2022 Inter-Plan Medicare and Provider Engagement - Advantage Care Management Program - Highmark Inc. Confidential and Proprietary - Do Not Distribute
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Highmark Inc. Confidential and Proprietary – Do Not Distribute
2022 Inter-Plan Medicare
Advantage Care Management
and Provider Engagement
Program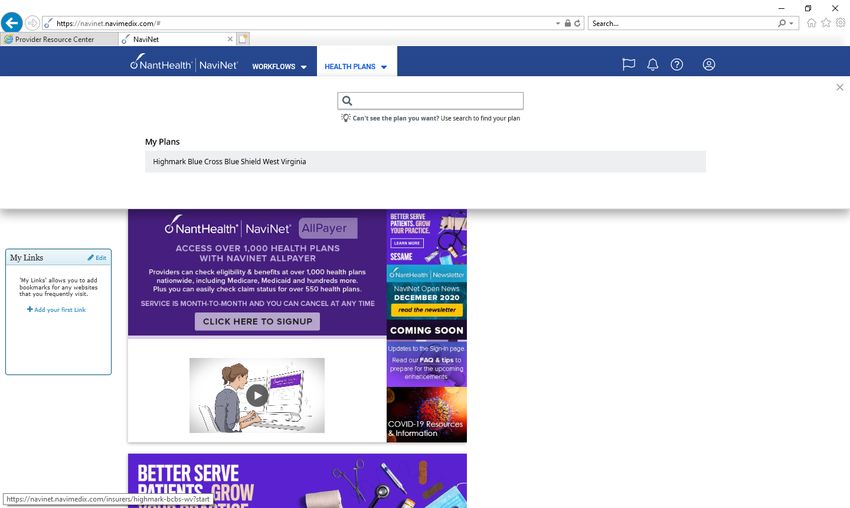
This presentation is the property of Highmark Health and is proprietary and confidential.
The material contained in it is educational and informational, is intended for this audience
only, and cannot be rebroadcasted to unapproved audiences. This presentation may not be
recorded in any manner including, without limitation, audio, video, photograph, screenshot,
or by any other means or in any other media. Broadcasting, publication, or sharing of these
materials without Highmark’s expressed permission is strictly prohibited.
Property and Confidential | 2022
Best Practices Disclaimer:
The guidance, best practices and guidelines (referred to as “best practices”) provided to you are presented
for your consideration and assessment only. They were selected from among best practices published by
various associations and organizations or discussed in studies and articles on the subject. Please assess
whether the described best practices are appropriate for you. There are no requirements that you use the
best practices, and the best practices are not required for any Highmark program or initiative. Please note
that the successful implementation of any program or initiative depends upon many factors and variables.
Therefore, Highmark makes no representation with respect to the described best practices and whether the
practices will positively impact your reimbursement, value-based payment or performance under a
Highmark program or initiative.
The best practices are not intended to situate Highmark as a provider of medical services or dictate the
diagnosis, care or treatment of patients. Your medical judgment remains independent with respect to all
medically necessary care to your patients.
Proprietary and Confidential | 2021
Agenda
1. Inter-Plan Program Overview
2. Risk Adjustment Programs
3. Education and Support for Risk
4. Annual Wellness Visits
5. HOS and CAHPS
Property and Confidential | 2022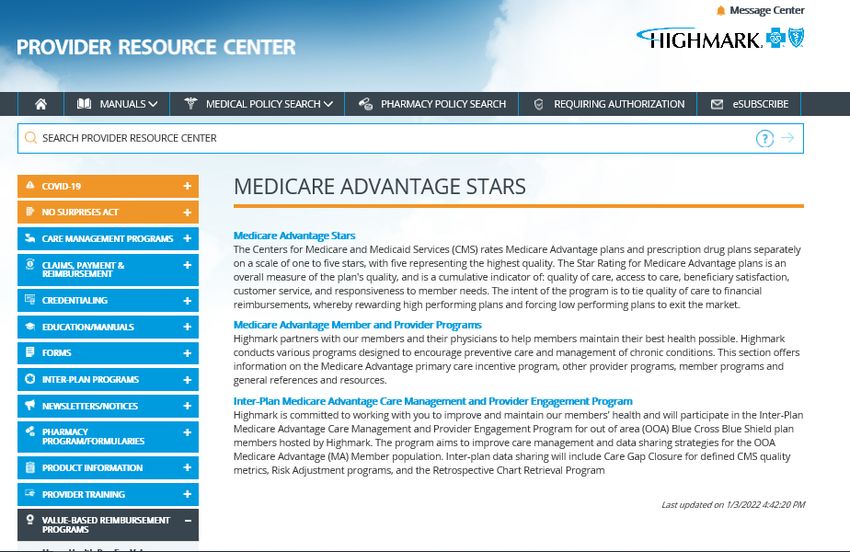
2022 Inter-Plan MA Care Management & Provider Engagement Program
Intent
• To increase the quality of members’ care by enabling Host BCBS MA members to receive appropriate care, wherever they access care.
• Improve the health and wellness of our Host Blue Cross Blue Shield members (your patients) by meeting CMS established Star Measure
benchmarks. Support providers with additional information about open gaps in care.
• Per the program structure, Stars or risk adjustment gaps for these members will be communicated through Highmark’s local processes.
• To facilitate a healthcare consciousness of population health management.
• To improve the quality of care for the Host Blue Cross Blue Shield Medicare Advantage population through enhanced collaboration and
claims data sharing.
Population Inclusions
• Applies to Highmark HOSTED Medicare Advantage population only
• Highmark hosted members are Blue Cross Blue Shield (BCBS) Medicare Advantage members who received care within the Highmark
Provider Network and pay insurance premium to another BSBC plan outside of the Highmark footprint.
Property and Confidential | 2022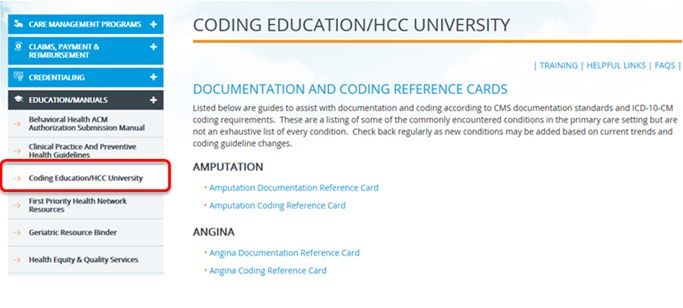
Program Eligibility
Eligible Practices HOSTED Attribution
• All Highmark Providers and practices within • This national program is dependent on member
Highmark’s provider network that treat and attribution results of BCBS HOME plans. Attribution
provide services to Highmark HOSTED BCBS will be defined and identified by the HOSTED
Medicare Advantage members. Members’ BCBS HOME plan, which is the plan to
which the member pays their premium.
• Eligibility is inclusive of those under Highmark’s
True Performance Program contracts and • Highmark does NOT generate the attribution therefore
Medicare Advantage Standalone programs. this attribution can/may differ from the corporate
Highmark attribution logic.
