Adoption and adaptation of e-health systems for developing nations: The case of Botswana
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Adoption and adaptation of e-health
systems for developing nations:
The case of Botswana
Benson Ncube, Botswana
Abstract
Due to limited resources in developing nations, limited access to quality health delivery systems is a
challenge. Botswana has a high cost of access to medical facilities in certain areas. The sparsely populated
nation lacks medical facilities; patients travel 400 km on average to receive medical treatment from referral
hospitals. Although hospital facilities exist in major cities, they are not fully equipped. There is a shortage of
certain skilled personnel, a condition that forces local patients to seek treatment in other countries, hence
raising the cost of access to medical facilities.
It is against this background that appropriate solutions are sought to improve the access and capability of the
health delivery systems. The research revealed that many countries are now using information-based services
to assist in the administration and delivery of medical services via telecommunication infrastructures.
Technological developments have ushered the development and implementation of telemedicine as a
complementary health delivery system. Several developed nations now have advanced telemedicine
initiatives that have resulted in improved access to medical facilities. However, only a few developing nations
have explored the value of telemedicine initiatives.
Interviews and a literature review were used to determine the development of telemedicine in
Botswana. The results indicate the infancy of telemedicine and the potential benefits due to widespread
telecommunications services. However, the local language poses a great barrier to the implementation of
telemedicine. Adoption and adaptation of telemedicine technologies would improve the delivery of health
services.
Keywords: Botswana; medical treatment; telemedicine; ICT
Introduction right to have access to a sound healthcare sys-
tem. Therefore, each government has a man-
It is generally argued that emerging econo- date to provide a basic health system that is
mies face healthcare problems and some health resourced and manned by government doctors.
delivery systems are on the verge of collapse.
Furthermore, a significant proportion of health Costs, access, and quality are the major chal-
funds are derived from donor funds. Due to lenges facing healthcare delivery systems. The
scarce resources, medical health deliverance is, sector is characterised by an expanding knowl-
in a way, rationed. Ultimately, the remote rural edge base, increased uncertainty, and signif-
population receives inadequate healthcare. The icant time and cost constraints as well as dis-
problem is further exacerbated by the fact that tance limitations. Therefore, governments need
rural health professionals already have a heavy to consider new technologies that could be
workload and have very little, if any, access to used as enablers in health practices. However,
healthcare information. This has a negative bear- the extent to which e-health would be effec-
ing on their professional careers. Therefore, few tive is not yet fully determined. This complex-
professionals are willing to work in these remote ity causes great challenges for governments in
areas. Thus, the quality of healthcare delivery terms of decisions to implement e-health sys-
is declining. Constitutionally, everybody has a tems. Without concrete information, the policy-
This document has been produced by DiploFoundation with the financial assistance of the European Union. The contents of this document are the
sole responsibility of the author and can under no circumstances be regarded as reflecting the position of the European Union or DiploFoundation.
1Adoption and adaptation of e-health systems for developing nations: The case of Botswana
maker cannot easily embark on the technolog- Background
ical innovations that may benefit the nations.
A telemedicine medical service is a service initi-
Telemedicine is the use of electronic information ated by a physician or provided by a health pro-
and communication technologies to provide and fessional under physician delegation, for the
support health care when distance separates the purpose of diagnosis, consultation by a physi-
participants (Institute of Medicine, 1996a, p.1). cian, treatment, or transfer of data, using inter-
active audio or video, still image capture, or
Therefore telemedicine, a kind of information any other technology that facilitates access of
technology, is required to address these challenges. health care services or medical specialty exper-
tise (Texas Department of Health, 2001).
The health care industry has barely begun even
to grasp information technology’s possibili- Literature suggests that many developed coun-
ties …. Perhaps the clearest example of a medi- tries using this technology have drastically
cal technology whose time ought to have come but reduced their national budgets. Even South
hasn’t is telemedicine (The Economist, 1998). Africa has now embarked on a telemedicine pilot
project. This is clear evidence that there is a solu-
Although the definition was presented fifteen tion in the form of technology applications. It is
years ago, to date it is still valid since health infor- the phenomenal benefit that motivates develop-
matics centres are rarely established to assist in ing countries to also embark on telemedicine ini-
awareness campaigns. The rapid development of tiatives as a way to improve their constrained
technology and the widening digital divide pro- health budgets. However, it must be pointed
vides us with the trajectory of the way health out that the success or failure of the system
delivery systems are lagging behind techno- depends very much on the key players. The liter-
logical advancements. The statement from The ature review elucidates this point. The Institute
Economist highlights the critical point that med- of Medicine identified five concerns that pre-
ical information systems are lagging behind the vent and slow down the growth of telemedicine
technologies that assist practitioners in enhancing (Simonson and Sparks, 2001): professional licen-
their practices. Drawing from these points, it is sure, malpractice liability, privacy, confidenti-
clear that telemedicine is a subset of e-health ser- ality and security, payment policies, and reg-
vices. Therefore, it can be inferred that e-health ulation of medical devices. However, some of
services in some developing countries, due to the these issues may not apply to the Botswana con-
digital divide, are still in their infancy and would text. The issues that have slowed the growth of
need bold decisions for medical professionals to e-health are critical and should be addressed.
embark on e-health initiatives and activities. In
the case of Botswana, a few telemedicine pilot Limited research is reported on the medical
projects are currently in progress. The initiative effectiveness and cost effectiveness of telemed-
is in line with the Botswana 2016 vision pillars of icine (Grigsby, 1995). Current research seems
being a prosperous, productive, and innovative to support the conclusion that telemedicine is
society. A clear policy direction is therefore nec- effective when practiced correctly, but that addi-
essary for the adoption and adaptation of appro- tional evaluation and assessment activities need
priate technologies. Since medical practices are to be conducted (Institute of Medicine, 1996b).
no exception to globalisation, there is no pos-
itive justification why national health profes-
sionals should desist from using e-health facili- Telemedicine – the concept
ties. However, it is of paramount importance that
health professionals and society as a whole accept Telemedicine has become an accepted concept
the technology. This calls for virtual collabora- in healthcare worldwide. But the definition of
tion amongst the key informants: health profes- the concept may differ from location to location.
sionals (doctors, nurses, assistant nurses, health According to the World Health Organisation
decision-makers, information technology manag- (WHO) Global Observatory for eHealth defini-
ers, and telecommunications network operators. tion telemedicine includes ‘the practice of health
2Benson Ncube, Botswana
care using interactive audio, visual and data com- spective of distance.
munication. This includes health care deliv- 2. Use of communications and computer sys-
ery, diagnosis, consultation and treatment, as tems to gain access to information.
well as education and transfer of medical data 3. Virtual collaboration by key participants.
