A BOOSTER DOSE OF mRNA COVID-19 VACCINATION FOR HEALTHCARE WORKERS NOVEMBER 2021 SHC 9679 - Superior Health Council
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Superior Health
Council
A BOOSTER DOSE OF mRNA COVID-19
VACCINATION FOR HEALTHCARE WORKERS
NOVEMBER 2021
SHC № 9679
Lorem ipsum
HCW
COPYRIGHT Federal Public Service Health, Food Chain Safety and Environment Superior Health Council Place Victor Horta 40 bus 10 B-1060 Brussels Tel.: 02/524 97 97 E-mail: info.hgr-css@health.fgov.be All rights reserved. Please cite this document as follows: Superior Health Council. A booster dose of mRNA COVID-19 vaccination for healthcare workers. Brussels: SHC; 2021. Report 9679. Public advisory reports as well as booklets may be consulted in full on the Superior Health Council website: www.css-hgr.be This publication cannot be sold.
ADVISORY REPORT OF THE SUPERIOR HEALTH COUNCIL no. 9679
A booster dose of mRNA COVID-19 vaccination for healthcare workers
In this scientific advisory report, which offers guidance to public health policy-makers,
the Superior Health Council of Belgium provides recommendations on vaccination against
COVID-19 for healthcare workers.
This version was validated by the members of the NITAG and the Board on
27 October 2021
This version will be validated by the College on 03 November 20211
I INTRODUCTION AND ISSUE
On September 30 2021, the Superior Health Council (SHC) received a request for advice from
the Task Force ‘Operationalisation vaccination strategy COVID-19’ on the need of booster
dose of COVID-19 vaccination for individuals working in the healthcare sector.
A third dose for immunocompromised patients to complete primary vaccination against
COVID-19 and a booster dose for elderly (≥ 65 years) and individuals living in care facilities
such as nursing homes has been already implemented in Belgium (SHC 9650).
II RECOMMENDATION
Vaccinating as many people as possible around the world is essential in managing this
pandemic. Within the COVAX project, Belgium is collaborating to fair and equitable access to
COVID-19 vaccines for every country in the world.
The SHC emphasizes the importance of primary vaccination against COVID-19 of the
general population; the SHC also recommends to make vaccination of workers in the health
care sector mandatory (SHC 9671, 2021). The term "people working in the healthcare sector"
includes all the socio-professional categories listed in the advisory report SHC 9597-9611 of
September 2020. Furthermore, the SHC would like to remind on the advisory report on
vaccination against seasonal influenza (SHC 9625) and simultaneous vaccination (SHC
9675).
1
The Council reserves the right to make minor typographical amendments to this document at any time. On the other hand,
amendments that alter its content are automatically included in an erratum. In this case, a new version of the advisory report is
issued.
Superior Health Council
www.shc-belgium.be −1−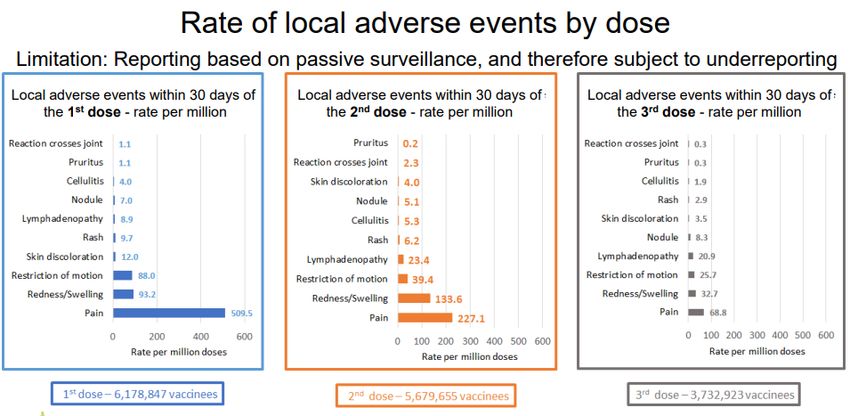
Based on currently available data,
- Healthcare workers are at the same risk of both symptomatic and severe infections
and are no more prone to symptomatic or severe infections than the general population
with the same vaccination status.
- Healthcare workers were vaccinated early in the COVID-19 primary vaccination
program: therefore they could have decreased immunity against viral colonization
and/or asymptomatic/pauci symptomatic infection.
- Healthcare workers present a risk of transmitting infections especially to vulnerable
patients because in healthcare structures masks are systematically worn during care
by healthcare workers but not always by patients in their rooms during care. In this
context, the SHC reminds the importance of barrier measures and hand hygiene during
care (SHC 9344, 2018) and reminds the procedure from RAG2 that any healthcare
worker found to be PCR positive should be removed from the healthcare system
whether symptomatic or not (except in certain circumstances, cfr RAG report 26 oct
2020).
