2023 SUMMARY OF BENEFITS - CCA Health Michigan CCA Medicare Maximum (HMO D-SNP) - 23900 Orchard Lake Road, Ste 210 Farmington Hills, MI 48336 ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
2023 SUMMARY OF BENEFITS CCA Health Michigan CCA Medicare Maximum (HMO D-SNP) 23900 Orchard Lake Road, Ste 210 Farmington Hills, MI 48336 H9861-003 H9861_23_048_M

INTRODUCTION TO SUMMARY OF BENEFITS H9861-003 CCA Health Michigan January 1, 2023 – December 31, 2023 CCA Medicare Maximum (HMO D-SNP) is a Coordinated Care plan with a Medicare contract and a contract with the Michigan Department of Health & Human Services. Enrollment in this Reliance plan depends on contract renewal. The benefit information provided does not list every service that we cover or list every limitation or exclusion. To get a complete list of services we cover, please request the “Evidence of Coverage (EOC).” WHO CAN JOIN? Your eligibility to enroll in this plan depends on your type of Medicaid. You must be entitled to Medicare Part A, be enrolled in Medicare Part B, and live in our service area (Genesee, Macomb, Oakland, St. Clair, Lapeer, Wayne counties) and also receive certain levels of assistance from the Michigan Medical Assistance program (Medicaid). If you receive both Medicare and Medicaid benefits, this means you are a dual eligible. You can enroll in this plan if you are in one of these Medicaid categories: Qualified Medicare Beneficiary Plus (QMB+): You get Medicaid coverage of Medicare cost-share and are also eligible for full Medicaid benefits. Medicaid pays your Part A and Part B premiums, deductibles, coinsurance and copayment amounts. You pay nothing, except for Part D prescription drug copays. Qualified Medicare Beneficiary (QMB): You get Medicaid coverage of Medicare cost-share but are not eligible for full Medicaid benefits. Medicaid pays your Part A and Part B premiums, deductibles, coinsurance and copayment amounts only. You pay nothing, except for Part D prescription drug copays. Specified Low-Income Medicare Beneficiary (SLMB+): Medicaid pays your Part B premium and provides full Medicaid benefits. You are eligible for full Medicaid benefits. At times you may also be eligible for limited assistance from your state Medicaid agency in paying your Medicare cost share amounts. Generally, your cost share is 0% when the service is covered by both Medicare and Medicaid.
WHICH DOCTORS, HOSPITALS, AND MEMBER SERVICE
PHARMACIES CAN I USE? INFORMATION
This Plan has a network of doctors, hospitals, For more information, please call us at
pharmacies, and other providers. Except in 855-959-5855 (TTY users should call 711).
emergency situations, if you use the providers
that are not in our network, CCA Health may Hours are 8 a.m. to 8 p.m., seven days a week from
not pay for these services. October 1 through March 31, except holidays, and 8
a.m. to 8 p.m., Monday through Friday, from April 1
For coverage and costs of Original Medicare, through September 30, except holidays. Messages
look in your current “Medicare & You” handbook. received on holidays and outside of our business
View it online at www.medicare.gov or get a copy hours will be returned within one business day. Or
by calling 1-800-MEDICARE (1-800-633-4227). visit us at ccahealthmi.org.
TTY users should call 1-877-486-2048.
You can get this document for free in other formats, such as large print, braille, or
audio. Call 855-959-5855 (TTY 711), 8 am to 8 pm, 7 days a week, from October 1 to
March 31. (April 1 to September 30: 8 am to 8 pm, Monday to Friday.) The call is free.CCA Medicare Maximum (HMO D-SNP)
Premiums & Benefits
H9861-003
Monthly Plan Premium* $0 Premium
Annual Medical Deductible No Deductible
Maximum
$0
Out-of-Pocket Costs
$0
In-Patient Hospital Stays
Authorization may be required
$0
Outpatient Hospital
Authorization may be required
Primary Care Copay $0
Specialist Copay $0
Preventive Care
$0
(e.g., flu vaccine, diabetic screenings)
Emergency Care $0
Urgently Needed Services $0
Lab Services $0
X-ray Services $0CCA Medicare Maximum (HMO D-SNP)
Premiums & Benefits
H9861-003
$0 annual exam
Hearing Services
You get up to $2,000 per year for 2 aids (1 per ear) every year
Dental Services
Dental Services are provided by
Delta Dental of Michigan. Limitations
and exclusions apply. You can reach $3,500 a year including dentures and crowns
Delta Dental of Michigan’s Member
Services Department at 800-330-2732 Prior authoization may be required
with questions about your dental
benefits Please contact Delta Dental
of Michigan prior to accessing
services to confirm benefits
Vision Services $300 flexible spending card for routine vision exams or eyewear
Mental Health Services $0
Skilled Nursing Facility $0
Physical Therapy $0
Ambulance $0CCA Medicare Maximum (HMO D-SNP)
Premiums & Benefits
H9861-003
Transportation (scheduled by CCA) 50 1-way medical trips
Medicare Part B Drugs $0
Outpatient Prescription Drugs
CCA Medicare Maximum (HMO D-SNP)
H9861-003
Phases of Part D Benefit
Deductible $0
Initial Coverage
Tier 1: Preferred Generic You pay $0 per prescription
Tier 2: Non-Preferred Generic You pay $0 per prescription
Tier 3: Preferred Brand You pay $0 per prescription
Tier 4: Non-Preferred Brand You pay $0 per prescription
Tier 5: Speciality Tier You pay $0 per prescriptionOutpatient Prescription Drugs
CCA Medicare Maximum (HMO D-SNP)
H9861-003
Once your total drug costs have reached $4,660,
Catastrophic Coverage
you will move to the next stage
Select Insulins $0 copay
Additional Benefits
CCA Medicare Maximum (HMO D-SNP)
H9861-003
Acupuncture, Chiropractic $0 for 20 acupuncture/chiropractic visits combined
Silver and Fit Program Benefits $0 membership that also includes a home fitness kit
In-home Support
60 hours per year
(non medical) – Papa Health
Over the Counter (OTC) Benefit
Up to $2,400 per year ($600 per quarter) for
Please visit our website to see our list of
over-the-counter health products or food**
covered itemsAdditional Benefits
CCA Medicare Maximum (HMO D-SNP)
H9861-003
Caregiver Support American House after hospital benefit up to 14 days
Routine Foot Care $0 for 5 visits
Meals 14 meals (7 days) post hospital discharge
Telehealth $0
Durable Medical Equipment (DME) $0
Sneakers $100 allowance each year**
Utility Flex Card $50 per month for gas, electric, or cable**
*You may need to continue to pay your Medicare Part B premium.