(WHO Global Observatory for eHealth, 2010) 4. Relief of secondary and tertiary care hospi-
tals from overloads due to poor referrals.
In principle, telemedicine involves the use of 5. Quick flow of clinical information between
communication networks to deliver medical ser- clinics and hospitals.
vices where there is distance between health-
care providers and their patients. Telemedicine
is not limited to a specific area of application – Research benefits and potential applications
diffuse technology. Therefore, applications such
as teleradiology, teleconsultation, and tele-edu- E-health is a relatively new concept in develop-
cation are used to highlight the area of selected ing countries. The major challenges encountered
telemedicine applications. The advancement in in African healthcare delivery systems are access,
both computer and telecommunications tech- quality, and costs. Conceptualising e-health from
nologies are key enablers in telemedicine. The a virtual collaboration perspective has a num-
advent of Internet and mobile communications ber of significant research benefits for developing
convergence has greatly improved the flexibil- nations. All stakeholders involved in the devel-
ity of e-health. Mobile communications imply opment of an e-health system enjoy some ben-
access to medical services from anywhere at efits. From the patient’s perspective, e-health
any time. Thus telemedicine has the poten- means access to medical facilities that other-
tial of reshaping the healthcare organisational wise could not be accessed through the tradi-
structures. This is a new concept in Botswana, tional health delivery system. A typical exam-
and has potential to improve and comple- ple is where patients in a flooded Okavango
ment the existing health delivery system. Delta are remotely located such that the terrain
does not permit the safe transfer of the patients
Conceptually, telemedicine is roughly to Gaborone major hospitals. Without technol-
the same shape. No agreed upon frame- ogy, it is extremely difficult to meet this kind
work for or definition of telemedicine exists of demand. However, e-health rapidly dissem-
(Institute of Medicine, 1996a; Office of Rural inates the information that is required for the
Health Policy, 1997; USGAO, 1997). treatment of the patient. The patient also avoids
unnecessary cost in terms of accommodation
Different definitions may result in differ- and transport. In many cases, patients are sent
ent data types being collected, thus impair- unnecessarily to the referral centres. Culturally,
ing data analysis. Data collected from differ- Africans live in communities and enjoy close-
ent sources can hardly be compared due to ness to their people. Elderly people would prefer
lack of compatibility. This has contributed to be treated while they are at their own homes
to the slow development of e-health applica- in proximity to their clan. This point should
tions. Software developers and telecommunica- never be under estimated in such social settings.
tions providers and clinical practitioners need
to work together to develop e-health standards. Remotely located medical practitioners suf-
fer professional isolation. In the Botswana con-
text, remote healthcare centres lack medical lit-
Major characteristics of e-health erature and professionals cannot manage to
advance their skills while they are in their work-
According to the ITU (International ing environment. The advent of e-health allows
Telecommunication Union) telemed- professionals to be knowledgeable practitioners
icine framework, the major charac- with global access to information. The practitio-
teristics of e-health include: ners have specialists at their disposal; complex
cases can be quickly resolved through virtual
1. Universal access to the medical services irre- collaboration. Global assistance is easily avail-
3Adoption and adaptation of e-health systems for developing nations: The case of Botswana
able through telemedicine technology typically tems in Africa on the brink of collapse, the con-
tele-education and teleconsultation. Such devel- tinent can use e-health to have certain diseases
opments tend to improve the quality of health- treated locally without patients having to spend
care services, hence benefiting the target market. large sums of money seeking treatment abroad.
The government is the greatest beneficiary; this
could drastically reduce the health budget lev- Statement of the problem
els. Limited resources, such as doctors, can be
effectively and efficiently allocated for the ben- Costs, access, and quality are the major chal-
efit of the entire nation. The doctor-to-patient lenges facing the healthcare delivery system.
ratio would be improved so as to improve the The sector is characterised by an expanding
quality of health delivery services. The govern- knowledge base, increased uncertainty, and sig-
ment then becomes so credible and attracts many nificant time and cost constraints. Therefore,
potential investors into the country. Local health- e-health, a kind of information technol-
care providers create job opportunities for local ogy, is required to address these challenges.
people since local institutions would retain the
revenues generated from the local patients. The
employment generated implies a contribution to Major research objectives
the government tax base. With rapid information
dissemination, it becomes easy to detect and con- The major objectives of the research are:
tain disease outbreaks. Since prevention is better
than cure, fewer cost would be incurred through 1. To identify the needs and priorities for the
use of telemedicine. E-health can be a quick solu- introduction of e-health in Botswana.
tion that can supplement the traditional health 2. To determine the major barriers to e-health
delivery system. The precondition of such a set- in Botswana.
up is the presence of a telecommunication ser- 3. To identify key players capable of champi-
vice. With the advent of high telecommunica- oning the implementation of telemedicine
tions penetration rate, the infrastructure is now in Botswana.
readily available to offer e-health services in a 4. To create the demand for e-health/creating
sparsely populated country like Botswana. awareness for e-health services.