- Even when vaccinated, the risk of confirmed infection by SARS-CoV-2 exists.
However, a recent publication in a large population (Israël) showed that this risk
decreases by a factor 11 after 15 days following the administration of a booster dose
(Bar-on et al., 2021).
- Healthcare workers will be confronted in the autumn/winter season with the
management of pandemic SARS-CoV-2 patients but also other infectious respiratory
diseases (such as seasonal influenza or RSV). By decreasing the risk of infection with
SARS-CoV-2, a booster dose might help to ensure the sustainability of the healthcare
system. A booster dose has been shown in preliminary data from Israël to be effective
in reducing symptoms.
- The safety data for a booster dose are similar to those for the first and second doses
of the vaccine.
Within this overall context, the SHC recommends that a booster dose of a mRNA
vaccine against COVID-19 should be given to all healthcare workers over 18 years of
age at least 4-6 months after the primary vaccination against COVID-19 essentially to
ensure the sustainability of the healthcare system and to reduce the risk of nosocomial
infections.
Keywords
Keywords Sleutelwoorden Mots clés Schlüsselwörter
Prevention Preventie Prévention Verhütung
Booster Booster Rappel (dose) Booster
COVID-19 COVID-19 COVID-19 COVID-19
Vaccination Vaccinatie Vaccination Impfung
Healthcare Gezondheidswerkers Travailleurs Mitarbeiter des
Workers du secteur de Gesundheitswesens
soins de
santé
2 RAG: Risk Assessment Group
Superior Health Council
www.shc-belgium.be −2−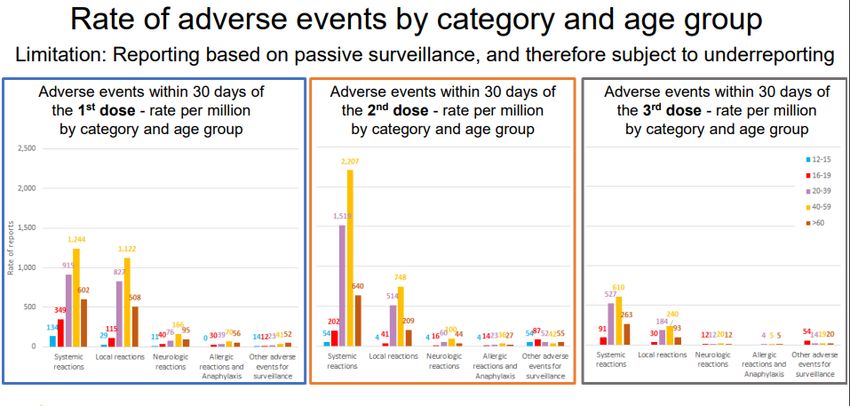
III METHODOLOGY After analysing the request, the Board and Chair of the area Vaccination identified the necessary fields of expertise. An ad hoc working group was then set up which included experts in hospital hygiene, microbiology, infectiology, epidemiology, vaccinology and general medicine. The experts of this working group provided a general and an ad hoc declaration of interests and the Committee on Deontology assessed the potential risk of conflicts of interest. This advisory report is based on a review of the scientific literature published in both scientific journals and reports from national and international organisations competent in this field (peer- reviewed), as well as on the opinion of the experts. Once the advisory report was endorsed by the working group and by the standing working group Vaccination (NITAG), it was ultimately validated by the members of the Board of the SHC. IV ELABORATION AND ARGUMENTATION List of abbreviations used CDC Centers for Disease Control and Prevention CEPI Coalition for Epidemic Preparedness Innovations ECDC European Center for Disease Prevention and Control HCW Healthcare workers NITAG National Immunization Technical Advisory Group RAG Risk Assessment Group SHC Superior Health Council VoC Variants of Concern WHO World Health Organization 1 WHO – statement on the administration of booster doses On October 4 2021, the WHO published a statement on the administration of booster doses. “The current primary goal of immunization in the COVID-19 pandemic remains to protect against hospitalization, severe disease and death. Hence, booster doses may only be needed if there is evidence of insufficient protection against these disease outcomes over time. The degree of waning of immunity and need for booster doses of vaccine may differ between vaccine products, target populations, circulating SARS-CoV-2 virus, in particular variants of concern (VoC), and intensity of exposure. In a period of continued global vaccine supply shortage equity considerations at country, regional and global level remain an essential consideration to assure vaccination of high priority groups in every country. Improving coverage of the primary vaccination series should be prioritized over booster vaccination”. (WHO, Oct 2021) Within the COVAX project, Belgium is collaborating to guarantee fair and equitable access for every country in the world. By the end of October 2021 around 3 million doses of COVID-19 vaccines will be donated by Belgium (https://observablehq.com/@tf-vaccination/belvax). Superior Health Council www.shc-belgium.be −3−
COVAX is co-led by the Coalition for Epidemic Preparedness Innovations (CEPI), Gavi and
the World Health Organization (WHO), alongside key delivery partner UNICEF.
