2021 Scottish Parliament Manifesto - Dying, death and bereavement: Getting it right for all of Scotland - Marie Curie
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

2021 Scottish Parliament Manifesto Dying, death and bereavement: Getting it right for all of Scotland

2021 Scottish Parliament Manifesto 2

2021 Scottish Parliament Manifesto
Contents
Introduction 4
What is palliative care? 6
Health inequities and inequalities in palliative care 9
Community support networks 10
Place of care and death 13
Social care 15
Supporting digital 17
Family (informal) carer support 19
Grief and bereavement 20
Education and training 21
Welfare and benefits 22
References 26
3
2021 Scottish Parliament Manifesto
Introduction
I
n Scotland in 2019/20, more than 58,100 The coronavirus pandemic has shown
people died¹. Around 90% of those the distressing impact dying, death and
(52,000) had a palliative care need in the bereavement can have on anyone at any
final years, months, weeks, days and hours time. It has intensified the complexities
of their life. Scotland’s ageing population associated with terminal illness for patients,
means more and more people will be dying families and carers, which will affect many
in the years to come, with Marie Curie people for years to come. The need to
research suggesting up to 10,000 more identify people with a terminal illness who
people dying every year with palliative care would benefit from palliative support as
needs by 20402. More and more of those early as possible has never been greater.
people will be dying in the community, with This will ensure the best possible quality
nearly two-thirds of all deaths taking place of life.
in care homes or people’s own homes3. Everyone will be affected by dying, death
Many of those living with a terminal illness and bereavement at some stage of their
will be supported by families, loved ones lives. Those who are dying have the right
and neighbours, who provide them with to an end of life experience which reflects
informal family care. There is a growing what’s most important to them.
need to support these carers throughout Marie Curie is here for people living with
their caring role and beyond, especially any terminal illness, their families and
when the person being cared for has carers. We offer expert care, guidance and
died. Every year, it can be estimated that support to help them make the most of the
around 40,000-50,000 carers in Scotland time they have left.
are bereaved4.
In Scotland in 2019/20 Our fundraising, care and
support services:
2 hospices
2 research leads posts
We cared for 8,534
15 active research projects
people with a terminal
31 local authorities supported
illness
by our nursing service
32 stores
100 fundraising groups
We need to raise £250,000 175 people supported by our
a week to support our volunteer Helper services
services in Scotland 1,571 volunteers
1/3 of care and support is
provided by gifts in Wills.
4
2021 Scottish Parliament Manifesto
Our vision 2021-2025
We believe the next Scottish Government must work towards a Scotland where
dying, death and bereavement is talked about openly, where people can plan and
discuss their care and preferences, and everyone affected has the best possible end
of life experience which reflects what is most important to them.
Asks for the next Scottish b. Establishes a new national Palliative
Government and End of Life Care Network linking
key stakeholders with NHS Boards and
Marie Curie is calling for the next Integration Authorities to identify
Scottish Government to support dying, gaps in care, share good practice and
death and bereavement in Scotland support innovation and learning.
through three key asks:
c. Works with all providers including
1. Appoint a new National Clinical the NHS, social care, the independent
Lead for Palliative and End of Life Care and third sectors to ensure everyone
for Scotland, who will be responsible gets the care they need and is working
for overseeing a new national strategy to end inequities and inequality.
that delivers place-based palliative
d. Empowers and equips communities
care in partnership with national
to care for and support those facing
and local stakeholders across public,
dying, death and bereavement to
private and third sectors.
experience as high a quality of life
2. Introduce a national strategy as possible.
for palliative and end of life care
3. Ensure all family and other carers
taking a whole-system, public health
get the support they need as they
approach that:
look after the person they are caring
a. Sets out vision for care in all for, and appropriate bereavement
settings including hospitals, hospices, and financial support when that
care homes and people’s own homes. person dies.
Dying, death and bereavement impacts
everyone and every part of our life. All
public policy including health and social
care, welfare, housing, education and
technology will interact with people living
with a terminal illness or when someone
is grieving.
A whole-system approach to terminal
illness should be adopted both nationally
Kieran Dodds/Marie Curie
and locally from Scottish Parliament and
Government to NHS Boards, and Health
and Social Care Partnerships, Local
Government and Community Councils.
5
2021 Scottish Parliament Manifesto
What is palliative care?
W Dying in Scotland today
e believe someone is terminally
ill if they are diagnosed with a
condition that will lead to their In 2018, more than 16,500 people died
death. Depending on the condition this of cancer, more than 14,700 died of
could be years, months, weeks or days. circulatory disease, more than 7,000 died
of respiratory disease and more than 4,000
Those who are terminally ill can be died of dementia or Alzheimer’s6.
supported with a palliative care approach.
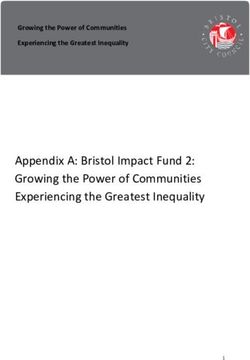
The aim of palliative care is to support a Figures below show where people died:
person to have a good quality of life – this
includes being as well and active as possible 6% of people
6%
in the time they have left. It can involve: died in hospice
25%
• managing physical symptoms such 28% 25% of people
died at home
as pain
48% of people
• emotional, spiritual and psychological
died in hospital
support
21 % of people
• social care, including help with things like 48% died in a care
washing, dressing or eating home
• support for family and friends.