5. To demonstrate the potential benefit of
E-health increases the demand levels of the tele- e-health in Botswana and developing nations
communication services. Telecommunications in general.
operators and Internet service providers (ISPs) 6. To develop a working guideline/model for a
would generate additional revenue streams successful implementation of e-health
due to telemedicine applications being trans- system.
mitted through telecommunications networks.
New business models would be established
between the health and telecommunications sec- Literature review
tors. More jobs would be created in the pro-
cess of e-health deployment. The technology Introduction
can also be applied in prisons, so that the pub-
lic is not exposed to dangerous prisoners. It is Literature about e-health in general and telemed-
costly to transport prisoners to the health cen- icine applications in particular was reviewed. The
tres. The chances of escape are increased while literature covered some of the major issues that
the prisoner is in transit. This risk can be min- include benefits to society, barriers for e-health,
imised through use of e-health services. technology, as well as the doctor-patient rela-
tionship. Proper funding structures are required
It is hoped that, in the long term, the research to successfully implement e-health projects.
would have a positive impact on the national The majority of the reviewed telemedicine proj-
budget, through a direct cost reduction within ects originated in the USA, the UK, Australia,
the Ministry of Health. With healthcare sys- Norway, Canada, Finland, and Sweden. Within
4Benson Ncube, Botswana
the region, telemedicine projects were carried A telemedicine medical service is a service initi-
out in South Africa, Senegal, and Mozambique. ated by a physician or provided by a health pro-
There was scant literature regarding the tele- fessional under physician delegation, for the
medicine initiatives at the time of the research. purpose of diagnosis, consultation by a physi-
According to national press articles, the Ministry cian, treatment, or transfer of data, using inter-
of Health in collaboration with Orange Botswana, active audio or video, still image capture, or
Click Diagnostics and Botswana University of any other technology that facilitates access to
Pennsylvania initiated the first telemedicine pilot health care services or medical specialty exper-
project in 2009. The project established a tele- tise (Texas Department of Health, 2001)
medicine link between the Scottish Livingstone
Hospital in Molepolole with the government hos- Telemedicine, telehealth, e-health, and telemat-
pital, Princess Marina in Gaborone. Some links ics are some of the terms used interchange-
were established for Tshabong, Maun, Serowe, ably when describing the use of informa-
Kasane to link to Goborone. The consulting doc- tion technology in health. There is abundant
tors and other medical specialists were based in literature with similar definitions regard-
the USA and the UK. The assessment results were ing each these terms, especially telemedi-
not yet established. All investigations were rela- cine and e-health. For the purposes of this
tively recent. The findings from each study were research these two terms are one and the same.
used as the framework to conceptualise telemed-
icine in Botswana. The research methodologies Australian New Zealand Telehealth Committee
that were used in these initiatives were redefined (ANZTC, 1996, p.2) defined telehealth/e-
to suit the Botswana context. Approximately health as: ‘a health delivery system which pro-
90% of the abstracted findings favoured e-health vides health related activities at a distance
deployments. A thorough needs assessment between two or more locations using tech-
should be used to enhance the validity of the nology assisted communications’.
findings. With telemedicine, generalisation is
limited to specific issues. Therefore, there is a The literature reviewed revealed that tele-
need to adopt the technology, but adapt it to suit medicine has become common in the medi-
the environment. In the case of Botswana, real- cal literature during the last decade. However,
time video conferencing might sound fantas- developing countries have recently started tele-
tic but the limited bandwidth infrastructure may medicine initiatives. In a White Paper, Dr
not effectively support such a service. Therefore Michael Simonson gives credit to Kenneth
only those areas with digital/ADSL networks Byrd who, with several others, formed a
could adopt this technology. Market segmenta- video microwave network in 1968 from
tion and targeting becomes very critical under Massachusetts General Hospital to Boston’s
such circumstances. Prior to any e-health imple- Logan Airport (Simonson and Sparks, 2001).
mentation, infrastructure auditing becomes vital.
However, there were other projects at the same
time but this effort is considered as the mod-
Telemedicine overview ern launching of the concept of e-health. But
other countries still claim that they had their
The literature suggests that many countries own pioneer telemedicine initiatives. As a
have long recognised the need for innova- result, the origins of e-health are blurred.
tive and alternative healthcare delivery sys-
tems in order to meet the healthcare needs of It seems developing countries are lagging
the diverse population and geographic areas. behind in terms of technology innovations.
In the USA, the State of Texas has a legislature Ironically such countries are the ones that have
that seeks to promote the telemedicine advance- major health problems which could be miti-
ment. In 1998, telemedicine services were recog- gated through the use of e-health technology.
nised in this state. Texas Department of Health, In developed countries and in South Africa for
in its document, Telemedicine Pilot Project, instance, federal and state governments and pri-
defines telemedicine in the following manner: vate institutions are funding e-health projects.
5Adoption and adaptation of e-health systems for developing nations: The case of Botswana
This approach highlights the Systems Approach shortage of pathologists; therefore it is justified
Theory that calls for collaboration. However, to start with the pathology application. It might
the funding issue appears to be different in most not be advisable to start with surgery applica-
African countries. In Botswana, there is a hier- tions since these are complex and require high-
archical structure within the health sector, and speed transmission links to connect the partici-
the private sector seems to pursue its private ini- pating sites. The challenges of power disruptions
tiatives. Without government incentives, the pri- within the SADC region pose a major barrier
vate players preferred to have their own ini- for the adoption of telesurgery applications. The
tiatives. Because of this fragmented approach, issue is that prioritisation is fundamental. In gen-
duplication of efforts resulted in inefficient allo- eral, to date, dominating telehealth applications
cation of resources. Therefore, the end-users are telepsychiatry, teleradiology, and renal tele-
found it very difficult to have universal access to medicine. The later was more pronounced in
health services. But the current government pol- Australia than elsewhere. Telemedicine appli-
icy appears to favour the collaboration platform. cation names are derived from the clinical area
If this approach is maintained then there are of interest. The clinical area of interest is pre-
high chances that patients will benefit from this fixed by the term ‘tele’. For example in radiol-
collaborative effort. In America, this approach ogy the application name is teleradiology.
has enhanced the telemedicine adoption rate.