Within the framework of the coordinated European approach 'Team Europe', Belgium gave
priority to the donation of COVID-19 vaccines to the countries of the Western Balkans, the
Eastern Neighbourhood and Southern Europe, as well as to Africa.
2 Vaccination against covid-19 for Healthcare workers
2.1 Four different COVID-19 vaccines used for healthcare workers in Belgium
The four vaccines used against COVID-19 in Belgium became available successively, with
the Comirnaty® vaccine (Pfizer/BioNtech) first (28 December 2020), followed by the Spikevax
vaccine Moderna® (11 January 2021), the Vaxzevria® vaccine (AstraZenecaOxford) (12
February 2021), and finally the COVID-19 Janssen® vaccine (Johnson & Johnson) (28 April
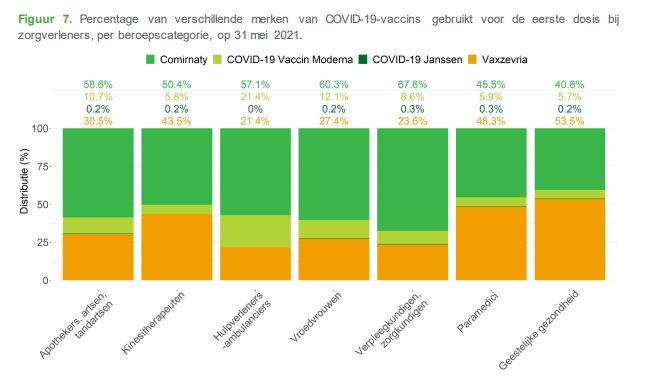
2021). Caregivers were among the first to be vaccinated, with the majority receiving the first
available vaccine, Comirnaty® (61.5%), followed by Vaxzevria® (29.7%). Only a small
proportion of caregivers received the COVID-19 Vaccine Moderna® (8.5 %) or the COVID-19
Janssen® (0.3 %) (Catteau et al., Sciensano 2021).
Figure 1: Percentage of different brands of COVID-19 vaccines used for the first dose among healthcare providers
in Belgium (Sciensano, Catteau et al. 2021)
Superior Health Council
www.shc-belgium.be −4−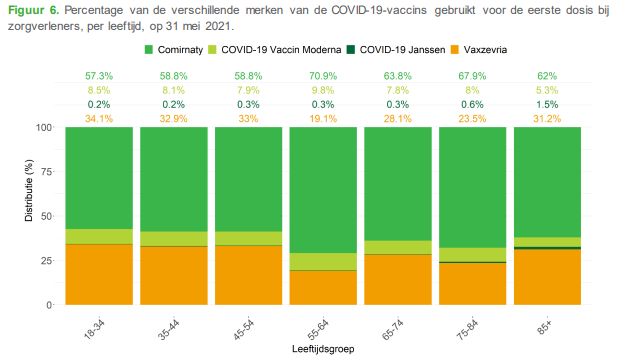
Figure 2. Percentage of different brands of COVID-19 vaccines used for the first dose among health care providers
by professional category (Sciensano, Catteau et al. 2021)
2.2 Vaccine effectiveness
The report of ECDC, published on September 1 2021, gives an update of the evidence on
vaccine effectiveness: https://www.ecdc.europa.eu/sites/default/files/documents/Interim-
public-health-considerations-for-the-provision-of-additional-COVID-19-vaccine-doses.pdf
A (preprint) study by Andrews et al. in the UK showed limited waning in vaccine
effectiveness against hospitalisation and death more than 20 weeks post-vaccination with
Vaxzevria® or Comirnaty®. There was greater waning in protection against hospitalisation
among the oldest age group, except in the 20+ weeks period with Vaxzevria®, though there
was limited data in the 40-64 years group for this period and confidence intervals overlapped
(Andrews et al., 2021).
A (preprint) study by Goldberg et al. from Israel indicated a strong waning in vaccine
effectiveness in all age groups after six months (Goldberg et al. 2021).
2.3 Studies on booster vaccination against Covid-19
The booster dose increases vaccine efficacy in cases of infection and severe forms. For
example, the effectiveness data observed in real life concerning a booster dose of Comirnaty®
vaccine administered first to people aged 60 years or more who were vaccinated with two
doses at least five months previously show a reduction in the risk of infection with Covid-19.
These results show 11.3 times fewer cases of infection and 19.5 times fewer cases of severe
disease among those who received a booster dose than among those who did not (Bar-on et
al., 2021).