• The identified MA Highmark Hosted members will
not be included in Highmark’s aggregated stars • Member attribution and enrollment files will update
score calculations. monthly through the entire year
Property and Confidential | 2022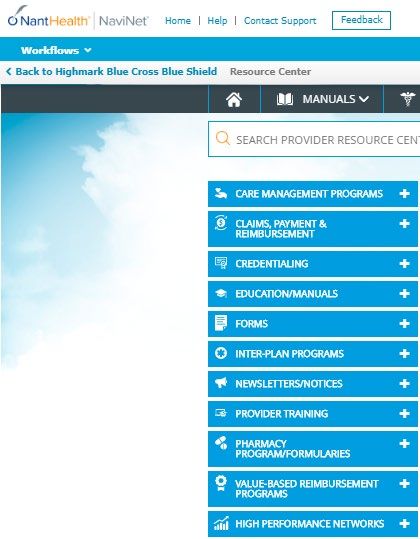
Inter-Plan MA Care Management & Provider Engagement Program
Difference from other Highmark Value Based Reimbursement Programs
• Highmark does NOT generate the attribution
• All Highmark Providers and member attribution are determined by the BCBS HOME plans.
• This attribution may differ from the corporate Highmark attribution logic that is used in other value-based
reimbursement programs.
• The identified MA Highmark Hosted members will not be included in Highmark’s aggregated stars score
calculations
• This program is separate from all other Highmark value-based reimbursement programs
• Highmark specific supplemental data sources are NOT open to HOSTED Members as part of this Program.
Property and Confidential | 2022
Clinical Quality Measure Set Static Measures Dynamic Measures
This program is structured to assess and HBA1c Controlled for Patients with
improve the process of care for Blue Cross Breast Cancer Screening
Diabetes (≤9%)
Blue Shield Highmark HOSTED Medicare
Advantage patients by their primary care Colorectal Cancer Screening Controlling High Blood Pressure
practices using specific CMS Stars
measures as the clinical quality component. Osteoporosis Management in Women with a
Medication Adherence for Hypertension
Fracture
Medication Adherence for Diabetes
Eye Exam for Patients with Diabetes
Static Measures are included in Medications
Quarterly Per Gap Closure
Compensation Comprehensive Diabetes Care: Medical Attention
Medication Adherence for Cholesterol
for Nephropathy **
Dynamic Measures Included in End
of Year Per Gap Closure Statin Therapy For Cardiovascular Disease
Compensation
Statin Use in Patients with Diabetes
Medication Therapy Management
TRC Medication Reconciliation Post Discharge
**Measure Retired on 4/26/2022
Property and Confidential | 2022
Quality Care Gap Closure
Care gaps assessed in the Program measure sets are categorized as either Static or Dynamic
based on when they can be considered “closed.”
Dynamic Care Gaps
Dynamic measures (care gaps) can
Static measures (care gaps)
close and reopen throughout the year
can be definitively closed prior
and require appropriate care
Static Care Gaps
to year end via claims.
management throughout the year.
Compliance rates will typically
Medication compliance rates will
start very low and steadily
typically start high and decrease
increase throughout the year.
throughout the year.
Each static CMS Star measure
Members/dynamic measures can be
care gap closed from 1/1/2022
flagged as “beyond remediation” if the
-12/31/2022 is eligible to
care gap cannot be "closed" based on
receive a care gap closure
the remaining time in the program
incentive.
measurement year.
Property and Confidential | 2022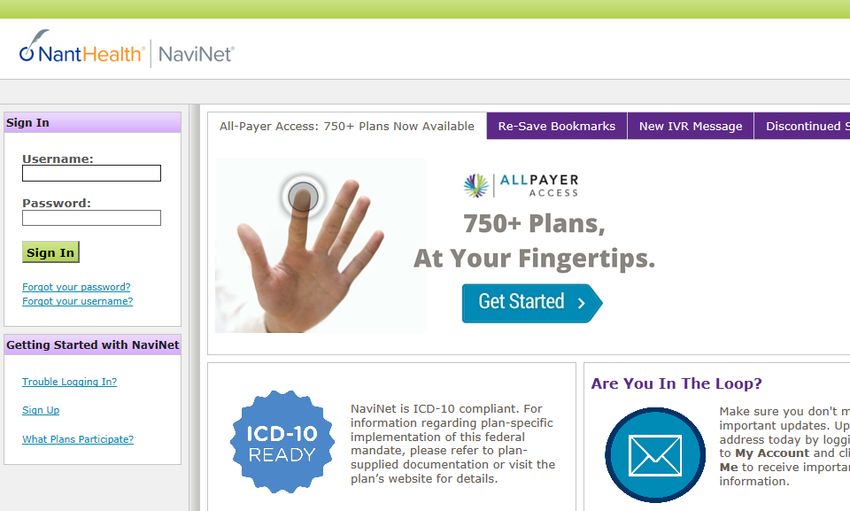
2022 Inter-Plan MA Care Management & Provider Engagement Program
Care Gap Closure Compensation
• 14 CMS Star measures are included and assessed for the • Static measures that are addressed and closed
Quality Care Gap Program. between January 1 and December 31, 2022 are eligible
for the $10 compensation payment per gap closed.
• 9 Star metrics which can be definitively closed prior to • Dynamic CMS measures that met compliance for
year-end via claims are denoted as “static” on the monthly calendar year 2022 are eligible for the following
care gap reports compensation:
• Medication adherence measures - $20 payment
• 5 CMS Star metrics which are resulted based upon for each member who complete the year with a >
member compliance as of 12/31/2022 may require 80% PDC rate
ongoing member monitoring and population management • SUPD compliance: $20/member payment
to ensure members receive the expected care are denoted • HbA1c Controlled compliance : $10/member
as “dynamic” on the monthly care gap reports. payment
• Controlling High Blood Pressure: $10/member
• Static care gap closure earnings will be calculated and payment
dispersed quarterly
• Results calculated in April 2023 allowing a 90-day
• Dynamic care gap closure will be calculated and claims run out following the calendar year end for 2022
dispensed June 2022. dates of service
Property and Confidential | 2022Program Enrollment
Enrollment Purpose: During the education and program roll out period, all
practices that meet the eligibility requirements may enroll for
participation. Program enrollment will remain open
• Ensure auditable trail of program participation throughout 2022.
election and structural understanding and
provider education. • Enrollment via electronic portal (NaviNet) including:
• Download of program manual
• Download of program education presentation
• Identify engaged practices for
provider engagement strategy • Attestation that materials have been received, reviewed,
planning. and understood.
• Practice contact information for any needed clarification.
• Ensure the accuracy and
integrity of risk adjustment
data submitted to CMS.
• Enrollment requested at the practice level, but can be
submitted at the entity level (practice Blue Shield ID)
• Improve the • Regardless of enrollment date (during enrollment period),
health &
wellness of
all performance for the program measurement period
HOSTED (calendar year) will be included in program.
members
Property and Confidential | 2022ACCESSING NAVINET https://navinet.navimedix.com
Log in to NaviNet by going to
https://navinet.navimedix.com/
Enter your Username and Password.