It is hoped that the same model will acceler- It is therefore a multimedia tool that can be uti-
ate the e-health adoption rate in Botswana. lised to improve the state of the heathcare deliv-
ery systems in developing nations. In this case,
technology is one of the fundamental enablers
Common telemedicine applications required in the implementation of e-health. It
was apparently clear that the success of such
Kvedar et al. (1998) list four major applications a system is centred on the Systems Approach
for e-health: remote consultation, remote mon- Theory. A total integrative approach is critical
itoring, remote education, and telemonitoring. to the sustainable implementation of telemedi-
Amongst all these applications remote consulta- cine in any nation. The approach recognises the
tion has become synonymous with telemedicine. interplay of the interdependent key stakehold-
ers. Such an integrated approach also recognises
Consistent with the ANZTC definition, the interaction and interdependences of several
e-health includes: crucial elements of success, i.e. people, technol-
ogy, process, training, programme management,
● Direct consultation cost optimisation, and community involvement.
● Case conferences Therefore, a taskforce consisting of the key stake-
● Educational activities holders should drive telemedicine/e-health ini-
● Medical images and data transfers tiatives. Proper identification of such members
● Passive information dissemination (e.g. is critical and necessary. The generic task force
through websites) consists of health agencies, telecommunications
operators, medical professionals, legal and tele-
The review revealed that telemedicine technol- communications regulators, and patients. Many
ogy is used in a variety of clinical areas includ- pilot projects used this generic model with some
ing psychiatry, emergence medicine, derma- kind of adaptations to suit the country of interest.
tology, cardiology, surgery, pathology, clinical
education, oncology, radiology, ophthalmol-
ogy, and renal medicine. The list offers a wide Different telemedicine activities and
selection of applications that e-health can pro- information technology configurations
vide. However, the exact applications are cus-
tomer driven. The needs assessment programme A telemedicine project involves both human and
must be initiated to determine which applica- technology interactions. As a result decision-
tions to start with. For example, in Botswana makers need to understand the effects of such
and neighbouring countries, there is a critical interactions.
6Benson Ncube, Botswana
Getting the human components-both individ- as the digitized x-rays from one terminal to
uals and organizations-to work well together the other. It normally includes a digitizer,
and with complex and changing technologies is which enables x-ray films to be converted
a never-ending challenge. By illuminating when into digital images.
and why these components are not performing 2. Videoconferencing involves the transfer of
as intended, evaluators can help program man- real-time audio and video from one loca-
agers decide whether to continue, discontinue, or tion to another, enabling the parties at both
redesign operations and can also suggests to ven- locations to see and interact with the other
dors and designers how their technologies might parties in a collaborated manner. It nor-
be better designed to accommodate human char- mally includes a document camera that
acteristics (Institute of Medicine, 1996a, p.73). can be used to transmit documents and
x-ray images. In terms of the transmission
Therefore, it is of paramount importance that capacity or bandwidth a minimum transmis-
the available technologies are adapted to suit sion rate of 128kbps is required to link the
the needs in question. Due to such issues, two videoconferencing centres
it was critical to administer a questionnaire 3. General multimedia includes video con-
to allow users to bring forth their attitudes ferencing capabilities and the real-time
and opinions about telemedicine projects. transfer, viewing and manipulation of data
files.
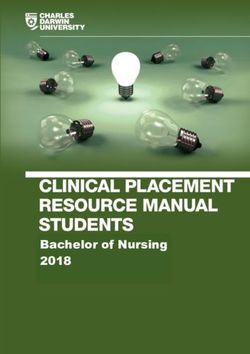
InformaƟon Technology ConfiguraƟon 4. Medical multimedia includes general mul-
timedia and high powered light sources
Medical MulƟmedia
to which medical devices can be attached,
General MulƟmedia enabling both parties to see, for example,
a patient’s ear. It may also include an elec-
Videoconferencing tronic stethoscope, which enables the other
party to hear the patient’s heartbeat and
SƟll Image Transfer
breathing. In complex facilities the terminal
equipment sometimes includes some kind of
robotics that allows telesurgery activities to
E-health Telemedicine AcƟviƟes
be carried out remotely.
Impact on Health
TeleconsultaƟons
Care Delivery
System
Distance Learning The use of different information technol-
ogy configurations is a function of the needs
TeleevaluaƟons
to be addressed. Ultimately the needs assess-
Figure 1. The impact of different telemedicine ment determines the selection of the appro-
activities and different information priate technology to be applied. In the
technology configurations (Paul, 2000). Zimbabwean context, it appears that the dom-
inant technologies could be the first three cat-
egories. However, the ideal situation is to have
Different information technology the medical multimedia system that will allow
configurations delivery of many e-health applications.
Information technology is viewed as a mediating
interaction, and the quality of technology deter- Telemedicine/e-health technology
mines the quality of this interaction (Schrage,
1995). Figure 1 represents the telemedicine model From a technology standpoint, telemedicine is the
in greater detail, relative to the information tech- application of telecommunications and computer
nology configurations. Basically the informa- technology that are already in use in other indus-
tion technology is divided into four categories: tries (USGAO, 1997). The technology includes the
hardware, software, and communication links of
1. Still image transfer involves an asynchro- the telemedicine project. Telemedicine, like any
nous transfer of graphical images files such other advanced ICT depends on complex techni-
7Adoption and adaptation of e-health systems for developing nations: The case of Botswana
cal and human infrastructures. Such infrastruc- the nearest health centre, and the emigration of
tures operate both within discrete institutions and medical professionals. Poor working conditions
across organisational and geographic boundar- also motivate staff to leave health institutions. As
ies. Therefore, there are many proprietary tele- such, Botswana is also facing similar challenges.