A person can receive palliative care at any There are still misconceptions about
stage of their illness. It can be delivered palliative care, with it often being
alongside treatments, therapies and associated with people dying of cancer,
medicines aimed at controlling the illness, but it supports a person with any terminal
such as chemotherapy or radiotherapy. condition including dementia, frailty, heart
Palliative care can be provided in different disease. Many people will die with multiple
places, including in a person’s home, in health conditionsii.
hospital, in a care home or nursing home, Currently, not everyone gets the support
and in a hospice. It can be delivered they need – one third of Scots with terminal
by general health and social care conditions die without an anticipatory
professionals, such as GPs, District Nurses care plan in place, meaning they could be
and social care teams, as part of the day- dying without some or any of the support
to-day care they provide. A person may also they need7. Research carried out by the
receive support from specialist palliative London School of Economics in 2015 also
care professionals who might be involved in suggested a significant number of people
managing more complex care needs. They who need specialist palliative care were not
will often work in partnership with other accessing it .
professionals to provide co-ordinated and
We know that many groups of people face
personalised care5.
difficulties accessing the care they need.
The disease a person is dying from can
increase or decrease the chance a person
has of accessing palliative care services.
Those with cancer are far more likely to get
the care they need compared to those with
other conditions, particularly those with
organ failure8.
62021 Scottish Parliament Manifesto
The inverse care law applies in palliative Data from the National Records for
care as it does in almost every other Scotland has already started to show a shift
aspect of life9. Minority, deprived and rural in care to the community is increasing,
communities are all far less likely to get the with more and more people dying at
help they need as they approach the end home or at their care home. There has also
of their lives10. We also know the majority been a steady increase in recent years in
of these groups are less likely to ask for the amount of time people spend in the
help, and existing research has shown that community in their last six months of life15.
this acts as a significant barrier for early During the recent COVID-19 pandemic
identification and engagement with those there has also been a significant and
who would benefit from palliative and end substantial increase in the number of
of life care11. people dying at home. There were 4,000
The impact of people not getting the care more deaths at home in 2020 than in
they need when they die is devastating previous years, with 1,500 more people
for them and can also have a significant dying at home with cancer, nearly 1,000
effect in the wider health and social more heart disease and circulatory-related
care system. There is a growing body of deaths, and increases in dementia and
evidence that shows that investing in respiratory-related deaths at home. This
palliative care services in the community has largely been driven by the need to
can increase efficiencies and reduce free up hospital beds for patients with
costs in the wider health and social care coronavirus. If this trend continues, then it
system, perhaps leading to significant is important to make sure these people are
savings12. More research is needed to better properly supported with all the care and
understand this. support they and their carers need as they
approach the end of life.
Dying in Scotland in 2040 The next Scottish Government will see
Marie Curie research suggests that between these changes accelerate toward the
2017 and 2040, Scotland will see a 14% 2040 projections.
increase in deaths, rising from 57,870 to We need to see action now, to ensure that
a predicted 65,756 in 2040. Research we can meet this challenge and ensure that
suggests that up to 95% of those people who are dying and approaching the
deaths are likely to require a palliative end of their lives have the best possible
care approach – this means nearly experience, and for that experience to
10,000 more people dying who will reflect what is most important to them.
need a palliative approach in Scotland
It is the duty of the next Scottish
every year13.
Government to meet this challenge and
Trends in place of death show that by 2040, ensure that we get it right for every person
up to two-thirds of people in Scotland at end of life.
are likely to die in a community setting,
including their own homes, care homes and
hospices, with hospital deaths accounting
for 34% (down from 50% in 2017)14. The
same research also suggests that without
investment in social care services this will
not be possible.
72021 Scottish Parliament Manifesto
Being identified for and The Scottish Government committed
accessing palliative care to everyone who needs palliative care
having access to it by 2021, including a
One of the biggest challenges facing commitment to ensuring that everyone
people who are diagnosed with a terminal who needs an Anticipatory Care Plan will
illness is being able to access the care and have one. Evidence currently suggests that
support they need. A lot of people who Scotland is short of meeting this ambition
miss out on some or all of the care they and more must be done to ensure that
need is because they are not identified people who would benefit from an ACP
for a palliative approach and never have a have the opportunity to get one.
chance to discuss with health and social
• Every person diagnosed with a terminal
care practitioners or their family the kind
illness should be given the opportunity
of support they need, their wishes and how
to have and discuss an Anticipatory
they would like to spend the time they
Care Plan, which can be read, updated
have left.
and easily shared electronically
We believe a palliative approach should be by anyone responsible for that
introduced as early as possible following person’s care.
a terminal diagnosis or very serious illness • The urgent roll-out of the National
where the possibility of it progressing to Digital Platform to facilitate accessible,
a terminal condition is high. A palliative easy exchange of ACPs between all
approach can be introduced while a person care providers, with appropriate digital
is still receiving curative treatment and can training for health and social care
often complement that care, so it does not workforces. Patients and carers, where
need to be a choice between approaches. appropriate, should also be able to
An Anticipatory Care Plan (ACP) can allow access ACPs.
patients and healthcare teams to discuss
treatments and care options, as well as
preferences such as place of care and where “Until I had personally had
a person would prefer to die. It also allows a to be involved in meetings to
social and spiritual preferences and wishes
to be captured and acted on, as well as help discuss care for my gran, I had
identify any carers. no idea that there were so many
Having an ACP in place can reduce the requirements, so many forms
69% amount of time a person spends in
or that the waiting times for
Currently, only hospital, including reducing the number of
69% of people unnecessary hospital admissions, reduce assessments could be so long. I
with a terminal
illness have an
the likelihood of having to go to A&E, and think that if people had a better
electronic care make it more likely that a person will die in
plan in place in their preferred place of choice. understanding of what might
Scotland
Currently, only 69% of people with a happen then they would take
terminal illness have an electronic care steps to prepare and make sure
plan in place in Scotland16; with those with
their loved ones won’t be faced
terminal cancer more likely to have one
than those with other conditions. This rate with worry over what is the right
has been improving, but we need to see thing to do.”
everyone with a terminal illness be given
the opportunity to develop an ACP. Marie Curie staff member
82021 Scottish Parliament Manifesto
Health inequities and inequalities in
palliative care
More must also be done to tackle Ethnically diverse groups
inequalities and inequities in access to • Marie Curie research has shown that
palliative and end of life care. There are many from ethnically diverse groups
many groups and populations that struggle including Black, Asian and other minority
to access vital health and social care groups are not accessing palliative care
services, including palliative care. These and, when they do, palliative care delivery
include rural communities, ethnic and is not always sensitive to their different
socially deprived groups, gypsy and traveller needs, particularly around culture and
communities, LGBTQ+, women, older religion18.
people and people with learning disabilities.