Superior Health Council
www.shc-belgium.be −5−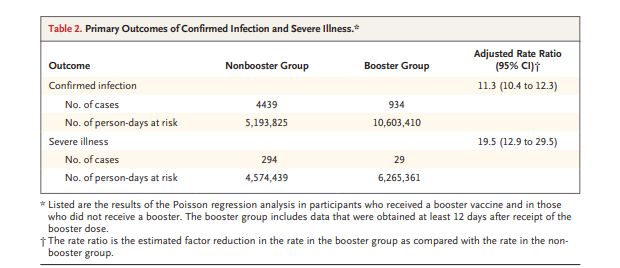
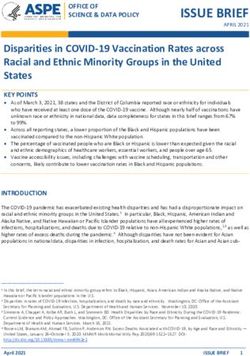
Table. Primary outcome of confirmed infection and severe illness after booster vaccination in Israël (Bar-on et al., 2021) The administration of a booster dose would also reduce the viral load and therefore probably the contagiousness of people who develop an SARS-CoV-2 infection. Falsey et al. administered a third dose of the Pfizer mRNA vaccine 7.9 to 8.8 months after dose 2 to 11 participants 18 to 55 years of age and to 12 participants 65 to 85 years of age. Neutralizing responses were determined after 2 and 3 doses of the mRNA vaccine. They found that 1 month after dose 3, neutralization GMTs against wild-type virus increased to more than 5 times as high (in 18-to-55-year-olds) and to more than 7 times as high (in 65-to-85-year- olds) as the GMTs 1 month after dose 2. Neutralization GMTs against the beta variant increased more after dose 3 than did GMTs against wild-type virus, to more than 15 times as high (in younger adults) and more than 20 times as high (in older adults) as those after dose 2 (figure below). Superior Health Council www.shc-belgium.be −6−
Figure. Neutralizing responses after two and three doses of BNT162b2 (Falsey et al. 2021)
Corbett et al. studied the immune response in nonhuman primates that received primary
vaccination series. Following boost, animals had increased neutralizing antibody responses
across all VOC3, which was sustained for at least 8 weeks post-boost. Nine weeks following
boost, animals were challenged with the SARS-CoV-2 β variant. Viral replication was low to
undetectable in bronchoalveolar lavages and significantly reduced in nasal swabs in all
boosted animals suggesting booster vaccinations may be required to sustain immunity and
protection (Corbett et al., 2021).
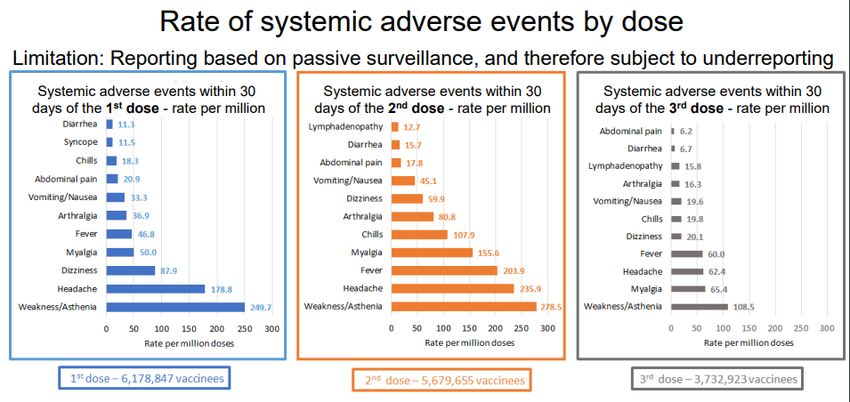
2.4 Safety of booster vaccination
Booster dose in Israel has a safety profile similar to the other doses. Data were presented at
the Vaccines and Related Biological Products Advisory Committee (VRBRAC) of October 14-
15, 2021: https://www.fda.gov/media/153086/download (figures here below)
3
VOC: variant of concern
Superior Health Council
www.shc-belgium.be −7−Superior Health Council www.shc-belgium.be −8−
2.5 Breakthrough infections for healthcare workers
Sciensano presented at the ad hoc meeting of Friday October 22 2021 its preliminary report
on protection offered by COVID-19 vaccines to healthcare workers in Belgium (Sciensano,
non-published data, van Loenhout et al., 2021).
These data showed that the probability of developing a breakthrough infection for healthcare
workers is not higher than for non-healthcare workers until at least 6 months after being fully
immunized.
Figure: Probability of breakthrough infection over time by healthcare worker status. From the 1st of February 2021
to 3th of October 2021; Belgium. No HCW = no healthcare worker, HCW = healthcare worker (Sciensano, 22 Oct
2021)
There was also no larger probability of infection observed for healthcare workers with an
assumed higher risk of exposure than for those with a moderate or low risk of exposure in
Belgium.
