV Program 907-269-3404 Kayli.Helvie@alaska.gov Alaska Immunization Helpline 907-269-8088 or 1-888-430-4321 immune@alaska.gov
AK ID ECHO ‐ 2023 Upcoming didactic topics • HCV Treatment in Non-Traditional Settings, March 14th • PrEP Series, April 4th, 11th, 18th and 25th • TB Update, May 9th • Expedited Partner Therapy • Managing STIs in Rural AK What topics would you like to learn about? Email akidecho@anthc.org V
ADDITIONAL LEARNING OPPORTUNITIES
Alaska Liver Disease ECHO
Third Thursday of every month from noon-1:00 PM
2023 theme ~ Ways You Can Help Reduce Morbidity of Mortality From
Liver Disease
www.anthc.org/project-echo/alaska-liver-disease-echo
LiverConnect
Second Tuesday of every month 8:00-9:00 AM
www.anthc.org/hep/liverconnectADDITIONAL LEARNING OPPORTUNITIES
Addiction Medicine ECHO
Second and fourth Thursday of each month from noon-1 p.m.
www.anthc.org/project-echo/addiction-medicine-echo
Questions: Email behavioralhealth@anthc.org
Indian Country ECHO Programs
Harm Reduction, Infectious Disease, and more!
www.indiancountryecho.org/teleecho-programsFree prevention resources available at
iknowmine.org/shopAK ID ECHO: CONSULTANT TEAM
Youssef Barbour, MD Hepatologist
Leah Besh, PA‐C HIV/Hepatology Provider
Terri Bramel, PA‐C HIV/STI Provider
Rod Gordon, R.Ph. AAHIVP Pharmacist
Jacob Gray, MD Infectious Disease Provider
Annette Hewitt, ANP Hepatology Provider
Brian McMahon, MD Hepatologist
Lisa Rea, RN HIV/STI Case Manager
Lisa Townshend, ANP Hepatology ProviderAK ID ECHO Contacts
ANTHC Staff
Leah Besh PA-C, Program Director: labesh@anthc.org
Jennifer Williamson, Program Coordinator:
jjwilliamson@anthc.org or 907-729-4596
Lisa Rea RN, Case Manager: ldrea@anthc.org
ANTHC Liver Disease and Hepatitis Program: 907-729-1560
ANTHC Early Intervention Services/HIV Program: 907-729-2907
Northwest Portland Area Indian Health Board
David Stephens: Director Indian Country ECHO: dstephens@npaihb.org
Jessica Leston: Clinical Programs Director: jleston@npaihb.orgThank you!
AK ID ECHO is supported by a grant from the Northwest Portland Area Indian Health Board and
funding is provided from the HHS Secretary’s Minority HIV/AIDS Fund.You can also read

















