LGBTQ+
A lack of knowledge about palliative and
end of life care options, and a reluctance to • One in six LGBTQ+ people are
engage with palliative and end of life care discriminated against using public
services are long-standing issues which services including palliative care, and
significantly impact palliative and end of life half of LGBTQ+ people expect to be
experiences for these groups. discriminated against. This can mean
LGBTQ+ people delay accessing the
Local statutory services for minority groups health and social care services they need,
are often under-resourced and work in making the process seem overwhelming,
silos, meaning a large proportion of people particularly at the end of life when they
in these groups fall between the cracks are most vulnerable19.
and are let down by unnecessarily complex
systems. Existing research has shown that Older people
fear of discrimination, a lack of knowledge • Older people are much less likely to get
about palliative and end of life care, and the palliative care they need at end of
not knowing where to find support can also life compared to younger age groups,
cause poor engagement with specialist primarily because their condition and
care providers. prognosis can be seen as a normal part
Gender inequalities of dying. They often have unmet pain
needs as a result of this and struggle to
• International research exploring gender access palliative care specialists who can
and palliative care has shown that co-ordinate services for them, such as
women face significantly more barriers Clinical Nurse Specialists20.
in accessing the palliative and end of
life support they need, primarily as a • We are calling for the Scottish
result of different social circumstances Government’s Ministerial Task Force on
and existing gender stereotypes around Health Inequalities to include a specific
care giving, among others17. There is focus on palliative and end of life care
significant evidence gap for this group in to ensure everyone has equal access to
Scotland, which must be explored. the palliative support they need.
92021 Scottish Parliament Manifesto
Talking about dying, death We believe that initiatives like this need
and bereavement greater support and investment and that
the Scottish Government should take more
Dying and death remains a taboo subject of a role in leading this national debate.
in the general population. Palliative care
• The Scottish Government should lead
still carries with it an association with crisis
a national public health discussion
intervention and/or imminent death, which
around dying, death and bereavement.
means the benefits of early engagement
are often not fully understood or taken • The Scottish Government must better
advantage of, or missed altogether. support existing resources and invest
in new ones to help everyone affected
Many organisations and movements, such by terminal illness feel equipped to
as the Good Life, Good Death, Good Grief manage issues relating to dying, death
alliance, have tried to encourage a more and bereavement in addition to well-
open society willing to talk about these signposted and accessible physical,
subjects, but more needs to be done. emotional and spiritual support.
Marie Curie supports Good Life, Good
Death, Good Grief’s End of life Aid Skills
for Everyone (EASE) resource, which has
been designed to enable people to be more
comfortable and confident in issues they
face around dying, death and bereavement.
Community support networks
Local community networks, including identified and will be supported in the
faith groups, can provide a vital source coming years.
of support for terminally ill people, their There is undoubtedly potential to harness
families and carers. the resource, compassion and dedication
Compassionate Community initiatives, of communities more deliberately and
such as Compassionate Inverclyde, which efficiently than is currently the case.
was established by Ardgowan Hospice in The pandemic has shown how quickly
2016, help provide information, support community initiatives can be mobilised and
and day-to-day respite for informal carers the difference this can make for the most
to cope with the pressures and implications vulnerable.
of caring for a terminally ill person at home, • We are calling for the establishment
as well as a release for patients themselves. of a Compassionate Communities
This is especially important, given a Network across all Integration
projected two-thirds of people will die in Authorities, with identified resource
community-based settings by 2040. to support capacity building in
The Truacanta Project which is run by communities.
the Scottish Partnership for Palliative • Empower and train volunteers to help
Care (SPPC) was set up to support local bridge statutory and non-statutory
communities across Scotland interested support and act as an early-warning
in taking community action to improve system to health and social care teams
people’s experiences of dying, death, loss as needs of those affected by terminal
and care. A number of projects have been illness change.
102021 Scottish Parliament Manifesto
Integration of health and uncertainties around long-term planning
social care and sustainability as a result of short-term
contracts, as well as reduced financial
The health and social care system is still support from statutory partners, but greater
less integrated than was intended when expectation on delivery.
the Public Bodies Act was passed. The third
There is a recognition and understanding
sector plays a key role in integrated services
that the third sector and statutory sources
but is not seen as an equal partner and is
will both have fewer financial resources in
often not included in early conversations
the future, highlighting a need for greater
with Integration Authorities regarding the
collaborative working and innovation with
strategic planning and commissioning of
all key stakeholders to ensure successful
palliative care services.
outcomes for communities. This will be
Marie Curie is the largest third sector even more crucial following the impact
provider of palliative care services for of coronavirus. However, this can only be
adults in Scotland, as well as being the achieved if there are sustainable funding
leading charitable funder of palliative and models for the third sector, especially
end of life care research. The third sector those commissioned by statutory bodies to
has the expertise, knowledge and skills deliver services.
that should be engaged with far sooner in
• We are calling for a commitment to
commissioning and planning processes of
innovation and sustainable funding
integration authorities.
by the Scottish Government with
• The third sector must be included as minimum three-year contracts
voting members of all Integration between the third sector and
Authorities in Scotland. statutory partners.