medicine technologies available from different
equipment vendors. Such a wide range raises the Botswana is a sparsely populated country; hence
issue of standards and compatibility. As a result, many patients are forced to travel on average 400
the ITU has developed an open system standard km to the referral centres. Poor patients can-
that allows connectivity of different telemedicine not afford transport costs caused by such dis-
equipment. Therefore, all telemedicine initiatives tances. The prevalent diseases are HIV/AIDS,
that include the ITU as one of the key stakehold- hypertension, diabetes, pulmonary tubercu-
ers are using the standardised terminal equipment. losis (TB) and pneumonia. These diseases
are threatening the traditional health deliv-
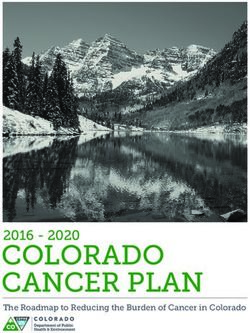
The technology infrastructure is a telecom- ery system. The shortage of medical special-
munications network with input and output ists, such as neurosurgeons, plastic surgeons,
devices at each connected location. Although maxillofacial surgeons, nephrologists, and vas-
there is no commonly recognised defini- cular surgeons aggravates the situation.
tion or set of devices that constitute telemedi-
cine, a generic telemedicine constituency will These skills shortages have forced the govern-
include the following those listed in Table 1. ment to engage foreign doctors, which puts a
further burden to pay more in order to attract
and retain critical staff. Foreign medical pro-
The health situation in Botswana fessionals in the government sector account
for 30% of the medical staff in Botswana.
Many developing countries are faced with many The working conditions for some doctors has
challenges that affect health delivery systems. been made worse by the poor patient/doc-
These challenges include limited health budgets, tor per day ratio (70–100/1). This is a heavy
shortage of medical specialist, long distances to load for the doctor to bear. This situation
Table 1. The impact of different telemedicine activities and different information technology
configurations (Paul, 2000).
Type of media used Telecommunications Services Available
Copper telephone lines Switched
Fibre Optic Lines ISDN
Satellite 64K Leased Lines
Microwave Frame Relay
Coaxial Cables Dedicated E1 (2 Mbps)
Peripherals Real-Time Videoconferencing
Endoscope
Electronic Stethoscope
Studio Videoconferencing
Otoscope
Desktop Videoconferencing
Ophthalmoscope
Full-Motion Uncompressed
Dermascope
Video Full-Motion Compressed
Microscope
Video Analogue Transmission
X-Ray Scanner
Digital Transmission
Document Camera
Remote Monitoring Equipment
Data/Image Transfer Types of cameras available
Real Time
1-chip CCD Camera
Full motion interactive video
3-chip CCD Camera
Still images with two-way audio
Analogue Video Camera
Video clips with two-way audio
Digitizing Still image Camera
Store and Forward
Document Camera
Still images for later review
Macro lens Camera with peripheral scope
Video clips for later review
Laser Scanner
Text Electronic Mail
8Benson Ncube, Botswana
might have been accelerated due to the fact that to diversify into the service industry. The soci-
Botswana did not have a medical school for a ety is a closed society that strives on strong busi-
long time. The University of Botswana Medical ness relationships and is highly dependent of
School has only been open for three years. government services and values the Setswana
language. This condition of dependency causes
a threat to the delivery of services since the bur-
Assessment in Botswana (findings) den of payment would be deemed to rest on the
government. Strong business relationships would
The backbone of telemedicine is centred on be desirable to establish new business part-
the telecommunications infrastructure that nerships for rolling out the e-health services.
provides the necessary links. The dominant Due to the strong cultural values, the appli-
national telecommunications operator that pro- cations for e-services would need to be trans-
vides fixed telephone connections is Botswana lated into the local language in order for e-health
Telecommunications Corporation (BTC). Prior to succeed and be owned by the citizens.
to the opening up of the telecommunications
sector, BTC enjoyed a monopoly for provid- Botswana’s legal structures exist and are cred-
ing basic telephone services. But this monop- ible. It has the capability to define the legal
oly has derailed the development of the tele- laws and issue data protection and confiden-
communications infrastructure. Therefore, tiality for the patients, as this data is opened
some areas still have no telecommunications up for transfer through ICT infrastructures.
services. Such situations present some tech- BTA regulates the provision of telecommuni-
nological barriers to telemedicine. Major cit- cations services and has the power to control
ies are connected on high-speed networks which the pricing of services, hence it has the influ-
are capable of transmitting video signals. ence to ensure that e-health services are rolled
out countrywide and at affordable rates.
There are now three mobile telecommuni-
cations operators in Botswana: be-Mobile, The use of computer systems supports the green
Mascom, and Orange Botswana. be-Mobile is environmental movement. Green comput-
a sister company to BTC while Mascom and ing means reduced use of paper, thus preserv-
Orange Botswana are privately owned com- ing the environment. E-health service delivery
panies. These companies have different capi- will also have a positive impact on the environ-
tal structures and controlling bodies. The gov- mentally friendly strategies since it is paper-
ernment has opened up the telecommunications less and minimises transportation emissions by
sector; hence there is a series of VANS licenses limiting hospital visits and distances travelled.
which mainly provide Internet services.