Click Sign In.
Property and Confidential | 2022ACCESSING NAVINET https://navinet.navimedix.com
Log in to NaviNet by going to
https://navinet.navimedix.com/
Enter your Username and Password.
Click Sign In.
For a direct link to the attestation
page, visit
https://highmark.co1.qualtrics.co
m/jfe/form/SV_cNELxYv3jcRH8BU
Property and Confidential | 2022Choose the appropriate
Highmark Plan from the
dropdown
Property and Confidential | 2022Select the Resource Center
to be redirected to the
Highmark website
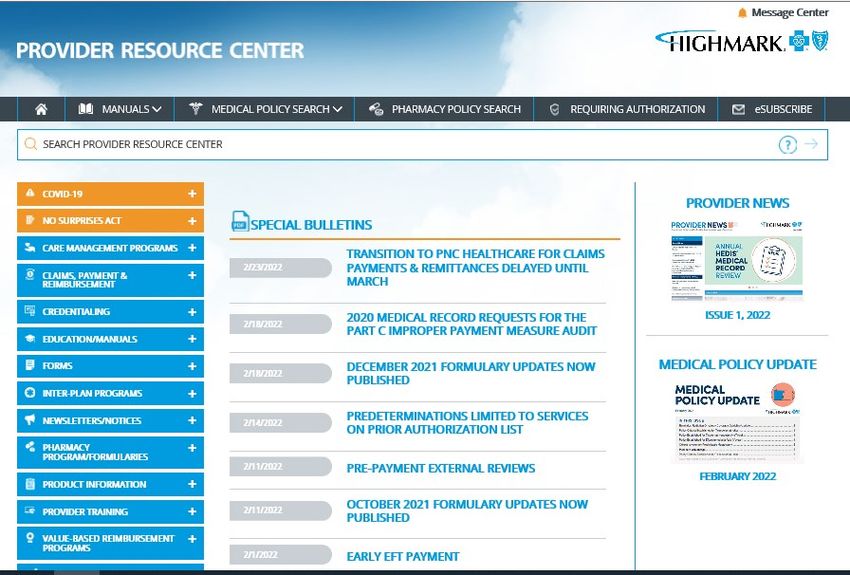
Property and Confidential | 2022Once on the Highmark Provider
Resource Center, select the
Value Based Reimbursement
Programs link
Property and Confidential | 20222022 Inter-Plan MA Care Management & Provider Engagement Program Attestation
Acknowledgement & Resources
Under Medicare Advantage
Stars, select the
Inter-Plan Medicare Advantage
Care Management and Provider
Engagement Program
Property and Confidential | 2022To attest into the program, select
Program Enrollment and
Acknowledgement
Property and Confidential | 2022Practices will access Care Gap reports through the NaviNet User Interface Portal.
• OOA members will appear on a separate tab within the Monthly Provider STARS gap report as "Inter-Plan MA Program
Members.”
• First 2022 Monthly Reports are scheduled for release 3/25/2022.
Property and Confidential | 2022Clinical Quality Measures
2022 Medicare Advantage Stars BCBS Highmark Hosted
MA Members Quality Measure Set
C01: Breast Cancer Screening C22: Statin Therapy for Patients with Cardiovascular Disease
C02: Colorectal Cancer Screening D13: Statin Use in Persons with Diabetes
C12: Osteoporosis Management in Women who had a Fracture D10: Medication Adherence for Diabetes Medications
C13: Eye Exam for Patients with Diabetes D11: Medication Adherence for Hypertension (RASA)
C14: Comprehensive Diabetes Care: Medical Attention for Nephropathy D12: Medication Adherence for Cholesterol (Statins)
C15: HBA1c Controlled for Patients with Diabetes (≤9%) D13: Medication Therapy Management
C16: Controlling High Blood Pressure
DMC19: TRC Medication Reconciliation Post-Discharge
**C14 Measure Retired on 4/26/2022General Guidelines
Continuous Enrollment
Hospice & Anchor Dates Palliative Care Race and Ethnicity Data
• Each measure has an enrollment • Exclusions for palliative care are • NEW for 2022 for Health Plan Reporting
• Members who use hospice benefits
period with gap defined by HEDIS specified in HEDIS measures where • NCQA requires reporting race and ethnicity
any time during the measurement
Part C or PQA Part D specifications. the services being captured may not as defined by the Office of Management
year, regardless of when the
This helps ensure adequate time to be of benefit for this population or and Budget (OMB) Standards for
services began, are excluded.
render services. may not be in line with patients’ goals Maintaining, Collecting, and Presenting
• Documentation that a member is
• Members must be enrolled and have of care. Federal Data on Race and Ethnicity. Race
near the end of life (e.g., comfort
benefits through anchor dates • Members receiving palliative care are and ethnicity is intended to be used to
care, DNR, DNI) or is in palliative
Identified within each measure captured and excluded via claims as further understanding of racial and ethnic
care does not meet criteria for the
specification. defined by the HEDIS Value sets disparities in care
Hospice exclusion.
(Palliative Care Assessment Value • The following measures instruct the
• Members may be identified using • Death and disenrollment will not
Set; Palliative Care Encounter Value organization to categorize race and
various methods, which may remove a member from a measure if
Set; Palliative Care Intervention ethnicity stratification:
include but are not limited to the continuous enrollment criteria is
Value Set) during the measurement Colorectal Cancer Screening.
enrollment data, claims/encounter met.
year Controlling High Blood Pressure.
data.
Hemoglobin A1c Control for
• Codes for Palliative Care
Patients With Diabetes
G9054; M1017; Z51.5
Stratification is not applied to scoring.STAR Measures with Advanced Illness and Frailty Exclusions
Source: HEDIS® 2022
Exclusion if claim submission on file
Frailty Advanced Illness reflects the diagnosis of one of the below
categories
• Per HEDIS guidelines Frailty exclusions • Per HEDIS guidelines Advanced Illness
are determined via administrative claim exclusions are determined via Measure Must have both
elements of Frailty AND
Can qualify under
Frailty alone in
data only. administrative claims data only These Description Advanced Illness in
population 66 yrs. of age
population 81 yrs. of
age or older
or older
can be submitted with telemedicine visit
Controlling High Blood Pressure
• For exclusion to be captured at least one claims. Yes Yes
claim that includes frailty (Frailty Value
Breast Cancer Screening
set) must be submitted during the • For exclusion, any of the following during Yes
measurement year. the measurement year or year prior to the Colorectal Cancer Screening
measurement year will be applied:
Yes
• For Osteoporosis, the diagnosis must be • At least two outpatient visits HbA1c Controlled for patients With
Diabetes Yes
captured during the intake period of (OBs, ED, or non acute inpatient
Eye Exam for patients with Diabetes
July1, 2021-June 30, 2022 through the on different date of service with Yes
end of the measurement year December an advanced illness diagnosis
Statin Therapy for Patients with
31, 2022. • At least one acute inpatient Cardiovascular Disease Yes
encounter with an advanced
Osteoporosis Management in
illness diagnosis Women Who Had a Fracture Yes Yes
• A dispensed dementia medicationC01: Breast Cancer Screening
Source: HEDIS® MY 2022 (BCS)
Percentage of female members 50–74 years of age who had a mammogram to screen for breast
cancer.