Many third sector organisations are • Commissioners to take a strategic,
commissioned and expected to deliver whole-system approach to developing
vital health and social care services services focused on outcomes and
to local communities, yet many third needs of terminally ill people in
sector organisations struggle to secure communities.
financial continuity. This can include
Layton Thompson/Marie Curie
112021 Scottish Parliament Manifesto
Place of care and death
Data from National Records Scotland Hospitals
(NRS), has shown a significant shift in place A third of patients in Scottish hospitals
of death from hospitals to communities are in their last year of life and 10% die on
during the pandemic for the vast majority their current admission22. We know that
of non-coronavirus patients over the last many of these people miss out on the care
eight months21. There has been an increase and support they need when they become
in cancer deaths at home, with 1,500 more terminally ill, are approaching the end of
deaths than average during this period. life, and when they die. In 2017/18, 26,917
Dementia deaths have seen an increase people in Scotland died in a hospital (47%
in both care home and home settings, of all people).
and there have been nearly 800 extra
respiratory deaths at home. There has been While there are examples of good practice
a significant reduction in hospital deaths for of palliative and end of life care being
people dying of non-coronavirus conditions identified and delivered through acute
at the same time. In normal times, dying at settings, many hospitals are still not
home is where the majority of patients tell identifying enough patients who could
us they want to be, therefore we believe this benefit from palliative care. Challenges
shift could be a positive development. for this include; IT barriers, failing to meet
specialist palliative and end of life care
There have been innovations and service staffing levels, training and education and a
responses to meet this shift. However, there ‘treat and cure’ ethos23.
are serious concerns that many terminally
ill people and their carers will not have As a result, these patients miss out on
received the care they needed at home the end of life support they need and
during the pandemic. This will include are entitled to24 and this is likely to have
accessing health and social care services, as worsened during the coronavirus pandemic
well as community support. In some cases, from hospitals being under intense
this may have meant patients dying without pressure. The impact on patients who
proper pain or symptom management, with have missed out on this palliative and end
family carers overwhelmed by the demands of life support in hospitals will have been
of caring, and struggling with grief and distressing, but equally for their families
bereavement following the death of the who have had to grieve for their loss in
cared-for person. much more isolating circumstances due to
the pandemic.
• Research and evidence should
be carried out to understand the • Scottish policy and any new palliative
experience of terminally ill people and care strategy must actively support
their carers during the pandemic, to palliative care in acute settings.
ensure that good practice is identified, • A full range of recommendations for
lessons are learned, and additional supporting palliative care in acute
support and resources are put in place settings can be found in Marie Curie
to ensure that people get the care they and the University of Glasgow’s report,
need to maintain this shift of care into Past, present and future caring for those
the community. approaching the end of life in Scottish
Hospitals, which was published in 2020.
122021 Scottish Parliament Manifesto
Unscheduled care • We are calling for more investment
The complexity of terminal conditions and development of primary care
means unscheduled and out-of-hours unscheduled services and NHS 24 to
care (telephone advice, primary care, maximise their potential to provide
ambulances, emergency departments cost-effective unscheduled care for
and hospital admissions) is heavily relied people approaching end of life.
on to support those affected by terminal • Enhanced data recording and analysis
illness, particularly in the final year of life, systems at GP practice, board and
as conditions worsen and become more national level to improve reliable
unpredictable, with those affected often at identification of people with palliative
breaking point. care needs and coordination of
their care.
University of Edinburgh research, funded
by Marie Curie and The Chief Scientist’s
Office for Scotland, has shown that more
than 90% of people in Scotland used
unscheduled care five times on average
in the last year of life and 34% of all
unscheduled care interaction happened
in the final month of life25.
Much of this support has been used by
terminally people with multiple health
conditions who have unidentified or unmet
palliative care needs in the community and
inadequate support for informal carers.
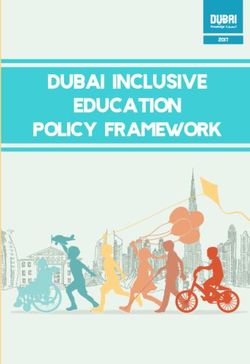
The total cost of unscheduled NHS care
for people in Scotland for people in their
last year of life was nearly £190 million,
of which only 3.9% was for provision of
primary care services. Innovating care
models to better support palliative care
delivery in communities could reduce
unscheduled care costs, as well as help the
majority of terminally ill people to die in
their place of choice.
Ambulance
£22m
Admissions A&E
£150mours £10m
GP OOH NHS
24
£4m £3m
132021 Scottish Parliament Manifesto
Homelessness In Scotland in 2018, there were an
People experiencing homelessness are estimated 195 homeless deaths, a 19%
often denied the right to die well with increase on the estimate of 164 in 201729.
dignity and face staggering levels of health Scotland had the highest rate of homeless
inequalities, as well as being unable to deaths in all GB countries in 2018 per
access palliative and end of life care when million population (35.9); this was more
they need it; we also know these groups are than double that of England (16.8) and
less likely to ask for help. Wales (14.5). Over half of those deaths in
2018 (53%) were drug related and 8% were
Many of those experiencing homelessness alcohol related.
have tri-morbidities consisting of a
physical condition, mental health issue and This data30 suggests that a significant
alcohol/substance dependency which has number of people experiencing
a significant impact on quality of life and homelessness will have died with a
life expectancy26 – in Scotland in 2018, the palliative care need but there is no
mean age at death was 43 for women and indication if, or when, they will have
44 for men27. received any specialist or generalist
palliative and end of life support.