A recent study in Qatar showed that a history of contact with a confirmed case and presence
of symptoms were independently associated with higher risk for breakthrough SARS-CoV-2
infection after vaccination. This study also showed a very low rate of breakthrough infections
in healthcare workers (Alishaq et al., Oct 15 2021).
2.6 Transmission of SARS-CoV-2
Limiting the transmission of the SARS-CoV-2 virus and protecting the most vulnerable remains
essential. It is therefore necessary to reinforce the vaccination protection of the populations
most exposed to the virus and likely to transmit the disease to people in contact with them, in
particular if they are at risk of developing a severe form of COVID-19 or dying from it. However,
despite the precautions taken (PPE), a significant number of SARS-CoV-2 infections are still
observed in institutions.
The Oxford University published in pre-print a study conducted by Eyre et al. showing that
vaccination reduces transmission of Delta, but less than the Alpha variant. The impact of
vaccination decreased over time. The authors conclude that booster vaccination may help
controlling transmission together with preventing infections (pre-print, Eyre et al., 2021).
Studies from several countries found significantly reduced likelihood of transmission to
household contacts from people infected with SARS-CoV-2 who were previously vaccinated
for COVID-19 (de Gier et al, 2021; Harris et al., 2021; Layan et al., 2021; Prunas et al., 2021;
Salo et al., 2021; Shah et al., 2021).
Superior Health Council
www.shc-belgium.be −9−Braeye et al. found significant protection against infection after a high-risk contact by a full
schedule of any of the vaccines currently administered in Belgium. Significant effects on
onward transmission in case of breakthrough infections were shown for mRNA-vaccines
(Braeye et al., 2021).
These data suggest that transmission risk is (substantially) reduced in vaccinated people and
that vaccinated people who become infected could be infectious for a shorter period of time
than unvaccinated people.
2.7 Countries recommending a booster dose for HCW
Several countries started vaccinating their HCW such as the USA (CDC), France (HAS), UK
(JCVI) and Germany (STIKO).
3 Recommendation
Vaccinating as many people as possible around the world is essential in managing this
pandemic. Within the COVAX project, Belgium is collaborating to fair and equitable access to
COVID-19 vaccines for every country in the world.
The SHC emphasizes the importance of primary vaccination against COVID-19 of the
general population; the SHC also recommends to make vaccination of workers in the health
care sector mandatory (SHC 9671, 2021). The term "people working in the healthcare sector"
includes all the socio-professional categories listed in the advisory report SHC 9597-9611 of
September 2020. Furthermore, the SHC would like to remind on the advisory report on
vaccination against seasonal influenza (SHC 9625) and simultaneous vaccination (SHC
9675).
Based on currently available data,
- Healthcare workers are at the same risk of both symptomatic and severe infections
and are no more prone to symptomatic or severe infections than the general population
with the same vaccination status.
- Healthcare workers were vaccinated early in the COVID-19 primary vaccination
program: therefore they could have decreased immunity against viral colonization
and/or asymptomatic/pauci symptomatic infection.
- Healthcare workers present a risk of transmitting infections especially to vulnerable
patients because in healthcare structures masks are systematically worn during care
by healthcare workers but not always by patients in their rooms during care. In this
context, the SHC reminds the importance of barrier measures and hand hygiene during
care (SHC 9344, 2018) and reminds the procedure from RAG4 that any healthcare
worker found to be PCR positive should be removed from the healthcare system
whether symptomatic or not (except in certain circumstances, cfr RAG report 26 oct
2020).
- Even when vaccinated, the risk of confirmed infection by SARS-CoV-2 exists.
However, a recent publication in a large population (Israël) showed that this risk
decreases by a factor 11 after 15 days following the administration of a booster dose
(Bar-on et al., 2021).
- Healthcare workers will be confronted in the autumn/winter season with the
management of pandemic SARS-CoV-2 patients but also other infectious respiratory
diseases (such as seasonal influenza or RSV). By decreasing the risk of infection with
SARS-CoV-2, a booster dose might help to ensure the sustainability of the healthcare
4 RAG: Risk Assessment Group
Superior Health Council
www.shc-belgium.be − 10 −system. A booster dose has been shown in preliminary data from Israël to be effective
in reducing symptoms.
- The safety data for a booster dose are similar to those for the first and second doses
of the vaccine.
Within this overall context, the SHC recommends that a booster dose of a mRNA
vaccine against COVID-19 should be given to all healthcare workers over 18 years of
age at least 4-6 months after the primary vaccination against COVID-19 essentially to
ensure the sustainability of the healthcare system and to reduce the risk of nosocomial
infections.
Superior Health Council
www.shc-belgium.be − 11 −V REFERENCES
- Alishaq M, Nafady-Hego H, Jeremijenko A, et al. Risk factors for breakthrough SARS-
CoV-2 infection in vaccinated healthcare workers. PLoS One. 2021;16(10):e0258820.