Numerator Denominator Exclusions
One or more mammograms during the Female members 52–74 years of age as of • Those who had a bilateral mastectomy any
measurement year or the 15 months the last date of the measurement year time during the member’s history through
prior to the measurement year. (female members who were 50 years of age the last day of the measurement year
or older as of OCT 2020). • Unilateral mastectomy with a bilateral
(OCT 1, 2020 – DEC 31, 2022) modifier (same procedure)
• Members receiving palliative care during
the measurement year
• Frailty and Advanced Illness exclusions
apply (supplemental data cannot be accepted)C01: Breast Cancer Screening
Source: HEDIS® MY 2022 (BCS)
Percentage of female members 50–74 years of age who had a mammogram to screen for breast cancer.
Best Practice
• Take the opportunity to cover personal review of member preventive screening needs through the Annual Wellness Visit/Initial
Preventive Physical Exam (Welcome to Medicare). Make most of this opportunity to communicate preventive care.
• Supply members with an order to enable flexibility in scheduling through walk in centers and breast cancer screening events.
• Issue member letters from your practice to non-compliant member to explain why regular breast cancer screening is
important.
.
Note: As we move into 2022, COVID will still play a crucial role in quality measures. Please make sure to schedule all
Mammograms as soon as possible in 2022 as appointments may once again be limited.
**Please distinguish between screening and diagnostic testing.C02: Colorectal Cancer Screening
Source: HEDIS® MY 2022 (COL)
Percentage of members 50–75 years of age who had appropriate screening for colorectal cancer.
Numerator Denominator Exclusions
One or more screenings for colorectal cancer. Percentage of members 51–75 years of • Those with a diagnosis of colorectal
Appropriate screenings are defined by any one of the age who had appropriate screening for cancer
five criteria below: colorectal cancer. • Those with evidence of a total
• FOBT – During the Measurement Year. Regardless colectomy
of FOBT type, guaiac (gFOBT) or immunochemical • Members receiving palliative care
(FIT), assume that the required number of samples during the measurement year
were returned. • Frailty and Advanced Illness
• Flexible Sigmoidoscopy – During the Measurement exclusions apply (supplemental data
cannot be accepted)
Year or the four years prior to the measurement year.
• Colonoscopy – During the Measurement Year or the
nine years prior to the measurement year.
• CT colonography during the measurement year or
the four years prior to the measurement year.
• FIT-DNA during the measurement year or the two
years prior to the measurement year.
*Please refer to the Primary Care Incentive Measure Guide for
testing compliance dates of serviceC02: Colorectal Cancer Screening
Source: HEDIS® MY 2022 (COL)
Percentage of members 50–75 years of age who had appropriate screening for colorectal cancer.
Best Practice
• The use of Fecal Occult Blood detection testing is accepted as a HEDIS numerator compliant form of non-invasive colorectal
screening. This testing is required to be completed annually.
• Initiate screening for members beginning at age 45 following guidelines from US Preventive Services Task ForceC12: Osteoporosis Management in Women who had a Fracture
Source: HEDIS® MY 2022 (OMW)
Percentage of female members 67–85 years of age who suffered a fracture and who had either a bone mineral
density (BMD) test or prescription for a drug to treat or prevent osteoporosis within 180 days of the fracture date.
Numerator Denominator Exclusions
Those female members age 67-85 Female members, 67–85 yrs. of age by the • Those who had a BMD test 24 months (730
who had suffered a fracture and who end of the measurement year who suffered a days) prior to the earliest date of service
had one of the below: fracture. Fractures of finger, toe, face and skull during the index period with diagnosis of
are not included in this measure. fracture (index episode start date)
• A BMD test, in any setting (including
• Those who had a claim encounter for
inpatient stays), within 180 days of the
Intake period is defined as a 12-month window osteoporosis therapy during the 365 days
fracture date.
that begins 6 months prior to the measurement prior to the episode date
• Osteoporosis therapy, or long-acting
year and ends after 6 months into the • Those who received a dispensed prescription
Osteoporosis therapy within 180 days of
measurement year. The intake period is used or had an active prescription to treat
the fracture date.
to capture the first fracture. osteoporosis during the 365 days prior to the
• A dispensed prescription to treat
Intake Period: JULY 1, 2021 – JUNE 30, 2022 index episode start date
osteoporosis filled the day of fracture or
• Those without pharmacy benefits through
180 days after the fracture date.
Medicare Advantage Part D.
• Members receiving palliative care during the
The drug classifications of Estrogen and
measurement year
Sex Hormone combinations are not
• Frailty and Advanced Illness exclusions apply
included in numerator compliance (supplemental data cannot be accepted)C12: Osteoporosis Management in Women who had a Fracture
Source: HEDIS® MY 2022 (OMW)
Best Practice
• Proper coding is essential in correctly identifying members who have recently suffered a fracture. Recent or new fractures are fractures that are
not yet healed and should be coded as such. However, if a fracture is healed, coding should indicate that the member has a history of fracture.
In this case, providers are encouraged to use the appropriate z-code from the list below* when coding for “History of Fracture”.
• Example ICD 10 Codes:
• Z87.310 Personal history of (healed) osteoporosis fracture
• Z87.311 Personal history of (healed) other pathological fracture
• Z87.312 Personal history of (healed) stress fracture
• Z87.81 Personal history of (healed) traumatic fracture
*List is not comprehensive and is intended to provide educational support only. Providers must follow CMS coding regulations and guidelines.
Fracture Prevention/Assess Contributing Factors:
• Screen members at risk for osteoporosis (bone mineral density test)
• Assess Risk of Falls
• Screen for Urinary Incontinence
• Review and evaluate Use of High Risk Medications
Osteoporosis Medications: Bisphosphonates are a class of drugs that prevent the loss of bone density, used to treat osteoporosis and
similar diseases. Bisphosphonates and other agents included as compliant as a drug to treat osteoporosis for HEDIS OMW: alendronate,
alendronate-cholecalciferol, ibandronate, risedronate, zoledronic acid (Reclast and Zometa), abaloparatide, denosumab (Prolia), raloxifene,
romosozumab, and teriparatide.
Note: Monotherapy with calcium supplements or Vitamin D supplements ( cholecalciferol or ergocalciferol) will not meet compliance for this measure.C12: Osteoporosis Management in Women who had a Fracture
Source: HEDIS® MY 2022 (OMW)
Percentage of female members 67–85 years of age who suffered a fracture and who had either a bone mineral density
(BMD) test or prescription for a drug to treat or prevent osteoporosis within 180 days of the fracture date.