End of life care wishes also remain poorly
understood for people experiencing • The Scottish Government should fully
homelessness, though research has shown implement the Homelessness and
a fear of needing care and losing control, Palliative Care Action Plan published
fear of dying alone, fear of being forgotten by Marie Curie in 2021.
and spiritual and practical concerns as
common concerns of homeless people
at end of life28. Similar to the general
195
population, not having early conversations
about end of life care wishes in partnership
with health and social care practitioners
and family/support networks (anticipatory homeless
care planning) can result in a more
distressing end of life experience.
deaths
In Scotland in 2018, there were
an estimated 195 homeless
deaths, a 19% increase on the
estimate of 164 in 2017.
In Scotland in 2018, the
mean age at death was 43
for women and 44 for men
142021 Scottish Parliament Manifesto
Social care
S
ocial care is an essential part of the but concluded that such a shift in care
care and support that terminally ill would not be possible without significant
people receive, helping them to live investment in social care.
as well as possible right up until their death. Marie Curie supports the Scottish
Social care can be provided in a person’s Government’s recent announcement
own home or through a care home. regarding establishing a National Care
It can help those who are terminally ill to Service in Scotland. We believe that this
remain at home for as long as possible, should be an early priority of the new
if that is their wish, through providing Scottish Government. Alongside colleagues
tailored, day-to-day support. Social care in MND Scotland, Hospice UK and Sue
teams often work in partnership with Ryder, we have identified the following key
specialist palliative care providers, such as issues which we believe any new national
Marie Curie, to deliver that care. service should address to support those
living with a terminal illness:
1. Anticipatory Care Planning:
In 2019/20, 88.6% of people in
Anticipatory Care Plans are developed
Scotland spent their last six months of
as early as possible, and are reviewed
life either at home or in a community
regularly, to support early intervention
setting, with 11.4% spending that time
and a proactive care approach to meeting
in hospital. This is equivalent to an
people’s changing social care needs.
average of 21 days in hospital in the six
months prior to death31. 2. Partnership working: Effective
Over the past 10 years, the partnership working, information sharing
percentage of time spent at home or and care co-ordination across statutory,
in a community setting in the last six voluntary and independent agencies
months of life has gradually increased in health and social care to support the
from 85.7% in 2010/11 to 88.6% in strategic planning, commissioning and
2019/2032. delivery of responsive services that meet
people’s social care needs.
However, long-standing fundamental 3. Workforce: The social care workforce
issues in social care in Scotland, including is supported and valued with sufficient
a lack of sustained financial support, numbers of staff in the right place with
workforce challenges and compromised the right skills and training to meet the
systems, have been exacerbated by the dynamic social care needs of people with
coronavirus pandemic. When combined terminal or life-shortening conditions.
with a sudden shift towards community 4. Commissioning: The commissioning
deaths since March 2020, coronavirus has and contracting of social care support
significantly impacted the care terminally services to have an agile response to the
ill people receive and placed already changing social care needs of people with
exhausted workforces under further terminal or life shortening conditions.
intense pressure.
5. Care packages: People with terminal
Before coronavirus, Marie Curie research or life shortening conditions are assessed
projected that by 2040 two-thirds of for social care packages swiftly and receive
people will die in community settings their full assessed care package without
152021 Scottish Parliament Manifesto
delay. These care packages should also In some cases, necessary care is simply
include regular carers, flexibility of visiting not available, and people wait for an
times and longer visits. unacceptably long time to be issued with
6. Self-directed support: People with independence or mobility aids or for care
terminal or life shortening conditions are packages to be arranged. Not only do these
supported to access the full range of self- factors contribute to people having to stay
directed support options, if they wish to, longer in hospital or hospice settings than
including allowing family members to be is necessary, but they can contribute to a
paid to care, where appropriate. worsening of a person’s physical, mental or
personal situation.
7. Carers: Informal and family carers of
people with terminal or life-shortening • There must be a much more rapid
conditions are fully supported during and response for aids and adaptations for
after the caring period, including respite those with a terminal illness.
and bereavement support. This should Wellbeing has been a long-standing issue
include recognising the financial impact in social care workforces, even before
of caring, particularly where many have coronavirus. There is often limited support
to reduce working hours or give up their available to staff to ensure they can address
jobs altogether. mental health concerns and issues, and
this can lead to staff becoming exhausted,
Among these issues, there are a number
extended sickness absences or even their
of specifics that we believe need to be
departure from social care.
addressed. A large proportion of social care
models/frameworks are rigidly confined to • Accessible emotional support must be
time and task, meaning carers are unable to available to all care providers which is
provide the full extent of care patients may proactively signposted through Health
require (usually more complex for palliative and Social Care Partnerships and
or end of life care service users) because statutory bodies to support social care
they only have 15-minute slots per patient. staff with their mental health, grief
This can have a domino effect throughout and bereavement.
the day and cause extensive overtime,
much of which is unpaid.
• We are calling for 15-minute time and
task models to be banned and replaced
by a strategic commissioning approach
which has person-centred outcomes at
the heart of delivery.
• The Real Living Wage per hour for
social care staff should be extended to
include overtime.
Greater investment and support in such
approaches and in organisations delivering
these services, such as Marie Curie, who
could work in partnership with social care
services would improve patient outcomes
and potentially relieve pressure on social
care services.
162021 Scottish Parliament Manifesto
Supporting digital
T
echnology has helped innovate Technology should support patient-centred
palliative and end of life care care for terminally ill people through a
services during the coronavirus blended approach with face-to-face
pandemic, allowing a continuity of care appointments and enable those working
and communication between terminally with patients to have the most up-to-date
ill patients, their families and carers and information about that care and be able to
health and social care teams. provide appropriate input.