With the globalisation movement, Botswana has
Using the PESTLEG model on Botswana, it become a global village; hence the need to inter-
was determined that the political environ- connect with other entities for remotely access-
ment is mature and stable, hence supportive of ing any information-based services indepen-
clear policies. It would be relative easy to con- dent of physical distance. The e-health platform
vince the government to consider implement- allows the delivery of health services through a
ing an e-health policy that will assist in roll- networked platform that reaches out to a con-
ing out e-health services on a wider scale. The sulting specialist located anywhere in the world.
economy is stable with a projected growth rate
of over 4% GDP; this means that new innova-
tion projects might have room for implementa- Regional telemedicine assessment
tion as the government, with a little help from
donors, would be able to execute the pilot proj- Although there were several regional telemed-
ects. However, the economy is highly dependent icine initiatives, there was scant information
on diamonds, so there are some challenges in that was drawn from the pilot projects that were
diversity. Telemedicine services with their mul- being rolled out. According to Giorgio Parentela,
tiplier effect apparently present an opportunity the Senior Strategy Officer at the Directorate of
9Adoption and adaptation of e-health systems for developing nations: The case of Botswana
Telecommunications and Integrated Applications cess should be put in place and effectively exe-
based in Paris there were no current telemedicine cuted to enable the success of such projects.
initiatives in the SADC region; only a recently
started project demonstration in two sub-Saha- Conceptually, telemedicine is roughly the same
ran countries, Senegal and Kenya. The European shape. No agreed-upon framework for, or defini-
Space Agency in cooperation with the European tion of telemedicine exists (Institute of Medicine,
Commission and the Telemedicine Task Force 1996a; Office of Rural Health Policy, 1997;
(TTF) recently established an 18-month initiative USGAO, 1997). Therefore different definitions
to support the extension of sustainable e-health may result in different data analysis. However,
services in Africa using satellite-based tech- even though there are such disparities, telemed-
nology as the telecommunications infrastruc- icine continues to be explored by various devel-
ture to reach remotely located rural patients. It oped countries. The initial champions of telemed-
was anticipated that the needs assessments for icine include Sweden, the USA, Australia, Greece,
this project would last for six months. This was Norway and most of the western European coun-
an indication that such projects need more time tries. These and other early telemedicine projects
to access and to correctly determine the prior- were perceived positively from a clinical perspec-
ities of the e-health applications based on the tive, but technologically these projects were quite
findings. Although the satellite communication complex. Due to such complexities, they became
might reach out to remote locations, the expen- expensive to operate. As a result, the rate of tech-
sive cost of the satellite space segment may affect nology adoption was very low. Only enthusiasts
the deployment of the telemedicine services. and early adopters were involved in these proj-
ects. Because of such market segmentation, some
areas benefited earlier than others. A strong char-
Issues and challenges for telemedicine acter of enthusiasm and early adoption is a fun-
damental requirement for the success of tele-
Despite the attention that telemedicine has medicine initiatives. Research indicated that few
received, information about ongoing telemedi- emerging economies participated in telemedi-
cine projects and investments is both scant and cine initiatives. Of all the articles reviewed, tele-
unreliable. This has made telemedicine evalu- medicine initiatives involved universities, health
ations very difficult to implement. From such agencies, telecommunications operators, tele-
perspectives, it was difficult to replicate pilot communications and legal regulators, med-
projects in other areas. It appears it is very dif- ical professionals, and research institutions.
ficult to determine the exact levels of govern- Therefore a strong research team is required to
ment spending on telemedicine. Most of the execute the telemedicine initiative. All the col-
projects are mere claims that are not substan- laborators contributed mainly in terms of fund-
tiated. For example, a study sponsored by the ing and human effort. This is also a critical pre-
Office of the Rural Health Policy (1997) in requisite for a successful initiative. The following
the USA noted that while close to 600 rural statement indicates how critical government par-
health facilities claimed to have onsite opera- ticipation and commitment to the project is.
tional telemedicine projects, over 20% of these
projects were not operational by the second Technological considerations and reduc-
time these facilities were re-contacted, roughly tion in government funding for telemedicine
eight months after they were initially con- spelled the end for the first wave of telemedi-
tacted. This statement indicates that telemed- cine projects. By, 1986 only one of these early
icine implementers should not take the bene- telemedicine projects had survived (Institute
fits at face value. A detailed situation analysis is of Medicine 1995b; USGAO, 1995).
required before engaging in such technology ini-
tiatives. An iterative process should be adopted Despite this information morass, telemedicine
when developing telemedicine projects so that is rapidly expanding. Governments and the ITU
true intrinsic values are determined. A sim- have taken the lead. This has made a positive
ple replication approach may be disastrous and impact in developing countries where the ITU
costly. A proper monitoring and evaluation pro- works with the local government to assist them
10Benson Ncube, Botswana
in setting up telemedicine pilot projects. South now migrating to 3G services, hence improving
Africa and Mozambique were involved in ITU- the geographical spread of data services that are
initiated telemedicine pilot projects. Normally fundamental to the success of e-health services.
these projects have central sites that are con- The access to East African Submarine System
nected via high-speed links to provincial hos- (EASSy) and West African Cable System (WACS)
pitals. These pilot projects have shown positive could boost the international Internet bandwidth
impacts on the respective healthcare delivery sys- that will further bring down the costs of Internet
tems. Therefore there is a need to alert policy- services. Although the market is competitive, the
makers to be aware of the potential benefit of data service costs are still high, since an ADSL
telemedicine. Disseminated information would line of 256kbps costs about USD$80. This is
reinforce the government position (Vision, 2016). still a major barrier to Internet access. Another
The review indicated that telemedicine projects challenge is the high cost of computers and low
are mainly driven by government agencies. For computer literacy rate within the country.
example, in the USA, ‘at least 35 federal agen-
cies were involved in telemedicine projects between The increased performance and dramatic reduc-
1994–1996, federal investment in telemedicine has tions in cost in computer and telecommuni-
been at least 600 million dollars’ (USGAO, 1997). cations hardware and software in the 1980s
paved the way for the resurgence of telemed-
The emphasis on telemedicine is expected to icine, and the wave of telemedicine activ-
continue, resulting in government author- ity began early this decade (Paul, 2000).
ities enacting Acts of Parliament that allow
the setting up of relevant infrastructures such Therefore, it is a duty of the government
as telecommunications and electricity. ‘The to ensure that an enabling environment
Telecommunications Act of 1996 directed the and infrastructure are in place and ready
Federal Communications Commission to explore to provide links for telemedicine applica-
actions that would provide telecommunications tions. Without such items it would be diffi-
services to all rural areas and further required tele- cult to fully develop telemedicine activities.