Best Practice
• Patients with current fractures maybe under an orthopedic specialist care. Discuss with the orthopedic provider a timeline for
required X-ray testing (monitoring of healing) and request DEXA scan be completed during the same outing; or discuss the
opportunity of prescribing an osteoporosis medication after the four-month healing process.Diabetes Care Measures
Source: HEDIS® MY 2022
Measures will now be separated into separate categories:
• Eye Exam for Patients With Diabetes
• Medical Attention for Nephropathy
• Hemoglobin A1c Control for Patients with DiabetesC13: Eye Exam for Patients With Diabetes
Source: HEDIS® MY 2022 (EED) (prior CDC measure – Eye Exam (Retinal) Performed) No spec changes)
Identifies adult diabetic members who received an eye screening for diabetic retinal disease.
Numerator Denominator Exclusions
Screening or monitoring for diabetic retinal disease Diabetic members age 18–75 years by • Diagnosis of gestational or steroid-induced
identified through one of the following: the end of the measurement year and diabetes during the measurement year or
who were enrolled in the plan at the end the year prior to the measurement year
• Diabetics who received a retinal or dilated eye of the measurement year. • Diagnosis of polycystic ovarian syndrome
exam by an eye care professional (optometrist during the measurement year or the year
or ophthalmologist) in the measurement year prior to the measurement year
• A negative retinal or dilated eye exam Please refer to Diabetic member
(negative for retinopathy) by an eye care definitions on Slide 15 – also applicable To remove a member with any of the above
professional in the year prior to the to this measure. from the denominator, member must not
measurement year. have a face-to-face encounter in any setting,
• Bilateral eye enucleation any time during the with a diagnosis of diabetes, during the
member’s history through December 31st measurement year or year prior to the
measurement year.
Eye exam claims submitted by optometrist or
ophthalmologist with the corresponding E11.9 Dx • Members receiving palliative care during the
code are recorded as negative for retinopathy measurement year
• Frailty and Advanced Illness exclusions
apply (supplemental data cannot be accepted)
• Members with ESRDC13: Eye Exam for Patients With Diabetes
Source: HEDIS® MY 2022 ) (prior CDC measure - No spec changes)
Identifies adult diabetic members who received an eye screening for diabetic retinal disease
Best Practice
• Complete AWV and assessment of diabetic member preventive care/disease progression indicators for all Value Based
Reimbursement quality programs.
• Provide script or referral to ophthalmologist or optometrist to complete the exam. Use referral form with results to be
faxed/emailed back to the PCP. Reference Diabetic retinal eye preventive screening requirement on referral sheet.
• Reference measure specifications for appropriate CPT2 code application. For measure specific educational material on
CPT2 codes, please contact your Clinical Transformation Consultant or Provider Account Liaison
• Issue member letters from your practice to noncompliant member to explain why retinal eye screening is important on an
annual basis.C14: Comprehensive Diabetes Care – Medical Attention for Nephropathy
Source: HEDIS® 2021 (prior CDC measure - No spec changes) **C14: Medical Attention for Nephropathy Measure Retired on 4/26/2022
Identifies adult diabetic members who had medical attention for nephropathy.
Numerator Denominator Exclusions
Those with evidence of nephropathy or Diabetic members age 18–75 years by the • Diagnosis of gestational or steroid-induced
a nephropathy screening test during the end of the measurement year and who diabetes during the measurement year or
measurement year. were enrolled in the plan at the end of the the year prior to the measurement year
measurement year. • Diagnosis of Polycystic Ovarian Syndrome
• A claim encounter with a code to indicate during the measurement year or the year
evidence of treatment for nephropathy. Please refer to Diabetic member definitions prior to the measurement year
• A nephrologist visit during the measurement on Slide 15 – also applicable to this
year. measure. To remove a member with any of the above
• Evidence of ACE inhibitor or ARB therapy in from the denominator, member must not have a
the measurement year. face-to-face encounter in any setting, with a
• Lab claim for a urinalysis that included diagnosis of diabetes, during the measurement
microalbumin year or year prior to the measurement year.
• Members receiving palliative care during the
measurement year
• Frailty and Advanced Illness exclusions
apply (supplemental data cannot be accepted)
• Members with ESRD
Note: Documentation of ACEI/ARB medication regimen in current measurement year results as numerator compliance for this measure.C14: Comprehensive Diabetes Care – Medical Attention for Nephropathy
Source: HEDIS® 2021 ( prior CDC measure - No spec changes) **C14: Medical Attention for Nephropathy Measure Retired on 4/26/2022
Identifies adult diabetic members who had medical attention for nephropathy.
Best Practice
• Complete AWV and assessment of diabetic member preventive care/disease progression indicators for all Highmark quality
incentive programs.
• Hardwire EHR to trigger preventive schedules- this is an annual test requirement.
• Assure processes are in place to submit appropriate test billing.
• Report when appropriate the CPTII code 4010F - ACE inhibitor or ARB therapy prescribed or currently being taken.
• Review recent hospitalizations within the measurement year for urine screens while member was in the inpatient setting.
Services billed in an inpatient setting will be billed as a bundle and may not be recorded for gap closure.
• Issue member letters from your practice (with order enclosed) to noncompliant member to explain why regular micro albumin
screening is important.C15: Hemoglobin A1c Control for Patients With Diabetes ≤9%
Source: HEDIS® MY 2022 (HBD) (prior CDC measure – HbA1c Controlled - No spec changes)
Percentage of members 18–75 years of age with diabetes (type 1 and type 2) whose most recent Hemoglobin A1C is ≤9.0%.
Numerator Denominator Exclusions
Diabetic members who received at least one Diabetic members age 18–75 years by the • Diagnosis of gestational or steroid-induced
HbA1c screening during the measurement end of the measurement year and who diabetes during the measurement year or
year with the last HbA1c test result for the were enrolled in the plan at the end of the the year prior to the measurement year
measurement year < 9%. measurement year. • Diagnosis of Polycystic Ovarian Syndrome
during the measurement year or the year
Please refer to Diabetic member prior to the measurement year
Control is demonstrated by CPTII Codes:
definitions on Slide 15 – also applicable to
3044F HbA1c: < 7.0%
this measure. To remove a member with any of the above from the
3051F HbA1c: ≥ 7.0 and < 8.0% denominator, member must not have a face-to-face
3052F HbA1c: ≥ 8.0 and ≤ 9.0% encounter in any setting, with a diagnosis of diabetes,
during the measurement year or year prior to the
measurement year.
• Members receiving palliative care during
the measurement year
• Frailty and Advanced Illness exclusions
apply (supplemental data cannot be accepted)
• Members with ESRDC15: Hemoglobin A1c Control for Patients With Diabetes ≤9%
Source: HEDIS® MY 2022 (HBD) (prior CDC measure - No spec changes)
Percentage of members 18–75 years of age with diabetes (type 1 and type 2) whose most recent Hemoglobin A1C is ≤9.0%.
Best Practice
• This is an outcome control measure which requires disease management and the demonstration of controlled HbA1c lab
values. HEDIS (CMS) requires the last result of the year to be the determinant of compliance and control.
• Lab providers (outpatient labs and facilities) submit claims for payment, which influences the last test of the year. All “draw”
claims without a resulting lab value are seen as non-compliant.