Remote consultations have become a • The Scottish Government must
pivotal, day-to-day part of health and social continue to invest in national digital
care services as a result of coronavirus. health innovations to sustain remote
While they will never replace face-to- consultations and enable all those
face appointments, it is important that supporting terminally illness patients,
technology’s role in the future of palliative and patients themselves, to easily
and end of life care is mapped out to access digital records which can be
complement existing services. updated by anyone responsible for that
Marie Curie research into the effect of person’s care.
digital health consultations on our hospice
teams, patients and their families during While technology has been a lifeline
coronavirus has shown: to many, especially throughout the
pandemic, there is still a high prevalence
of digital exclusion. Minority groups,
Benefits: including ethnically diverse, the elderly
• An increase in patient choice in and low-income households, in addition
how they want to access palliative to rural communities which have limited
care services. or no access to digital devices and/or
connectivity, makes establishing and
• More flexible carer support making
maintaining engagement with palliative
clinical advice easily accessible for
care services significantly more complex.
those caring for someone with a
It has also led to high levels of isolation
terminal illness.
and loneliness.
• New modes of service delivery.
Challenges:
• With relationship building on first “Most of my clients do not
assessment. have access to technology or
• Patient/carer communication
difficulties.
don’t know how to use it and,
• Advanced Care Planning where especially during lockdown, this
an early relationship had not has made them very isolated and
been established.
has impacted heavily on their
mental health. Better access to
technology is needed and help
with using it.” Marie Curie Nurse
172021 Scottish Parliament Manifesto
Philip Hardman/Marie Curie
Marie Curie research indicates that While digital training/skills and connectivity
telephone consultations have been is vital, there needs to be greater
the preferred option of our patients recognition of issues with access to devices
throughout the pandemic, which may be as well as education and upskilling.
due to patients not having the appropriate • As part of the suggested
technology to facilitate video consultations Compassionate Community
at home, nervousness about the ease Network initiative, funding should
of using video consultations or feeling be specifically allocated to support
uncomfortable on camera. outreach and engagement with
• As part of the Scottish Government’s minority groups to ensure they can
investment in digital health, training engage with the palliative and end of
must be included for using digital life support they need.
systems and devices to upskill health
and social care workforces, terminally
ill patients and their families to
increase user confidence.
182021 Scottish Parliament Manifesto
Family (informal) carer support
T
he role of family carers in a person’s more and more carers and families have
palliative and end of life care is needed support.
crucial in helping terminally ill people • Carers need to be identified by health
get the day-to-day support they need for a and social care professionals and
good quality of life. But support for family then referred for support where
carers themselves is often overlooked and appropriate, including for an Adult
needs to be more greatly recognised33. Carer Support Plan (ACSP) or Young
Identifying informal carers to ensure they Carers Statement (YCS). For those
receive the support they are entitled to can caring for someone with a terminal
often be difficult and must be improved, as illness it will be important that this
many informal carers do not self-identify as support is prioritised and fast-tracked
carers or get picked up by formal services to avoid a breakdown in care40.
and therefore miss out on support and Carers should be able to access respite
benefits they may be eligible for. care when needed, as well as information
Family carer breakdown is the most likely and peer support through carers’ centres,
factor in a person with a terminal illness and others, to enable them to continue to
being admitted to a hospital, hospice or a provide care to the person they are looking
care home34. Having a live-in carer is also after and maintain their own wellbeing.
the single most important factor in whether This is especially important given the recent
someone is able to die at home or not35. shift from hospital to community deaths,
as well as the projected increase to two-
It has been estimated that an additional
thirds of people dying in community-based
400,000 people took on unpaid caring
settings by 2040.
roles during the first COVID 19 lock down
due to health and social care restrictions, Marie Curie’s report Life after death:
taking the total number of unpaid carers supporting carers after bereavement, in
in Scotland to around one million36. Before partnership with Reform Scotland and Sue
coronavirus, the estimated value of unpaid Ryder, calls for more recognition of the
care work in Scotland is £36 billion37. impact of death on the carer and the effect
on the carer’s physical and mental health,
Unpaid care in Scotland over the course
their relationships, their ability to work and
of the pandemic to date has been
their finances:
valued at £10.9 billion38 and 3 in 5 of
us will become carers at some point in • A new Carers (Bereavement Support)
our lives39. (Scotland) Bill should be introduced
early in the next Parliament to provide
Evidence from Marie Curie services working
support plans for carers following the
during the early part of the pandemic
end of their caring role.
found that many people with family carers
were slow to engage with services and • A new fund should be allocated to
often much later at crisis point which support training and education for
caused further challenges. carers returning to work/seeking
employment.
Latterly, with the greater shift in care into
• A new Post-Caring Support Payment
the community and people’s own homes.
should be created to help carers
Marie Curie’s nursing and community
struggling financially following the end
services have been in considerable
of their caring role.
demand and stretched to capacity, as
192021 Scottish Parliament Manifesto
Grief and bereavement
W
hen you lose a loved one, sadness where lockdown regulations significantly
and grief can make dealing restricted hospital, hospice and care home
with everyday life a challenge. visiting which caused distress to patients,
It can be hard to concentrate and make families and carers and resulted in a lonelier
simple decisions. end of life experience for many.
People experience grief and bereavement Coronavirus regulations also influenced
at different stages and in different ways, how people were able to grieve for their
in some cases even starting before the loss, which often were in much more
person has died. Grief can also continue for isolating environments and will have a
extended periods after someone has died. lasting physical and emotional impact.