communications companies to provide discounts to
health providers in rural areas’ (USGAO, 1997). Several countries have reported success-
ful implementation of telemedicine pilot proj-
Reference was made to Telecommunications ects. In 2003, an American surgeon (in the
Authority Act 1996 for the establishment of BTA USA) directed an operation on a French lady
to regulate the provision of services to, from, and (in France) remotely over a telemedicine sys-
within Botswana. The telecommunications mar- tem known as telesurgery. In this case France
ket is fairly liberal and now there is talk of pri- Telecom provided the high-speed fibre link that
vatising the state Botswana Telecommunications was used for video conferencing. All this evi-
Corporation (BTC) by the end of 2011. Currently dence suggested that the future of the medi-
there are three public telecommunications oper- cal fraternity would be anchored in modern
ators (PTOs), namely BTC, Mascom Pty Ltd. and technology. However, in Botswana and some
Orange Botswana Pty Ltd. BTA (2010) reported other African nations, the issue of telemedi-
that there are 43 Value Added Network Services cine has just unfolded. The Ministry of Health
(VANS) that provide data and Internet services. has established a few telemedicine initiatives
In addition to these licensed operators are 15 that connect some remote district hospitals to
private network operators (PNOs) that oper- the Gaborone referral hospital. Also Gaborone
ate private networks to carry data and voices ser- is connected to Francistown. Private hospi-
vices. PNOs are for the sole use of the licensed tals like Bokomoso also have their own pri-
entity and may not be linked to the public net- vate telemedicine projects. The links are mainly
work operators. This open market has led to a used to exchange patient information and some
rise in mobile telecommunications penetration x-ray images. It must be pointed out that these
of 105% by March 2009 premised on a popula- services per se do not constitute a telemedi-
tion of 1 776 494. Most of these mobile subscrib- cine interactive video consultation. The cur-
ers are pre-paid services. All the operators are rent telemedicine systems are still proprietary,
11Adoption and adaptation of e-health systems for developing nations: The case of Botswana
and fail to meet the minimum ITU standards. Bashur (1998) stated that: ‘There is concern
Therefore, there is still a window of opportunity about the wisdom of rapid deployment of tele-
to develop and implement telemedicine systems health systems before we have developed appro-
that adhere to the ITU’s open standard specifi- priate organizational structures, uniform tech-
cations. With such systems, interoperability with nical standards, and effective clinical protocols
other countries’ telemedicine systems is guaran- for the proper implementation of telemedicine.
teed. Compatibility is a requirement for the glo- Most importantly, we are yet to understand and
balisation of medical activities. This condition demonstrate fully how telemedicine can effec-
results in the availability of medical health ser- tively deal with the nation’s persistent prob-
vices to many patients whilst the medical spe- lems of cost, quality and access to health care.’
cialist can be located anywhere in the world.
Prior to developing technological systems,
A review of the Botswana health delivery sys- a thorough needs assessment and evalua-
tem suggests that Botswana is a typical nation tion is essential. Such needs are specific and
that has a tremendous challenge to overcome in should be correctly prioritised to have an effec-
the health industry. This is a sector that requires tive system. There appears to be claims that
substantive resources both human and financial. technology assessment can be used to speed
With the high death rates of skilled personnel up adoption of technology that improves
and the scourge of HIV/AIDS in Botswana, the the efficiencies of the e-healthcare system.
standards of the health delivery system continue Furthermore, possible telemedicine barriers
to deteriorate. It was on record that many social would be revealed and addressed well on time.
workers, for example, doctors, pharmacists, and
nurses, are leaving the country for greener pas-
tures and better standards of living. This is an Anticipated consequences of using
undesirable position as the majority of those pro- telemedicine/ potential benefits and barriers
fessionals were educated and trained by the gov-
ernment institutions and used public funds. The The many issues, consequences, benefits and
Government trained those professionals with the drawbacks of telemedicine highlighted by the
hope that they would plough back the benefits literature are often anecdotal in nature. It is
into the society as a whole. Unfortunately, most argued that the lack of adequate data, espe-
of them continue to emigrate resulting in a posi- cially economic data, hinders the outcome of
tion whereby the government has to depend on evaluation (Lobley, 1997). Benefits and bar-
foreign specialists and the associated challenge of riers can be both quantitative and qualita-
attracting and retaining these foreign profession- tive. The nature of the benefits and barri-
als. Such challenges demand high levels of inno- ers make it extremely difficult to evaluate the
vation in the form of telemedicine applications. effectiveness of the system. Intangible bene-
fits could not be easily explained by those peo-
Although technology was a key enabler, there ple with a bias towards quantitative analyses.
was little focus on that area. It was appar-
ently clear that many technological initiatives Almost every telemedicine article reviewed
had proven to be robust. Therefore, the focus described the benefits of telemedicine. Some
was on the utilisation of the available technol- authors argue that bias exists due to a ‘novelty
ogy to enhance the health delivery system. The effect’, whereby new technology is usually viewed
research also highlighted the critical success in a favourable light. In practice, this state-
factors as well as the barriers that could ren- ment can be challenged. A case in point is the
der the telemedicine initiative difficult to imple- comparison between telecommunications ana-
ment. The areas of concern involved information logue and digital systems. Digital systems rep-
confidentiality, and security of both the infor- resent new technology while analogue systems
mation and the transmission media. The leg- represent old technology. Digital systems are
islation that governed the medical practitio- more reliable, robust, high speed, and carry sev-
ners needs to be reviewed to find out what legal eral kinds of information signals. Therefore,
issues could affect telemedicine implementation. the new technology provides greater benefits.