Published 2021 Oct 15. doi:10.1371/journal.pone.0258820
https://journals.plos.org/plosone/article?id=10.1371/journal.pone.0258820
- Andrews N, Tessier E, Stowe J, Gower C, Kirsebom F, Simmons R et al. Vaccine
effectiveness and duration of protection of Comirnaty, Vaxzevria and Spikevax against
mild and severe COVID-19 in the UK. Oct 6, 2021 MedRxiv preprint doi:
https://doi.org/10.1101/2021.09.15.21263583;
- Bar-On YM, Goldberg Y, Mandel M, Bodenheimer O, Freedman L, Kalkstein N et al.
Protection of BNT162b2 Vaccine Booster against Covid-19 in Israel. N Engl J Med.
2021. doi: 10.1056/NEJMoa2114255.
https://www.nejm.org/doi/full/10.1056/NEJMoa2114255
- Bergwerk M, Gonen T, Lustig Y, Amit S, Lipsitch M, Cohen C et al. Covid-19
Breakthrough Infections in Vaccinated Health Care Workers. New England Journal of
Medicine. 2021. doi: 10.1056/NEJMoa2109072.
- Braeye T, Cornelissen L, Catteau L, Haarhuis F, Proesmans K, De Ridder K, et al.
Vaccine effectiveness against infection and onwards transmission of COVID-19:
Analysis of Belgian contact tracing data, January-June 2021. Vaccine. 2021 Aug
19;S0264-410X(21)01108-7.
- Catteau L. Billuart M., Serrien B., Hubin P. Haarhuis F., Lizroth A., Stouten V.,
Wyndham Thomas C. Surveillance van COVID-19 vaccinatie bij zorgverleners in
België. Intermediaire resultaten tot en met 31 mei 2021. Brussel, België: Sciensano;
2021. Wettelijk depotnummer: D/2021/14.440/46. https://covid-
19.sciensano.be/sites/default/files/Covid19/COVID-
19_THEMATIC%20REPORT_SURVEILLANCE_VAN_DE_VACCINATIE_BIJ_ZORG
VERLENERS_1.pdf
- CDC – Centers for Disease Control and Prevention. Statement on ACIP Booster
Recommendations https://www.cdc.gov/media/releases/2021/p0924-booster-
recommendations-.html
- CDC - Evidence to Recommendation Framework: Pfizer-BioNTech COVID-19 Booster
Dose. ACIP Meeting September 23, 2021.
https://www.cdc.gov/vaccines/acip/meetings/downloads/slides-2021-9-23/03-COVID-
Oliver.pdf
- Considerations in boosting COVID-19 vaccine immune responses. Lancet. 2021. doi:
10.1016/S0140-6736(21)02046-8.
- COVAX project. https://www.who.int/initiatives/act-accelerator/covax
- Corbett S., Gagne M., Wagner D., O’Conelle S., Narpala S., et al. Protection against
SARS-CoV-2 beta variant in mRNA-1273 vaccine–boosted nonhuman primates.
Science. 21 Oct 2021. DOI: 10.1126/science.abl8912
- de Gier B, Andeweg S, Joosten R, Ter Schegget R, Smorenburg N, van de Kassteele
J, et al. Vaccine effectiveness against SARS-CoV-2 transmission and infections
among household and other close contacts of confirmed cases, the Netherlands,
February to May 2021. Euro Surveill. 2021;26(31).
- European Centre for Disease Prevention and Control. Interim public health
considerations for the provision of additional COVID-19 vaccine doses, 1 September
2021. ECDC: Stockholm; 2021.
https://www.ecdc.europa.eu/sites/default/files/documents/Interim-public-health-
considerations-for-the-provision-of-additional-COVID-19-vaccine-doses.pdf
- Eyre D., Taylor D., Purver M., Chapman D., Fowler T et al. The impact of SARS-CoV-
2 vaccination on Alpha & Delta variant transmission. Preprint. medRxiv
2021.09.28.21264260; doi: https://doi.org/10.1101/2021.09.28.21264260
https://www.medrxiv.org/content/10.1101/2021.09.28.21264260v2
Superior Health Council
www.shc-belgium.be − 12 −- Falsey A et al. SARS-CoV-2 Neutralization with BNT162b2 Vaccine Dose 3. Oct 21,
2021. N Engl J Med 2021; 385:1627-1629. DOI: 10.1056/NEJMc2113468.
https://www.nejm.org/doi/full/10.1056/NEJMc2113468
- FDA – Food and drug administration https://www.fda.gov/advisory-
committees/advisory-committee-calendar/vaccines-and-related-biological-products-
advisory-committee-september-17-2021-meeting-announcement#event-materials
- Goldberg Y, Mandel M, Bar-On Y, Bodenheimer O, Freedman L et al. Waning immunity
of the BNT162b2 vaccine: A nationwide study from Israel. Preprint
doi: https://doi.org/10.1101/2021.08.24.21262423
https://www.medrxiv.org/content/10.1101/2021.08.24.21262423v1
- Harris RJ, Hall JA, Zaidi A, Andrews NJ, Dunbar JK, Dabrera G. Effect of Vaccination
on Household Transmission of SARS-CoV-2 in England. N Engl J Med.