While the pandemic has acted as a catalyst We also know that minority groups are less
to improve some support being offered, it likely to ask for help, and usually experience
previously has not been well recognised or more complicated grief as a result of social
available for people who have experienced circumstances than the general population
a bereavement; this also includes health which has been exacerbated during
and social care professionals. the pandemic.
The impact on families can be equally as • Marie Curie supports the Bereavement
damaging, with a significant increase in Charter for Scotland which champions
levels of grief and bereavement, as well as everyone’s right to access the support
more complicated grief, being recorded they need following a bereavement;
for those whose family members did not which will be different for each person.
get the palliative support they needed.
This has been exacerbated by coronavirus,
Philip Hardman/Marie Curie
202021 Scottish Parliament Manifesto
Education and training
T
raining is a vital element of • There must be a flexible, ongoing
professional development, palliative and end of life care
knowledge and experience education programme established
building but many health and social care which reflects a blend of face-to-
professionals face significant challenges face and digital learning to provide
accessing and undertaking palliative and better training for everyone delivering
end of life care training. This can result in palliative care including families and
(early) referral opportunities being missed informal carers.
due to lack of knowledge, and terminally ill Within our education system for young
patients missing out on the care they need. people, there is a wide spectrum of
A Palliative and End of Life Care willingness and capability in teachers
Education and Training Framework by and staff to talk about dying, death and
NHS Education for Scotland (NES) and the bereavement in schools, colleges and
Scottish Social Services Council (SSSC) to universities, yet we are still producing a
support health and social care professionals younger generation who are not equipped
has been developed, but it is unknown to be able to handle bereavement, or even
how workforces are performing against the to talk about it. The education system must
framework’s principles and what structure build resilience and support by working
is in place (if any) to ensure consistent to remove taboos around dying, death
training delivery. and bereavement.
Currently, we understand that much of the • The Curriculum for Excellence should
social care workforce does not currently be reviewed to ensure that talking
have palliative and end of life care training, about dying, death and bereavement
yet is expected to deliver it for patients at is a key component and that teachers
home and in care homes. across Scotland have the resources and
support to engage students in open
• We are calling for a review of health
conversations and discussions about
and social care workforces against
these issues.
the NES/SSSC and Palliative and End
of Life Care Framework to understand
current care delivery and areas for
improvement.
• The introduction of mandatory
palliative and end life care training for
all health and social care staff working
with terminally ill people to ensure
high, consistent standards of care.
Resource is one of the main obstacles for
being unable to release staff for palliative
and end of life education and training,
which has been exacerbated through
the coronavirus pandemic by additional
demands on acute settings, primary care
and social care.
212021 Scottish Parliament Manifesto
Welfare and benefits
T
he financial impact of terminal illness • Extend eligibility for the Carer’s
on the person affected and their Allowance and Carer’s Allowance
family is often significant. Terminal Supplement for up to six months after
conditions require a range of support at all the person’s caring role comes to an
levels, especially as they advance, which end (from the current eight weeks).
many people are unable to fund themselves Any replacement to Carer’s Allowance
independently. introduced by the next Scottish
Easy access to benefits is paramount Government must continue for at least
for terminally ill people, their families six months after the death of the cared
and carers to enable them to have as for person.
high quality of life as possible. But many There has been some progress in helping
people affected by terminal illness do terminally ill people access benefits more
not apply for benefits because they do quickly and easily. In 2018, Marie Curie
not know what they are entitled to, they and MND Scotland successfully led the
do not think they will be eligible, there is campaign for the Social Security (Scotland)
a stigma associated with claiming some Bill to include a legal definition of terminal
benefits and people can be put off by long illness that was based on clinical judgement
application processes. and not one that included timescales,
We know that in many cases people as currently used by the DWP, to support
affected by terminal illness can be eligible decision-making for those applying for
for more than one benefit. benefits through the Special Rules. This also
means doctors and nurses can express this
• We are calling for a simple online clinical judgement to enable the quickest
application form to be created to response possible.
support applications for multiple
benefits to minimise time spent However, it will create a two-tier system in
completing forms and provide a better Scotland upon its introduction in 2021 –
experience for those applying for as Universal Credit and Employment and
multiple benefits. Support Allowance will remain reserved to
Westminster.
• Easy to read materials should be
distributed to accessible locations This could mean that potentially, a person
to ensure essential information is in Scotland may be able to access fast
available to help everyone affected by tracked disability benefits but be denied
terminal illness understand what they the same if applying for Universal Credit. It
are entitled to and how to claim it. will require doctors to use two very different
As outlined above, informal family carers definitions and potentially reach two
face considerable financial pressures, both different conclusions for a person who is
during their caring and following the end of terminally ill and wishing to access benefits
the caring role, particularly when the cared under the special rules for terminal illness.
for person has died. We believe that carers It will also require doctors and nurses to
should be better supported financially, use two forms, and work with two social
particularly following a bereavement. security agencies.
222021 Scottish Parliament Manifesto
• Marie Curie and our partners are reduction of hours or may have even lost
calling for the UK Government to adopt their job. Many may also have been unable
the Scottish Government’s definition of to return to work as the terminal condition
terminal illness for all benefits, which of the person they are caring for may
will not only lead to a fairer system, have deteriorated further throughout the
but will prevent a two-tier system pandemic requiring greater care, which
in Scotland. they have been unable to access.