• Submit zero dollar (performance reporting only) CPT2 claims on every result received
• Encourage partner facilities to include lab results with procedure claims submission.C16: Controlling High Blood Pressure Source: HEDIS® MY 2022 (CBP) Percentage of members 18-85 years of age who had a diagnosis of hypertension (HTN) and whose BP was adequately controlled during the measurement year (systolic
C16: Controlling High Blood Pressure Source: HEDIS® MY 2022 (CBP) Percentage of members 18-85 years of age who had a diagnosis of HTN and whose BP was adequately controlled (systolic
C23: TRC Medication Reconciliation Post-Discharge
Source: HEDIS® MY 2022 (TRC)
Percentage of discharges in the measurement year for members 18 years of age and older for
whom medications were reconciled on the date of discharge through 30 days after discharge.
Numerator Denominator Exclusions
Medication reconciliation conducted Acute or nonacute inpatient discharges on or • If the discharge is followed by a readmission
by a prescribing practitioner, clinical between January 1st and December 1st of or direct transfer to an acute or nonacute
pharmacist, physician assistant or the measurement year. inpatient care settings on the date of
discharge through 30 days after discharge,
registered nurse on the date of count only the last discharge.
discharge through 30 days after
discharge (31 total days) in which • If the member remains in an acute or
the discharge medications are Measure is based on discharges, not members. If nonacute facility through December 1st of the
reconciled with the most recent members have more than one discharge, include all measurement year.
medication list in the outpatient discharges.
medical record. Exclude both the initial and the
readmission/direct transfer discharges if the last
discharge occurs after DEC 1 of the
measurement year.
Note: Medication Reconciliation Post-Discharge measure is now a component of the Transitions of Care MeasureC23: TRC Medication Reconciliation Post-Discharge
Source: HEDIS® MY 2022 (TRC)
Percentage of discharges in the measurement year for members 18 years of age and older for whom medications were
reconciled the date of discharge through 30 days after discharge.
Best Practice
• Partner/coordinate with other providers in the care continuum that have held a patient visit within 30 days of discharge to
obtain medication reconciliation information for inclusion in the outpatient record.
• Coordinate with hospital partners for SNF discharges/transfers.
Note: If a member is admitted within 30 days of a discharge or transferred directly to a skilled nursing facility, the medication
reconciliation is required after the SNF discharge.
Note: A medication reconciliation performed without the member present meets criteria.C23: TRC Medication Reconciliation Post-Discharge
Source: HEDIS® MY 2022 (TRC)
Percentage of discharges in the measurement year for members 18 years of age and older for whom medications were reconciled the date of discharge through 30
days after discharge.
Medical Record Documentation Requirements
Any of the following will meet criteria:
• Documentation of the current medications with a notation that the provider reconciled the current and discharge
medications.
• Documentation of the current medications with a notation that references the discharge medications (e.g., no changes in
medications since discharge, same medications at discharge, discontinue all discharge medications).
• Documentation of the member’s current medications with a notation that the discharge medications were reviewed.
• Documentation of a current medication list, a discharge medication list and notation that both lists were reviewed on the
same date of service.
• Documentation of the current medications with evidence that the member was seen for post-discharge hospital follow-up
with evidence of medication reconciliation or review. Requires documentation that indicates the provider was aware of the
member’s hospitalization and discharge.
• Documentation in the discharge summary that the discharge medications were reconciled with the most recent medication
list in the outpatient medical record. There must be evidence that the discharge summary was filed in the outpatient chart
on the date of discharge through 30 days after discharge (31 total days).
• Notation that no medications were prescribed or ordered upon discharge.
Note: Only documentation in the outpatient chart meets the intent of the measure, but an outpatient visit is not required. Please
make sure documentation reflects that the Med Reconciliation is being completed after discharge.C22: Statin Therapy for Patients with Cardiovascular Disease
Source: HEDIS® MY 2022 (SPC)
Percentage of members who had at least one dispensing event for a high or moderate-intensity
statin medication in the measurement year.
Numerator Denominator Exclusions
Members who filled at least one Male members ages 21–75 and females age 40–75 • Those with a diagnosis of cirrhosis in the
ambulatory prescription for high or identified by event or diagnosis during the year prior to measurement year or year prior
moderate-intensity statin medication. the measurement year who were: • Those with a diagnosis of myalgia, myositis,
-Discharged from an inpatient setting with myocardial myopathy or rhabdomyolysis during the
infarction measurement year
• Those with a diagnosis of pregnancy during the
-Had a CABG, PCI or other revascularization
measurement year or year prior
procedure in any setting
• Those who have In vitro fertilization in the
OR measurement year or year prior
-By Diagnosis, as having Ischemic Vascular Disease • Those who filled at least one prescription for
during both the measurement period and the year clomiphene during the measurement year or
prior. Criteria need not be the same across both years year prior
but meet at least one of the following criteria: • Those without pharmacy benefits through
-at least one acute inpatient encounter with an IVD Highmark.
diagnosis without telehealth • Members receiving palliative care during the
-at least one outpatient visit, telephone, e-visit, or measurement year
virtual check in with an IVD diagnosis • Members with ESRD
-at least one acute inpatient discharge with an IVD • Frailty and Advanced Illness exclusions apply
diagnosis (supplemental data cannot be accepted)C22: Statin Therapy for Patients with Cardiovascular Disease
Source: HEDIS® 2021 (SPC)
Percentage of members who had at least one dispensing event for a high- or moderate-intensity statin medication in the measurement year.
Description Prescription (one Pharmacy claim required)
• Rosuvastatin 20-40 mg
High-Intensity Statin • Atorvastatin 40-80 mg • Simvastatin 80 mg
Therapy • Amlodipine-atorvastatin 40-80 mg • Ezetimibe-simvastatin 80 mg
• Atorvastatin 10-20 mg • Pravastatin 40-80 mg
Moderate-Intensity Statin • Amlodipine-atorvastatin 10-20 mg • Lovastatin 40 mg
Therapy • Rosuvastatin 5-10 mg • Fluvastatin XL 80 mg
• Simvastatin 20-40 mg • Fluvastatin 40 mg bid
• Ezetimibe-simvastatin 20-40 mg • Pitavastatin 2-4 mg
Note: NCQA will post a comprehensive list of medications and NDC codes to www.ncqa.org by NOV 1, 2021.C22: Statin Therapy for Patients with Cardiovascular Disease
Source: HEDIS® MY 2022 (SPC)
Percentage of members who had at least one dispensing event for a high- or moderate-intensity statin medication in the measurement year.