**Some extra benefits are special supplemental benefits, which not all members will qualify for. Contact the plan for more
information.
The above chart reflects in-network costs. Costs may vary depending on plan type, product, or service. For details on
out-of-network costs, see the Plus Evidence of Coverage document or the Choice Evidence of Coverage document.NOTICE OF NONDISCRIMINATION
Commonwealth Care Alliance, Inc.® complies with identity), sexual orientation, national origin, race, color,
applicable Federal civil rights laws and does not religion, creed, public assistance, or place of residence,
discriminate on the basis of, or exclude people or treat you can file a grievance with:
them differently because of, medical condition, health
status, receipt of health services, claims experience, OptumRx Civil Rights Coordinator
medical history, disability (including mental impairment), 11000 Optum Circle
marital status, age, sex (including sex stereotypes and Eden Prairie, MN 55344
gender identity), sexual orientation, national origin, race, Phone: 1-800-562-6223 (TTY 711)
color, religion, creed, public assistance, or place of Fax: 855-351-5495
residence. Commonwealth Care Alliance, Inc.: Email: optum_civil_rights@optum.com
• Provides free aids and services to people with You can file a grievance in person or by mail, fax, or
disabilities to communicate effectively with us, such as: email. If you need help filing a grievance, the OptumRx
- Qualified sign language interpreters Civil Rights Coordinator is available to help you.
- Written information in other formats (large print,
audio, accessible electronic formats, other formats) You can also file a civil rights complaint with the U.S.
• Provides free language services to people whose Department of Health and Human Services, Office for
primary language is not English, such as: Civil Rights, electronically through the Office for Civil
- Qualified interpreters Rights Complaint Portal, available at ocrportal.hhs.gov/
- Information written in other languages ocr/portal/lobby.jsf, or by mail or phone at:
If you need these services, contact Member Services. U.S. Department of Health and Human Services
200 Independence Avenue, SW
If you believe that Commonwealth Care Alliance, Inc. Room 509F, HHH Building
has failed to provide these services or discriminated in Washington, D.C. 20201
another way based on medical condition, health status, Phone: 800-368-1019, 800-537-7697 (TDD)
receipt of health services, claims experience, medical
history, disability (including mental impairment), marital Complaint forms are available at www.hhs.gov/ocr/
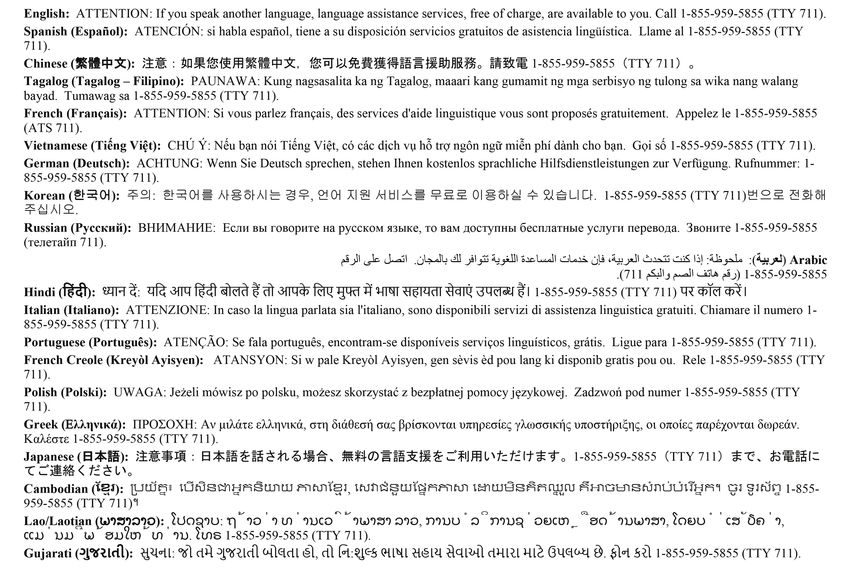
status, age, sex (including sex stereotypes and gender office/file/index.html.MULTI-LANGUAGE INTERPRETER SERVICES
You can also read