The current economic climate and • The Scottish Government should fund
recession caused by coronavirus has further research to understand what
created even greater financial pressures impact the pandemic has had on those
and reliance on social security for some caring for someone with a terminal
terminally ill people, their families and illness at home, and subsequently
carers. Carers who were working pre- help inform the role of Scottish Social
pandemic may not have been able to Security in coronavirus recovery
throughout the coronavirus pandemic and beyond.
due to being on furlough, have seen a
232021 Scottish Parliament Manifesto
References
1. National Records of Scotland: Vital Events pmc/articles/PMC5914070/” Palliative
Reference Tables 2019 Open 2021 Care for Homeless People; a systematic
2. Finucane. A et al How many people will review of the concerns, care needs
need palliative care by 2040? A mixed and preferences and the barriers and
method study of projected palliative care facilitators for providing palliative care
need and recommendations BMJ Open 2018
2021 12. https://www.mariecurie.org.uk/
3. Finucane, A.M., Bone, A.E., Evans, C.J. et al. globalassets/media/documents/policy/
The impact of population ageing on end- campaigns/equity-palliative-care-uk-
of-life care in Scotland: projections of report-full-lse.pdf
place of death and recommendations for 13. Finucane. A et al How many people will
future service provision. BMC Palliat Care need palliative care by 2040? A mixed
18, 112 (2019). https://doi.org/10.1186/ method study of projected palliative care
s12904-019-0490-x need and recommendations BMJ Open
4. Grande, G., Stajduhar, K., Aoun, S., Toye, 2021
C., Funk, L., Addington-Hall, J, Todd, C. 14. Finucane. A et al The impact of
(2009). Supporting lay carers in end of life population ageing on end-of-life care in
care: current gaps and future Scotland: projections of place of death
5. https://www.mariecurie.org.uk/help/ and recommendations for future service
support/diagnosed/recent-diagnosis/ provision
palliative-care-end-of-life-care#what 15. https://www.isdscotland.org/Health-
6. National Records of Scotland (NRS) (2018) Topics/Health-and-Social-Community-
7. Finucane. A et al: Electronic are
Care/End-of-Life-Care/
coordination systems for people with 16. https://www.ncbi.nlm.nih.gov/pmc/
advanced progressive illness: a mixed- articles/PMC6917358/
methods evaluation in primary care. 17. Gott, M, Morgan T, Williams L: Gender
British Journal of General Practice https:// and Palliative Care: A Call to Arms SAGE
bjgp.org/content/70/690/e20 Journals
8. Finucane. A et al: Electronic are 18. https://www.mariecurie.org.uk/
coordination systems for people with globalassets/media/documents/policy/
advanced progressive illness: a mixed- briefings-consultations/scotland-
methods briefings/marie-curie-briefing-
9. https://www.mariecurie.org.uk/ inequities-bame.pdf
globalassets/media/documents/policy/ 19. https://www.mariecurie.org.uk/
campaigns/equity-palliative-care-uk- globalassets/media/documents/policy/
report-full-lse.pdf briefings-consultations/scotland-
10. https://www.mariecurie.org.uk/ briefings/marie-curie-briefing-
globalassets/media/documents/policy/ inequities-lgbt.pdf
campaigns/equity-palliative-care-uk- 20. https://www.mariecurie.org.uk/
report-full-lse.pdf globalassets/media/documents/policy/
11. Klop et al “https://www.ncbi.nlm.nih.gov/ briefings-consultations/scotland-
242021 Scottish Parliament Manifesto
briefings/marie-curie-briefing- Spent in a Community Setting
inequities-older-people.pdf 33. https://www.mariecurie.org.uk/
21. Ibid globalassets/media/documents/policy/
22. Clark, D., et al Imminence of death policy-publications/2018/marie-curie-
among hospital inpatients: Prevalent and-macmillan-getting-it-right-for-
cohort study. Palliative Medicine, 28(6), carers-final-report-november-2018.pdf
474–479. (2014) 34. https://www.goldstandardsframework.
23. https://www.mariecurie.org.uk/ org.uk/cd-content/uploads/files/
globalassets/media/documents/policy/ Library%2C%20Tools%20%26%20
policy-publications/2020/f405_past- resources/ABC%20Palliative%20Care.pdf
present-and-future-eolc-in-scottish- 35. https://www.mariecurie.org.uk/
hospitalsv7.pdf globalassets/media/documents/policy/
24. https://www.mariecurie.org.uk/ campaigns/equity-palliative-care-uk-
globalassets/media/documents/policy/ report-full-lse.pdf
policy-publications/2020/f405_past- 36. https://www.carersuk.org/images/
present-and-future-eolc-in-scottish- CarersWeek2020/CW_2020_Research_
hospitalsv7.pdf Report_WEB.pdf
25. Mason B, Kerssens JJ,Stoddart A, et al. 37. Time to Care Report 2020; Oxfam https://
Unscheduled and out-of-hours care oxfamapps.org/scotland/2020/01/20/
for people in their last year of life: a unpaid-care-worth-36bn/
retrospective cohort analysis of national 38. Carers Scotland; https://www.carersuk.
datasets. BMJ Open 2020;0:e041888. org/scotland/news/unpaid-carers-save-
26. Webb WA, Mitchell T, Nyatanga B, scottish-government-43-million-every-
Snelling P How to explore end of life day-of-the-pandemic
preferences of homeless people in the UK 39. Carers Scotland; Facts and Figures
European Journal of Palliative Care 2018 https://www.carersuk.org/scotland/news/
27. National Records Scotland: Homeless facts-and-figures
Deaths 2017 and 2018
28. Mitchell Webb T, Snelling P, Nyatanga
B Life’s hard and then you die: the end
of life priorities of people experiencing
homelessness in the UK Academic Journal
March 2020
29. National Records Scotland: Homeless
Deaths 2017 and 2018
30. National Records Scotland: Homeless
Deaths 2017 and 2018
31. In 2019/20 there were 56,011 deaths in
Scotland, including falls, but excluding
other external causes of death. The
statistics quoted reflect these figures.
PHS Percentage of Last Six Months of Life
Spent in a Community Setting.
32. PHS Percentage of Last Six Months of Life
25You can also read