Description Prescription (one Pharmacy claim required)
High-Intensity Statin • Atorvastatin 40-80 mg • Rosuvastatin 20-40 mg
Therapy • Amlodipine-atorvastatin 40-80 mg • Simvastatin 80 mg
• Ezetimibe-simvastatin 80 mg
Moderate-Intensity Statin • Atorvastatin 10-20 mg • Pravastatin 40-80 mg
Therapy • Amlodipine-atorvastatin 10-20 mg • Lovastatin 40 mg
• Rosuvastatin 5-10 mg • Fluvastatin 40-80 mg
• Simvastatin 20-40 mg • Pitavastatin 1-4 mg
• Ezetimibe-simvastatin 20-40 mg
Note: NCQA will post a comprehensive list of medications and NDC codes to www.ncqa.org by NOV 1, 2022.C22: Statin Therapy for Patients with Cardiovascular Disease
Source: HEDIS® MY 2022 (SPC)
Percentage of members who had at least one dispensing event for a high- or moderate-intensity statin medication in the measurement year
Best Practice
• Educate diabetic members on the increased risk of cardiovascular disease, so that they may understand the benefits of
statin therapy in reducing their risk of stroke, heart attack and cardiovascular death
• Only select diagnoses can be submitted if statin therapy is contraindicated which would include myalgia, myositis,
myopathy, and rhabdomyolysis (most popular listed below). Claim must be submitted within the measurement year with
the appropriate diagnosis codes. Documentation in chart must be clear in stating symptoms. Phrasing of “intolerance",
"reaction”, and “cannot take” are not evidence enough for an exclusion.
• Review monthly gap reports and assure the member is on correct moderate or high dose medication to meet complianceD14: Statin Use in Persons with Diabetes
Source: PQA 2021 (SUPD)
Percentage of members who were dispensed a medication for diabetes that receive a statin medication.
Numerator Denominator Exclusions
Members who receive a prescription fill for a Members aged 40–75* as of the first day of the • Members with rhabdomyolysis or myopathy
statin or statin combination during the measurement year who were dispensed two or
measurement year. more prescription fills on different dates of • Members with a diagnosis of pregnancy,
service for a hypoglycemic agent during the lactation, or fertility (identified via a
measurement year. prescription claim for clomiphene)
• Members with a diagnosis of liver disease
*Members that turn 76 within the
measurement year require a Part D statin • Members with a diagnosis of pre-diabetes
fill prior to turning 76 for Health Plan The index prescription for the first hypoglycemic
• Members with a diagnosis of Polycystic
compliance. medication must occur at least 90 days prior to
Ovarian Syndrome (PCOS)
the end of the measurement year for
denominator inclusion. • ESRDD14: Statin Use in Persons with Diabetes
Source: PQA 2021 (SUPD)
Percentage of members who were dispensed a medication for diabetes that receive a statin medication.
PQA Table: Statin Medications
Statin Medications
• lovastatin • fluvastatin • pravastatin
• simvastatin
• rosuvastatin • atorvastatin • pitavastatin
Statin Combination Products
• niacin & lovastatin
• niacin & simvastatin • ezetimibe & simvastatin
• atorvastatin & amlodipineD14: Statin Use in Persons with Diabetes
Source: PQA 2021 (SUPD)
Percentage of members who were dispensed a medication for diabetes that receive a statin medication.
Best Practice
• Educate diabetic members on the increased risk of cardiovascular disease, so that they may understand the benefits of
statin therapy in reducing their risk of stroke, heart attack and cardiovascular death
• Only select diagnoses can be submitted if statin therapy is contraindicated which would include myopathy and
rhabdomyolysis. Claim must be submitted within the measurement year with the appropriate diagnosis codes.
Phrasing of “intolerance", "reaction”, and “cannot take” are not evidence enough for an exclusion.
• Review members chart for other exclusions that can be submitted to exclude member from the measure.
• Consider statins with fewer drug interactions such as rosuvastatin, pravastatin, and fluvastatin to reduce risk of adverse
events
• Members who do not tolerate one statin may be able to tolerate a different statinD10: Medication Adherence for Diabetes Medications
Source: PQA 2021
Percentage of members with a prescription for a diabetes medication who fill their prescriptions often enough to cover 80% or
more of the time they are supposed to be taking the medication. The classes of diabetes medication includes: biguanides,
sulfonylureas, thiazolidinediones, DDP_IV inhibitors, Incretin Mimetic Agents, Meglitinides , and SGLT2 Inhibitors.
Numerator Denominator Exclusions
Those members with a prescription for Members 18 years of age or older as of the first • Those without pharmacy benefits through
diabetes medication who fill their day of the measurement year with at least two Medicare Advantage Part D.
prescriptions often enough to cover fills on different dates of medication(s) across • Members who take insulin
any of the drug classes during the measurement
80% or more of the time they are period. • ERSD
supposed to be taking their
medications. * Members are only included in the measure
calculation if the first fill of their medication
occurs at least 91 days before the end of the
*Derived from the prescription daily dosage. measurement period.
Note: Medication Adherence for Diabetes medications have been updated, and NDC codes are progressive.D11: Medication Adherence for Hypertension: Renin Angiotensin System
Antagonists (RASA)
Source: PQA 2021
Percentage of members with a prescription for a blood pressure medication who fill their prescriptions often enough to cover
80% or more of the time they are supposed to be taking the medication. Blood pressure medication includes: ACE (angiotensin
converting enzyme) inhibitor, ARB (angiotensin receptor blocker), a direct renin inhibitor or combinations thereof.
Numerator Denominator Exclusions
Those members with a prescription Members18 years of age or older as of the first day
for recommended hypertension of the measurement year with at least two fills on • Those without pharmacy benefits through
medication who fill their different dates of medication(s) across either the Medicare Advantage Part D.
same medication or medications (s) in the drug • Members who take sacubitril/valsartan.
prescriptions often enough to cover classes during the measurement period.
80% or more of the time they are • ESRD
supposed to be taking their Members are only included in the measure
medications. * calculation if the first fill of their medication occurs
at least 91 days before the end of the measurement
period.
*Derived from the prescription daily
dosage.
Note: Medication Adherence for Hypertension medications have been updated, and NDC codes are progressive.D12: Medication Adherence for Cholesterol: Statins
Source: PQA 2021
Percent of plan members with a prescription for a cholesterol medication (a HMG CoA Reductase Inhibitor-statin
drug or statin combination) who fill their prescriptions often enough to cover 80% or more of the time they are
supposed to be taking the medication.
Numerator Denominator Exclusions
Those members with a prescription for Members18 years of age or older as of the first day
a cholesterol medication (a statin drug of the measurement year with at least two fills on • Those without pharmacy benefits
or statin combination) who fill their different dates of either the same medication or through Medicare Advantage Part D.
medication(s) in the drug classes during the
prescriptions often enough to cover measurement period.
80% or more of the time they are • ESRD
supposed to be taking their Members are only included in the measure
medications.* calculation if the first fill of their medication occurs at
least 91 days before the end of the measurement
period.
*Derived from the prescription daily dosage.
Note: Medication Adherence for Cholesterol medications have been updated, and NDC codes are progressive.D10, D11, D12: Medication Adherence Measures
Source: PQA 2021
Percentage of members who were dispensed a medication who fill their prescriptions often enough to cover 80% or more of the time they are supposed to be taking the medication.
Best Practice
• Identify all members who are prescribed medication for these categories
• Prep chart to ensure that provider discusses importance of ongoing compliance
• Discuss with the member the benefits of adhering to medication - Nurse/Physician/Medical assistant/Physician extender
• Provide ongoing patient outreach to those showing as non-compliant
• Identify reason for noncompliance and attempt to solve
• Educate members about their condition and explain why the medication is being prescribed
• Use motivational interviewing to help members commit to taking their medication and set goals for taking their medications
• Ask members what routine they use to help them remember to take their medications (apps, alarms, pillboxes)
• Discourage “pill splitting” or taking medications every other day. If dosage changes, rewrite prescription to accurately show prescribed dose.