12Benson Ncube, Botswana
Lobley (1997) suggests that telehealth has the Previous studies indicated that benefits can be
potential to introduce a cheaper way of deliver- perceived from different angles. All the key
ing services, but can also increase costs through stakeholders derived some benefits from the
additional capital expenditure and the expansion telemedicine initiatives. In totality, the benefits
of treatment into areas where it is currently not are worth trying the telemedicine projects. The
available. The availability of telehealth might biggest challenge in implementing telemedicine
increase demand for services such that a multi- projects involves the economic evaluation of such
plier effect is realised amongst the key players. initiatives. Most economic evaluations have failed
Therefore all the key players are likely to derive to capture those intangible benefits, such as
some benefits from telemedicine initiatives. reduced professional isolation. Therefore project
Typically the network operators may use the evaluations must be clear on what benefits should
initiatives as a marketing strategy that delivers be derived from telemedicine initiatives.
long-term benefits. Orange Botswana has taken a
similar view by being engaged in telemedicine However, past studies also identified com-
pilot project with the Ministry of Health. mon barriers for telemedicine that need to
be dealt with. Using Kurt Lewin Force Field
Lobley (1997) identified other, non-financial analysis, the telemedicine task force should
benefits which have been widely publicised but ensure that the supporting forces are rein-
are difficult to quantify: They include: forced while the restraining forces are
removed or minimized. The classical bar-
● Qualitative improvement in patient care riers encountered in telemedicine are:
through improved treatment.
● Faster and more accurate diagnosis. ● Initial capital costs
● Reduced need for patient referral due to ● Doctor and patient acceptance
remote consultation. ● Resistance to change
● Improvement in patient referral through ● Regulatory issues
better knowledge and preparation. ● Data security
● Improved training and education. ● Medical licensing
● Reduced patient disruption due to reduced ● Professional liability
travel. ● Hospital credentials
● Improved training due to knowledge transfer ● Poor infrastructure
from the specialist to the remote site.
● The reducing need for specialist consultation The interesting point is that most of these barri-
as a result of knowledge transfer. ers can be handled using the existing norms and
rules. But, in order to assure a complete inte-
On the other hand, the Emergence Care gration of healthcare activities and the informa-
Research Institute (1999) reported that tion society, extensive legislative work should be
the benefits of telehealth include: done. This was noted mostly in the American
society, where various laws were enacted so
● The ability to bring care services closer to that an enabling environment was created. The
patients, rather that converse. review indicated that Botswana has a positive
● Providing under-served and isolated areas attitude towards the creation of such an envi-
with health care virtually equal in quality to ronment since it has a sound legal framework
that delivered to heavily populated area. that supports business entities and protects the
● Improving the continuity of care that patients interests of the people. The integrity and con-
receive. fidentiality of the patient information should
● Helping clinicians to improve their own continue to be observed and respected regard-
skills, by facilitating continuing medical less of the manner in which services are pro-
education. vided through the use of e-health technologies.
13Adoption and adaptation of e-health systems for developing nations: The case of Botswana
Conclusion eral weeks. Information that is obtained from the
web is normally recent and reliable as opposed
Existing telemedicine programmes demon- to that obtained from the traditional librar-
strate that technology can be made operational, ies. However, time must be spent on qualifying
but most of the studies assessing the efficacy of the credibility and validity of the information.
costs are insufficient to permit definitive state-
ments about the evidence supporting or disput- Talking to people is a good way to obtain infor-
ing the use of telemedicine. Since situations are mation during the early stages of the research. It
unique from country to country, it is the duty of assists in building up the foundation of the
the task team to assess and determine the exact research. It can be used to gather information
requirements of its nation. The critical challenge that is not publicly available at the time of the
is to have technology acceptance within specific research or too new to be found in the literature.
social settings. This is related to the history of Examples might include meetings with prospec-
the country or its religion, its economy, geogra- tive players, customers, suppliers, and other types
phy, and culture. Once that has been dealt with, of business conversation at trade fairs, seminars,
technology is then applied as an overlay to the and association meetings. The biggest drawback
structure and organisational environment. The of this approach is its validity. Although often
Botswana people are very culturally centred and valuable, the information has questionable
proud of their language, hence the telemedicine validity because it is highly subjective and might
deployment must be culturally centred as well. not be representative of the population.
The developed systems must be in a Setswana
language for easy adoption. Therefore, the tech-
nology should not be viewed as a new system Focus group
to replace the traditional health delivery system
but as a complimentary service delivery system A focus group is used as a preliminary research
that cuts across all facets of medical practices. technique to explore people’s ideas and atti-
tudes. It is often used to test new approaches
and to discover customer concerns. A group
Research methods of about 6 to 20 people meets in a conference-
room-like set-up and the moderator leads the
There are many ways to get information that group discussion and keeps the focus on the
relates to specific problems. However, the area to be explored. It is relatively cheap and can
most common research methods are literature be conducted within a couple of weeks. Its dis-
searches, talking to target groups, focus groups, advantage is that the sample size is small and
personal interviews, telephony surveys, mail sur- may not be representative of the population.
veys, e-mail surveys, and Internet surveys.
Personal interview
Literature research
Personal interviews are a way to get in-depth
A literature search involves reviewing all read- and comprehensive information from the target
ily available materials. Such materials can include group. The interview involves one person inter-
internal organisation information, relevant viewing another person for personal or detailed
trade publications, journals, magazines, annual information relating to the subject of interest.
reports, company profile, online databases, stra- Personal interviews are very expensive because of
tegic business plans, and any other published the one-to-one nature of the interview. Typically
materials. This method is otherwise known as an interviewer will ask questions from a writ-
secondary research. It is a very expensive method ten questionnaire and record the responses ver-
of gathering information, although it often batim. Sometimes the questionnaire is a sim-
does not yield timely and accurate information. ple list of topics that the researcher wants to
Literature searches over the web are the fastest, discuss with the industry experts. Since per-
while traditional library searches can take sev- sonal interviews are expensive, they are gen-
14You can also read