2021;385(8):759-60.
- JCVI statement regarding a COVID-19 booster vaccine programme for winter 2021 to
2022. 14 September 2021. https://www.gov.uk/government/publications/jcvi-
statement-september-2021-covid-19-booster-vaccine-programme-for-winter-2021-to-
2022/jcvi-statement-regarding-a-covid-19-booster-vaccine-programme-for-winter-
2021-to-2022
- Haute Autorité de Santé. Covid-19 : la HAS élargit le périmètre de la dose de rappel.
6 octobre 2021
https://www.has-sante.fr/jcms/p_3290677/fr/covid-19-la-has-elargit-le-perimetre-de-
la-dose-de-rappel
https://www.has-sante.fr/jcms/p_3283044/fr/avis-n-2021-0061/ac/seesp-du-23-aout-
2021-du-college-de-la-has-relatif-a-la-definition-des-populations-a-cibler-par-la-
campagne-de-rappel-vaccinal-chez-les-personnes-ayant-eu-une-primovaccination-
complete-contre-la-covid-19
- Hoge Gezondheidsraad. Gelijktijdige toediening van vaccins tegen COVID-19 met
andere vaccins (Simultane vaccinatie). Brussel: HGR; 2021. Advies nr. 9675.
- Hoge Gezondheidsraad. Aanbevelingen inzake handhygiëne tijdens de zorgverlening
- (vorig advies HGR 8349). Brussel: HGR; 2018 HGR 9344.
- Hoge Gezondheidsraad. Aanbevelingen voor het prioriteren van subgroepen van
patiënten jonger dan 65 jaar voor vaccinatie tegen SARS-CoV-2 (fase Ib). Brussel:
HGR; 2021. Advies nr. 9618.
- Hoge Gezondheidsraad. Aanbevelingen voor de vaccinatie tegen SARS-CoV-2 met
messenger-RNA-vaccins (Pfizer/ Moderna) van vrouwen die zwanger zijn, willen
worden of borstvoeding geven. Brussel: HGR; 2021. Advies nr. 9622.
- Hoge Gezondheidsraad. Vaccinatie tegen seizoensgebonden griep - Winterseizoen
2021-2022. Brussel: HGR; 2021. Advies nr. 9625.
- Hoge Gezondheidsraad. Vaccinatie tegen COVID-19 voor personeel uit de
gezondheidssector: Noodzaak voor verdere omkadering tot verplichting? Brussel:
HGR; 2021. Advies nr 9671
- Layan M, Gilboa M, Gonen T. Impact of BNT162b2 vaccination and isolation on SARS-
CoV-2 transmission in Israeli households: an observational study. medRxiv.
2021;https://www.medrxiv.org/content/10.1101/2021.07.12.21260377v1
- Magnusson K, Nygard K, Methi F, et al. Occupational risk of COVID-19 in the first
versus second epidemic wave in Norway, 2020. https://doi.org/10.2807/1560-
7917.ES.2021.26.40.2001875.
https://www.eurosurveillance.org/content/10.2807/1560-
7917.ES.2021.26.40.2001875?emailalert=true
- Marks M, Millat-Martinez P, Ouchi D, Roberts CH, Alemany A, Corbacho-Monne M, et
al. Transmission of COVID-19 in 282 clusters in Catalonia, Spain: a cohort study.
Lancet Infect Dis. 2021.
- Prunas O, Warren JL, Crawford FW, et al. Vaccination with BNT162b2 reduces
transmission of SARS-CoV-2 to household contacts in Israel. medRxiv.
2021;https://www.medrxiv.org/content/10.1101/2021.07.13.21260393v1
Superior Health Council
www.shc-belgium.be − 13 −- RAG. Health staff with covid-19 infection. 26 October 2020. https://covid-
19.sciensano.be/sites/default/files/Covid19/20201026_Advice_RAG_COVID%2B%20
health%20workers.pdf
- RKI: https://www.rki.de/DE/Content/Kommissionen/STIKO/Empfehlungen/PM_2021-
10-07.html
https://www.rki.de/DE/Content/Infekt/EpidBull/Archiv/2021/Ausgaben/43_21.pdf?__bl
ob=publicationFile
- Salo J, Hagg M, Kortelainen M, et al. The indirect effect of mRNA-based Covid-19
vaccination on unvaccinated household members. medRxiv.
2021;https://www.medrxiv.org/content/10.1101/2021.05.27.21257896v2.