• Consider 90 day fills when writing prescriptions.
• Encourage members to utilize their insurance card, as this may help to identify other services that may be beneficial to them. Samples, paying in cash and
using discount cards will not generate an insurance claim.. These members will appear as non-compliant with the measure.
• Be proactive. Evaluate practice processes for opportunities to close gaps every time the member is seen rather than reacting to gap closure reportsD13: Medication Therapy Management (MTM)
Source: CMS 2022 & Highmark developed measure.
Percentage of MTM eligible members who received a Comprehensive Medication Review (CMR) during the
measurement year.
Numerator Denominator Exclusions
Eligible members who complete a CMR by Members who meet eligibility requirements:
an approved CMS vendor during the • Those that opt out within 60 days of program
Those with three or more chronic conditions, who take a eligibility
measurement year.*
minimum of seven Part D medications, and are likely to incur
annual costs of at least $4,696 for all covered Part D drugs.
Note: Members in long-term care facilities are not excluded from the denominator.D13: Medication Therapy Management (MTM) Source: CMS 2022 Percentage of MTM eligible members who received a Comprehensive Medication Review (CMR) during the measurement year. Best Practice • Review Monthly Star Care Gap MTM detail reports for members that have become eligible. • Discuss the benefits of completing the CMR with the members during AWV and other office visits
D13: Medication Therapy Management (MTM)
Source: CMS 2021
What is the MTM Program and how will it be conducted?
Program Specifics
• Medicare Part D covered benefit
• Designed to aid members with certain disease states who take many medications and have high prescription costs.
• Providers members access to a health care professional who can help support their health and safety and complement the
care they receive by having a pharmacist work with them and their doctor.
• This program is free, and members are automatically enrolled if eligible.
• They will receive information on how to access the program and will be contacted to schedule/complete a CMR.
CMR/TMR
• During this one-on-one telephone consultation with a pharmacist or nurse, the member’s entire medication profile is reviewed
(CMR –Comprehensive Medication Review), including prescriptions, over-the-counter (OTC) medications, herbal
supplements, and samples. The pharmacist or nurse will check for appropriateness of therapy and potential interactions.
They will also discuss therapy goals, medication-related problems and any specific questions the member may have.
Targeted Medication Reviews (TMR) are also conducted focusing on identifying cost savings, safety concerns, prescribing
adherence to national treatment guidelines and whether members have been following their medication regimens.
• CMR Follow-up Letter - This letter includes a Personal Medication List and Medication Action Plan detailing the member’s
conversation with the pharmacist or nurse.
• Member / Doctor Outreach - If an issue is found during a medication review (CMR or TMR), the team may contact the
member and/or doctor via phone, fax, or mail to discuss recommendations for adding or changing drug therapy, potential
drug interactions or safety issues.HIGHMARK RISK
ADJUSTMENT
PROGRAMS
Property and Confidential | 2022Highmark Risk Adjustment Programs
Unconfirmed Diagnosis Enhanced Annual Risk Score Accuracy Retrospective Chart Retrieval
Code (UDC) Program Wellness Visit (eAWV) (RSA Program): Program:
Program
The UDC program is a Using the Vatica Wellness Several tools are available that This program supports a Centers
clinically based program that 365+ software, providers can work within or in conjunction for Medicare and Medicaid Services
promotes Provider/Highmark perform enhanced Annual with provider EMR systems to (CMS) requirement to ensure the
collaboration to evaluate Wellness Visits for their present unconfirmed diagnosis accuracy and integrity of risk
previously reported and/or Highmark Medicare Advantage conditions at the point of care in adjustment data submitted to CMS.
suspected diagnosis members. The tool assists order for the clinician to
conditions. providers in appropriately evaluate, disposition, treat and
documenting an AWV along document when appropriate.
with evaluating unconfirmed
diagnosis conditions.
Property and Confidential | 2022Highmark Risk Adjustment Programs
Our 2022 Risk Adjustment Programs help guide practices through program requirements
After Logging into NaviNet, Click Select Education / Material from Select Risk Adjustment from
on Resource Center under the dropdown menu the dropdown menu
Workflows for this Plan
Property and Confidential | 2022HIGHMARK CODING
EDUCATION
AND SUPPORT
Property and Confidential | 2022Available Resources
HCC University is a provider coding resource on NaviNet. It contains guides to assist with
documentation and coding according to CMS documentation standards and ICD-10-CM
coding requirements
1. Log into NaviNet
2. Navigate to the Provider
Resource Center 3
3. Select “Education
/Manuals” from the menu
bar to expand the 4
selection
4. Select “Coding
Education/HCC University” to
open the page with
corresponding resources
Property and Confidential | 2022Provider Education Resources
1. Documentation and Coding Reference Cards
• Top HCC conditions seen in both Primary Care and Specialist Practice settings
2. Training Presentations
• Risk Adjustment in Clinical Practice
• Risk Adjustment Overview
• Quarterly Coding & Quality Knowledge College
3. Helpful Links (CMS and other coding resources)
• AAPC
• AHIMA
• 2019 ICD-10-CM
• MLN Web-based training
• CMS Guide for AWV
Property and Confidential | 2022IMPORTANCE OF ANNUAL WELLNESS VISITS Property and Confidential | 2022
C51: Annual Wellness/Initial Preventive Physical Exam Rate The Importance of AWVs/IPPEs The Annual Wellness Visit allows the provider/practice to provide a comprehensive wellness visit and communicate needed preventive care for their patients without visit co-pays or cost sharing. Key Elements of the Annual Wellness visit include acquire beneficiary information (Health risk assessment, medical/family history, risk factors, functional ability and level of safety) assessment, and counseling. Coverage for AWVs Annual wellness visits are covered in full by ALL BCBS Plans. CMS provides guidance on provider documentation requirements, and appropriate coding/billing. Reference sites have been attached below. https://www.cms.gov/Outreach-and-Education/Medicare-Learning-NetworkMLN/MLNProducts/downloads/awv_chart_icn905706.pdf Property and Confidential | 2022
Health Outcomes Survey (HOS)
&
Customer Assessment of
Healthcare Providers and
Systems (CAHPS)
Property and Confidential | 2022Health Outcomes Survey (HOS)
The HOS survey scores health plans on 5 measures - these 5 measures combine for 14% of the overall
Star rating.
• Administered annually by CMS to a random sample of our MA members
• A baseline survey is administered to a new cohort each year (approximately 1200 members per
plan) and two years later, these same respondents are surveyed again (approximately 500
members per plan)
HOS Measures
The five HOS measures include two functional health measures and three HEDIS effectiveness of Care
measures:
• Improving or maintaining physical health (PCS)
• Improving or maintaining mental health (MCS)
• Monitoring physical activity
• Reducing the risk of falling
• Improving bladder control
Property and Confidential | 2022You can also read