- Shah A, Gribben C, Bishop J, et al. Effect of vaccination on transmission of COVID-
19: an observational study in healthcare workers and their households. medRxiv.
2021;https://www.medrxiv.org/content/10.1101/2021.03.11.21253275v1
- Smriti Mallapaty. Nature 05 October 2021. COVID vaccines cut the risk of transmitting
Delta — but not for long. doi: https://doi.org/10.1038/d41586-021-02689-y
- WHO. Interim statement on booster doses for COVID-19 vaccination. Oct 4,2021.
https://www.who.int/news/item/04-10-2021-interim-statement-on-booster-doses-for-
covid-19-vaccination
Superior Health Council
www.shc-belgium.be − 14 −VI COMPOSITION OF THE WORKING GROUP
The composition of the Committee and that of the Board as well as the list of experts appointed
by Royal Decree are available on the following website: About us.
All experts joined the working group in a private capacity. Their general declarations of
interests as well as those of the members of the Committee and the Board can be viewed on
the SHC website (site: conflicts of interest).
An ad hoc meeting was organised on Friday October 22, 2021. Based on the discussions and
conclusions of this meeting, this advisory report was drafted and send for approval to the
standing working group Vaccination (NITAG) by email on Wednesday October 27, 2021. The
following experts participated at the ad hoc meeting and/or approval of the report. The
standing and ad hoc working group were chaired by Yves VAN LAETHEM; the scientific
secretariat were Veerle MERTENS, Fabrice PETERS and Muriel BALTES.
BEUTELS Philippe Health Economics UAntwerpen
BLUMENTAL Sophie Infectiology HUDERF
BYL Baudouin Hospital Hygiene, Epidemiology CHU Erasme, ULB
CALLENS Steven Infectiology, Internal medicine UZ Gent
CHATZIS Olga Pediatrics, Vaccinology UCL
CORNELISSEN Laura Epidemiology, Obstetrics, Sciensano
Gynaecology
DAELEMANS Siel Infectiology, Vaccinology, Travel clinic UZBrussel
DE LOOF Geert General medicine BCFI
DE SCHEERDER Marie- Internal medicine, Infectiology, Travel UZ Gent
Angélique clinic, HIV
DESMET Stefanie Microbiology UZ Leuven
DOGNE Jean- Michel Farmacovigilance UNamur, EMA
FLAMAING Johan Geriatrics KU Leuven
FRERE Julie Pediatrics, Infectiology CHU Liège
GERARD Michèle Hospital Hygiene, Infectiology CHU St Pierre, ULB
LEROUX-ROELS Isabel Vaccinology, Infection prevention, UZ Gent
Microbiology
MANIEWSKI Ula Infectiology, Tropical infectious ITG-IMT
diseases, Vaccinology
MALFROOT Anne Pediatrics, Infectiology UZ Brussel
PELEMAN Renaat Infectiology, Vaccinology UZ Gent
ROBERFROID Epidemiology KCE, UNamur
Dominique
SCHELSTRAETE Petra Pediatrics, Pneumology, Vaccinology UGent
SCHOEVAERDTS Geriatrics UCLouvain
Didier
SIMON Anne Microbiology, Hospital hygiene Jolimont
SOENTJENS Patrick Internal medicine, Tropical infectious ITG - Defensie
diseases
SWENNEN Béatrice Epidemiology, Vaccinology ULB
THEETEN Heidi Vaccinology UAntwerpen
Superior Health Council
www.shc-belgium.be − 15 −TILMANNE Anne Pediatrics, Infectiology CHU TIVOLI
TUERLINCKX David Pediatrics, Vaccinology CHU UCL Namur
VAN DAMME Pierre Epidemiology, Vaccinology UAntwerpen
VAN DER LINDEN Pediatrics, Infectiology UCLouvain
Dimitri
VAN KERSSCHAEVER General Medicine Domus Medica
Greet
VAN LAETHEM Yves Infectiology, Vaccinology, Travel CHU Saint-Pierre, ULB
medicine, HIV
VAN LOENHOUT Joris Epidemiology, Infectiology Sciensano
VANDEN DRIESSCHE Pediatrics, Immunology, Pneumology UZA
Koen
VERHAEGEN Jan Microbiology, Bacteriology UZ Leuven
WAETERLOOS Quality of vaccines and blood products Sciensano
Geneviève
WYNDHAM-THOMAS Epidemiology, Infectiology Sciensano
Chloé
The following experts or administrations were heard but did not take part in endorsing the
advisory report.
CARRILLO ONE
SANTISTEVE Paloma
DAEMS Joël RIZIV-INAMI
Superior Health Council
www.shc-belgium.be − 16 −www.css-hgr.be
This publication cannot be sold.
federal public service
HEALTH, FOOD CHAIN SAFETY
AND ENVIRONMENTYou can also read